This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
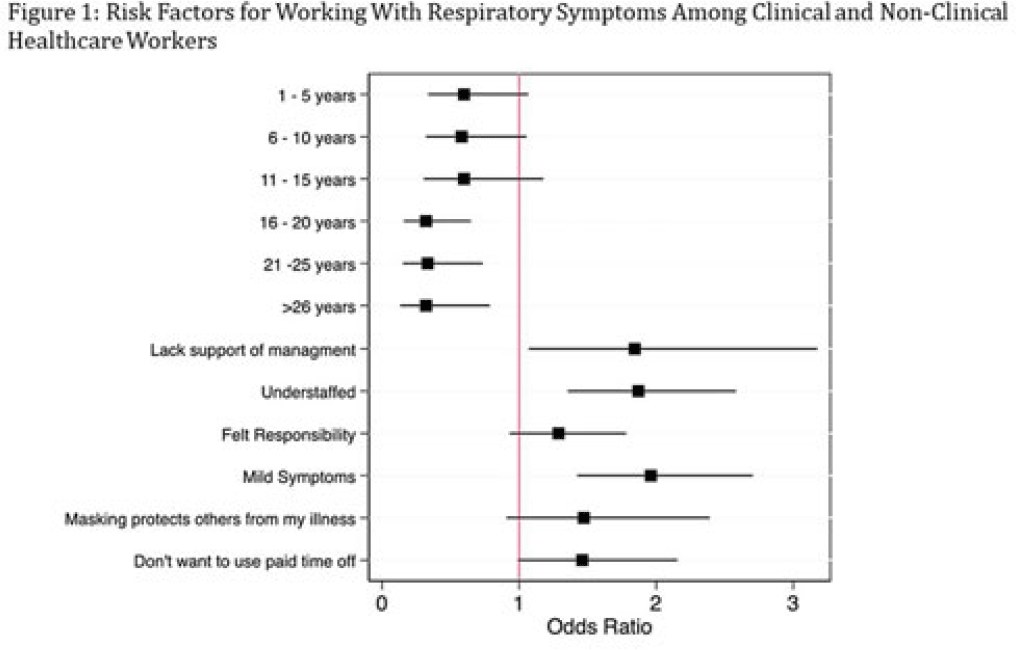
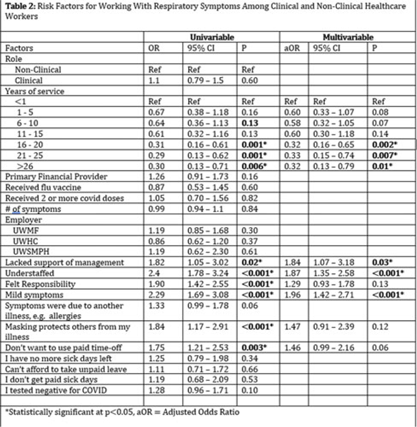
Background: Amid the COVID-19 pandemic, healthcare systems were stretched thin, with staffing shortages posing substantial challenges. Limiting spread of COVID-19 among healthcare professionals (HCP) is paramount to preventing exacerbation of such shortages, but strategies are highly dependent on HCP self-screening for symptoms and isolating when present. We examined HCP perceptions of barriers and factors that facilitate staying home when experiencing respiratory symptoms. Methods: At an academic tertiary-care referral center, in inpatient and ambulatory settings, we conducted an anonymous electronic survey between March 11, 2022, and April 12, 2022. Using logistic regression analysis, we analyzed predictors of employees reporting to work with respiratory symptoms using STATA and SAS software. Results: In total, 1,185 individuals including 829 clinical staff and 356 nonclinical staff responded to the survey. When excluding participants who reported working “remotely” (N = 381) and those who reported being unsure of whether they had worked with symptoms (N = 14), the prevalence of working with respiratory symptoms was 63%. There was no significant difference between clinical and nonclinical staff (OR, 1.1; 95% CI, 0.8–1.5; P = .60). Increasing number of years of service was protective against working with symptoms, achieving statistically significance in multivariable analysis after 16 years. Compared to those having worked <1 year, the odds ratios of working with symptoms were 0.32 (95% CI, 0.16–0.65; P = .002), 0.33 (95% CI, 0.15–0.74; P = .007), and 0.32 (95% CI, 0.13–0.79; P = .007) for those working 16–20 years, 21–25 years, and ≥26 years, respectively. More than half of HCP who worked with symptoms identified being understaffed (56.9%), having mild symptoms (55.3%), and sense of responsibility (55.1%) as reasons to work with respiratory symptoms. The following barriers, or reasons to work with symptoms, were more commonly identified as significant by those who worked with symptoms compared to those who did not: being understaffed (OR, 1.87; 95% CI, 1.35–2.58; P ≤ .001), having mild symptoms (OR, 1.96; 95% CI, 1.42–2.71; P < .001), and lack of support from management (OR, 1.84; 95% CI, 1.07–3.18; P = .03). Conclusions: Working with respiratory symptoms is prevalent in clinical and nonclinical HCP. Those with fewer years of work experience appear to be more susceptible to misconceptions and pressures to work despite respiratory symptoms. Messaging should stress support from leadership and the significance of even mild respiratory symptoms and should emphasize responsibility to patients and colleagues to stay home with respiratory symptoms. Strategies to ensure adequate staffing and sick leave may also be high yield.
