This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
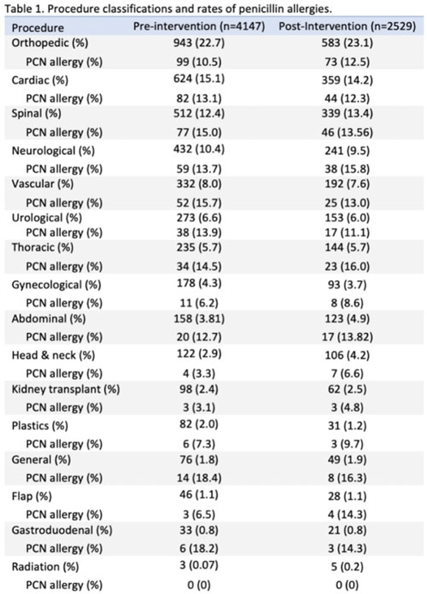
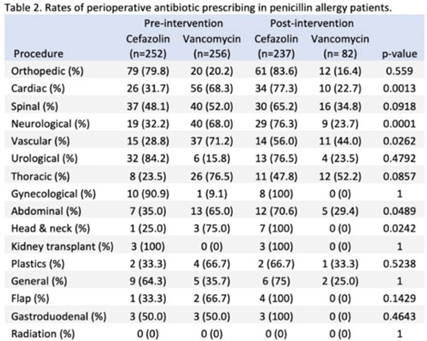
Background: Cefazolin is the preferred antimicrobial for prevention of surgical-site infections in most procedures at our institution. Our first alternative is vancomycin which is associated with higher adverse events and infection rates. The presence of penicillin allergies can influence prescribing of vancomycin despite a low risk of cross-reactivity between penicillin and cephalosporins. Nebraska Medicine implemented a systemwide change in April 2022 that suppressed alerts for non–IgE-mediated penicillin allergies in the electronic medical record (EMR, Epic Systems) upon cephalosporin prescribing. We evaluated changes in perioperative antimicrobial surgical infection prophylaxis after this change. Methods: We conducted a quasi-experimental study of all patients undergoing procedures for which cefazolin is considered preferred per institutional guidance. Preintervention data were from April 1, 2021, to March 31, 2022, and postintervention data included patients from April 11, 2022, to October 31, 2022, after guidance was distributed to surgeons, operating room staff, and pharmacists. Patients were excluded if they were aged <19 years, had a hospital length of stay <24 hours, underwent procedures after their first throughout the time frame, or received both vancomycin and cefazolin. Statistical significance was set at P < .05, determined using the Fisher exact test. Results: The study included 6,676 patients: 4,147 in the preintervention group and 2,529 in the postintervention group. We identified 15 procedure categories, with no significant differences between periods (Table 1). The average age was 61 years. Penicillin allergy was reported in 508 patients (12.3%) in the preintervention group and in 319 patients (12.6%) in the postintervention group. In individuals with penicillin allergy, cefazolin prescribing increased from 49.6% to 74.3% (P < .01) and vancomycin prescribing decreased from 50.4% to 25.7% (P < .01). The largest changes occurred in patients undergoing cardiac, spinal, neurological, and vascular procedures. For patients without penicillin allergy, prescribing remained unchanged. Overall, cefazolin prescribing increased from 92.0% to 95.0% (P < .01), and the rate of vancomycin prescribing decreased from 8.0% to 5.0% (P < .01) in procedures for which cefazolin was preferred. Conclusions: Following the suppression of EMR alerts for non–IgE-mediated allergies when ordering cephalosporins, penicillin prescribing rates of cefazolin for surgical infection prophylaxis improved significantly in procedures for which it was the preferred agent. Further research on infection rates and adverse events with these and other alternative agents are needed.
Disclosures: None
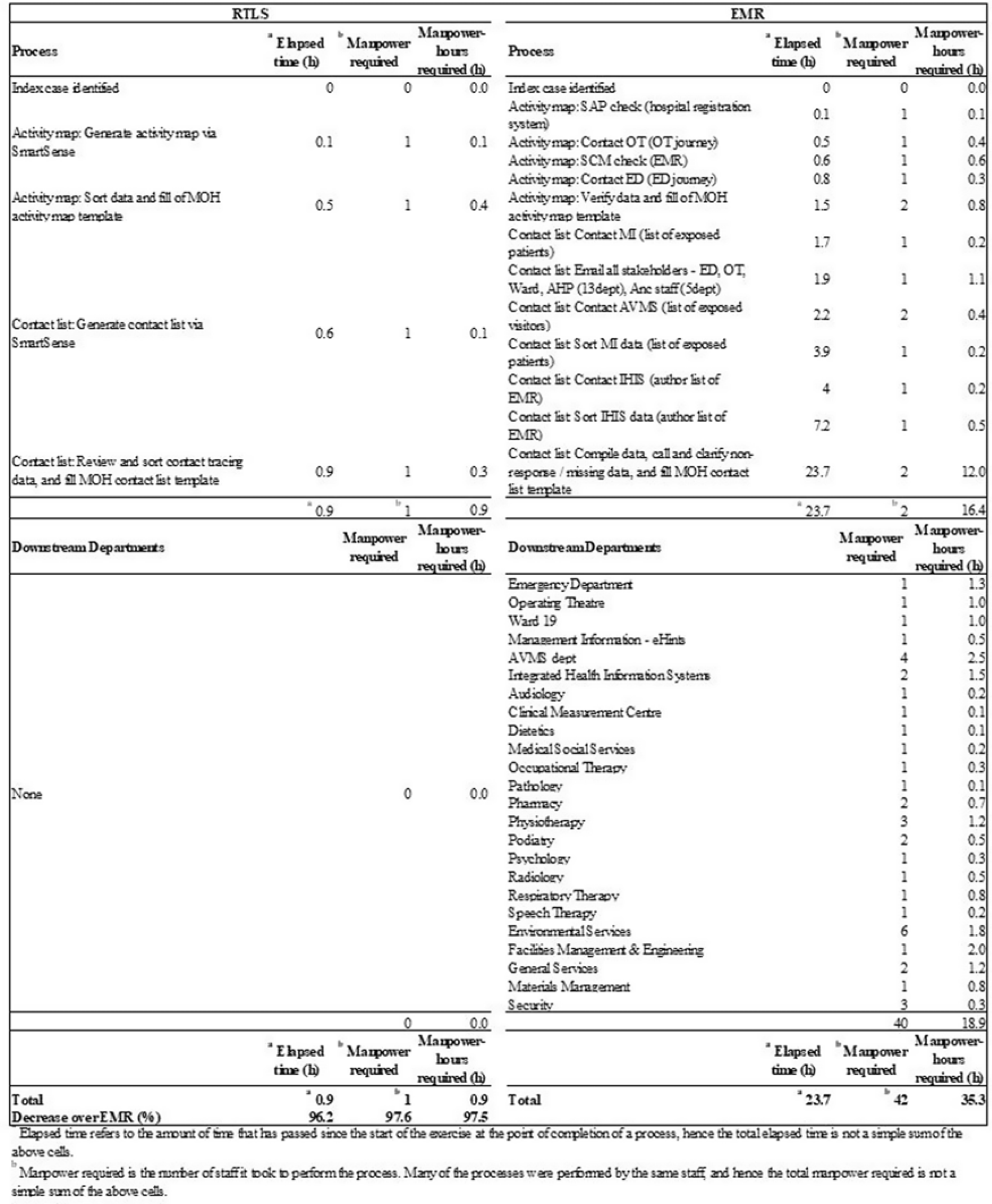
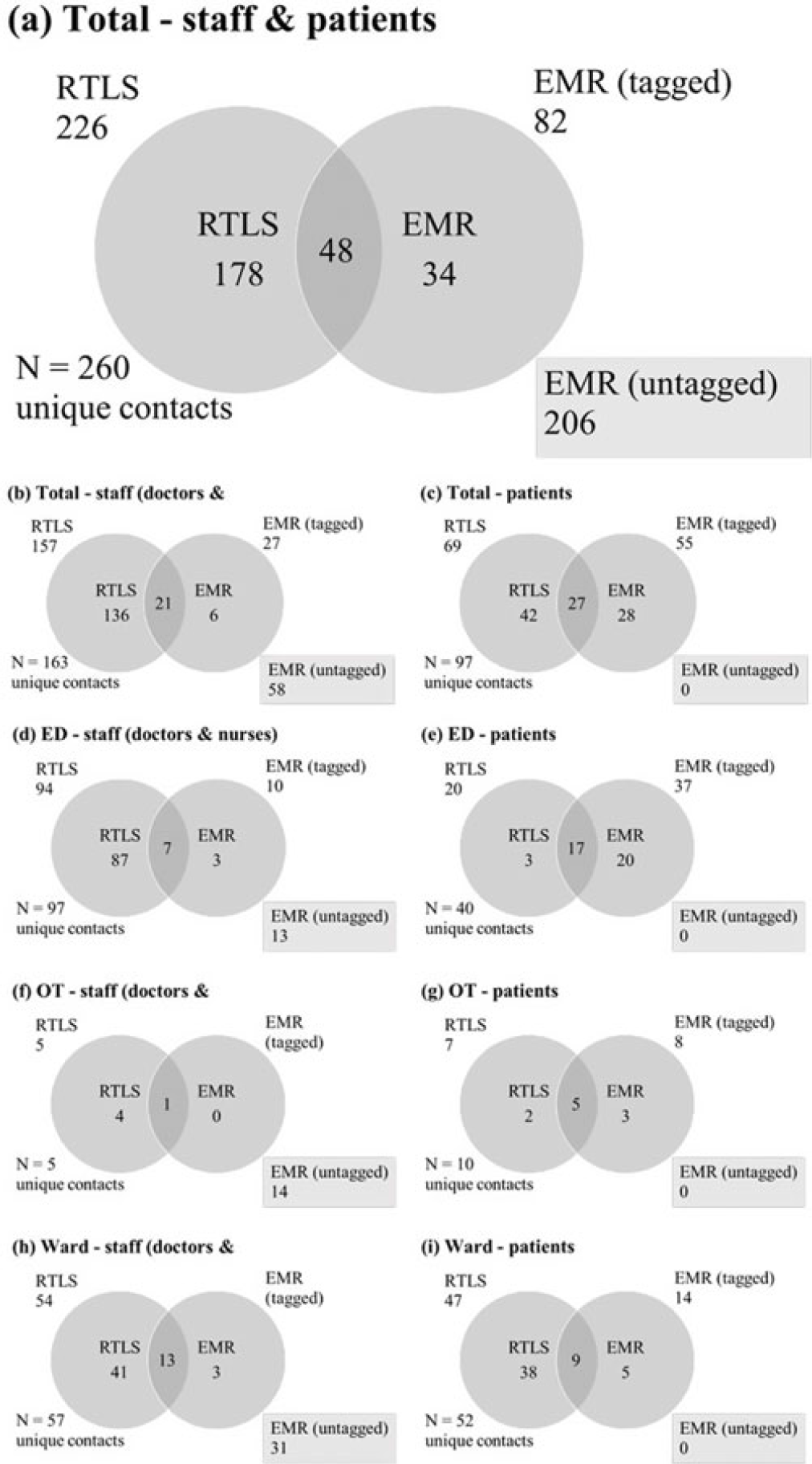
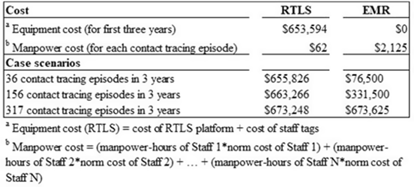
Background: Densely populated metropolitan cities like Singapore are susceptible to emerging infectious disease (EID) outbreaks. Singapore’s pandemic control measures include running biennial simulation exercises for all public hospitals on EID case management, in which a key assessment criterion is contact tracing. Current methods of contact tracing that involve retrospective review of the electronic medical record (EMR) are time-consuming and heavily manpower dependent, and they fail to capture a significant number of contacts. A real-time location system (RLTS) was accurate and effective in contact tracing. We compared the time taken to perform contact tracing and list of contacts identified for RTLS versus EMR, and we compared manpower and manpower hours required to perform contact tracing for RTLS versus EMR. Then we extrapolated the cost incurred by RTLS versus EMR. Methods: A prospective case study was conducted during a simulation exercise to determine and compare the list of contacts, time required, manpower