This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
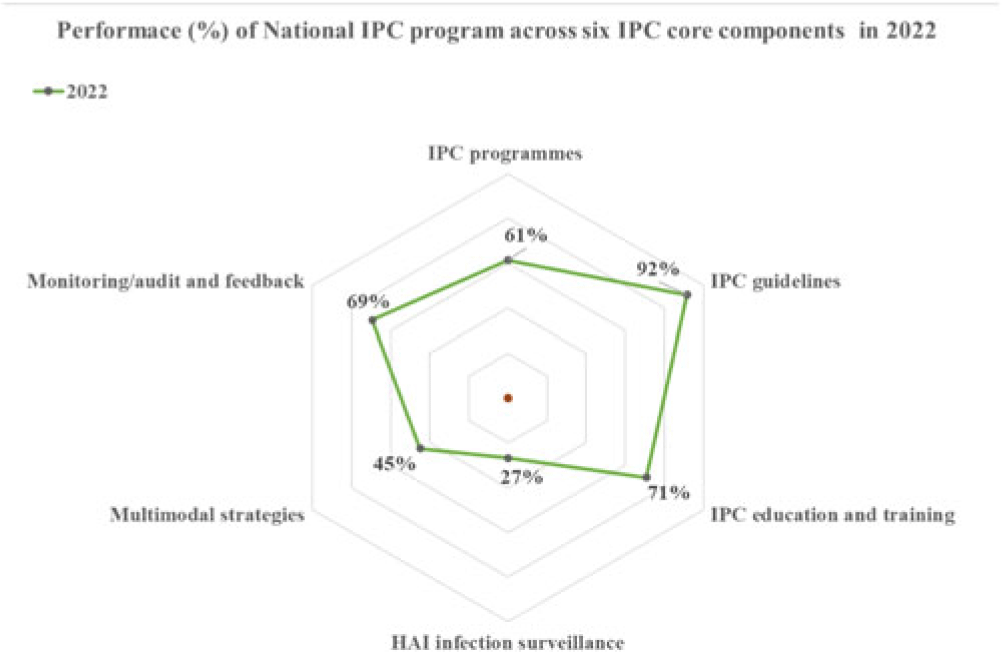
Background: Infection prevention and control (IPC) is a clinical and public health discipline based on a scientific approach and practical preventive and control measures. During the 2014–2016 West African Ebola outbreak, the high number of healthcare worker infections was attributed to inadequate IPC in Sierra Leone. This stimulated the establishment of national and subnational IPC programs. Since then, IPC has remained a priority to improve the health systems and strategic interventions during public health emergencies. Therefore, we conducted a detailed review to assess the status of the IPC programs. Methods: A descriptive analysis of the status of IPC programs in Sierra Leone was done using data from IPC assessments conducted in 2022 by the national IPC team, reviews of reports on program implementation, and experts’ objective opinions. Results: Performance. The national IPC assessment revealed strengths in 4 of 6 WHO IPC core components, with an overall score of 61% positioned at the ‘intermediate’ level of implementation. The best-performing component was ‘IPC guidelines’ (92%) with evidenced-based guidelines being developed and implemented over the years. Secondly, ‘Education and training’ (71%) made progress in basic and advanced IPC training, including the development of a preservice training curriculum. Also, ‘monitoring and audit and feedback’ (69%) and ‘IPC program’ (61%) met the basic requirements of an established Monitoring & Evaluation (M&E) system. Similar progress was made at the healthcare facility level, but with major gaps in ‘workload, staffing, bed-occupancy’ and ‘safe or built environment.’ Sustainability efforts. Evidence-based data on IPC have always been scarce due to a limited capacity to conduct IPC research. The Structured Operational Research and Training Initiative (SORT-IT) on antimicrobial resistance has helped promote evidence-informed decisions and build OR capacity that is relevant to improving program performance. In 2019, Sierra Leone instituted in-country production of alcohol-based handrub and liquid soap as a strategic intervention for providing hand hygiene products for use in healthcare facilities. This intervention was essential during the peak of the COVID-19 pandemic. Although most aspects of IPC implementation are government led with strong leadership support, stable funding and sustainability planning are yet to be achieved and will be crucial for long-term success. Conclusions: Most aspects of the IPC core components have been well implemented at the national level since the establishment of the IPC program. However, the program should continue improving the scope and quality of implementation and focus on the development of long-term plans to sustain existing gains and further improve on gap areas at the national level and especially the healthcare-facility level.
