This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
Background: Identification of predictors of antibiotic use can inform targeted antimicrobial stewardship initiatives and can account for sources of bias in before-and-after interventional stewardship studies. To date, no study has identified clinical predictors of antimicrobial use within intensive care units (ICUs), where antimicrobial resistance is most prevalent and problematic. Methods: As part of an ongoing prospective, single-arm, pilot feasibility trial of an ICU diagnostic stewardship intervention, we performed a nested retrospective cohort study to explore associations between patient clinical variables and ICUs antimicrobial use and resistance rates (AURs). We included all patients hospitalized in 3 ICUs (surgical, medical, and cardiac) from 2017 to 2021 at Michigan Medicine, a large, tertiary-care, academic medical center. Data were extracted from the electronic medical record using a structured query. Admission-level data were captured, including patient demographics, medical comorbidities, International Classification of Disease, Tenth Revision (ICD-10) admission diagnoses, as well as calendar day-level data including vital signs, clinical and microbiologic laboratory data, measures of acute severity of illness, ventilator–supplemental oxygen metrics, and procedural interventions using current procedural terminology (CPT) codes. ICU AURs were defined as total antibiotic days of therapy per patient per 100 ICU days. Associations between clinical variables and ICU AURs were calculated as rate ratios (RRs). Multiple imputation using fully conditional specification was performed to create 25 imputation data sets. Negative binomial regression models were constructed for each data set using backward selection. Variables retained in >50% of models were included in a final multivariate model. Results: In total, 15,177 ICU patient admissions were captured. Age, sex assigned at birth, and race did not independently associate with ICU AURs. Comorbidities, medical interventions, admission diagnoses, and laboratory data that independently associated with ICU-AURs are shown in Table 1. The clinical variables most strongly associated with increased ICU-AURs were pneumonia (RR, 1.55; 95% CI, 1.451.64), bacteremia (RR, 1.35; 95% CI, 1.25– 1.46), intraabdominal infection (RR, 1.35; 95% CI, 1.18–1.55), SOFA score (RR, 1.27; 95% CI, 1.14–1.42), abnormal WBC (RR, 1.26; 95% CI, 1.20–1.32), and immunocompromised status (RR, 1.20; 95% CI, 1.10–1.31). Clinical variables most strongly associated with decreased ICU-AURs were cardiac ICU (RR, 0.56; 95% CI, 0.52–0.60), COVID-19 (RR, 0.62; 95% CI, 0.56–0.70), and receipt of an invasive nonsurgical procedure (RR, 0.90; 95% CI, 0.82–0.98). Conclusions: In this single-center retrospective cohort study, several clinical variables were independently associated with ICU-AURs. These results may be used to identify patient subgroups for potentially high-yield ICU-based stewardship interventions and to account for sources of bias in before-and-after studies of ICU-based stewardship interventions.

Disclosures: None
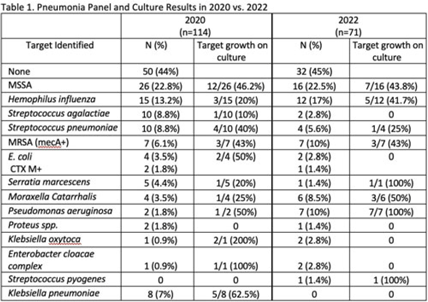
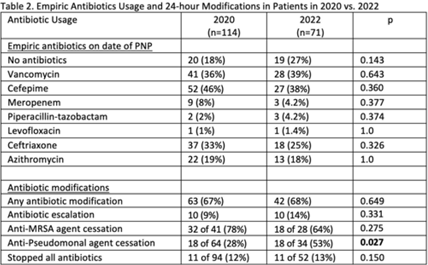
Background: Antibiotics are frequently prescribed in patients with COVID-19 infections to treat secondary bacterial pneumonia. The pneumonia panel (PNP) is a molecular diagnostic tool that rapidly detects 33 bacterial and viral targets. The utility of this panel in COVID-19 patients and how it may direct antibiotic use is unknown. We sought to understand the utilization of PNP in patients with COVID-19 pneumonia over time by comparing clinical parameters, microbiologic results, and antibiotic use between May–December 2020 and January–July 2022. Methods: We implemented the PNP in May 2020 with antimicrobial stewardship guidance, provider education, and order restriction to critical care and infectious disease clinicians. From February–July 2021 prescribers received regular structured antimicrobial stewardship feedback regarding PNP results; from August 2021 to January 2022, no antimicrobial stewardship feedback was provided; from February to July 2022, intermittent feedback