required, and manpower hours required between RTLS and EMR. The costs of both methods were also compared. Results: RTLS identified almost 3 times more contacts than EMR (Fig. 2) with a 96.2% reduction in time taken, a 97.6% reduction in manpower, and a 97.5% reduction in manpower hours (Fig. 1). RTLS incurred significant equipment cost and therefore might require many contact-tracing episodes before providing economic benefit (Fig. 3). However, its speed and accuracy provided during contact tracing will allow the hospital to quickly isolate potentially exposed contacts, reducing the number of infected people during the spread of an infectious disease, particularly one like COVID-19. Conclusions: Albeit costly, RTLS is effective at contact tracing. RTLS has the potential to be the gold standard in contact-tracing methods of the future, particularly considering the current pandemic.
Disclosures: None
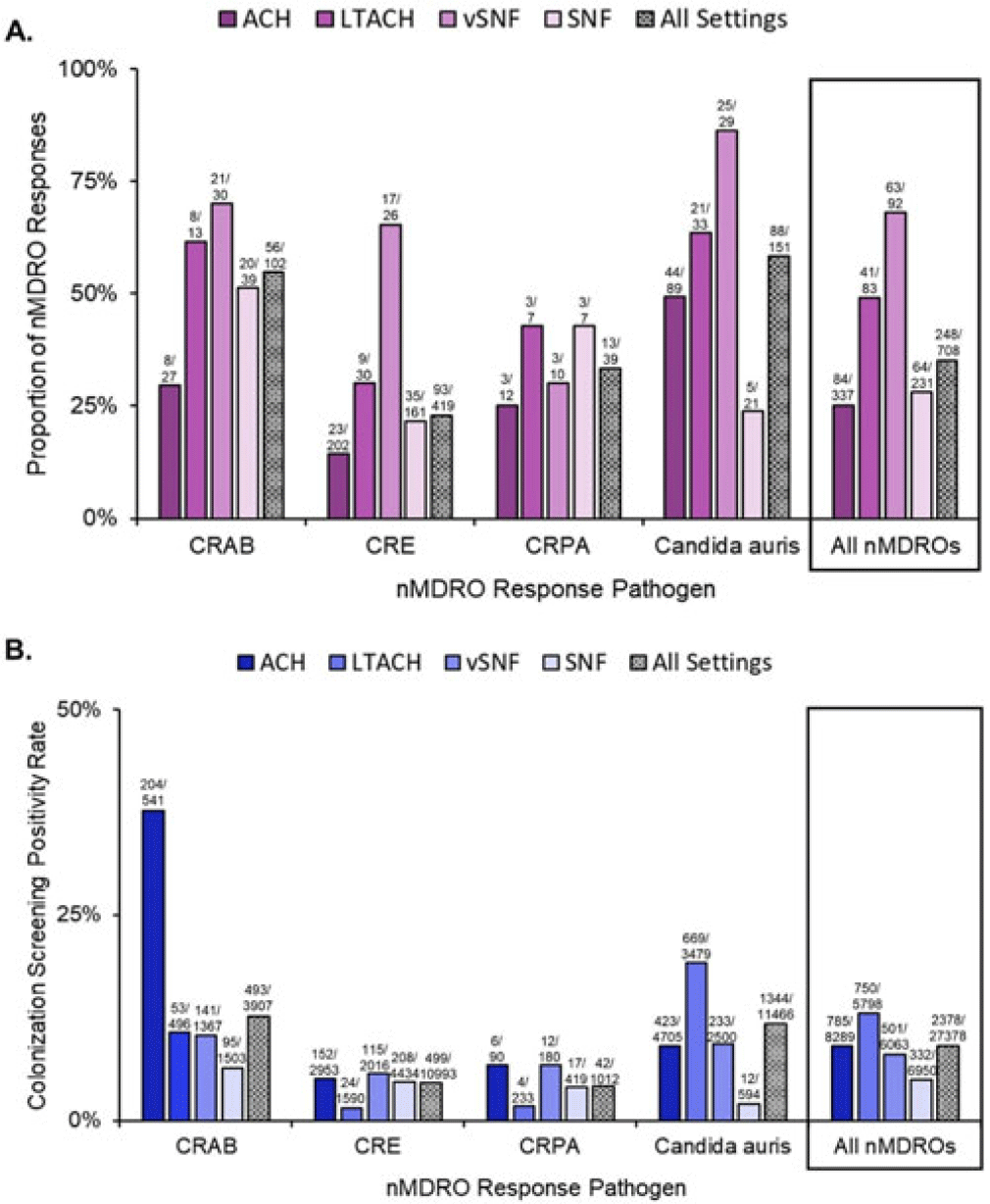
Background: The CDC recommends a public health response when novel and targeted multidrug-resistant organisms (nMDROs), such as carbapenem-resistant organisms or Candida auris, are identified in healthcare settings in nonendemic areas. nMDRO responses are supported by healthcare-associated infection-antimicrobial resistance programs in 50 state and 6 local and territorial health departments. Annually, health departments report nMDRO responses to the CDC. We summarize nMDRO responses nationally and report our assessment of colonization screening positivity rates by healthcare setting and pathogen. Methods: We analyzed nMDRO response data reported by health departments for the period August 2019–July 2021; we excluded prevention efforts (ie, widespread screening based on facility-level risk factors). Among nMDRO responses in which colonization screening was performed, we calculated the proportion of responses in which screening detected additional cases of the index nMDRO and the colonization screening positivity, by healthcare setting and pathogen. Results: Among 2,051 nMDRO responses, 732 (36%) had ≥1 colonization screening (representing 44,845 colonization screenings), of which 24 (representing 17,467 colonization screenings) were prevention efforts and were excluded. Among the remaining 708 nMDRO responses, the healthcare setting most frequently included was acute-care hospitals (ACHs; 337 of 708, 48%); the least frequently included was long-term ACHs (LTACHs; 83 of 708, 12%). Carbapenem-resistant Enterobacterales were the most common index nMDRO prompting a response (408 of 708, 58%). Screening identified additional cases of the index nMDRO in 248 responses (35%) and 2,378 (9%) of 27,378 colonization screenings. Identification of the index nMDRO varied by pathogen and setting (Fig. 1). Overall, ventilator-capable skilled nursing facilities (vSNFs) were the facility type in which colonization screening most frequently identified additional cases of the index nMDRO (63 of 92 responses, 63%), and LTACHs had the highest colonization screening positivity (750 of 5,798, 13%). Similar colonization screening positivity was observed in ACHs (9%) and vSNFs (8%). On average, Candida auris and carbapenem-resistant Acinetobacter baumannii (CRAB) had the highest colonization screening positivity rates across all healthcare settings: CRAB, 493 (12.6%) of 3,907 screened; Candida auris, 1,344 (11.7%) of 11,466 screened (Fig. 1B). More than one-half of responses identified ≥1 case of the index nMDRO. Conclusions: During public health nMDRO responses, additional cases were regularly identified through colonization screening. Responses in vSNFs and LTACHs and to environmental pathogens like Candida auris and CRAB detected additional cases in more than one-half of responses, suggesting that spread commonly occurred prior to detection of the first clinical case. The use of colonization screening is an effective strategy to detect unidentified nMDRO colonization, especially in high-acuity postacute-care settings.