Disclosures: None
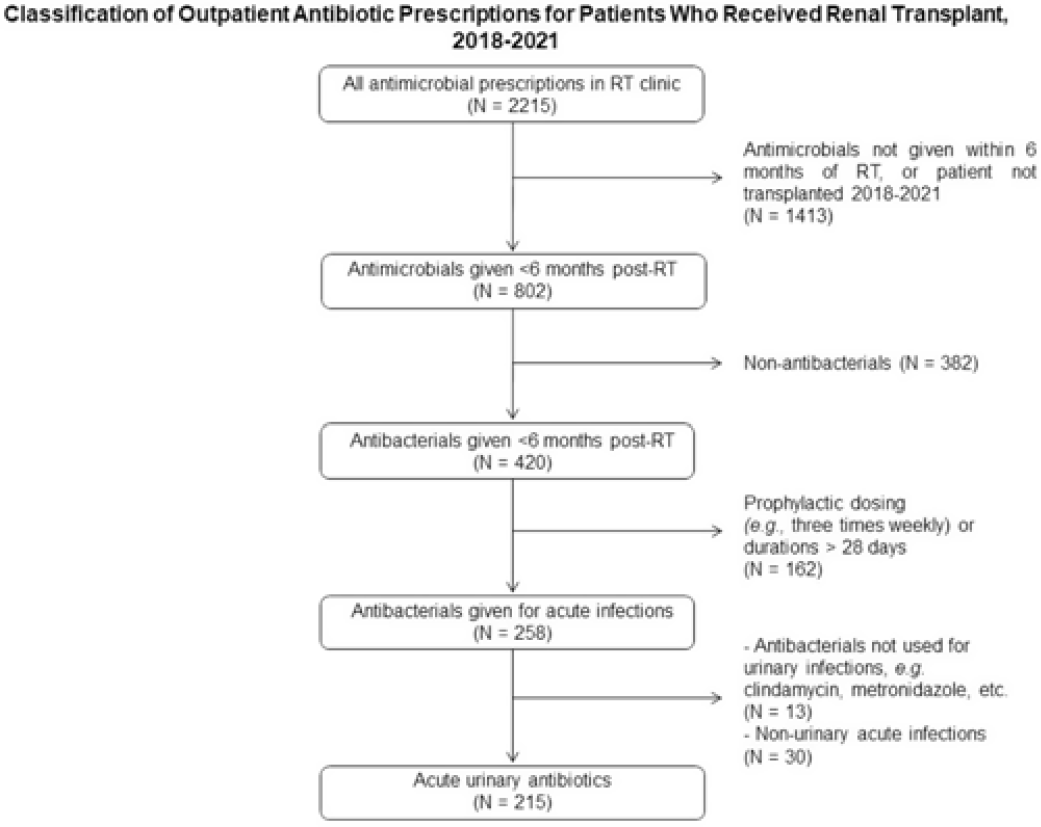
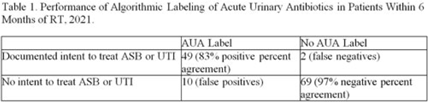
Background: International Classification of Diseases, Tenth Edition (ICD-10) data help track outpatient antibiotic prescribing but lack validation in immunocompromised populations or subspecialty clinics for this purpose. Asymptomatic bacteriuria (ASB) and urinary tract infection (UTI) are important stewardship targets in renal transplant (RT) patients, but they may require alternative metrics to best monitor prescribing patterns. We describe ICD-10 utilization for RT clinic encounters in which antibiotics were prescribed. We developed a metric classifying “acute urinary antibiotics” (AUA) to track antibiotic use for ASB and UTI, and we validated systematic identification of AUA to enable practical implementation. Methods: We examined RT clinic visit and telemedicine encounters from 2018 to 2021 conducted 1 month after transplant. This project was deemed non–human-subjects research by the Stanford Panel on Human Subjects in Medical Research. Results: The analytic cohort included 420 antibacterial prescriptions from 408 encounters (Fig. 1). Of 238 patients, 136 (57%) were male and 112 (47%) were Hispanic or Latino. The most common primary ICD-10 code was Z94.0 (kidney transplant status) (N = 302 of 408 encounters, 75%); 26 encounters (6%) were coded for UTI (eg, N39.0, urinary tract infection, site not specified); and 214 encounters (53%) had multiple ICD-10 codes. The R82.71 code (bacteriuria) was never used. However, 215 prescriptions (51%) were classified as AUA (Fig. 2). The validation cohort included 130 prescriptions; 59 (45%) were classified as AUA and 51 (39%) had documented intent to treat ASB or UTI (positive percent agreement, 83%; negative percent agreement, 97%) (Table 1). For patients >1 month after transplant, the positive percent agreement was 95% and the negative percent agreement was 98%. Of 51 patients receiving AUA, 32 (63%) were asymptomatic despite frequently having a code for UTI (Fig. 3). Conclusions: ICD-10 coding may not be helpful in monitoring antibiotic prescribing in RT patients. The AUA metric offers a practical alternative to track antibiotic prescribing for urinary syndromes and reliably correlates with physician intent. Monitoring AUA prescribing rates could help identify opportunities to optimize antibiotic use in this complex outpatient setting.