was provided. We compared PNP and culture results from sputum or bronchoalveolar lavage samples and antibiotic use and modification within 24 hours of PNP result from patients with confirmed COVID-19 pneumonia between May–December 2020 and January–July 2022. Clinical data and antibiotic use were abstracted through chart review. We excluded patients who died within 72 hours of PNP, those who had concurrent nonpulmonary infections, and those whose COVID-19 test was >30 days prior. Results: We included 114 patients in 2020 and 71 patients in 2022. The overall median age was 61 years, 71% were male, and 66% were mechanically ventilated without statistical differences between the cohorts, including their comorbidities. Acute or worsening hypoxia remained the predominant indication for PNP (77% in 2020 vs 75% in 2022, NS). The median number of days between admission and PNP was 4 (IQR, 1–8) in 2020 versus 3 (IQR, 1–7), and the difference was not significant. PNP and culture results in Table 1 show that Staphylococcus aureus and Hemophilus influenzae were the pathogens most commonly identified. Table 2 describes empiric prescribing and modifications for commonly prescribed antibiotics. Prescribers used empiric cefepime and ceftriaxone more in 2020 and vancomycin more in the 2022 group; however, these were not statistically significant. Cefepime de-escalation was more common in 2022 (53% vs 28%; P = .03). Antibiotic modifications within 24 hours of PNP remained similar in 2020 vs 2022. Although vancomycin cessation was more common in 2020 (78%) versus 2022 (57%), the difference was not statistically significant. Conclusions: With ASP guidance, PNP may be a useful tool to stop or target antibiotics for secondary bacterial pneumonia in COVID-19 pneumonia. Early vancomycin cessation (prior to culture results) may be an enduring consequence of PNP implementation.
Disclosures: None
Background: Most antibiotic use occurs in ambulatory settings. Antibiotic prescribing for children living in the United States in medically underserved areas or in populations is not well understood.
Objective: To characterize antibiotic prescribing for children in a practice-based research network (PBRN).
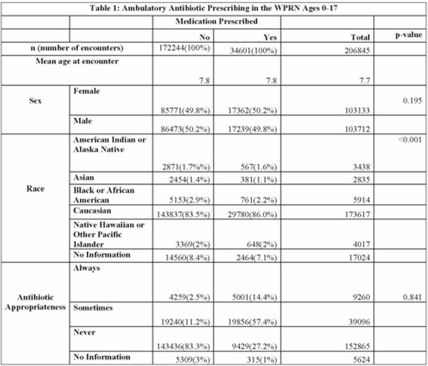
Design and Methods: In this retrospective cohort study, we characterized oral antibiotic prescribing in a large PBRN. Patients aged 0–17 years with at least 1 in-person visit between January 1, 2014, and December 31, 2018, at 1 of 25 primary-care clinics located within the WWAMI (Washington, Wyoming, Alaska, Montana, and Idaho) region of the Practice and Research Network (WPRN) were included. Data were extracted from DataQUEST, a centralized data repository from included primary-care clinics. Encounters for wellness visits or those lacking a diagnosis code and patients with complex chronic conditions were excluded. Diagnoses were categorized using International Classification of Disease, Ninth Revision (ICD-9) and ICD-10 codes. Oral antibiotics prescribed within 3 days of an encounter were associated with that encounter. Demographic data included age, sex, race, and ethnicity. Antibiotic appropriateness was determined using a previously published 3-tiered classification system using diagnosis codes as always, sometimes, or never appropriate. Patient-level data (ZIP codes) were used to designate medically underserved areas (MUAs) and medically underserved populations (MUPs). Antibiotic prescribing was then analyzed within these groups. Results: In total, 37,314 patients across 206,845 encounters were included, of which 34,601 encounters (17%) resulted in antibiotic prescription (Table 1). Of those, appropriateness data were available for 34,286 (99%). Of the antibiotics prescribed, 14% were always appropriate, 57% were sometimes appropriate, and 27% were never appropriate (1% missing). In total, 64% and 35% of encounters occurred with patients from an MUA and MUP, respectively. Conclusions: Targets to improve oral antibiotic prescribing for children in a large PBRN include antibiotic prescribing for diagnoses that never require an antibiotic. Larger comparative studies may focus on the role (if any) that MUA/MUP has on antibiotic prescribing.