Disclosures: None
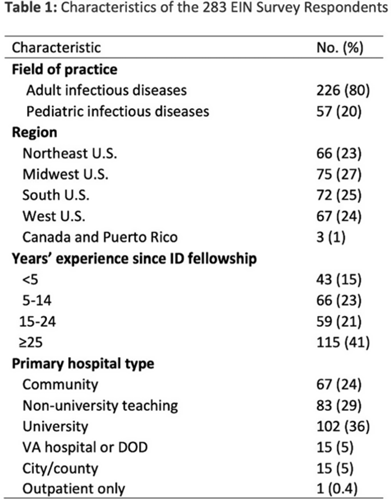
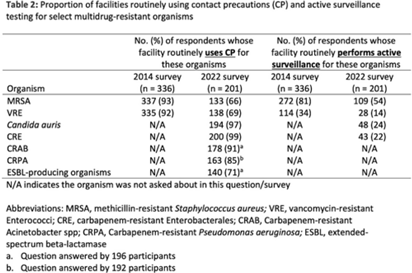
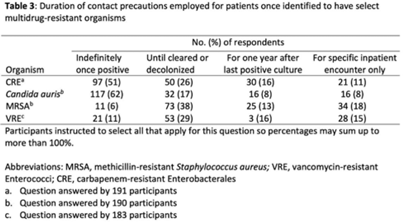
Background: The CDC recommends routine use of contact precautions for patients infected or colonized with multidrug-resistant organisms (MDROs). There is variability in implementation of and adherence to this recommendation, which we hypothesized may have been exacerbated by the COVID-19 pandemic. Methods: In September 2022, we emailed an 8-question survey to Emerging Infections Network (EIN) physician members with infection prevention and hospital epidemiology responsibilities. The survey asked about the respondent’s primary hospital’s recommendations on transmission-based precautions, adjunctive measures to reduce MDRO transmission, and changes that occurred during the COVID-19 pandemic. We sent 2 reminder emails over a 1-month period. We used descriptive statistics to summarize the data and to compare results to a similar EIN survey (n = 336) administered in 2014 (Russell D, et al. doi:10.1017/ice.2015.246). Results: Of 708 EIN members, 283 (40%) responded to the survey, and 201 were involved in infection prevention. Most respondents were adult infectious diseases physicians (n = 228, 80%) with at least 15 years of experience (n = 174, 63%). Respondents were well distributed among community, academic, and nonuniversity teaching facilities (Table 1). Most respondents reported that their facility routinely used CP for methicillin-resistant Staphylococcus aureus (MRSA, 66%) and vancomycin-resistant Enterococcus (VRE, 69%), compared to 93% and 92% respectively, in the 2014 survey. Nearly all (>90%) reported using contact precautions for Candida auris, carbapenem-resistant Enterobacterales (CRE), and carbapenem-resistant Acinetobacter spp, but there was variability in the use of contact precautions for carbapenem-resistant Pseudomonas aeruginosa and extended-spectrum β-lactamase–producing gram-negative organisms. In 2014, 81% reported that their hospital performed active surveillance testing for MRSA, and in 2022 this rate fell to 54% (Table 2). The duration of contact precautions varied by MDRO (Table 3). Compared to 2014, in 2022 facilities were less likely to use contact precautions indefinitely for MRSA (18% vs 6%) and VRE (31% vs 11%). Also, 180 facilities (90%) performed chlorhexidine bathing in at least some inpatients and 106 facilities (53%) used ultraviolet light or hydrogen peroxide vapor disinfection at discharge in some rooms. Furthermore, 89 facilities (44%) reported institutional changes to contact precautions policies after the start of the COVID-19 pandemic that remain in place. Conclusions: Use of contact precautions for patients with MDROs is heterogenous, and policies vary based on the organism. Although most hospitals still routinely use contact precautions for MRSA and VRE, this practice has declined substantially since 2014. Changes in contact-precaution policies may have been influenced by the COVID-19 pandemic, and more specifically, contemporary public health guidance is needed to define who requires contact precautions and for what duration.
Disclosures: None
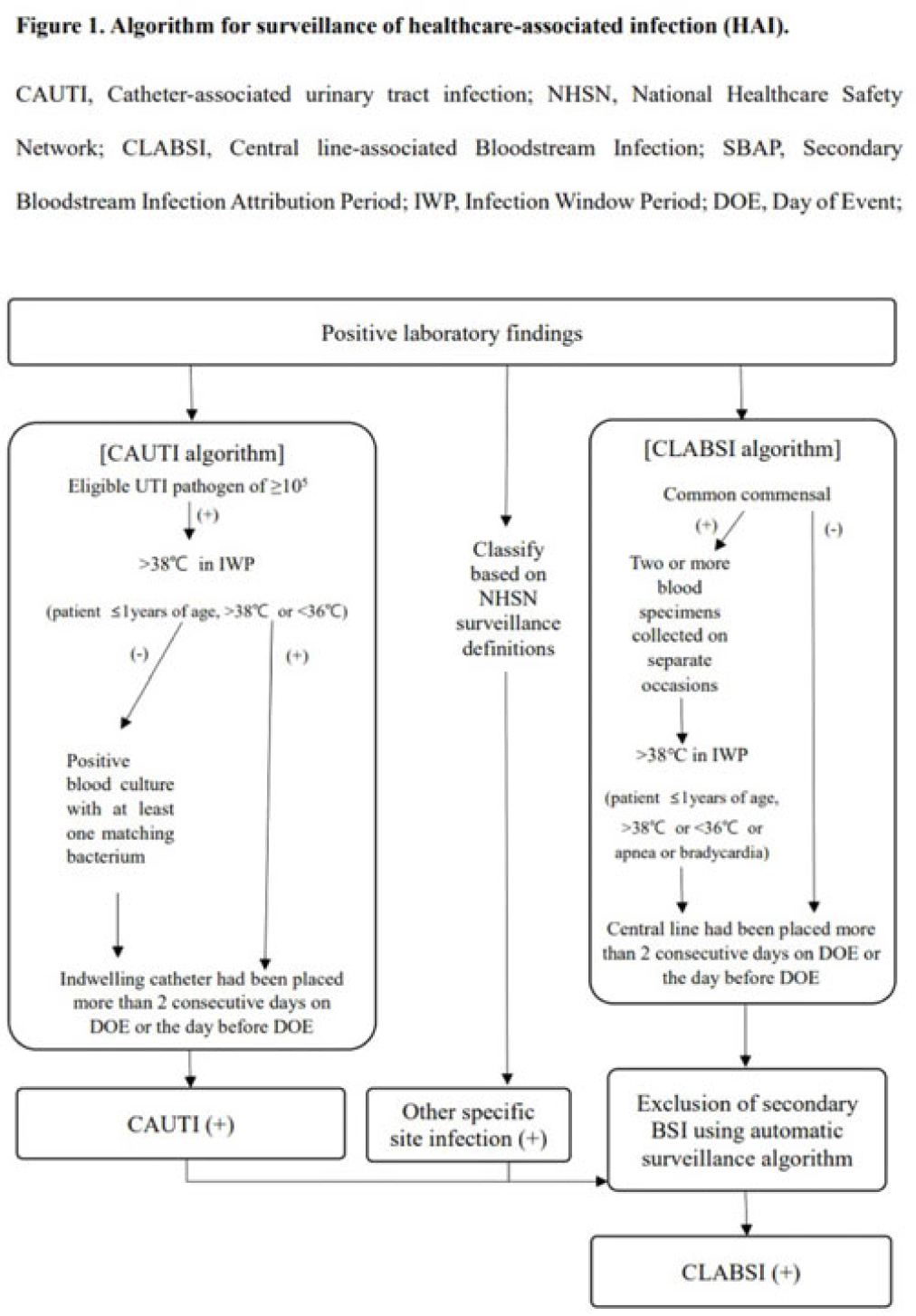
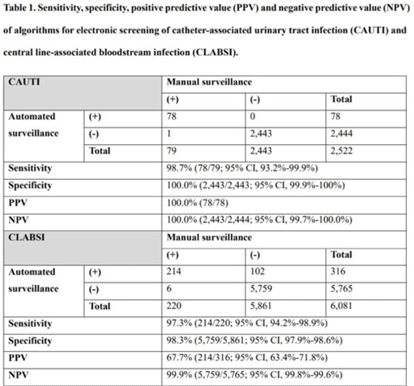
Background: Surveillance of healthcare-associated infection (HAI) is the basis of infection prevention programs. However, manual review of medical records is a labor-intensive and time-consuming process. We evaluated the diagnostic performance of automated surveillance of HAI using electronic screening algorithms. Methods: Between April and June 2022, we conducted surveillance of HAI manually and automatically using electronic screening algorithm on 75 units (general medical and surgical wards and ICUs) in a 2,700-bed, tertiary-care hospital in South Korea. Algorithms for surveillance of HAI were developed accordance with NHSN surveillance definitions (Fig. 1). Catheter-associated urinary tract infections (CAUTIs) were automatically detected when eligible pathogen and fever (>38°C) were matched within infection window period. Other specific types of infection were automatically classified based on laboratory results that met NHSN criteria. After the algorithm showed possible cases that met laboratory-confirmed bloodstream infection (LCBI) criteria, we excluded secondary BSIs using the automatic surveillance algorithm. We analyzed sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for the automated surveillance system compared to manual surveillance. Results: An algorithm for detecting CAUTI showed 98.7% sensitivity (78 of 79), 100.0% specificity (2,443 of 2,443), 100.0% PPV (78 of 78), and 100.0% NPV (2,443 of 2,444). For CLABSI, the algorithm had 97.3% sensitivity (214 of 220), 98.3% specificity (5,759 of 5,861), 67.7% PPV (214 of 316), and 99.9% NPV (5,759 of 5,765). In total, 102 cases of possible CLABSI were identified by the algorithm, and 76 (74.5%) were eventually diagnosed as secondary BSIs. Also, by chart review, 20 BSIs (19.6%) were present on arrival in ER (ER-POA). In 4 cases (3.9%), an original pathogen reoccurred in a repeated infection timeframe (RIT), and 2 cases (2%) were mucosal barrier injury-LCBI (MBI-LCBI). When we additionally performed manual surveillance for intra-abdominal infection secondary BSI, ER-POA, and assigning pathogen to original BSI in RIT, PPV increased to 87.7% (214 of 244). Conclusions: Algorithm for automated surveillance of CAUTI had good performance; however, automated surveillance of CLABSI was suboptimal. More elaborate screening algorithm for diagnosis CLABSI is needed, and further studies are needed to determine whether an automated surveillance system can reduce workload for surveillance of HAI.
