This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
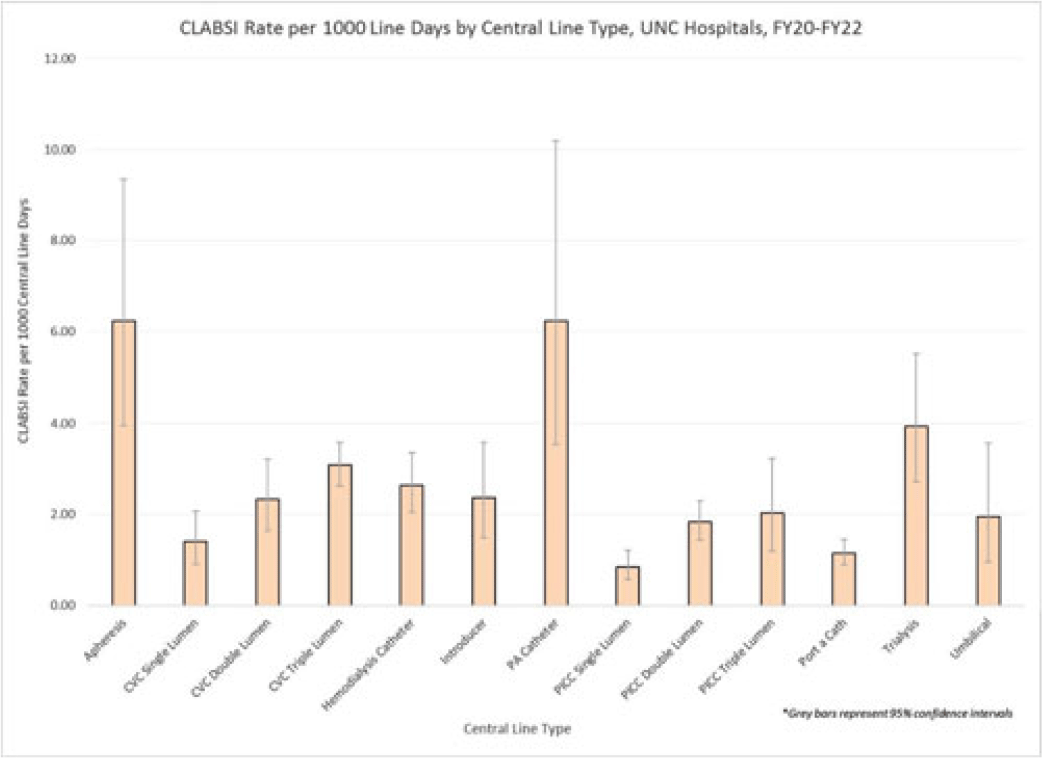
Background: Central-line–associated bloodstream infections (CLABSIs) are linked to increased morbidity and mortality, longer hospital stays, and significantly higher healthcare costs. Infection prevention guidelines recommend line placement in specific insertion locations over others because of the relative risk of infection. The purpose of this study was to assess CLABSI rates by line type to determine whether some central lines had a lower risk of infection and should be recommended over others given similar clinical indications. Methods: At UNC Hospitals, data were obtained on central lines across a 3-year period (FY20–FY22) from the EMR (Epic Systems). Central lines were categorized as apheresis catheters, CVC lines (single, double, or triple lumen), hemodialysis catheters, introducer lines, pulmonary artery (PA) catheters, PICC lines (single, double, or triple lumen), port-a-catheters, trialysis catheters, or umbilical lines. The line type(s) associated with each CLABSI during the same period were recorded, and CLABSI rates by line type per 1,000 central-line days were calculated using SAS software. If an infection had >1 central-line device type associated, the infection was counted twice when calculating the CLABSI rate by line type. We calculated 95% CIs for each point estimate to assess for statistically significant differences in rates by line type. Results: During FY20–FY22, there were 264,425 central-line days and 458 CLABSIs, for an overall CLABSI rate of 1.73 CLABSIs per 1,000 central-line days. Also, 16% of patients with a CLABSI had >1 type of central line in place. Stratified data on CLABSI rates by each central-line type is presented in the Figure. CLABSI rates were highest in patients with apheresis lines (6.22; 95% CI, 3.96–9.35) and PA catheters (6.22; 95% CI, 3.54–10.20), and the lowest CLABSI rates occurred in patients with PICC lines (1.44; 95% CI, 1.19–1.73) and port-a-catheters (1.14; 95% CI, 0.89, 1.45). For both CVC and PICC lines, as the number of lumens increased from single to triple, CLABSI rates increased, from 0.91 to 2.63 and from 0.57 to 1.20, respectively. Conclusions: At our hospital, different types of central lines were associated with statistically higher CLABSI rates. Additionally, a higher number of lumens (triple vs single) in CVC and PICC lines were also associated with statistically higher CLABSI rates. These findings reinforce the importance of considering central-line type and number of lumens to minimize risk of CLABSI while ensuring that patients have the best line type based on their clinical needs.
