This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
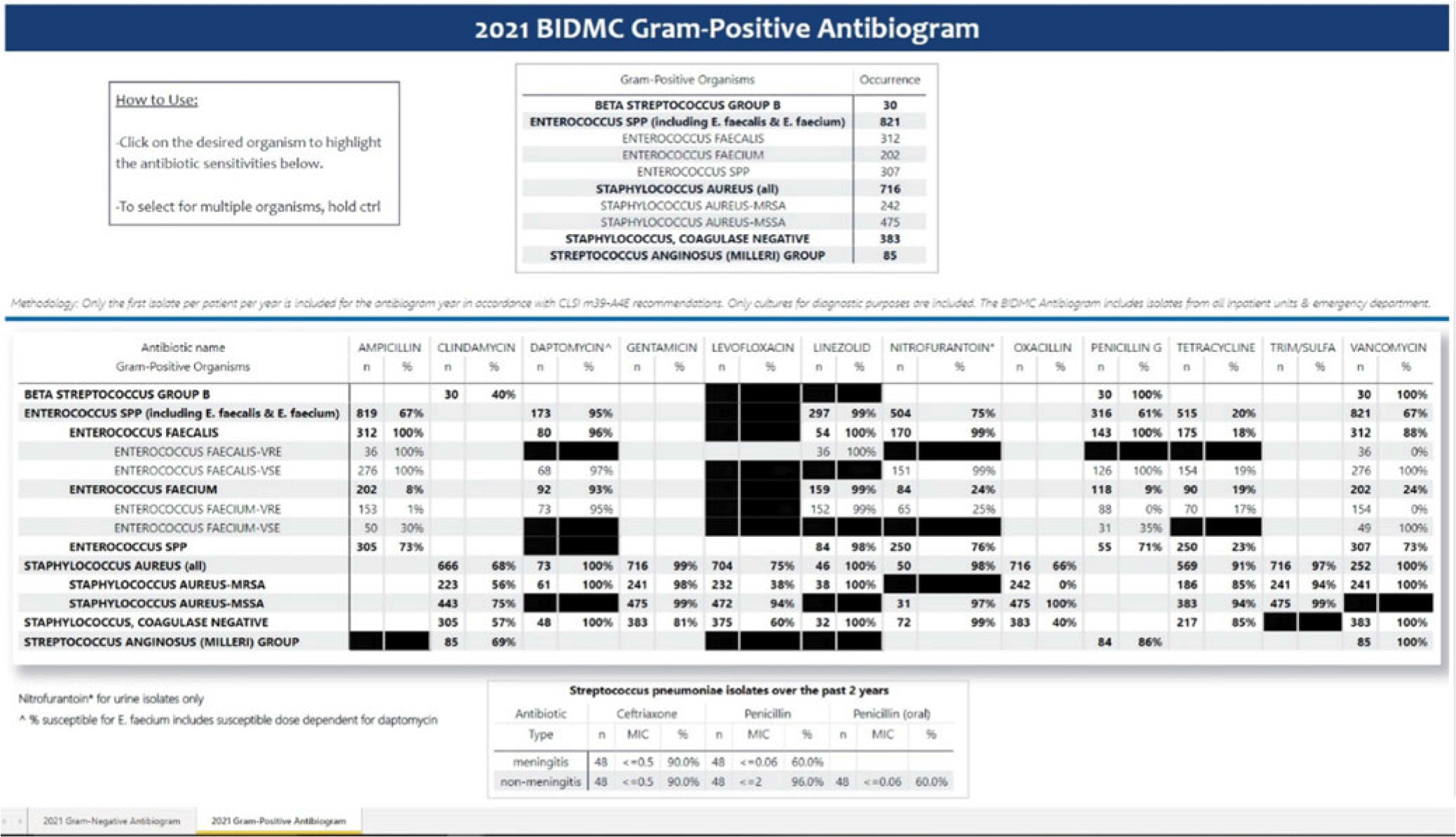
Background: Previously, our hospital manually built a static antibiogram from a surveillance system (VigiLanz) culture report. In 2019, a collaboration between the antimicrobial stewardship team (AST) and the infection control (IC) team set out to leverage data automation to create a dynamic antibiogram. The goal for the antibiogram was the ability to easily distribute and update for hospital staff, with the added ability to perform advanced tracking and surveillance of organism and drug susceptibilities for AST and IC. By having a readily available, accurate, and Clinical and Laboratory Standards Institute (CLSI)–compliant antibiogram, clinicians have the best available data on which to base their empiric antibiotic decisions. Methods: First, assessment of required access to hospital databases and selection of a visualization software (MS Power BI) was performed. Connecting SQL database feeds to Power BI enabled creation of a data model using DAX and M code to comply with the CLSI, generating the first isolate per patient per year. Once a visual antibiogram was created, it was validated against compiled antibiograms using data from the microbiology laboratory middleware (bioMerieux, Observa Integrated Data Management Software). This validation process uncovered some discrepancies between the 2 reference reports due to cascade reporting of susceptibilities. The Observa-derived data were used as the source of truth. The antibiogram prototype was presented to AST/IC members, microbiology laboratory leadership, and other stakeholders to assess functionality. Results: Following feedback and revisions by stakeholders, the new antibiogram was published on a hospital-wide digital platform (Fig. 1). Clinicians may view the antibiogram at any time on desktops from a firewall (or password)–protected intranet. The antibiogram view defaults to the current calendar year and users may interact with the antibiogram rows and columns without disrupting the integrity of the background databases or codes. Each year, simple refreshing of the Power BI antibiogram and changing of the calendar year allows us to easily and accurately update the antibiogram on the hospital-wide digital platform. Conclusions: This interdisciplinary collaboration resulted in a new dynamic, CLSI-compliant antibiogram with improved usability, increased visibility, and straightforward updating. In the future, a mobile version of the antibiogram may further enhance accessibility, bring more useful information to providers, and optimize AST/IC guidelines and education.