Disclosures: None
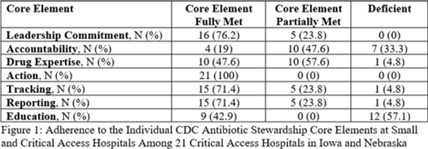
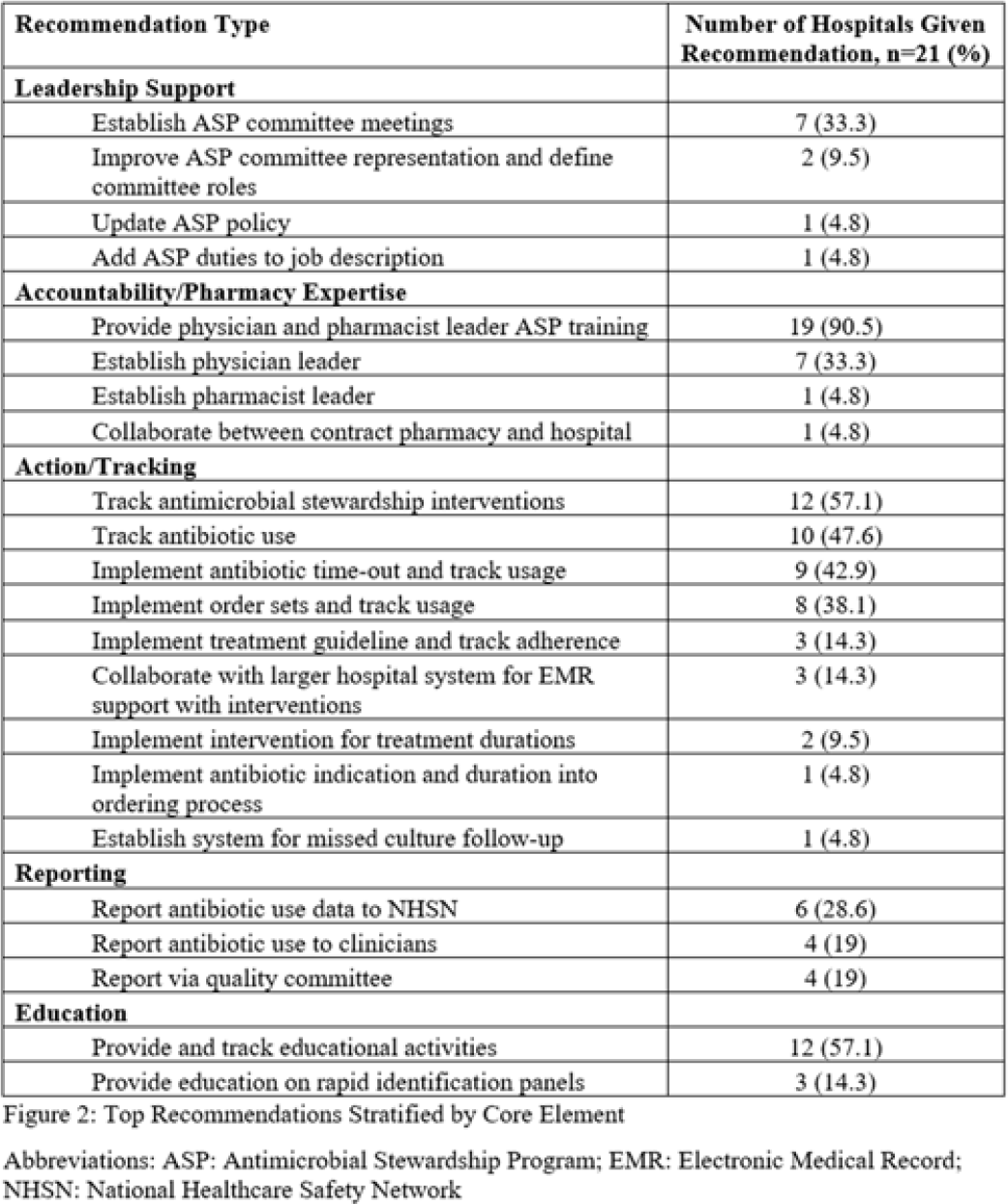
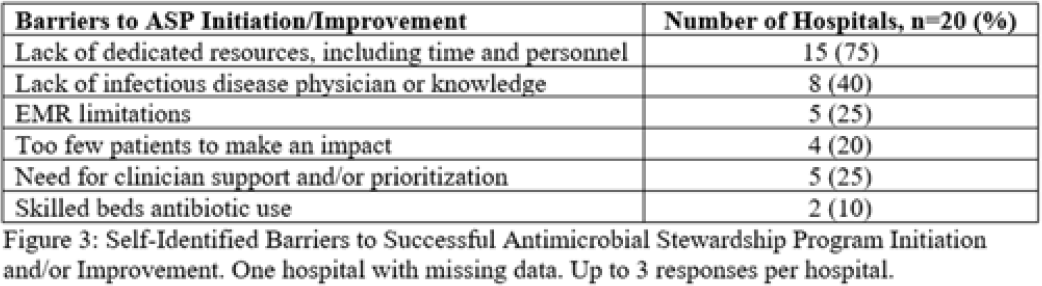
Background: Critical-access hospitals (CAHs) are required to meet the CDC 7 Core Elements of antimicrobial stewardship programs (ASPs). CAHs have lower adherence to the core elements than larger acute-care hospitals, and literature defining which core-element deficiencies exist within CAHs as well as barriers to adherence is lacking. Methods: We evaluated 21 CAH ASPs (5 in Nebraska and 15 in Iowa) that self-identified as potentially deficient in the Core Elements, via self-assessment followed by in-depth interviews with local ASP team members to assess adherence to the CDC Core Elements for ASPs. Core-element compliance was rated as either full (1 point), partial (0.5), or deficient (0), with a maximum score of 7 per ASP. High-priority recommendations to ensure core-element compliance were provided to facilities as written feedback. Self-reported barriers to implementation were thematically categorized. Results: Among the 21 CAH ASPs, none fully met all 7 core elements (range, 2.5–6.5), with a median of 5 full core elements met (Fig. 1). Only 6 ASPs (28.6%) had at least partial adherence to each of the 7 core elements. Action (21 of 21, 100%) and leadership commitment (16 of 21, 76.2%) were the core elements with the highest adherence, and accountability (4 of 21, 19%) and education (9 of 21, 42.9%) were the lowest. The most frequent high-priority recommendations were to provide physician and pharmacist leader ASP training (19 of 21, 90.5%), to track antimicrobial stewardship interventions (12 of 21, 57.1%), and to provide or track educational activities (12 of 21, 57.1%) (Fig. 2). One-third of programs were recommended to establish a physician leader. The most commonly self-identified barriers to establishing and maintaining an ASP were a lack of dedicated resources such as time of personnel (15 of 20, 75%), lack of infectious diseases expertise and training (8 of 20, 40%), and electronic medical record limitations (5 of 20, 25%) (Fig. 3). Conclusions: CAH ASPs demonstrate several critical gaps in achieving adherence to the CDC Core Elements, primarily in training for physician and pharmacist leaders and providing stewardship-focused education. Further resources and training customized to the issues present in CAH ASPs should be developed.
Disclosures: None