Disclosures: None
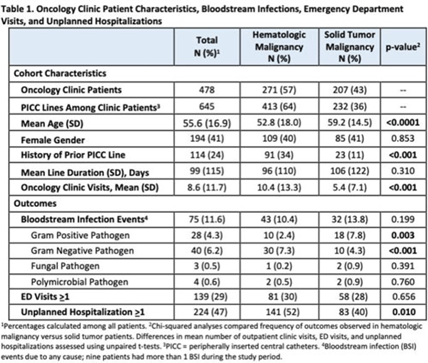
Background: Oncology patients are at high risk for bloodstream infection (BSI) due to immunosuppression and frequent use of central venous catheters. Surveillance in this population is largely relegated to inpatient settings and limited data are available describing community burden. We evaluated rates of BSI, clinic or emergency department (ED) visits, and hospitalizations in a large cohort of oncology outpatients with peripherally inserted central catheters (PICCs). Methods: In this prospective, observational study, we followed a convenience sample of adults (age>18) with PICCs at a large academic outpatient oncology clinic for 35 months between July 2015 and November 2018. We assessed demographics, malignancy type, PICC insertion and removal dates, history of prior PICC, and line duration. Outcomes included BSI events (defined as >1 positive blood cultures or >2 positive blood cultures if coagulase-negative Staphylococcus), ED visits (without hospitalization), and unplanned hospitalizations (excluding scheduled chemotherapy hospitalizations). We used χ2 analyses to compare the frequency of categorical outcomes, and we used unpaired t tests to assess differences in means of continuous variable in hematologic versus solid-tumor malignancy patients. We used generalized linear mixed-effects models to assess differences in BSI (clustered by patient) separately for gram-positive and gram-negative BSI outcomes. Results: Among 478 patients with 658 unique PICC lines and 64,190 line days, 271 patients (413 lines) had hematologic malignancy and 207 patients (232 lines) had solid-tumor malignancy. Cohort characteristics and outcomes stratified by malignancy type are shown in Table 1. Compared to those with hematologic malignancy, solid-tumor patients were older, had 47% fewer clinic visits, and had 32% lower frequency of prior PICC lines. Overall, there were 75 BSI events (12%; 1.2 per 1,000 catheter days). We detected no significant difference in BSI rates when comparing solid-tumor versus hematologic malignancies (P = 0.20); BSIs with gram-positive pathogen were 69% higher in patients with solid tumors. Gram-negative BSIs were 41% higher in patients with hematologic malignancy. Solid-tumor malignancy was associated with 4.5-fold higher odds of developing BSI with gram-positive pathogen (OR, 4.48; 95% CI, 1.60–12.60; P = .005) compared to those with hematologic malignancy, after adjusting for age, sex, history of prior PICC, and line duration. Differences in gram-negative BSI were not significant on multivariate analysis. Conclusions: The burden of all-cause BSIs in cancer clinic adults with PICC lines was 12% or 1.2 per 1,000 catheter days, as high as nationally reported inpatient BSI rates. Higher risk of gram-positive BSIs in solid-tumor patients suggests the need for targeted infection prevention activities in this population, such as improvements in central-line monitoring, outpatient care, and maintenance of lines and/or dressings, as well as chlorhexidine bathing to reduce skin bioburden.