Disclosures: None
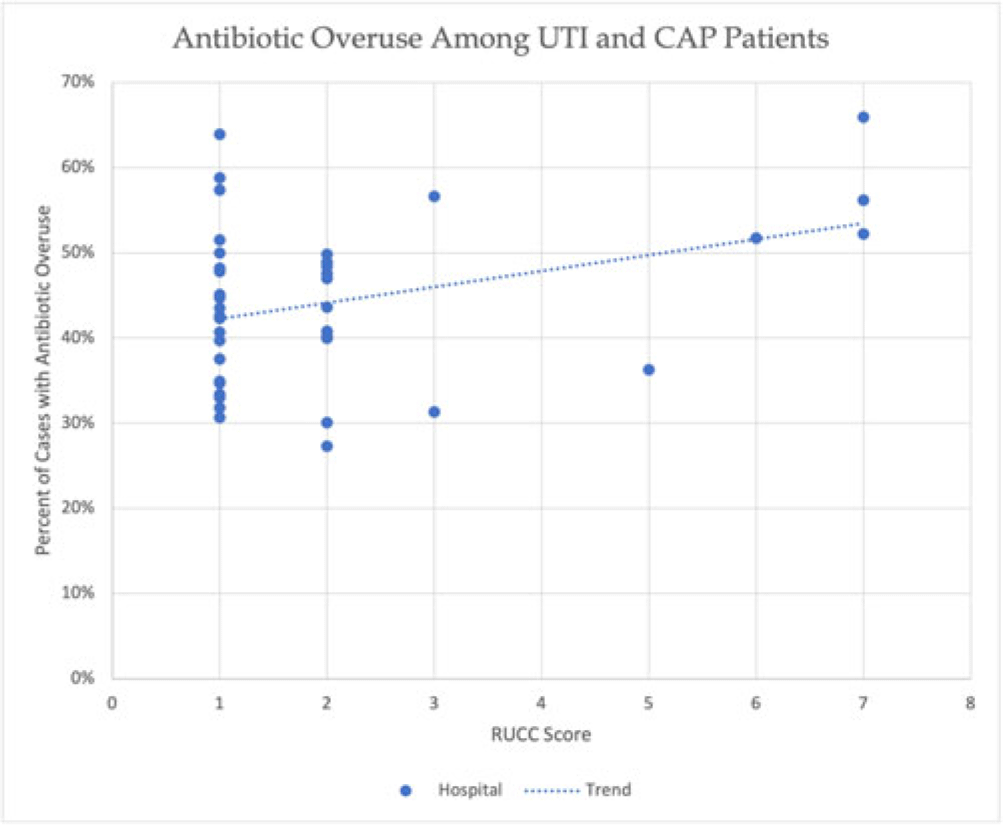
Background: Antibiotic overuse and the resulting patient outcomes span all hospitals. However, although antibiotic stewardship can improve antibiotic use, effective stewardship programs require expertise and an infrastructure that are not present in all hospitals. Rural hospitals have less access to resources, infectious disease expertise, and participation in academic research. Thus, we compared antibiotic overuse at discharge between rural and nonrural hospitals for patients diagnosed with community-associated pneumonia (CAP) or urinary tract infection (UTI)—the 2 most common hospital infections. Methods: To determine whether antibiotic overuse at discharge was higher among rural versus nonrural hospitals, we analyzed data from a 41-hospital prospective cohort of patients treated for CAP or UTI between July 1, 2017, and July 30, 2019, in Michigan. Antibiotic overuse was defined as treatment that was unnecessary (ie, patient did not have an infection), excessive (ie, duration >4 days for CAP), or included suboptimal fluoroquinolone use (ie, safer alternative available). Overuse was determined based on patient risk factors, symptoms, allergies, diagnostic results, and time to stability. Hospital rurality was defined using the Rural–Urban Continuum Codes (RUCC) score. We defined rural as a score ≥4 and very rural as a score of 7–9. We used t tests to compare the mean percentage of patients with antibiotic overuse at discharge between nonrural and rural (and very rural) hospitals. Results: Across 41 hospitals, we included 23,449 patients with CAP or UTI. There were 5 rural (and 3 very rural) hospitals with 2,039 (and 1,082) patients. Antibiotic overuse at discharge was present in 43.1% of patient cases in nonrural hospitals, 52.5% in rural hospitals (P = .04 vs nonrural) and 58.1% in very rural hospitals (P = .007 vs nonrural). Compared to nonrural hospitals, the mean percentage of cases with antibiotic overuse at discharge in rural hospitals was 9.4% higher (15.1% higher in very rural hospitals). Results were similar in a subgroup analysis of only patients with UTI (47.0% in rural vs 37.5% in nonrural, mean difference, 9.5%; P = .03) but were not statistically significant in patients with CAP (53.8% vs 48.0%, respectively; mean difference, 5.8%; P = 0.23). Conclusions: In this retrospective study, rural hospitals—especially very rural hospitals, had higher rates of antibiotic overuse at discharge than nonrural hospitals. Our findings suggest that antibiotic stewardship interventions tailored toward the unique differences in infrastructure, resources, and needs of rural hospitals are essential to community health.