Disclosures: None
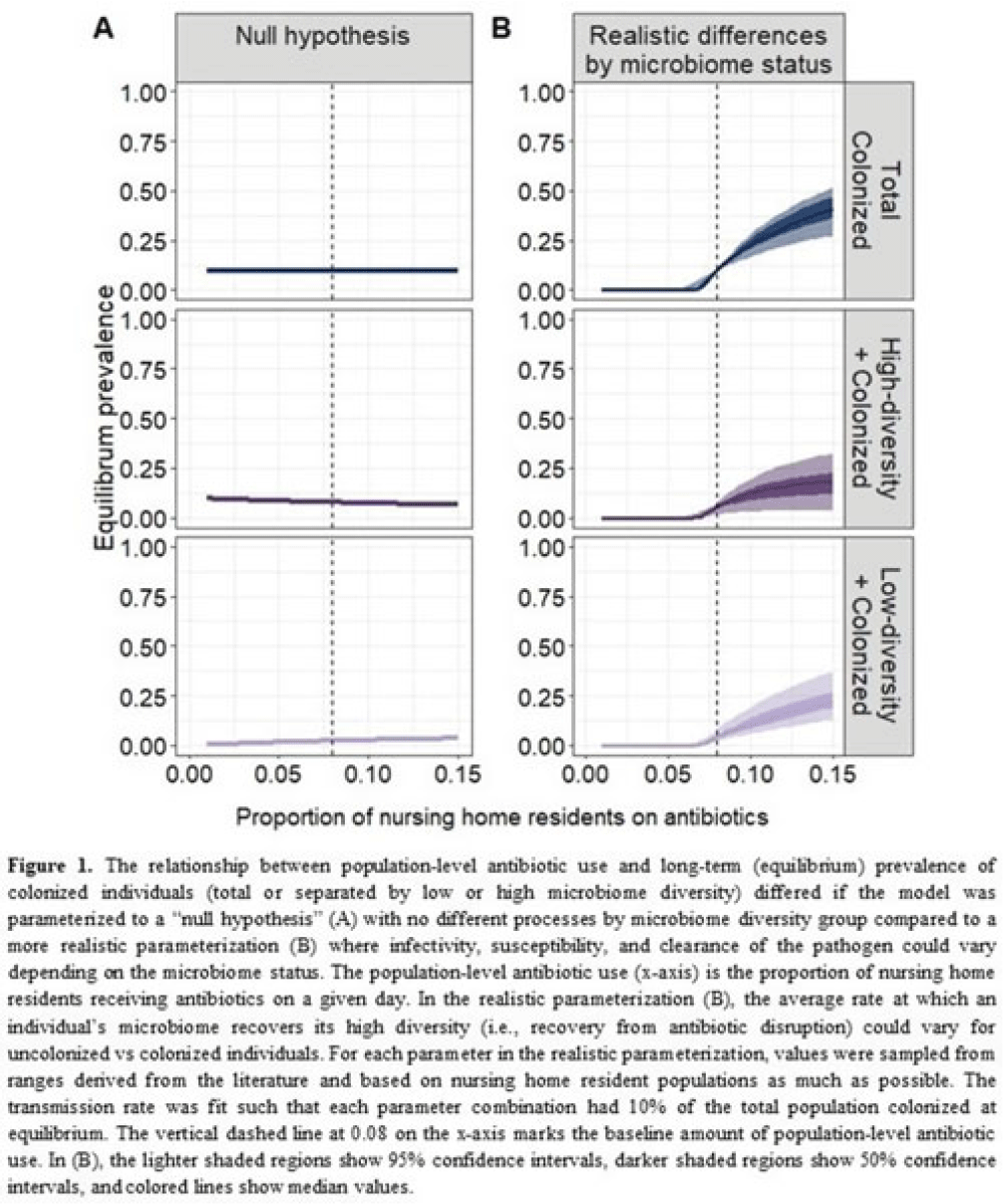
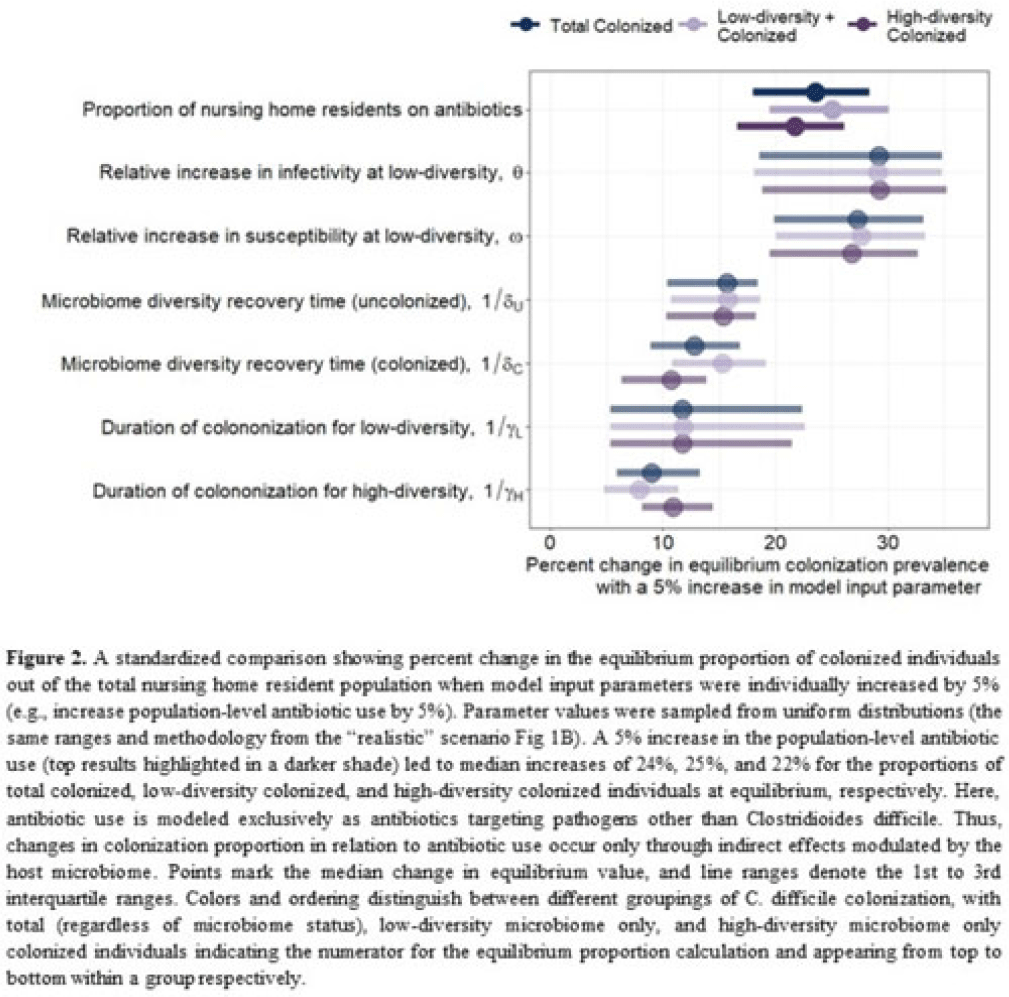
Background: Clostridioides difficile and multidrug-resistant organisms (MDROs) pose challenges due to treatment complexities and substantial morbidity and mortality. Susceptibility to colonization with these organisms and potential onward transmission if colonized (ie, infectivity) is influenced by the human microbiome and its dynamics. Disruptive effects of antibiotics on the microbiome imply potential indirect effects of antibiotics on C. difficile colonization. Mathematical models can help explore the relative impact of key pathways linking antibiotic use to C. difficile colonization, including the relationship between population-level antibiotic use and colonization prevalence. Methods: We built a compartmental model of long-term C. difficile colonization prevalence of nursing home residents (though malleable for any MDRO), allowing interactions between the microbiome and the colonization process. Based on proportional abundance of microbial taxa, we classified individuals into high and low α diversity groups, each further stratified into uncolonized or colonized with C. difficile. The rate of transition from the high to low microbiome diversity group was proportional to the population-level rate of antibiotic use. Transmission dynamics followed a susceptible–infectious–susceptible framework with the possibility for increased susceptibility and infectivity for the low-diversity microbiome group. First, as a comparator, we used a “null model” in which microbiome diversity did not influence host susceptibility or infectivity. Next, we sampled from realistic (literature informed) parameter ranges to analyze how the microbiome mediates the effect of antibiotics on colonization in this population. Results: Our analysis suggests that antibiotic use can catalyze colonization with C. difficile through interactions with the host microbiome, resulting in a sharp increase in colonization with a modest increase in antibiotic use (Fig 1). Increasing the population-level antibiotic use by 5% led to a median 24% increase in long-term colonization prevalence in the model (Fig 2). In contrast, increasing susceptibility or infectivity rates by 5% resulted in slightly higher increases in total colonization (27% and 29%, respectively). However, there was considerable uncertainty around these estimates, with interquartile ranges of up to 20% for some parameters (Fig 2). Conclusions: Higher population-level antibiotic use likely increases colonization by C. difficile through indirect effects of the microbiome. The increased colonization burden attributable to increasing antibiotic use may be substantial. With high uncertainty around some estimates, conducting observational studies to better understand key colonization and microbiome parameters (eg, the relative increase in susceptibility or infectivity with lower microbiome diversity) is critical for future efforts to estimate the impact of antibiotic use on colonization with C. difficile and MDROs.
