
Volume 25 - 2010
Contents
Neuroimaging
PW01-155 - Seasonal Alterations Of Serotonin-1a Receptor Binding In The Healthy Human Brain
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1554
-
- Article
-
- You have access
- Export citation
PW01-156 - Exploration Of Irony Appreciation In Schizophrenia: A Functional Mri Study
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1555
-
- Article
-
- You have access
- Export citation
PW01-157 - Mesolimbic Dysfunction During Novelty Detection In Schizophrenia
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1556
-
- Article
-
- You have access
- Export citation
Others
PW01-158 - Differentials Effects Of Olanzapine And Risperidone On Plasma Adiponectin Levels Over Time: A Prospective Study
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1557
-
- Article
-
- You have access
- Export citation
-
Introduction
Recent research has shown that adiponectin levels in patients with schizophrenia vary similar to the general population. Moreover, antipsychotic medication may influence adiponectin levels, independent of metabolic parameters. We hypothesise different antipsychotics might vary in their effect on adiponectin levels independent of BMI and metabolic syndrome (MetS) status.
Methods113 patients, with similar baseline demographic and metabolic characteristics, received either risperidone (n=54) or olanzapine (n=59). They were followed prospectively for 12 weeks. Adiponectin levels as well as general metabolic parameters were measured at baseline, 6 weeks and 12 weeks.
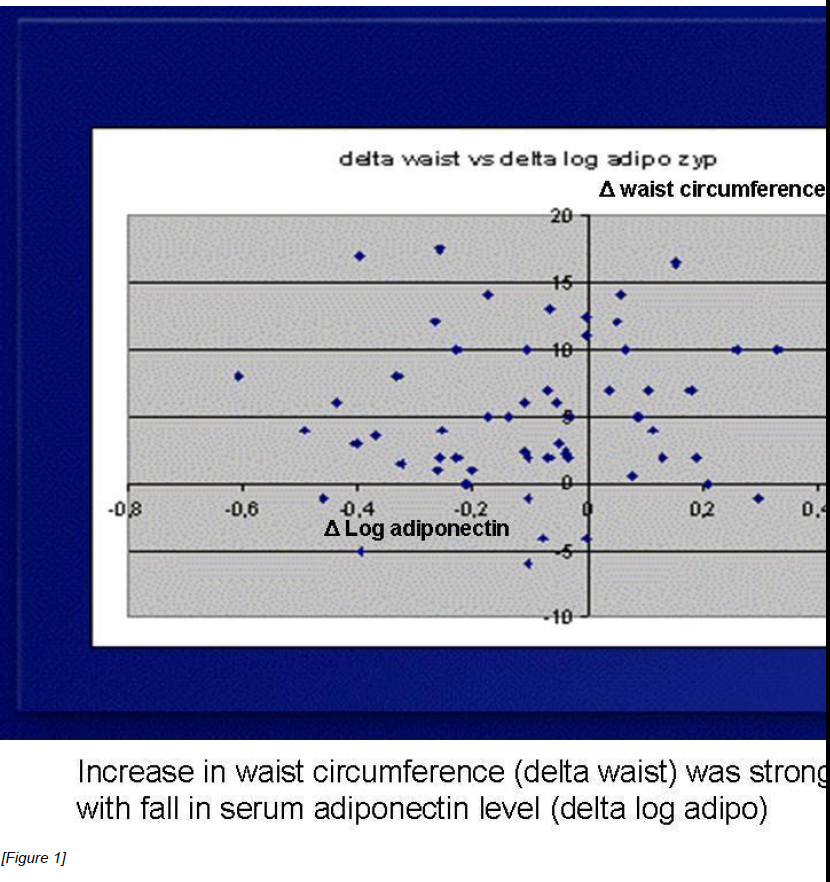
ResultsWe observed a significant treatment by time interaction, showing an adiponectin increase in the risperidone treated patients and an adiponectin decrease in olanzapine treated patients. This effect was independent of BMI and the presence/absence of the metabolic syndrome. There was a significant association between fall in adiponectin and increase in waist circumference in the Olanzapine treated group (Figure 1).There was no change in HOMA-IR as a measure of insulin resistance in either group.
 Conclusion
ConclusionWe observed a differential effect of antipsychotic treatment (risperidone vs olanzapine) on adiponectin levels over time, independent of BMI (and MetS) suggesting an effect of olanzapine on adipose tissues, similar to what has been observed in animals models. The effects on adiponectin levels may partly explain the increased rates of obesity with Olanzapine.

PW01-159 - Neuropsychiatric Disturbances In Chronic Viral Liver Diseases Treated With Interferon: Prevalence And Management
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1558
-
- Article
-
- You have access
- Export citation
PW01-160 - Burden Of Chronic Insomnia Characterized By Nighttime Awakenings Among Diabetes Patients
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1559
-
- Article
-
- You have access
- Export citation
PW01-161 - Generalized Anxiety Disorder And Immunity Markers In A Stratified Population Sample
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1560
-
- Article
-
- You have access
- Export citation
PW01-162 - Destigmatizing Mental Ilness
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1561
-
- Article
-
- You have access
- Export citation
PW01-163 - The Rate And Causes Of Mortality In Psychiatric Patients
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1562
-
- Article
-
- You have access
- Export citation
PW01-164 - Neuropsychological Assessment Of Cardiac Rehabilitation Following Cardiac Surgery - Preliminary Results
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1563
-
- Article
-
- You have access
- Export citation
PW01-165 - Identification Of A De Novo 22q11.2 Distal Deletion In An Adult Female Referred For An Anxiety Disorder
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1564
-
- Article
-
- You have access
- Export citation
PW01-166 - Agmatine Enhances The Anticonvulsant Effect Of Lithium Chloride On Ptz-Induced Seizure In Mice: Involvement Of L-Arg-Nitric Oxide Pathway
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1565
-
- Article
-
- You have access
- Export citation
PW01-53 - Investigation Of Job Satisfaction And Mental Health In Health Care Workers In Central Greece
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1566
-
- Article
-
- You have access
- Export citation
PW01-54 - Correlation Of A Set Of Gene Variants, Life Events And Personality Features On Adult Adhd Severity
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1567
-
- Article
-
- You have access
- Export citation
PW01-55 - Stress And Burnout In Train Engine Drivers
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1568
-
- Article
-
- You have access
- Export citation
Philosophy and psychiatry
PW01-167 - The Emergence Of Neural Stem Cells As Example For “Kuhnian” Revolution In Biology Or Misconception Of The Scientific Community?
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1569
-
- Article
-
- You have access
- Export citation
PW01-168 - Disturbance Of Intentionality: A Phenomenological Approach For The Development Of Schneiderian First-Rank Symptoms In Schizophrenia
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1570
-
- Article
-
- You have access
- Export citation
PW01-169 - Affective Attunement. Towards An Alternative Explanation Of Delusion
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1571
-
- Article
-
- You have access
- Export citation
Prevention of mental disorders
PW01-170 - The Stress-Vulnerability Model; How Does Stress Impact On Mental Illness At The Level Of The Brain....And What Are The Consequences?
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1572
-
- Article
-
- You have access
- Export citation
PW01-171 - Coping Strategies In Adolescents With Psychotic-Like Experiences
-
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1573
-
- Article
-
- You have access
- Export citation