Disclosures: None
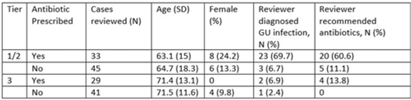
Background: Diagnosis and management of suspected urinary tract infection (UTI) in outpatient settings has been shown to be suboptimal. We previously developed a set of stewardship metrics for UTIs based on electronic health record (EHR) data (Antimicrobial Stewardship & Healthcare Epidemiology 2022;2 suppl 1:S5–S6. doi:10.1017/ash.2022). A tier-based approach was used to more fully capture antibiotic use associated with genitourinary (GU) symptoms and diagnoses. Herein we report a preliminary analysis of validity and reliability of these metrics based on chart abstraction. Methods: The study cohort consisted of patients who visited Veterans Affairs emergency departments or primary care clinics between 2015 and 2022 and who had a GU diagnosis based on International Classification of Disease, Tenth Revision (ICD-10) codes, divided into 3 categories: tier 1 (antibiotics always indicated), tier 2 (antibiotics sometimes indicated), and tier 3 (antibiotics not indicated). Visits related to urological procedures, nontarget settings, or concomitant non-GU infections were excluded. Cases were randomly sampled for manual review from within 8 strata based on tier, use of antibiotics, and visit type. An infectious disease physician and pharmacist abstracted charts using a standardized data-collection instrument. Clinical judgments regarding diagnosis and treatment were recorded on a Likert scale without knowledge of how the patient was managed. The intraclass correlation coefficient (ICC) was used to estimate interrater reliability. Results: To date, 148 cases have been reviewed (50 by both reviewers). Mean (SD) age was 67.5 (15.3) years and 12.2% were female. In a majority of tier 1 and 2 visits in which antibiotics were given, the reviewers found evidence for GU infection (69.7%) and favored prescribing of antibiotics (60.6%) (Table). In contrast, most patients in the tier 3 category who received antibiotics were judged to have noninfectious conditions (eg, benign prostatic hypertrophy) and to not require antibiotics. In the subset of records examined by both reviewers, the interrater reliability of judgments of whether antibiotics were warranted was good (ICC = .704). Conclusions: This preliminary validation provides support for a tier-based approach for stewardship metrics for GU conditions that relies upon electronic data to identify patients for whom antibiotics are generally not indicated.