Disclosures: None
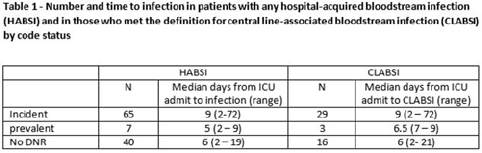
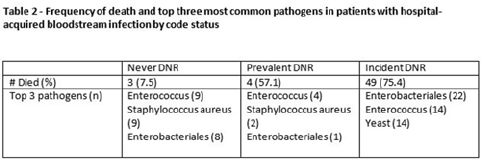
Background: All critically ill patients are at risk for hospital-acquired bloodstream infection (HABSI). At any time, however, there is heterogeneity among patients in the ICU; some patients have the added complexity of end-of-life discussions. We sought to better understand the patients in our medical intensive care unit (MICU) with HABSIs that do and do not meet the NHSN definition for a central-line–associated bloodstream infection (CLABSI) event by evaluating for the presence of a do-not-resuscitate (DNR) order. Methods: The study was conducted at our 66-bed MICU at the Cleveland Clinic Main Campus between January 2021 and September 2022. Surveillance for HABSI to include determination of CLABSI is performed prospectively according to the NSHN definition. The electronic health record was queried for each patient with a HABSI for the presence of a DNR order. DNR orders were categorized as follows: prevalent (DNR orders present at the time of admission to the MICU), incident (orders entered after admission to the MICU), or no DNR (for patients without an order at any time during their MICU stay). For incident orders, time from order to HABSI was recorded. Time to event was calculated as days between ICU admission to HABSI. Results: During the observation period there were 36,477 MICU patient days and 4,815 admissions. There were 112 HABSIs, of which 48 (43%) were CLABSIs. Overall, 65 patients were categorized as incident DNR, 7 were categorized as prevalent DNR, and 40 were categorized as no DNR. For patients with an incident DNR order, 50 HABSIs occurred on the date of or before the order and 15 occurred after the order. In patients in whom HABSI occurred after the incident DNR order, the median number of days between DNR order and HABSI was 11 days (range, 1–69). Discussion: In our MICU, >50% of HABSIs and 60% of CLABSIs occurred in patients with a DNR order incident to their MICU stay. Interventions to prevent hospital-acquired bloodstream infection and the analysis of the events are inextricably linked to issues of end-of-life care for critically ill patients. Further exploration of patient characteristics easily obtainable from the EHR, such as DNR orders, is necessary to inform best practices for prevention and risk adjustment of bloodstream infection rates.
Disclosures: None
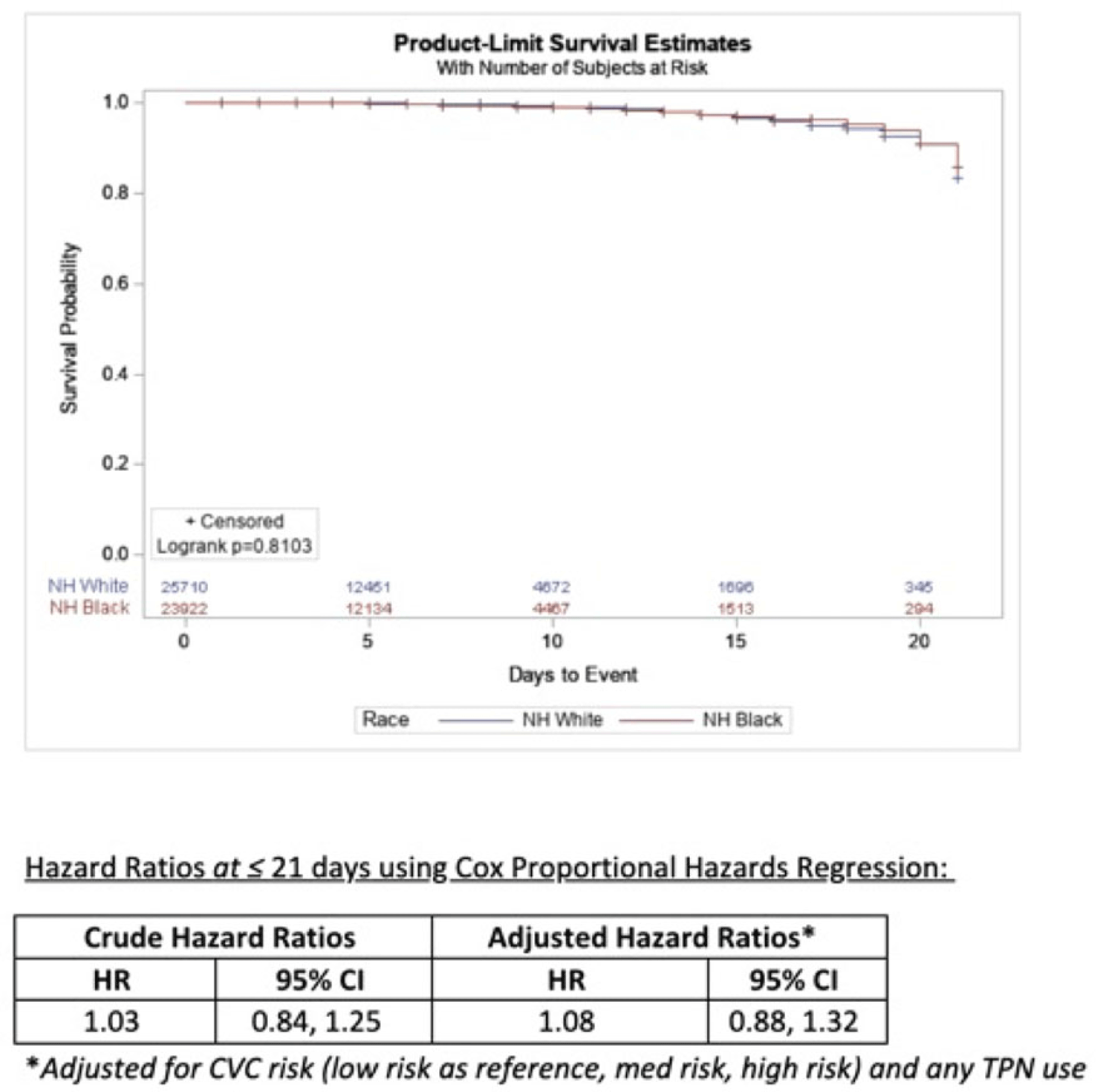