Disclosures: None
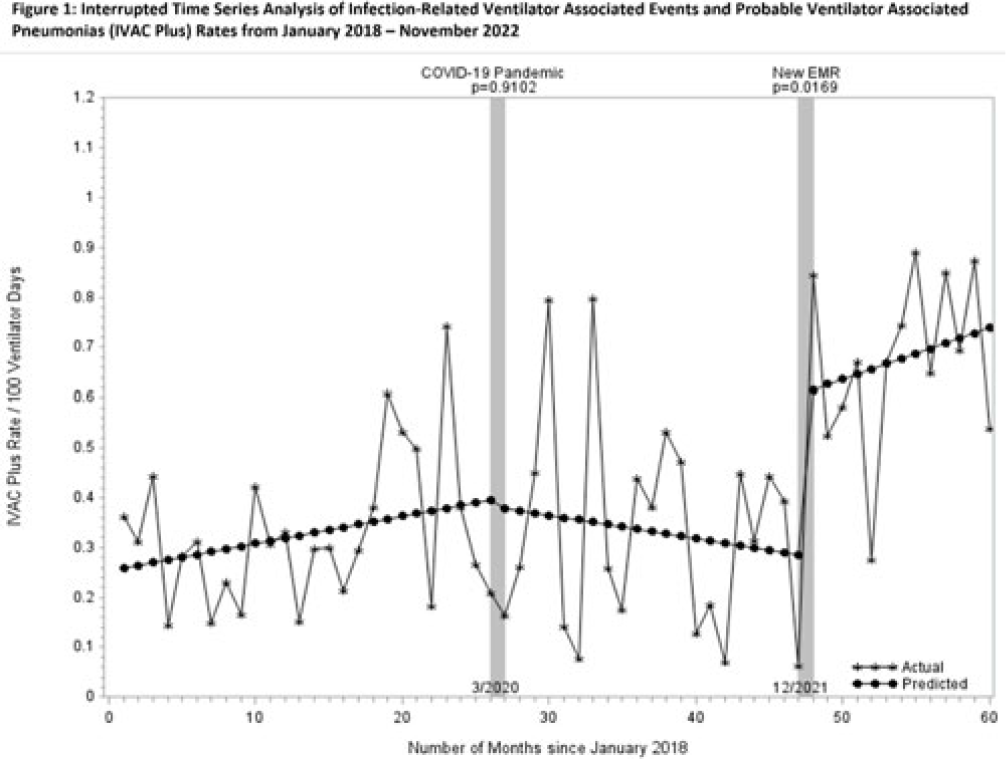
Background: Rates of ventilator-associated events (VAEs), including infection-related ventilator-associated complications (IVACs) and probable ventilator-associated pneumonia (PVAPs) have increased nationwide since the onset of the COVID-19 pandemic. In December 2021, our health system adopted a new electronic medical record (EMR), which changed the way surveillance for VAEs is performed. We reviewed surveillance criteria, COVID-19 status, and culturing practices in attempts to understand why VAE rates continue to be elevated. Methods: We collected data on VAE type, culture data, COVID-19 status, and surveillance criteria for all patients meeting NHSN definitions for VAE from 2018 through November 2022. For all patients in 2022 (post-EMR transition), 2 physicians (A.D. and M.D.) manually reviewed documented ventilator settings from flow sheets to validate the automated EMR data, and they evaluated culture data for appropriateness. Cultures were defined as appropriate unless they were included in “pancultures” for leukocytosis without concern for pneumonia documented. Rates were compared using an interrupted time series (ITS) analysis before and after the onset of the COVID-19 pandemic and the EMR transition. Patient level data were compared across periods using the χ2 test. All analyses were performed using SAS version 9.4 software. Results: COVID-19 has been implicated in the increasing number of VAEs since the pandemic began: 6% of patients in 2020, 18% in 2021, and 23% in 2022 (P < .001). The percentage of patients meeting criteria for VAE by positive end-expiratory pressure (PEEP) decreased from 2018 to 2022 (92%, 95%, 93%, 85%, 85%, respectively; P = .0004). Patients meeting criteria for VAE by fraction of inspired oxygen (FiO2) increased from 2018 to 2022 (9%, 6%, 11%, 17%, 19%, respectively; P = .0002). Manual review of 2022 data indicated opportunities for test stewardship in 8 of 65 patients with cultures (12%). ITS analysis revealed that IVAC+ rates were climbing prior to the onset of the COVID-19 pandemic (Fig. 1). We observed a marked increase in rates with the implementation of our new EMR and the changes to our surveillance process (0.32 cases per 100 ventilator days). Manual review of records from 2022 revealed 5 patients in which documentation of ventilator settings to meet VAE diagnosis could not be retrieved from flow sheets. Conclusions: COVID-19 continues to affect VAE despite vaccine availability and may partially account for elevated rates nationwide. However, changes in EMR-automated VAE surveillance may also affect rates. Our findings suggest that automated surveillance captures transient or spurious changes in ventilator machine settings that do not accurately represent clinical status. These data may contribute to spurious increases in VAE. More studies are needed to better understand the impact of both COVID-19 and automated surveillance on VAE.
Disclosures: None
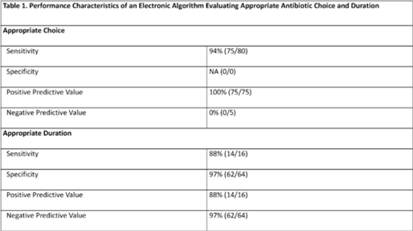
Background: Community-acquired pneumonia (CAP) is a common indication for antibiotic use in hospitalized children and is a key target for pediatric antimicrobial stewardship programs (ASPs). Building upon prior work, we developed and refined an electronic algorithm to identify children hospitalized with CAP and to evaluate the appropriateness of initial antibiotic choice and duration. Methods: We performed a cross-sectional study including children 6 months to 17 years hospitalized for CAP between January 1, 2019, and October 31, 2022, at a tertiary-care children’s hospital. CAP was defined electronically as an International Classification of Disease, Tenth Revision (ICD-10) code for pneumonia, a chest radiograph or chest computed tomography scan (CT) performed within 48 hours of admission, and systemic antibiotics administered within the first 48 hours of hospitalization and continued for at least 2 days. We applied the following exclusion criteria: patients transferred from another healthcare setting, those who died within 48 hours of hospitalization, children with complex chronic conditions, and those with intensive care unit stays >48 hours. Criteria for appropriate antibiotic choice and duration were defined based on established guidelines. Two physicians performed independent medical record reviews of 80 randomly selected patients (10% sample) to evaluate the performance of the electronic algorithm in (1) identifying patients treated for clinician-diagnosed CAP and (2) classifying antibiotic choice and duration as appropriate. A third physician resolved discrepancies. The electronic algorithm was compared to this medical record review, which served as the reference standard. Results: Of 80 children identified by the electronic algorithm, 79 (99%) were diagnosed with CAP based on medical record review. Antibiotic use was classified as the appropriate choice in 75 (94%) of 80 cases, and appropriate duration in 16 (20%) of 80 cases. The sensitivity of the electronic algorithm for identifying appropriate initial antibiotic choice was 94%; specificity could not be calculated because no events of inappropriate antibiotic choice were identified based on chart review. The sensitivity and specificity for determining appropriate duration were 88% and 97%, respectively (Table 1).
Conclusions: The electronic algorithm accurately identified children hospitalized with CAP and demonstrated acceptable performance for identifying appropriate antibiotic choice and duration. Use of this electronic algorithm may improve the efficiency of stewardship activities and could facilitate alignment with updated accreditation standards. Future studies validating this algorithm at other centers are needed.