Disclosures: None
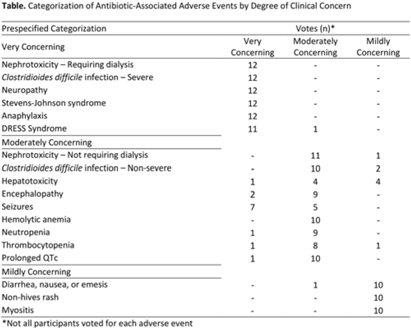
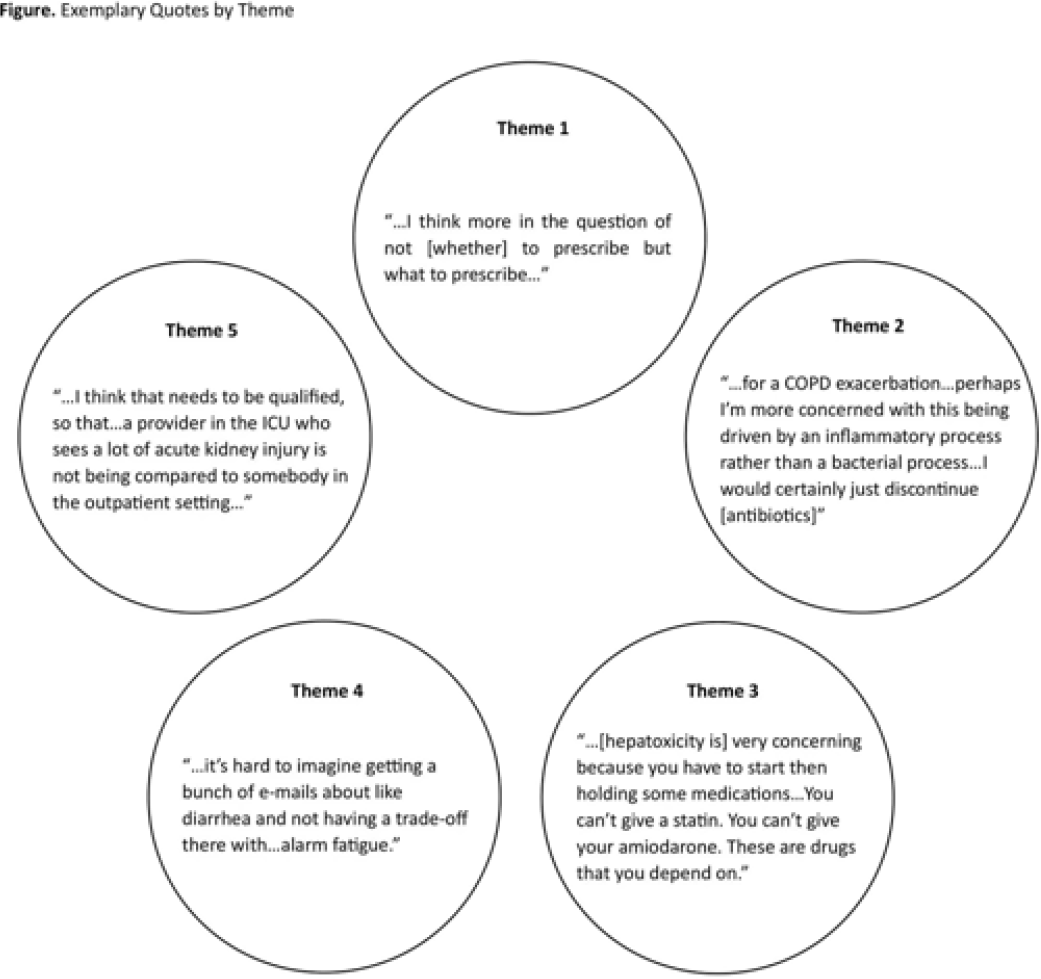
Background: Feedback regarding antibiotic-associated adverse events (ABX-AEs) may assist clinicians with antibiotic decision making. We sought to understand how clinicians account for ABX-AEs when prescribing and their preferences for ABX-AE feedback. Methods: We conducted 1-hour virtual focus groups with 3–5 physicians or advance practice practitioners (APPs) per session at Johns Hopkins Hospital. Participants discussed the role of ABX-AEs in antibiotic decision making and feedback preferences. Participants evaluated prespecified categorization (mildly, moderately, or very concerning) of several ABX-AEs. Focus groups were recorded and transcribed. Transcripts were coded inductively by 2 independent reviewers; discrepancies were resolved by consensus. Codes were used to conduct thematic analysis. Results: Overall, 3 focus groups were conducted with 12 participants: 41.6% were house staff, 16.7% were attending physicians, and 41.6% were APPs. Most were female (91.6%) and were white (41.7%) or Asian (41.7%). Clinicians generally agreed with the prespecified categorizations of ABX-AEs based on degree of clinical concern (Table). We identified 5 themes: (1) The risk of ABX-AE is considered during initial prescribing but influences agent selection more than the decision to prescribe antibiotics. (2) The occurrence of an ABX-AE leads to assessment of need for continued antibiotic therapy. (3) The impact of an ABX-AE on other management decisions is as important as the direct harm of the ABX-AE when assessing severity. (4) Feedback