Background: Socioeconomic barriers or divergent implementation of prevention measures may impact risk of healthcare-associated infections by racial groups. We utilized a previously studied cohort of patients to quantify disparities in central-line–associated bloodstream infection (CLABSI) risk by race accounting for inherent differences in risk related to device utilization. Methods: In a retrospective cohort of adult patients at 4 hospitals (range, 110–733 beds) from 2012 to 2017, we linked central-line data to patient encounter data: race, age, comorbidities, total parenteral nutrition (TPN), chemotherapy, CLABSI. Analysis was limited to patients with >2 central-line days and <3 concurrent central lines. Patient exposures were calculated for each central-line episode (defined by insertion and removal dates); analysis of central-line episode-specific risk of CLABSI among Black versus White patients adjusted for clinical factors, duration of central-line episode, and central-line risk category (ie, low: single port, dialysis or PICC; medium: single temporary or nontunneled; or high: any concurrent central-lines) in Cox proportional hazards regression of time to CLABSI. Results: In total, 526 CLABSIs occurred a median of 14 days after insertion among 57,642 central-line episodes in 32,925 patients. CLABSIs occurred in similar frequency across racial groups: 217 (1.7%) among Black patients, 256 (1.6%) among White patients, and 11 (1.6%) among Hispanic patients (also 42 among unknown or other race). Duration of central-line episode was similar between racial groups (median, 5 days). Black patients were less likely to have medium-risk central lines (34%) compared to white patients (RR, 0.82; 95% CI, 0.79–0.84), but they had a similar frequency of high-risk central lines (21%; RR, 1.0; 95% CI, 1.0–1.1). Compared with low-risk central lines, risk of CLABSI was increased among medium-risk central lines (RR, 1.3; 95% CI, 1.0–1.7) and high-risk central lines (RR, 2.2; 95% CI, 1.8–2.7). CLABSIs were more likely in TPN central lines (RR, 2.3; 95% CI, 1.9–2.7) than others, but they were not more likely among Black patients than White patients (RR, 0.9; 95% CI, 0.1–1.1). In survival analysis, there were 24,700 central-line episodes among Black patients compared to 26,648 episodes among White patients; adjusting for central-line risk and TPN, the risk of CLABSI was similar during the first 21 days of central-line use (adjusted hazard ratio, 1.08; 95% CI, 0.88–01.32) (Fig. 1). Conclusions: After accounting for central-line configuration, Black patients did not have a higher risk of CLABSI within 21 central-line days. Further evaluation is warranted to assess racial disparities in risks of other healthcare-associated infections and to determine whether a lack of CLABSI-specific racial disparities can be replicated in other regions and healthcare systems.