Disclosures: None
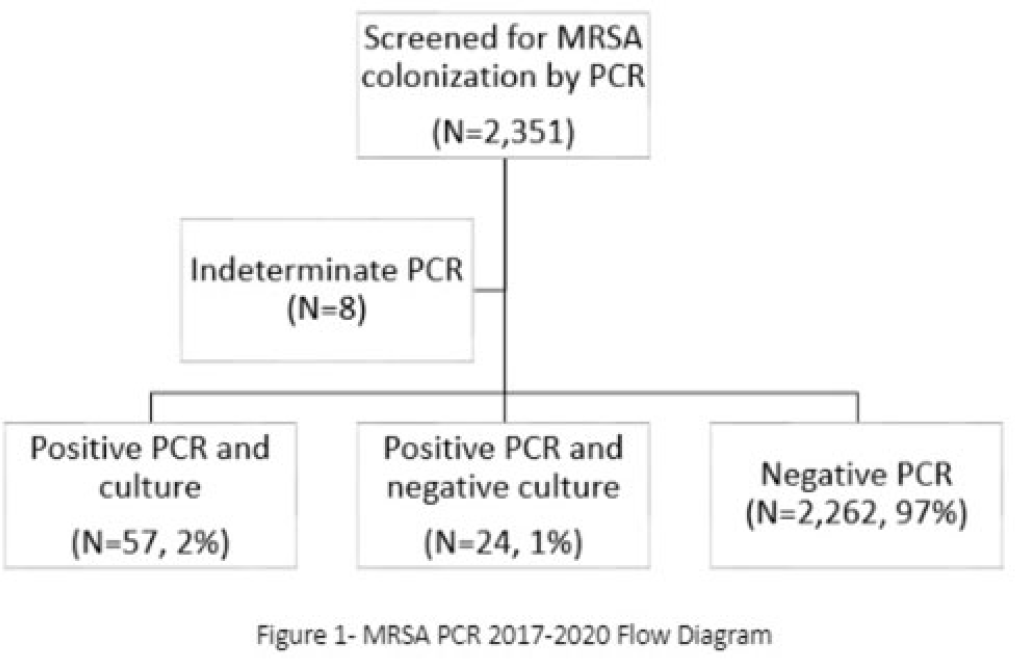
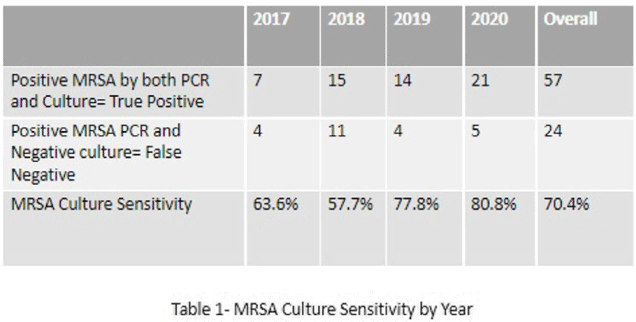
Background: Neonates colonized with methicillin-resistant Staphylococcus aureus (MRSA) are at high risk of developing life-threatening MRSA infection. Due to lack of evidence, national guidelines do not currently recommend a specific methodology for detecting MRSA colonization. We hypothesize that surveillance for MRSA colonization via polymerase chain reaction (PCR) is superior to culture for the detection of colonization. Methods: In this retrospective study, we compared results of MRSA surveillance by 2 methodologies, culture and PCR, after implementation of an MRSA surveillance and decolonization protocol in the Texas Children’s Hospital Pavilion for Women, a 42-bed neonatal intensive care unit. MRSA colonization of 3 body sites via the 2 methodologies was assessed from June 2017 through December 2020. All neonates were screened for MRSA upon admission to the NICU and weekly thereafter until MRSA-positive or discharged. Swab specimens were initially tested by PCR (Xpert MRSA NxG, Cepheid) and when MRSA-positive reflexed to culture to recover the organism for further characterization. This study was approved through the Baylor College of Medicine Institutional Review Board. Results: During the study period, 2,351 neonates were assessed for MRSA colonization by PCR; 81 (3.4%) infants were PCR positive (Fig. 1). Of those 81, 57 (70.4%) had concordant MRSA PCR and culture results, and 24 (29.6%) were MRSA PCR positive but no isolate was recovered in culture. Also, 8 specimens were indeterminate by PCR. However, 1 infant who was negative by culture but was PCR positive developed an MRSA orbital infection. Compared to PCR, the overall sensitivity of MRSA culture was 70.4% (range, 57.7%–80.8%, depending on the year) (Table 1). Conclusions: PCR is more sensitive than culture for detecting MRSA colonization in neonates. Utilizing a PCR method enhances the ability to identify MRSA colonized infants more readily and allows for prompt initiation of infection control interventions including isolation precautions and decolonization strategies. Reflex to culture remains important for strain characterization during outbreak investigations and for additional susceptibility testing. Resource utilization and cost–benefit analyses should be done in future studies to influence changes in national guidelines for the control of Staphylococcus aureus colonization and infection in neonatal intensive care units.