must be curated to prevent clinicians from being overwhelmed with data. (5) Clinicians will be more receptive to feedback regarding ABX-AEs if feedback is contextualized (Fig.). Conclusions: The themes identified and assessment of ABX-AEs of greatest clinical concern may help inform the development of effective ABX-AE feedback methods to improve antibiotic safety.
Disclosures: None
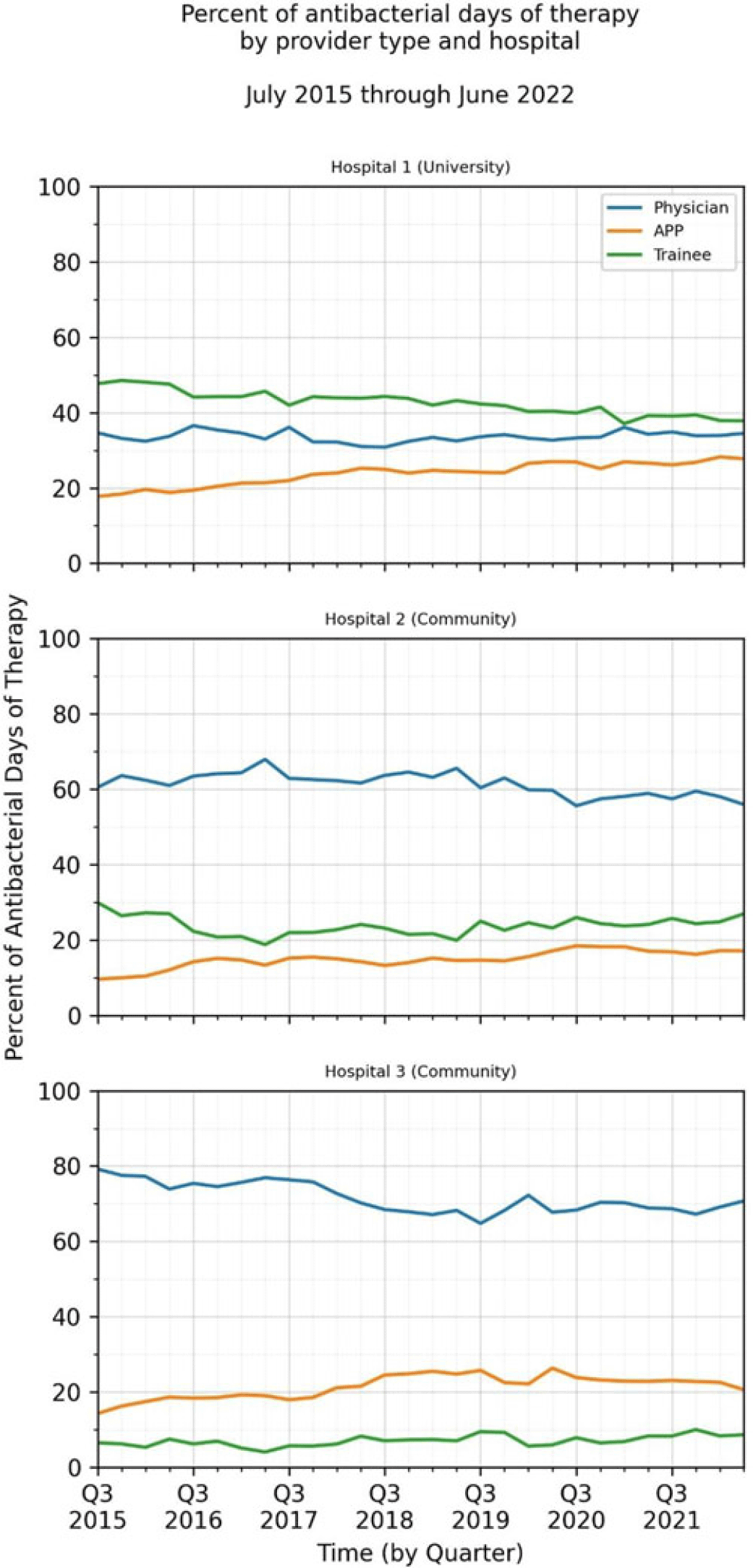
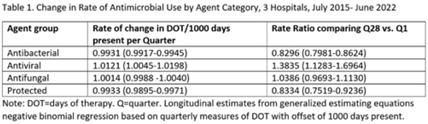
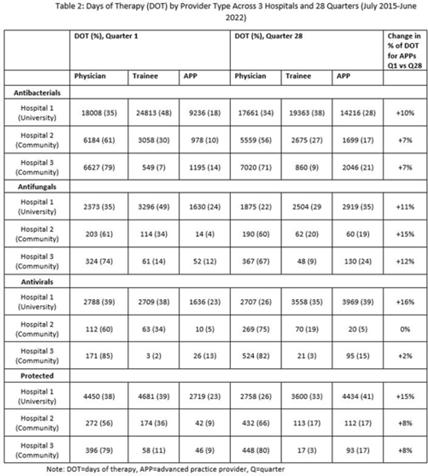
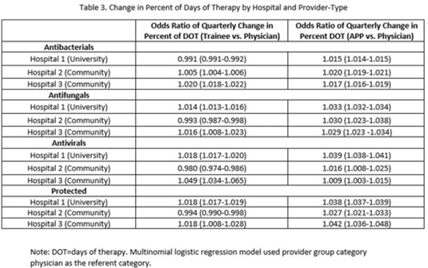
Background: Antimicrobial stewardship strategies must be tailored to effectively engage prescribers with distinct training, experiences, and career paths. Advanced practice providers (APPs) have taken on increasing roles as primary team members in acute-care hospitals, but the impact of this practice shift on antimicrobial prescribing is unknown. We describe longitudinal trends in antimicrobial days of therapy (DOT) by attributed provider type in 3 hospitals. Methods: We performed a retrospective time-series analysis of antimicrobial use for the 7-year period of July 2015–June 2022 to investigate the changes by provider type at 3 hospitals: a major university hospital and 2 community hospitals. DOT, antibacterial, and antifungal agent groups were defined using National Healthcare Safety Network methods. We included anti-influenza and antiherpesvirus agents in the antiviral group. We defined protected agents as those targeted by hospital antimicrobial stewardship program policy (eg, requiring preauthorization). Provider type was defined by electronic health record user profiles in 3 