Disclosures: None
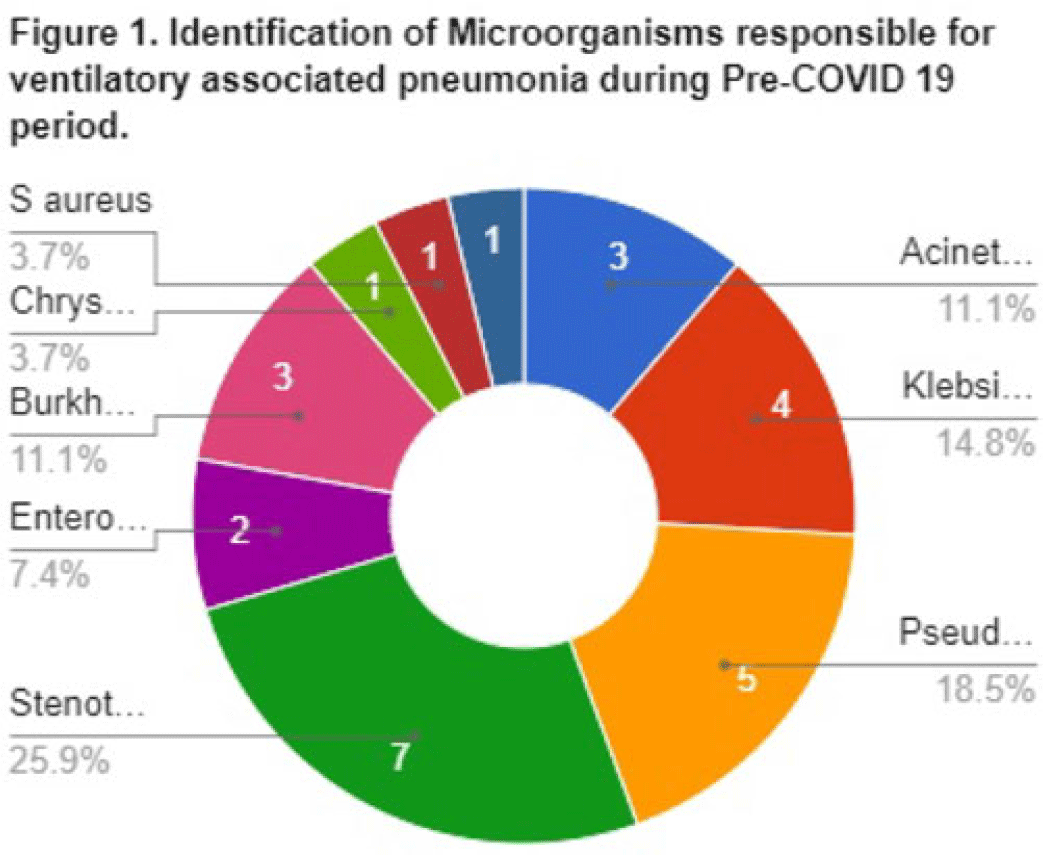
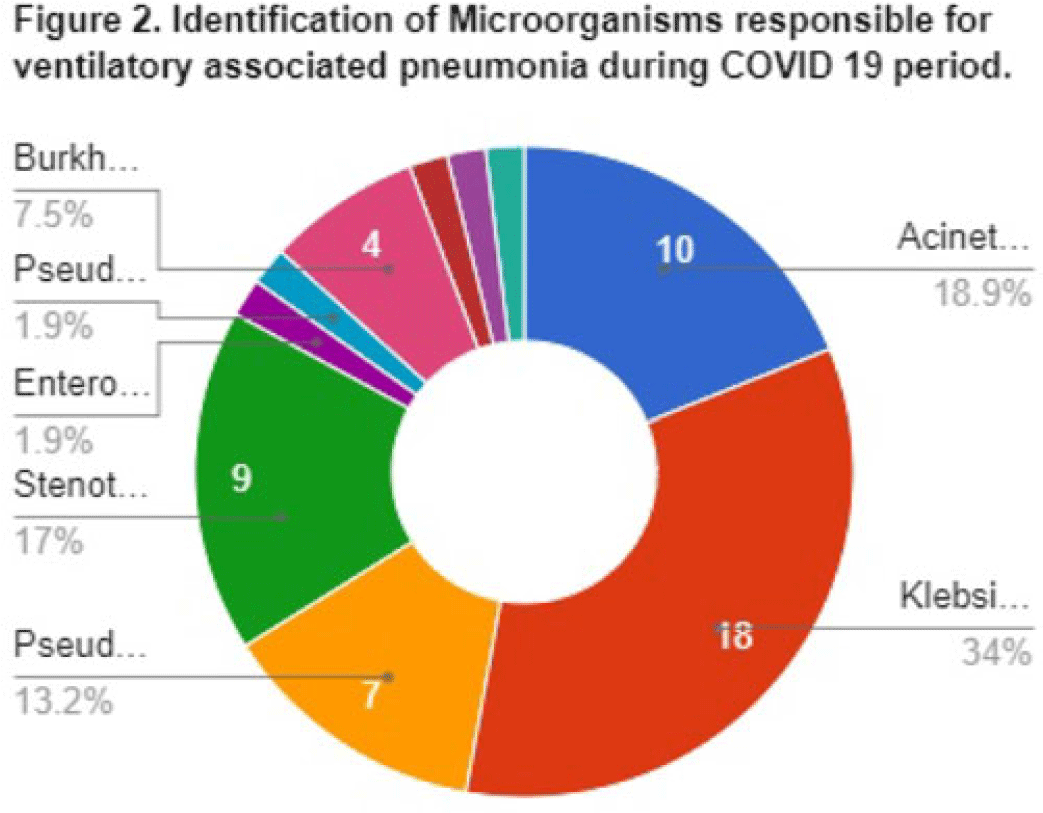
Background: Data on the incidence and outcome of ventilator-associated pneumonia (VAP) and multidrug-resistant VAP (MDR-VAP) among COVID-19 patients are limited. We compared the incidence and incidence density (ie, number of VAP per 1,000 ventilatory days) of MDR-VAP prior to and during the COVID-19 period in an urban, tertiary-care hospital. Methods: A retrospective study was conducted to compare the incidence, profile, and outcomes of patients with MDR-VAP during the pre–COVID-19 period (2018–2019) and during the COVID-19 pandemic (2020–2021). Results: In total, 80 (22%) of 362 patients developed VAP and were included in the cohort: 27 (33.75%) from the pre–COVID-19 period and 53 (66.25%) from the COVID-19 period, respectively. Most were male [20 (74%) of 27 vs 34 (64%) of 53], with median ages of 66 years (range, 35–90) and 67 years (range, 32–92) in the pre–COVID-19 and COVID-19 periods, respectively. Comorbidities were similar between the 2 periods, except for cardiovascular disease (14 vs 11; P = .005) and chronic lung disease (14 vs 9; P = .0012), which decreased significantly from the pre–COVID-19 period to the COVID-19 period. Only 15 (56%) of 27 versus 37 (70%) of 53 patients