Disclosures: None
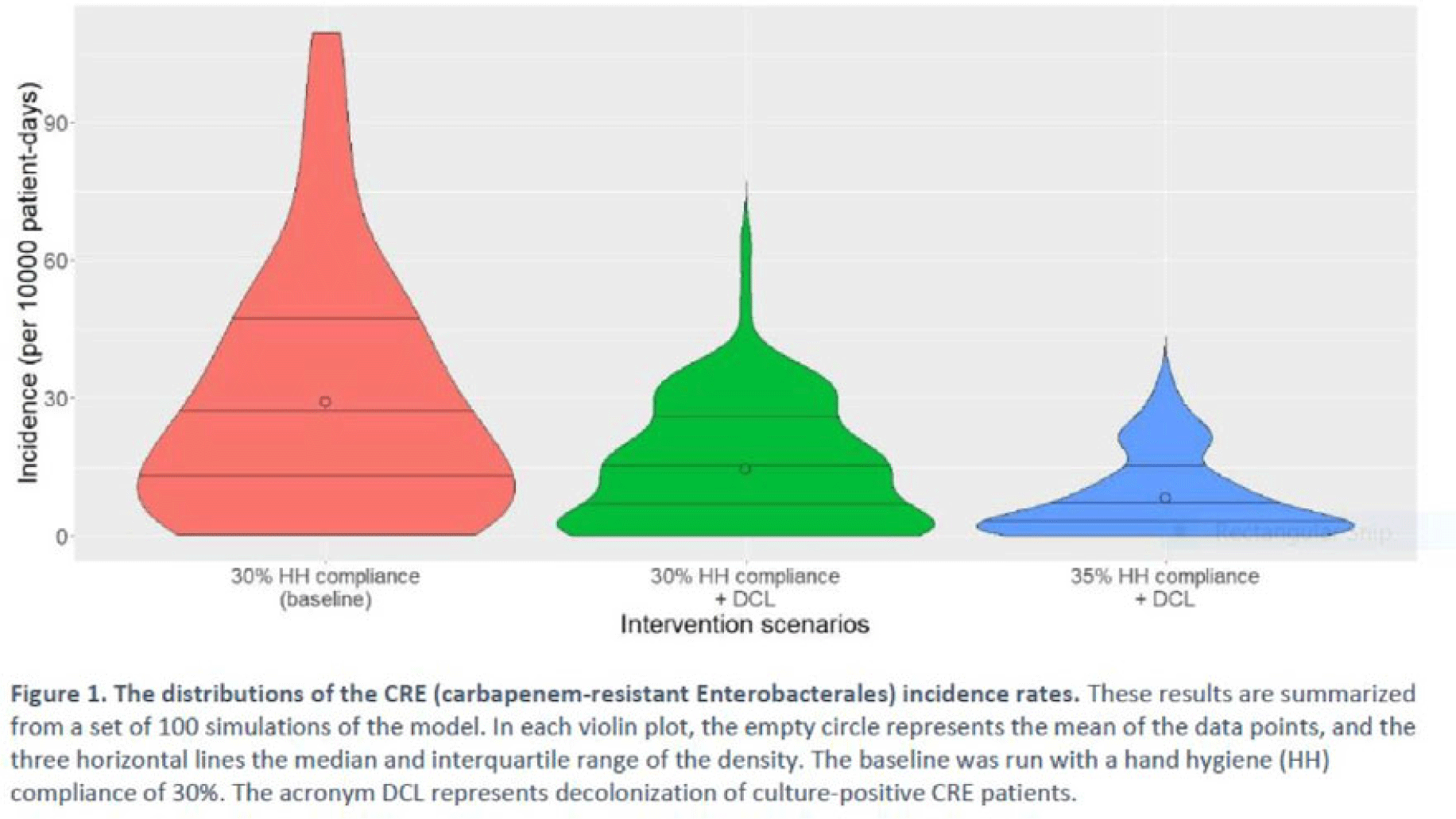
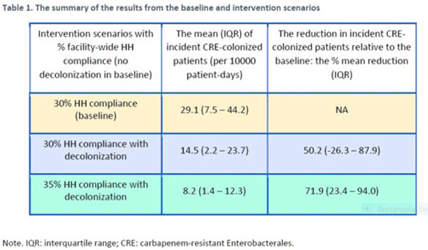
Background: Multimodal approaches are often used to prevent transmission of antimicrobial-resistant pathogens among patients in healthcare settings; understanding the effect of individual interventions is challenging. We designed a model to compare the effectiveness of hand hygiene (HH) with or without decolonization in reducing patient colonization with carbapenem-resistant Enterobacterales (CRE). Methods: We developed an agent-based model to represent transmission of CRE in an acute-care hospital comprising 3 general wards and 2 ICUs, each with 20 single-occupancy rooms, located in a community of 85,000 people. The model accounted for the movement of healthcare personnel (HCP), including their visits to patients. CRE dynamics were modeled using a susceptible–infectious–susceptible framework with transmission occurring via HCP–patient contacts. The mean time to clearance of CRE colonization without intervention was 387 days (Zimmerman et al, 2013). Our baseline included a facility-level HH compliance of 30%, with an assumed efficacy of 50%. Contact precautions were employed for patients with CRE-positive cultures with assumed adherence and efficacy of 80% and 50%, respectively. Intervention scenarios included decolonization of culture-positive CRE patients, with a mean time to decolonization of 3 days. We considered 2 hypothetical intervention scenarios: (A) decolonization of patients with the baseline HH compliance and (B) decolonization with a slightly improved HH compliance of 35%. The hospital-level CRE incidence rate was used to compare the results from these intervention scenarios. Results: CRE incidence rates were lower in intervention scenarios than the baseline scenario (Fig. 1). The baseline mean incidence rate was 29.1 per 10,000 patient days. For decolonization with the baseline HH, the mean incidence rate decreased to 14.5 per 10,000 patient days, which is a 50.2% decrease relative to the baseline incidence (Table 1). The decolonization scenario with a slightly improved HH compliance of 35% produced a relative reduction of 71.9% relative to the baseline incidence. Conclusions: Our analysis shows that decolonization, combined with modest improvement in HH compliance, could lead to large decreases in pathogen transmission. In turn, this model implies that efforts to identify and improve decolonization strategies for better patient safety in health care may be needed and are worth exploring.
Disclosures: None
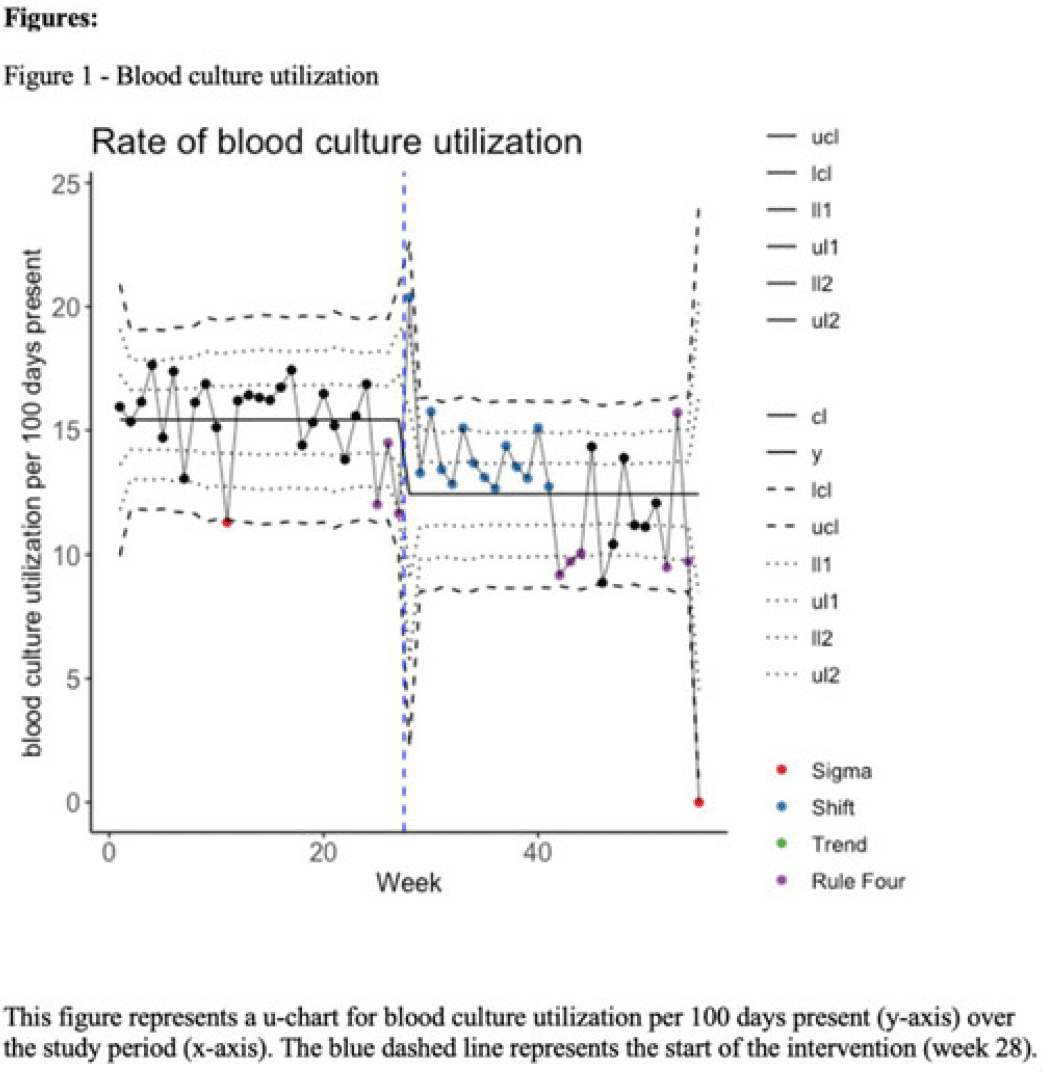
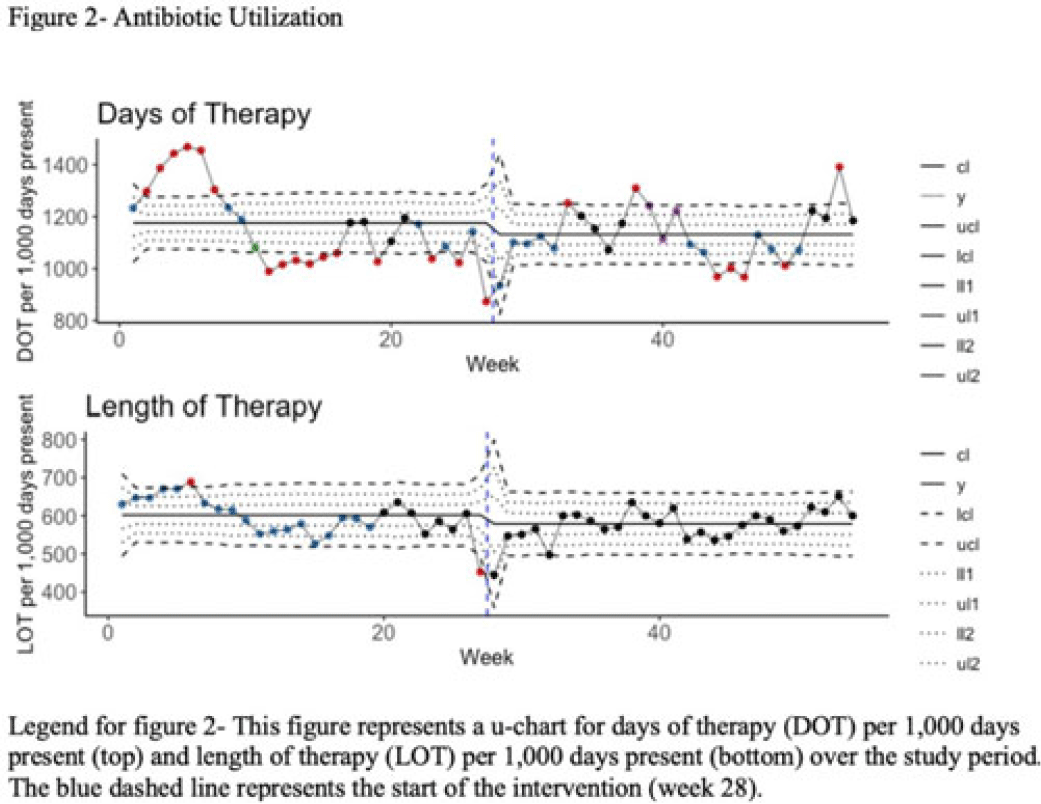
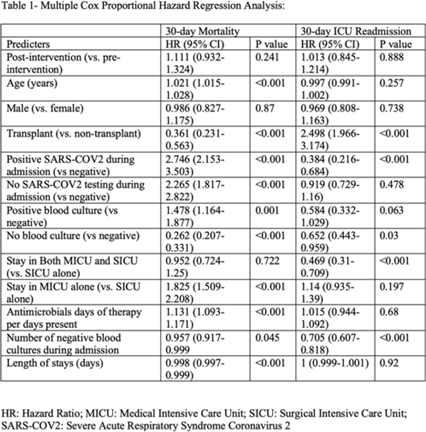
Background: Blood cultures are often ordered when an infection is suspected; however, they have a low yield in most cases. The overuse of blood culture is associated with high contamination rates, resulting in excess diagnostics, unnecessary antibiotics, longer hospital stays, and higher hospital costs. We evaluated the safety of a multifaceted intervention, which encompassed education and blood-culture restriction, and its impact on blood-culture utilization and antibiotic use in adult intensive care unit (ICU) patients. Methods: The study was performed between October 2020 and October 2021 in the 12 general medicine and specialty ICUs of a quaternary academic care center. The intervention, implemented in April 2021, included providing education to ICU and infectious disease physicians based on an algorithm adapted from the Johns Hopkins DISTRIBUTE study in addition to restricting blood-culture ordering on these