categories: physician, trainees (residents, fellows and medical students), and APPs (nurse practitioners, physician assistants, and nurse anesthetists). We evaluated DOT per 1,000 days present over time by agent group to assess quarterly rate trends. Then, we calculated the percentage of total DOT by provider group. We used multinomial logistic regression to measure changes in percentage DOT across the clinician groups over time using physicians as the referent. Results: Across hospitals and provider groups, we observed an overall decrease in use rates for antibacterial and protected agents (17% each) and increased use rates for antiviral agents (38%) and antifungal agents (4%) (Table 1). Baseline distribution of DOT by provider group and change in distribution over time varied by hospital and agent group (Fig. and Table 2). The largest increases in percentage DOT attributed to APPs compared with physicians occurred in the university hospital with the following average increases per quarter: 1.5% for antibacterials, 3.9% for antivirals, 3.3% for antifungals, and 3.8% for protected agents (Table 3). Community hospitals had higher initial percentage DOT attributed to physicians, but both hospitals experienced increased percentage DOT attributed to APPs. Percentage DOT attributed to trainees varied significantly across agent groups and hospitals. Conclusions: Hospitals had differing baseline patterns of DOT attributed to provider groups, but all experienced increases in DOT attributed to APPs. APPs have increasing involvement in antimicrobial use decisions and should be engaged in future antimicrobial stewardship initiatives.