Disclosures: None
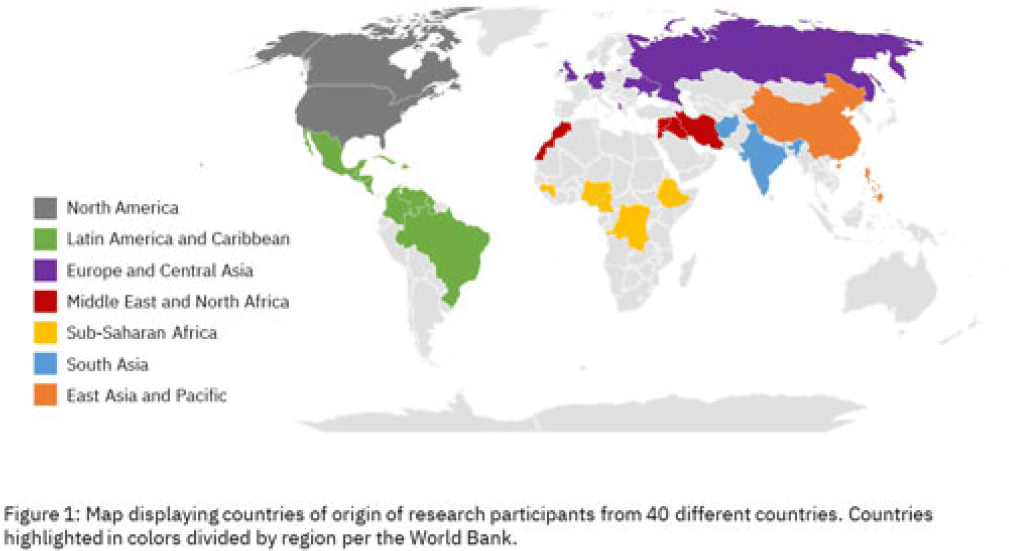
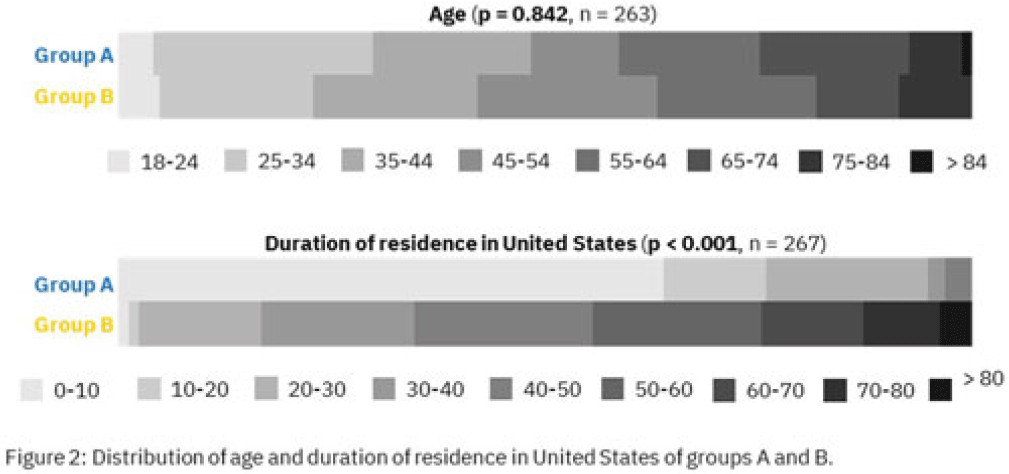
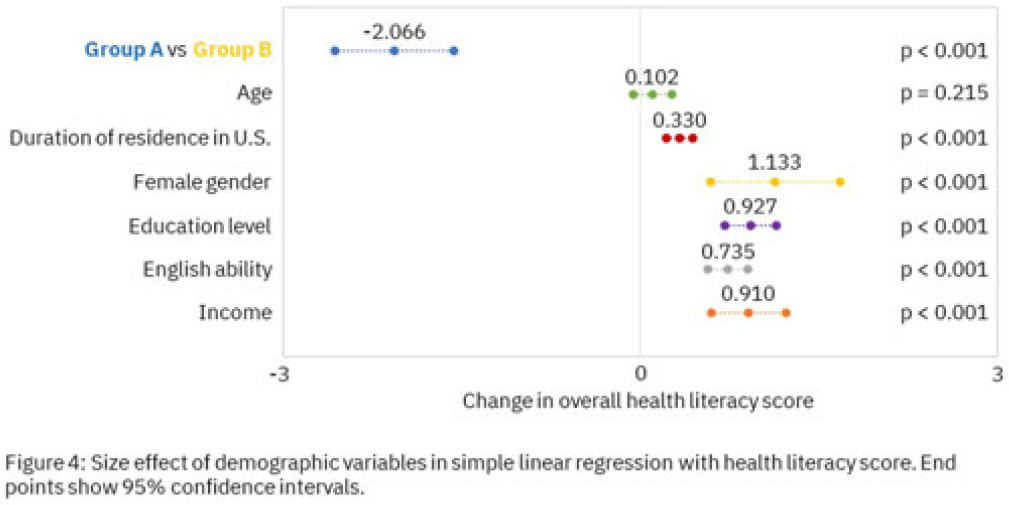
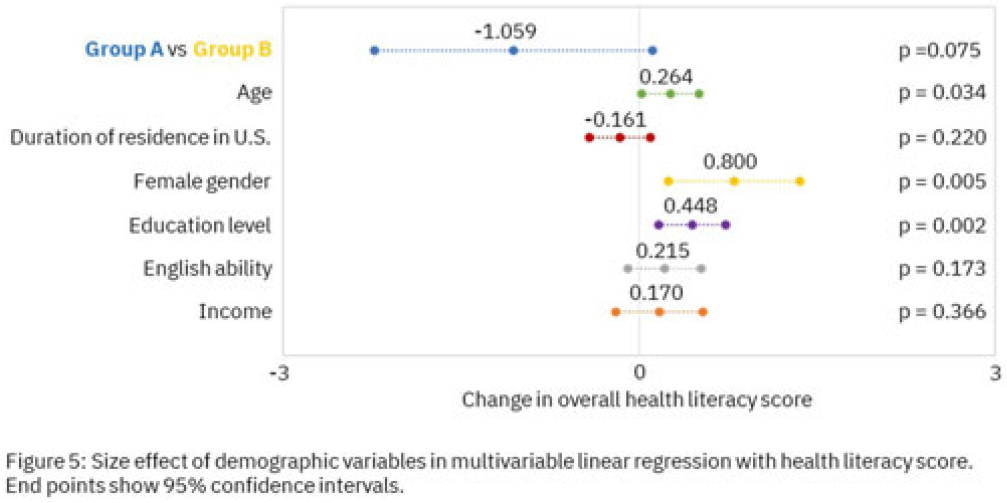
Background: Antimicrobial resistance (AMR) is a global health threat, particularly in refugee populations, due to challenges posed by migration. Little guidance has been provided by public health agencies regarding antimicrobial stewardship specific to this demographic. Studies have primarily focused on encampment areas abroad. We sought to better understand health literacy and beliefs regarding AMR in local refugee and immigrant populations in southeastern Michigan. Methods: From November 1, 2022 to March 10, 2023, we distributed an anonymous questionnaire to adult patients at four primary care clinics in Southeastern Michigan and made it available online. The questionnaire collected demographic information and used 5-point Likert scale responses regarding antibiotic use in children with symptoms of respiratory infection. We binarized the questions and responses to determine whether respondents provided the preferred response and added these to create an overall health literacy score, then used simple linear and multivariable linear regression modeling to identify demographic variables independently associated with the health literacy score. Chi-squared and Mann-Whitney tests were also performed where appropriate. Results: Immigrants and refugees/asylum-seekers from low or middle-income countries (group A, n = 109) were compared to native-born Americans and immigrants from high-income countries (group B, n = 171) with participants from 40 countries (Figure 1). Age distribution did not differ between groups, while group B had generally longer duration of living in the United States (Figure 2). Differences were found in other demographic categories except female gender, with group B reporting higher income, educational levels, and English ability (Figure 3). Simple linear regression revealed that all demographic variables except age significantly correlated with responses (Figure 4). Multivariable linear regression showed that female gender, educational level, and age correlated with greater health literacy, while being in group A trended towards significance with respect to correlating with lesser health literacy (Figure 5). Conclusions: Immigrants and refugees/asylum-seekers from LMICs demonstrated beliefs suggesting deficits in knowledge of AMR compared to native-born Americans and those from high-income countries, independent of other potentially confounding demographic characteristics. Female gender, educational level, and age independently correlated with greater health literacy. These results could inform future patient-centered antimicrobial stewardship educational interventions in certain target populations such as immigrants and refugees/asylum-seekers in the United States.

Disclosures: None
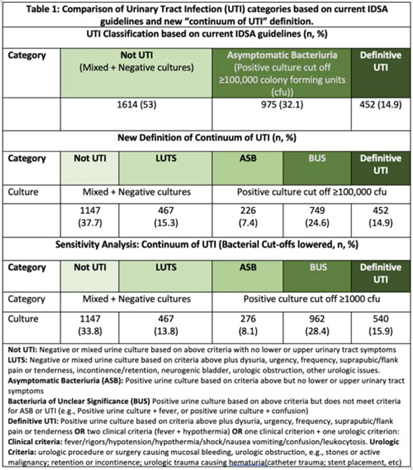
Background: Historically, diagnosis of urinary tract infections (UTIs) has been divided into 3 categories based on symptoms and urine culture results: not UTI, asymptomatic bacteriuria (ASB), or UTI. However, some populations (eg, older adults, catheterized patients) may not present with signs or symptoms referrable to the urinary tract or have chronic lower urinary tract symptoms (LUTS), making the diagnosis of UTI challenging. We sought to understand the clinical presentation of patients who receive urine tests in a cohort of diverse hospitals. Methods: This retrospective descriptive cohort study included all adult noncatheterized inpatient and ED encounters with paired urinalysis and urine cultures (24 hours apart) from 5 community and academic hospitals in 3 states (NC, VA, GA) between January 1, 2017, and December 31, 2019. Trained abstractors collected clinical and demographic data using a 60-question REDCap survey. The study group met with multidisciplinary experts (ID, geriatrics, urology) to define the “continuum of UTI” (Table 1), which includes 2 new categories: (1) LUTS to capture patients with chronic lower urinary tract symptoms and (2) bacteriuria of unclear significance (BUS) to capture patients who do not clinically meet criteria for ASB or UTI (eg, older adults who present with delirium and bacteriuria). The newly defined categories were compared to current guideline-based categories. We further compared ASB, BUS, and UTI categories using a lower bacterial threshold of 1,000 colony-forming units. Results: In total, 220,531 encounters met study criteria. After using a random number generator and removing duplicates, 3,392 encounters were included. Based on current IDSA guidelines, the prevalence of ASB was 32.1% (n = 975), and prevalence of patients with “not UTI” was 1,614 (53%). Applying the expert panel’s new “continuum of UTI” definitions, the prevalence of “not UTI” patients decreased to 1,147 (37.7%), due to reassignment of 467 patients (15.3%)to LUTS. The prevalence of ASB decreased by 24% due to reassignment to BUS. Lowering the bacterial threshold had a slight impact on the number of definitive UTIs (14.9 vs 15.9%) (Table 1). Conclusions: Our rigorous review of laboratory and symptom data from a diverse population dataset revealed that diagnostic uncertainty exists when assessing patients with suspicion for UTI. We propose moving away from dichotomous approach of ASB versus UTI and using the “continuum of UTI” for stewardship conversations. This approach will allow us to develop nuanced deprescribing interventions for patients with LUTS or BUS (eg, watchful waiting, shorter course therapy) that account for the unique characteristics of these populations.