units to these providers. The month of April 2021 was excluded as a washout period. Study outcomes comprised blood-culture utilization, blood-culture positivity, days of therapy (DOT), and length of therapy (LOT), which were compared across the study periods using IRR or the Pearson χ2 test, as appropriate. In addition, 30-day mortality and 30-day ICU readmission were evaluated utilizing multiple COX regression models. Results: In total, 6,303 patients (2,087 MICU, 3,636 SICU, and 580 both) were included in the study, with a median age of 65 years (IQR, 21). Most participants were male (57.5%), with a median length of stay of 175 hours (IQR, 186). After the intervention, blood-culture utilization rates decreased from 15.4% to 12.4% (IRR 0.80, 95% CI, 0.76–0.85) (Fig. 1). There was no difference in blood-culture positivity between the preintervention period (11.05%) and the postintervention period (11.64%; P = .459). Days of therapy decreased from 1,180 to 1,130 per 1,000 patient days (IRR, 0.96; 95% CI, 0.95–0.98), and the length of therapy decreased from 602 to 579 per 1,000 patient days (IRR, 0.96; 95% CI, 0.94–0.99) (Fig. 2). There was no difference in 30-day mortality (P = .241) nor 30-day ICU readmission (P = .888) across the study periods after adjusting for potential confounders (Table 1). Conclusions: Our multifaceted intervention decreased blood-culture and antimicrobial utilization in the ICUs without significantly affecting the positivity rate, mortality, or readmission. This study suggests that educating providers on appropriate blood-culture use along with restriction could safely improve healthcare outcomes. Further studies are warranted to validate our results across various institutions and to evaluate the impact of blood-culture optimization in non-ICU patients.