Disclosures: None
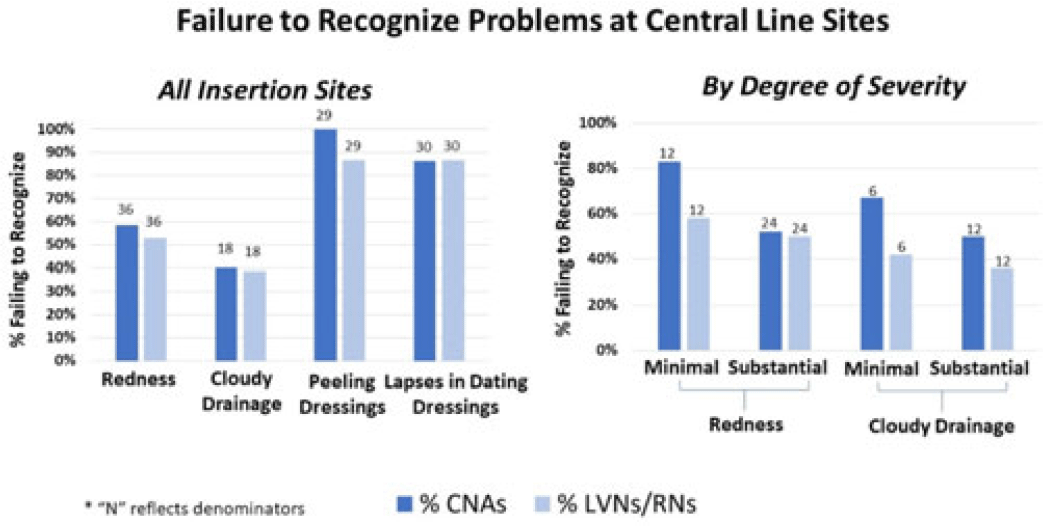
Background: Recognizing problematic central-line insertion sites is an important activity for CNAs, LVNs, and RNs in nursing homes (NHs). Although CNAs are not responsible for assessing central lines, they are often the first line of defense for noticing and relaying problems with a line because of the greater amount of time they spend with residents. We sought to assess how well CNAs, LVNs, and RNs could identify problematic insertion sites in NHs. Methods: We conducted a prospective observational study of central-line care in 8 NHs in Orange County, California. A convenience sample of central lines with a range of problematic elements was selected for quality improvement purposes. Research staff used standardized observation forms to evaluate presence of redness, cloudy drainage, and dressing integrity and change date. NH CNAs, LVNs, and RNs were asked to directly observe devices and to comment on problems or concerns. Participants were also asked open-ended questions about elements for a “picture-perfect line” and standard frequency of line checks and dressing changes. Failures to recognize existing problematic elements were tabulated for CNAs and LVNs or RNs separately. Results: In total, 50 CNAs (nursing home range, 3–6) and 50 LVNs and RNs (NH range, 4–6) directly observed lines with 131 problematic elements, including redness (N = 36), cloudy drainage (N = 30), peeling dressings (N = 29), and inappropriately dated dressing (N = 36). Failure to identify problematic elements involved redness [CNAs (50%) and LVNs or RNs (53%)], cloudy drainage [CNAs (40%) and LVNs or RNs (39%)], peeling dressings [CNAs (100%) and LVNs or RNs (87%)], and inappropriately dated dressing [CNAs (71%) and LVNs or RNs (68%)]. For both CNAs and LVNs and RNs, recognition of redness and cloudy drainage improved with severity. Failure to recognize minimal erythema [CNAs (83%) and LVNs or RNs (58%)] was higher than substantial erythema [CNAs (54%) and LVNs or RNs (50%)]. Similarly, failure to recognize minimal cloudy drainage [(CNAs (67%) and LVNs or RNs (50%)] was higher than substantial cloudy drainage [CNAs (42%) and LVNs or RNs (36%)]. Overall, identification of problematic elements did not vary by whether the staff member was assigned to care for that resident. Descriptions of “picture-perfect lines” were uniformly poor, with respondents not knowing what elements to mention. Conclusions: Failure to recognize redness, cloudy drainage, peeling dressings, and lapses in dressing change dates was common for CNAs and LVNs and RNs in nursing homes. This lack of recognition could prevent proper response to early and late signs of localized infection at central-line sites. Dedicated training regarding key elements of a “picture-perfect line” is needed, including changing the threshold for concern for both small and large amounts of redness and pus.