Disclosures: None
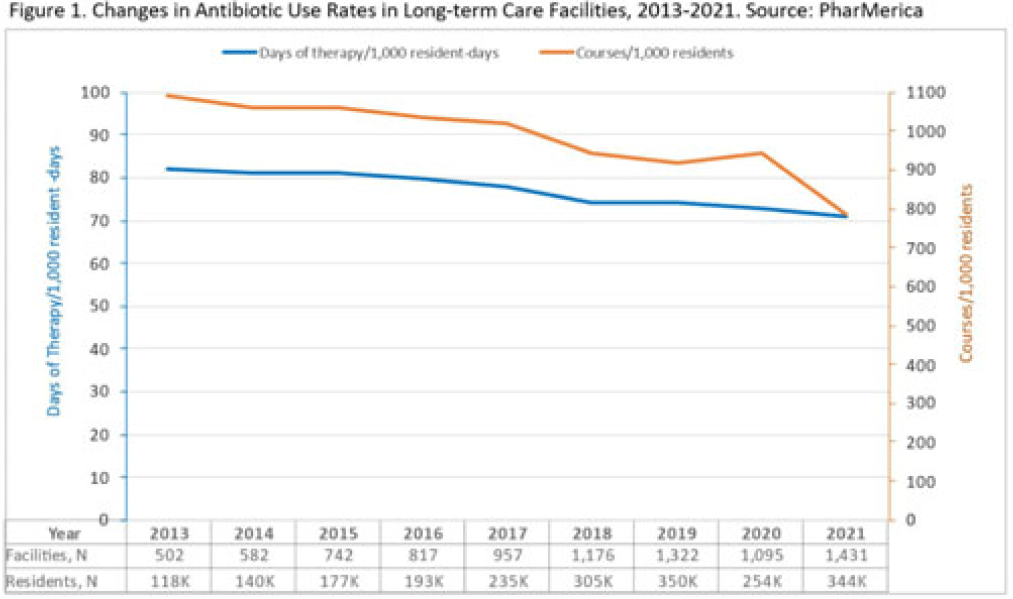
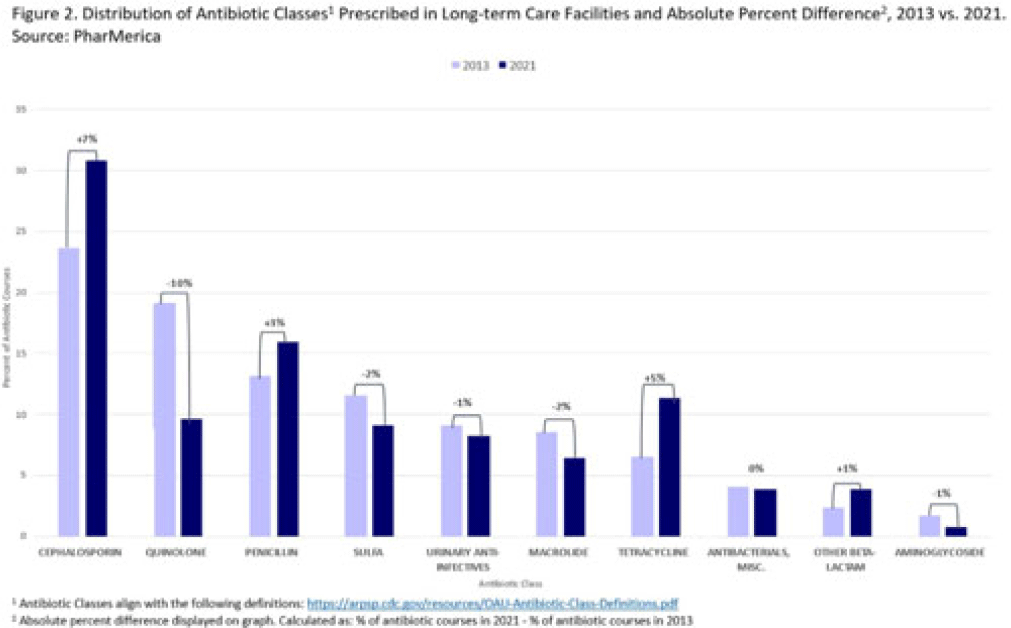
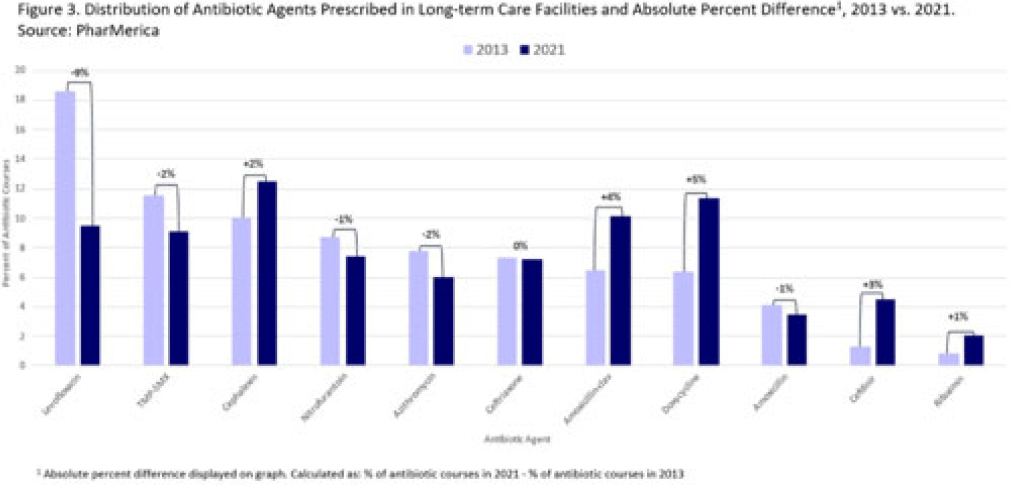
Background: Antibiotic use (AU) data are needed to improve prescribing in long-term care facilities (LTCFs). CMS requires AU tracking in LTCFs (effective 2017). Although most LTCFs have limited resources for AU tracking, LTCFs contract with LTCF pharmacies to dispense, monitor, and review medications. The objective of our analysis was to report LTCF antibiotic prescribing and characterize temporal changes from 2013 to 2021. Methods: We estimated annual systemic AU rates using prescription dispenses and resident census data from PharMerica, a LTCF-pharmacy services provider that covers ~20% of LTCFs nationwide, although the number of LTCFs and residents serviced by PharMerica varied over time (Fig. 1). We included LTCFs with ≥4 months of antibiotic dispensing and 12 months of census data. We identified courses by collapsing the same drug dispensed to the same resident within 3 days of the preceding end date. Course duration was calculated as the difference between the end and dispense dates. We reported yearly AU rates as courses per 1,000 residents and days of therapy (DOT) per 1,000 resident days from 2013 to 2021. We compared AU rates (percentage change) and antibiotic courses by class and agent (absolute percent difference) between 2013 and 2021. Results: From 2013 to 2021, AU course rates reported as antibiotic courses per 1,000 residents decreased (percentage change, −28%), with a notable increase in 2020 (Fig. 1). However, the median course duration remained the same (Table 1). The AU decline was mostly driven by decreases in fluoroquinolone courses (absolute difference, −10%, most commonly levofloxacin) and macrolide courses (−2%, most commonly azithromycin) (Figs. 2 and 3). Increases in cephalosporin courses (absolute difference, +7%, most commonly cephalexin) and tetracycline courses (+5%, most commonly doxycycline) were also observed (Figs. 2 and 3). During this period, AU DOT rates reported as DOT per 1,000 resident days decreased (percentage change, −13%) (Table 1). Conclusions: The LTCF AU rates, especially for fluoroquinolones, have decreased in recent years with associated shifts in the distribution of antibiotic classes. This finding may be due to CMS stewardship requirements and increased awareness of adverse events, including the FDA fluoroquinolone warnings. The observed increase in 2020 could be secondary to changes in prescribing practices and resident population during the COVID-19 pandemic. Opportunities to improve prescribing in LTCFs include optimizing treatment duration and leveraging LTCF-pharmacy resources to provide stewardship expertise and support AU tracking and reporting.