Disclosures: None
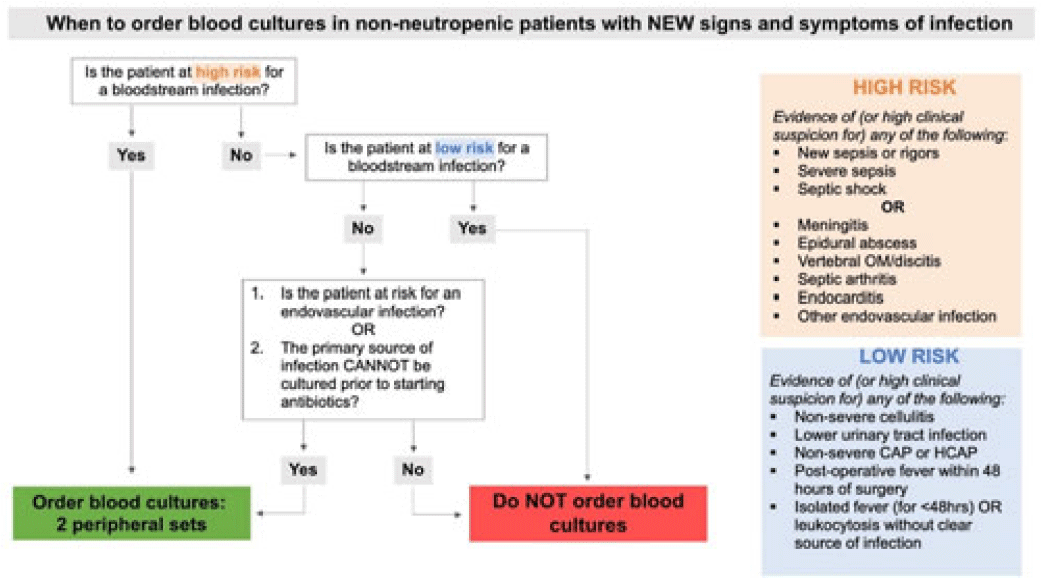
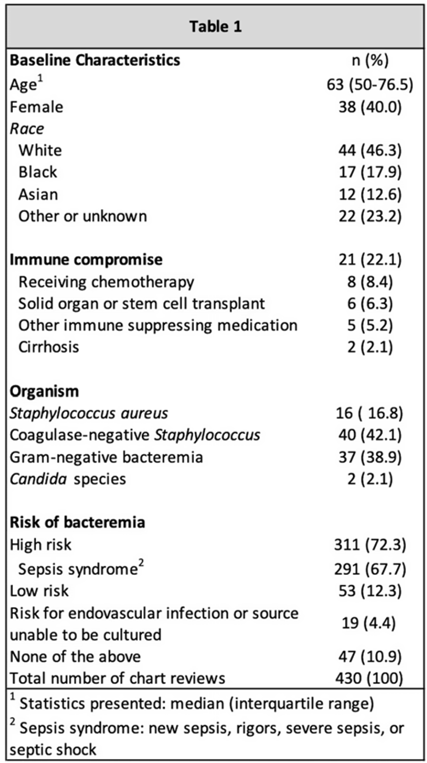
Background: Blood cultures are a fundamental tool in the diagnosis of infections, but they can lead to clinical confusion and waste resources when they yield false results. To optimize blood-culture orders at our institution, we developed an evidence-based clinical guideline (Fig. 1) to be used by frontline providers on nonneutropenic hospitalized adult inpatients. We retrospectively reviewed charts of patients with positive blood cultures to evaluate whether frontline providers and infectious diseases (ID) attending physicians were able to consistently interpret the guidelines to determine whether blood cultures were drawn appropriately. Methods: In total, 95 nonneutropenic adults with an initial positive blood culture collected while on an inpatient unit were identified through a query of the electronic medical record from January 2021 through June 2022. Patients with polymicrobial bacteremia and bacteremia due to Enterococcus, Streptococcus, and gram-positive rods were excluded. Moreover, 4 medical resident physicians reviewed all patients and 2 ID attending physicians reviewed one-quarter of cases; all were blinded to the culture results. Blood cultures were determined to be either appropriately or inappropriately performed based on our institution’s guideline. The free-marginal multirater κ statistics with 95% CIs were calculated to evaluate interrater agreement. Results: Baseline patient demographics are shown in Table 1. Immune compromise without neutropenia was noted in 21 of 95 patients. Most patients were at high risk for bacteremia (72%) per our institutional guideline, most of whom were septic (67.7%). Low risk for bacteremia was found in only 12.3% of reviews. Medical resident physicians, ID attending physicians, and all reviewers combined agreed on whether blood cultures were drawn appropriately or inappropriately (84.2%, 92%, and 86.4% agreement