developed MDR-VAP during the pre–COVID-19 and COVID-19 period, with incidence densities of 19.3 of 1,000 and 27.8 of 1,000 ventilator days (P = .0371), respectively. The median length of stay prior to VAP for the pre–COVID-19 and COVID-19 periods were 17 and 10 days, respectively (P < .0001). Extended-spectrum β-lactamase (ESBL) resistance increased significantly from 1 (3.7%) of 27 before COVID-19 to 15 (28.3%) of 53 during the COVID-19 period. Carbapenem-resistant Enterobacteriaceae (CRE) resistance was higher before COVID-19 than during the COVID-19 period: 15 (56%) of 27 versus 10 (19%) of 53. In both periods, Klebsiella pneumoniae and Acinetobacter baumannii were the most common pathogens isolated. Mortality was high in both periods at 93% and 83%, respectively. Only female sex was associated with MDR-VAP in the COVID-19 period on multivariate analysis (OR, 3.47; 95% CI, 1.019–11.824; P < .047). Conclusions: The frequency of VAP and MDR-VAP increased during the COVID-19 period, despite a shorter median hospital stay. Mechanisms of resistance differed in the pre–COVID-19 and COVID-19 periods. Mortality with VAP was extremely high. The factors associated with increased risk of VAP and COVID-19 need to be studied further, and measures to prevent VAP should be prioritized.
Disclosures: None