Disclosures: None
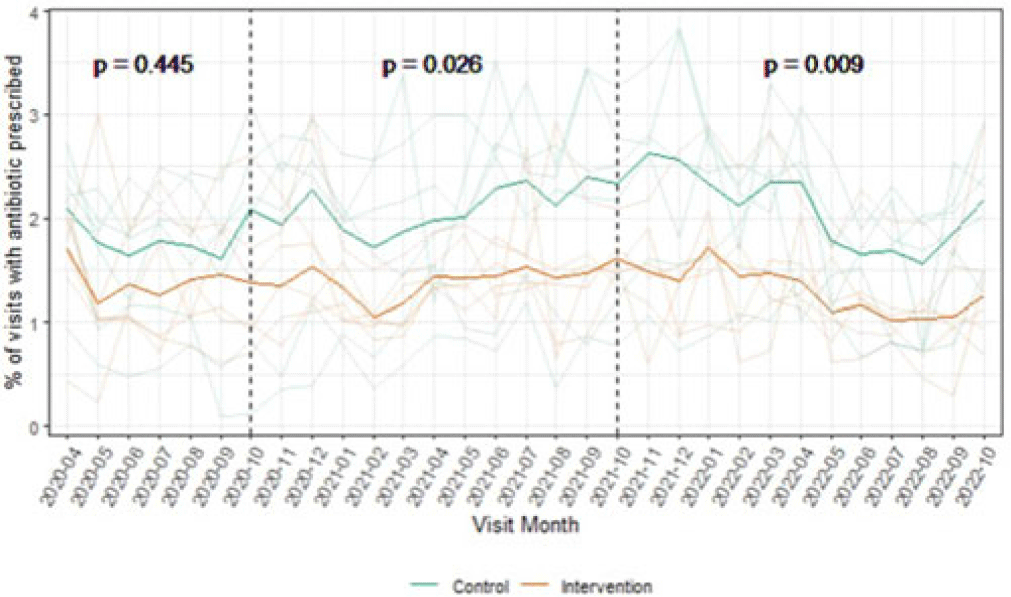
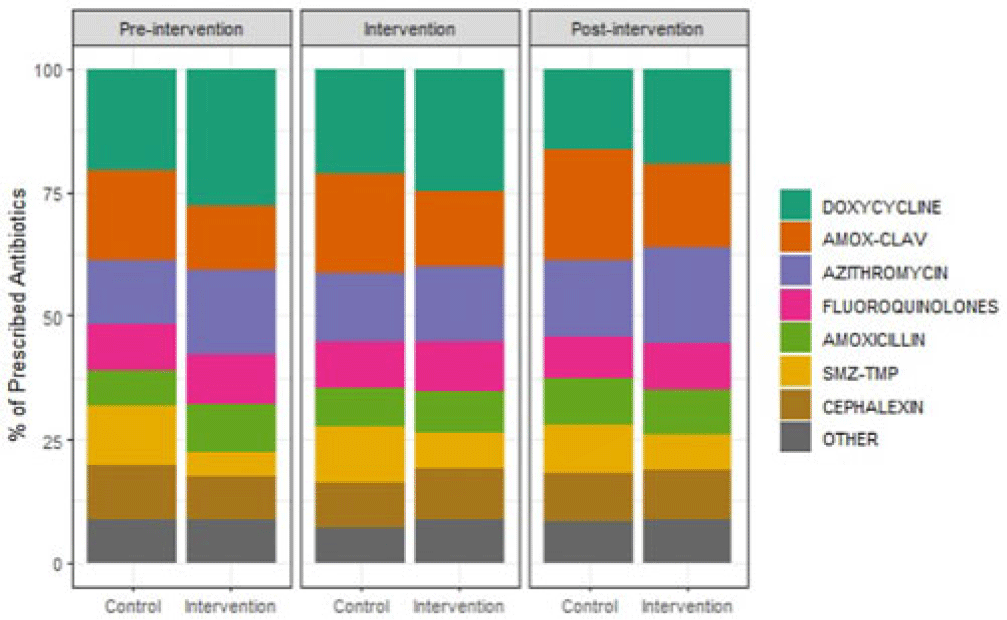
Background: Overall, ~12% of outpatient visits result in an antibiotic prescription, and 30% of those prescriptions are inappropriate. Behavioral nudges help influence practitioner behavior. We hypothesized that peer comparison combined with a behavioral nudge (a patient alert letter) would influence prescribers to reduce antibiotic prescriptions and improve antimicrobial stewardship in the outpatient setting. We pilot-tested this intervention in outpatient primary care clinics associated with a large Veterans Affairs (VA) medical center. Methods: We conducted a clustered randomized controlled trial of 12 community-based outpatient clinics. All practitioners in the intervention arm received quarterly comparative feedback reports and, when indicated, quarterly patient alert letters. Comparative feedback reports gave personalized feedback about antibiotic prescriptions for upper respiratory tract infections, comparing the recipient’s antibiotic prescriptions to the average for all practitioners at the primary care clinics included in our study. Patient alert letters notified practitioners to patients in their panel with recently detected Clostridioides difficile or resistant organism and their antibiotic exposures. We assessed outpatient visits during the preintervention period (April–September 2020), the intervention period (October 2020–September 2021), and the postintervention period (October 2021–September 2022). A mixed-effects logistic regression model predicting antibiotic prescriptions compared the arms across these periods. Results: The outpatient populations observed in the intervention and control arms were similar during each phase of the study. Prior to the intervention, the average proportion of visits with an antibiotic prescription was lower among clinics in the intervention arm (1.4% vs 1.8% in control arm; P = .45). This difference broadened slightly during the intervention period (1.4% vs 2.1%, respectively; P = .03) and the postintervention period (1.3% vs 2.1%, respectively; P = .01) (Fig. 1). Throughout the study, clinics in the intervention arm typically used more doxycycline and azithromycin and less amoxicillin-clavulanate and sulfamethoxazole-trimethoprim compared to clinics in the control arm. (Fig. 2). In the 6-month preintervention period, which coincided with the early phase of the COVID-19 pandemic, antibiotic prescriptions in the intervention compared to control clinics were similar. During the intervention and postintervention periods, the proportion of visits with an antibiotic prescription remained steady for clinics in the intervention arm and increased for those in the control arm. These results suggest that this pilot study using a low-intensity intervention consisting of comparative feedback reports and patient alert letters was successful in influencing the antibiotic prescribing behavior of primary care clinicians practicing in community-based outpatient clinics affiliated with a VA medical center.
Financial support: This study was funded by Merck.
Disclosures: None
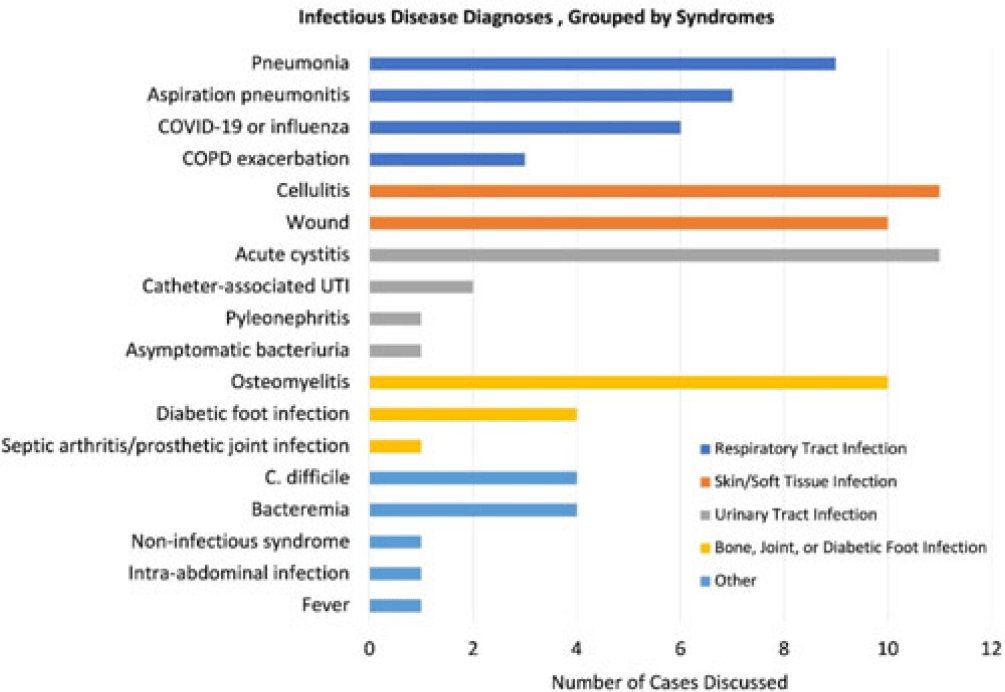
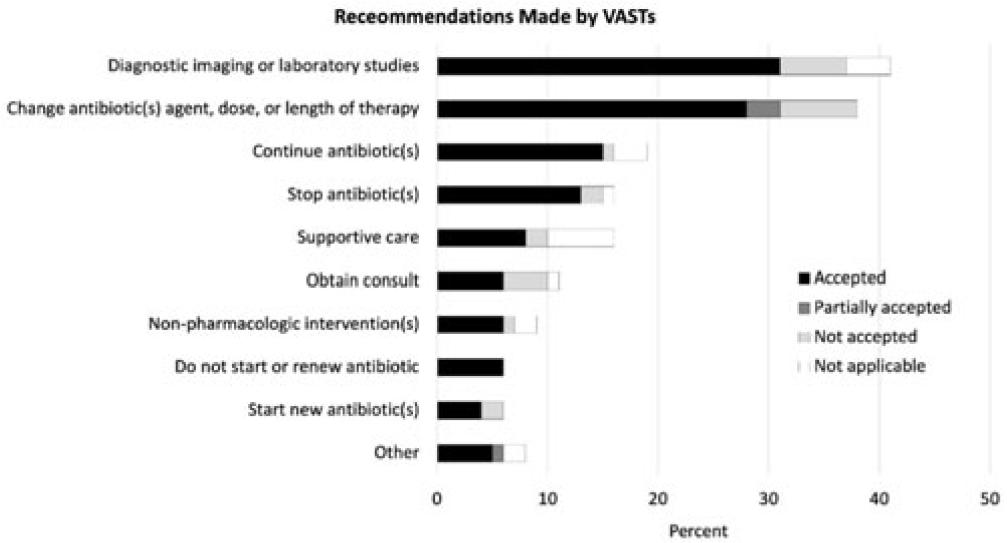
Background: Healthcare settings without access to infectious diseases experts may struggle to implement effective antibiotic stewardship programs. We previously described a successful pilot project using the Veterans Affairs (VA) telehealth system to form a Videoconference Antimicrobial Stewardship Team (VAST) that connected multidisciplinary teams from rural VA medical centers (VAMCs) with infectious diseases experts at geographically distant locations. VASTs discussed patients from the rural VAMC, with the overarching goal of supporting antibiotic stewardship. This project is currently ongoing. Here, we describe preliminary outcomes describing the cases discussed, recommendations made, and acceptance of those recommendations among 4 VASTs. Methods: Cases discussed at any of the 4 participating intervention sites were independently reviewed by study staff, noting the infectious disease diagnoses, recommendations made by infectious diseases experts and, when applicable, acceptance of those recommendations at the rural VAMC within 1 week. Discrepancies between independent reviewers were discussed and, when consensus could not be reached, discrepancies were discussed with an infectious diseases clinician. Results: The VASTs serving 4 different rural VAMCs discussed 96 cases involving 92 patients. Overall, infection of the respiratory tract was the most common syndrome discussed by VASTs (Fig. 1). The most common specific diagnoses among discussed cases were cellulitis (n = 11), acute cystitis (n = 11), wounds (n = 11), and osteomyelitis (n = 10). Of 172 recommendations, 41 (24%) related to diagnostic imaging or laboratory results and 38 (22%) were to change the antibiotic agent, dose, or duration (Fig. 2). Of the 151 recommendations that could be assessed via chart review, 122 (81%) were accepted within 1 week. Conclusions: These findings indicate successful implementation of telehealth to connect clinicians at rural VAMCs with an offsite infectious diseases expert. The cases represented an array of common infectious syndromes. The most frequent recommendations pertained to getting additional diagnostic information and to adjusting, but not stopping, antibiotic therapy. These results suggest that many of the cases discussed warrant antibiotics and that VASTs may use the results of diagnostic studies to tailor that therapy. The high rate of acceptance suggests that the VASTs are affecting patient care. Future work will describe VAST implementation at 4 additional VAMCs, and we will assess whether using telehealth to disseminate infectious diseases expertise to rural VAMCs supports changes in antibiotic use that align with principles of antimicrobial stewardship.
Disclosures: None