rates, respectively). The free-marginal κ statistic was highest for ID attending physicians (0.84; 95% CI, 0.62–0.78), followed by attending physicians and resident physicians combined (0.73; 95% CI, 0.56–0.90), and resident physicians alone (0.68; 95% CI, 0.58–0.78). In the 21 patients with immune compromise, the agreement rates on blood culture appropriateness remained high among all reviewers, resident physicians, and ID attending physicians were 86.6%, 90.5%, and 95%, respectively. Conclusions: In our retrospective study of nonneutropenic hospitalized adult inpatients, frontline providers and ID attending physicians interpreted blood-culture guidelines consistently, largely agreeing on which patients had cultures drawn appropriately. Agreement among ID attending physicians was excellent and remained substantial among medical resident physicians. Guidelines on the appropriate use of blood cultures are vital to limiting unnecessarily collected cultures, which can lead to extended length of stay and increase cost across hospital systems. Further analyses on the clinical impact of this guideline are ongoing.
Disclosures: None
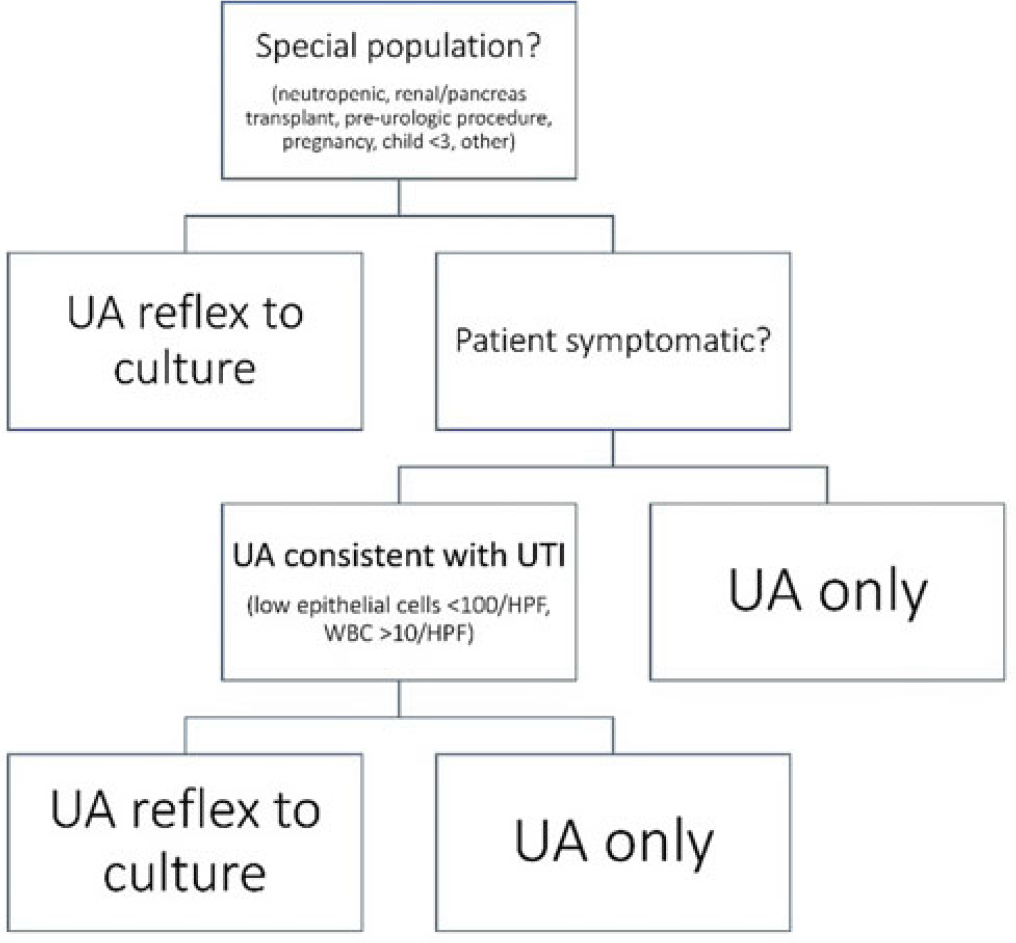
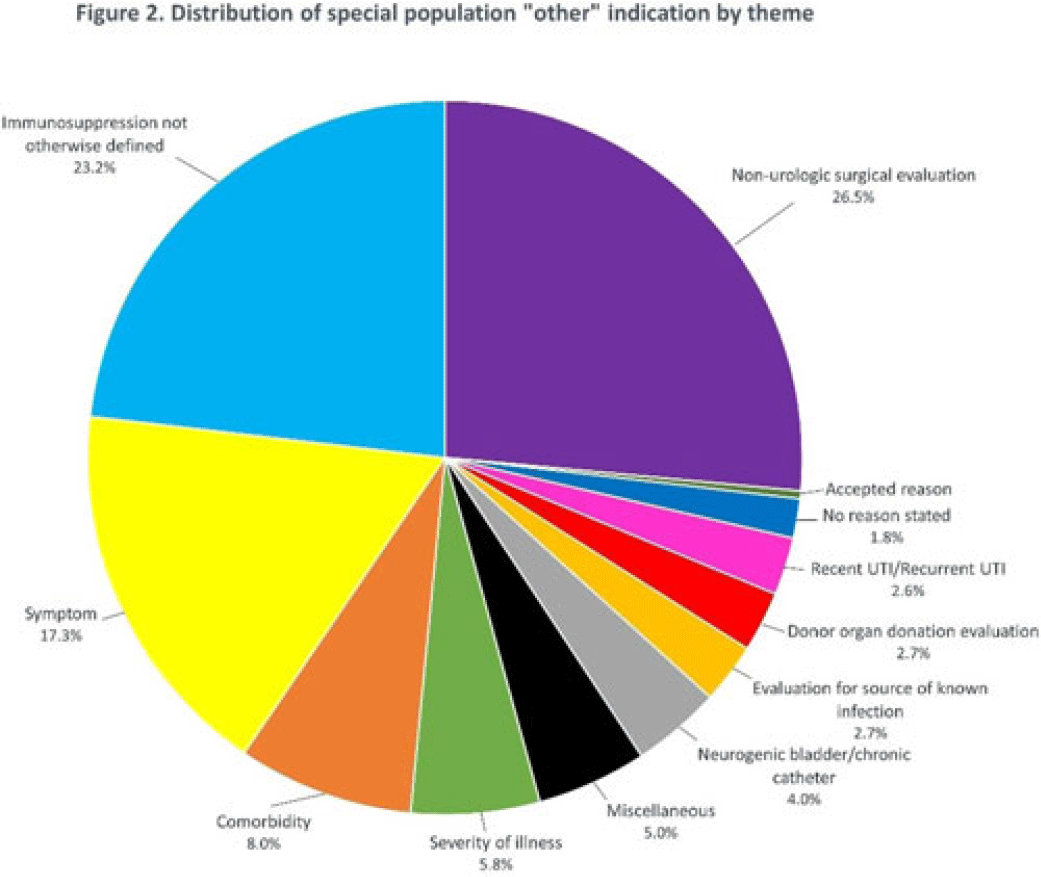
Background: Asymptomatic bacteriuria (ASB) is a widespread problem in hospitalized patients in which only a small subset of patients benefit from treatment. Other patient populations with ASB are harmed by treatment. In 2014, our institution implemented a urinalysis (UA)-driven reflex culture protocol which evaluated patient symptoms, risk factors, and the UA to determine whether bacterial culture was performed (Fig. 1). The goal of this process was to ensure that urine cultures were only performed in those patients who had symptoms of UTI and an abnormal urinalysis while allowing for exceptions in populations where treatment of ASB may be appropriate (ie, pregnancy, aged <3 years, impending urologic surgery, kidney transplant) or where the urinalysis may not be useful in determining