Disclosures: None
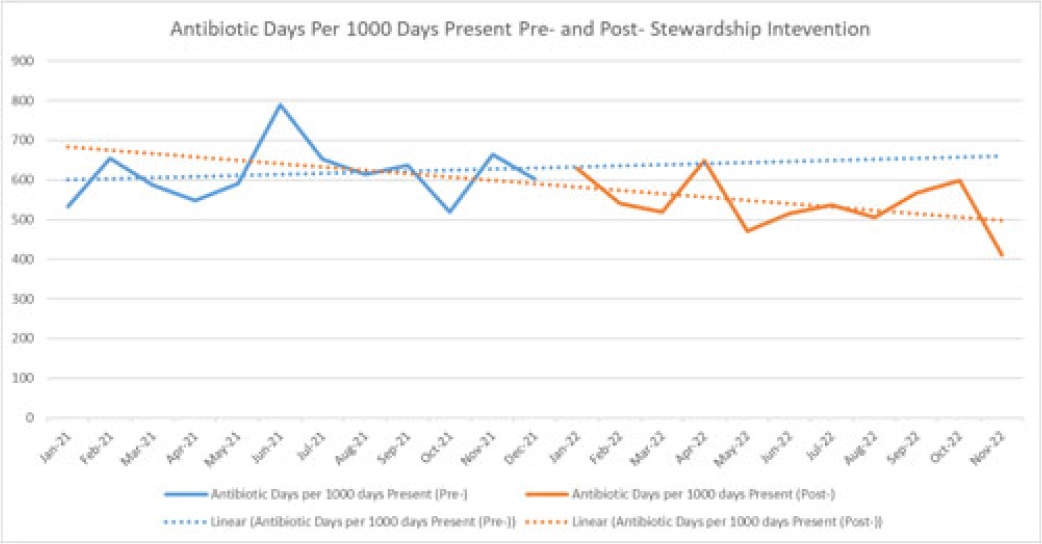
Background: Handshake stewardship is a variation of prospective audit and feedback that entails the individual review of patient charts by a physician–pharmacist collaborative team followed by in-person feedback to primary teams to communicate recommendations regarding optimal antibiotic use. Handshake stewardship has been shown to have durable effects in reducing antimicrobial use in children’s hospitals, but data regarding this intervention in adult hospitals are scarce. In particular, no data are available regarding the impact of this type of stewardship intervention on adult surgical units. We examined the effect of a handshake stewardship intervention at a large academic medical center on adult trauma and acute- and critical-care surgery (ACCS) units. Methods: The antimicrobial stewardship program (ASP) at Barnes-Jewish Hospital launched a handshake stewardship intervention targeting surgical floor teams in January 2022. These teams included the ACCS teams and a number of other surgical services. The intervention consisted of once weekly reviews and in-person rounds with the surgical floor teams along with the establishment of a 7 day per week “hotline” in which the surgical teams could contact an ID physician or pharmacist with questions regarding antibiotic use. Patients with formal ID consultations were not reviewed. Recommendations were tracked including the type, the antibiotic targeted, and recommendation acceptance or rejection. Descriptive statistics were performed to analyze these results. At the end of 12 months, antibiotic use in the floors covered by the ACCS teams were pulled from the NHSN AU module to perform an interrupted time-series analysis 12 months before and after the intervention. Results: Overall, 3,127 charts were reviewed during the intervention period and 637 recommendations were made to all the surgical teams. Opportunities for antibiotic use optimization were identified in ~20% of antibiotic orders. The overall recommendation acceptance rate was 71%. In the ACCS units, 272 interventions were recommended, with an acceptance rate of 67%. The most frequent recommendations were for antibiotic discontinuation (37%), antibiotic de-escalation (17%), shortening duration (12%), and broadening coverage (12%). Antibiotic usage trends (Fig. 1) on the ACCS floors, which were showing a nonsignificant increasing trend (P = .70) before and after the intervention, now show a nonsignificant decreasing trend (P = .20). Conclusions: There are numerous opportunities for antibiotic optimization on adult surgical floors. Although handshake stewardship is a labor-intensive intervention, preliminary findings after 1 year show that, on ACCS units, there may be a trend toward a sustained impact.
Disclosures: None