whether infection is present (ie, neutropenia). An “other” indication with free-text documentation required was included to allow for unique situations. We evaluated the free-text option to determine whether additional indications were needed and whether data entered were medically appropriate. Methods: This retrospective review at a Midwestern, tertiary-care, academic medical center included inpatient UA with UTI evaluation order sets between July 1, 2020, and June 30, 2022. Descriptive statistics analyzed order-set utilization. Results: In total, 35,469 “urinalysis to reflex culture” order sets were submitted, of which 9,493 resulted in culture. Of these, 839 (8.8%) were ordered with an indication of “other.” “Other” was the most cited indication for special population override contributing to 40% (n = 839 of 2,085) of these indications, followed by kidney or pancreas transplant (29%) and neutropenia (13%). The write-in options fell into 1 of 11 themes (Fig. 2). The 3 most common reasons a urine culture was obtained using the free-text option were nonurologic surgical intervention (n = 223 of 839), immunosuppression not otherwise defined (n = 195 of 839), and symptom presence (n = 146 of 839). Based on current literature, 97% of other indications were inappropriate (n = 816 of 839). If the UTI protocol had been strictly followed, 696 of 839 (83%) cultures ordered with an indication of “other” would not have been obtained, due either to lack of symptoms or, if symptomatic, lack of pyuria. Conclusions: Most cultures obtained by selecting the “other” special population option on the algorithm were obtained in situations in which a urine culture was unnecessary. Removing the “other” indication from the algorithm may improve appropriateness of urine culturing with a possible decrease in CA-UTI and treatment of ASB. Although most write in rationales were inappropriate, adding an additional category for deceased donor-organ evaluation would be reasonable.
Disclosures: None