Disclosures: None
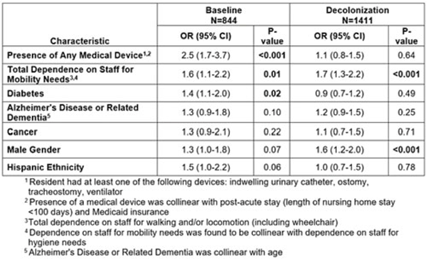
Background: A regional decolonization intervention (SHIELD-OC) involving universal chlorhexidine for routine bathing and 5 days of twice-daily nasal iodophor every other week in nursing homes (NHs) recently demonstrated marked reductions in multidrug-resistant organisms, all-cause hospitalizations, and infection-related hospitalizations in Orange County, California. Specific to methicillin-resistant Staphylococcus aureus (MRSA), NH prevalence (nares, skin, or perirectal) decreased from 43% to 29%. Methods: We conducted a retrospective cohort study evaluating the impact of decolonization on factors associated with MRSA carriage. The cohort included residents from 18 SHIELD-OC NHs who were sampled for MRSA using nares, axilla, groin, and perirectal cultures. A point-prevalence survey was conducted in 2016–2017 (before decolonization, 50 randomly sampled residents per NH) and in 2018–2019 (decolonization, all residents sampled). Resident characteristics were obtained from their most proximal admission, quarterly, and/or discharge assessment using data mandated for NH reporting (CMS minimum data set), and included demographics, medical devices, comorbidities (including Alzheimer’s disease and related dementias or ADRD), and mobility and hygiene needs. We used generalized-linear mixed models stratified by decolonization and clustered by NH to identify differences in factors associated with MRSA carriage. Results: Of the 2,351NH residents, 2,255 (96%) had characteristics available in the CMS data set. Of the 2,255 residents included, 774 (34%) were MRSA carriers. Before decolonization, medical devices (OR, 2.5), limited mobility (OR, 1.6), and diabetes (OR, 1.4) were significantly associated with MRSA carriage in an adjusted model (Table). During decolonization, these effects were mitigated (medical device OR, 2.5–1.1; diabetes OR, 1.4–0.9) and were no longer significantly associated with MRSA carriage. Male sex appeared to have more of an effect in the decolonization phase (OR, 1.3–1.6), but limited mobility remained stable (OR, 1.6–1.7). Several variables were collinear. Presence of a medical device was collinear with postacute stays (<100 days) and Medicaid insurance. Limited mobility was associated with limited ability for hygienic self-care. ADRD was collinear with age. Final adjusted models accounted for medical devices, limited mobility, diabetes, ADRD, cancer, sex, and ethnicity. Conclusions: In a large interventional cohort of 18 NHs, factors associated with MRSA carriage changed after adoption of universal decolonization. Specifically, the increased risk of MRSA associated with medical devices and diabetes were substantially mitigated by decolonization, suggesting that these risks are modifiable. These long-term care findings are consistent with clinical trials showing reductions in MRSA carriage after implementing chlorhexidine bathing in ICUs and in non-ICU patients with devices. The ability of decolonization to attenuate the risk of MRSA carriage among diabetics or other potential high-risk groups deserves further study.
Disclosures: None
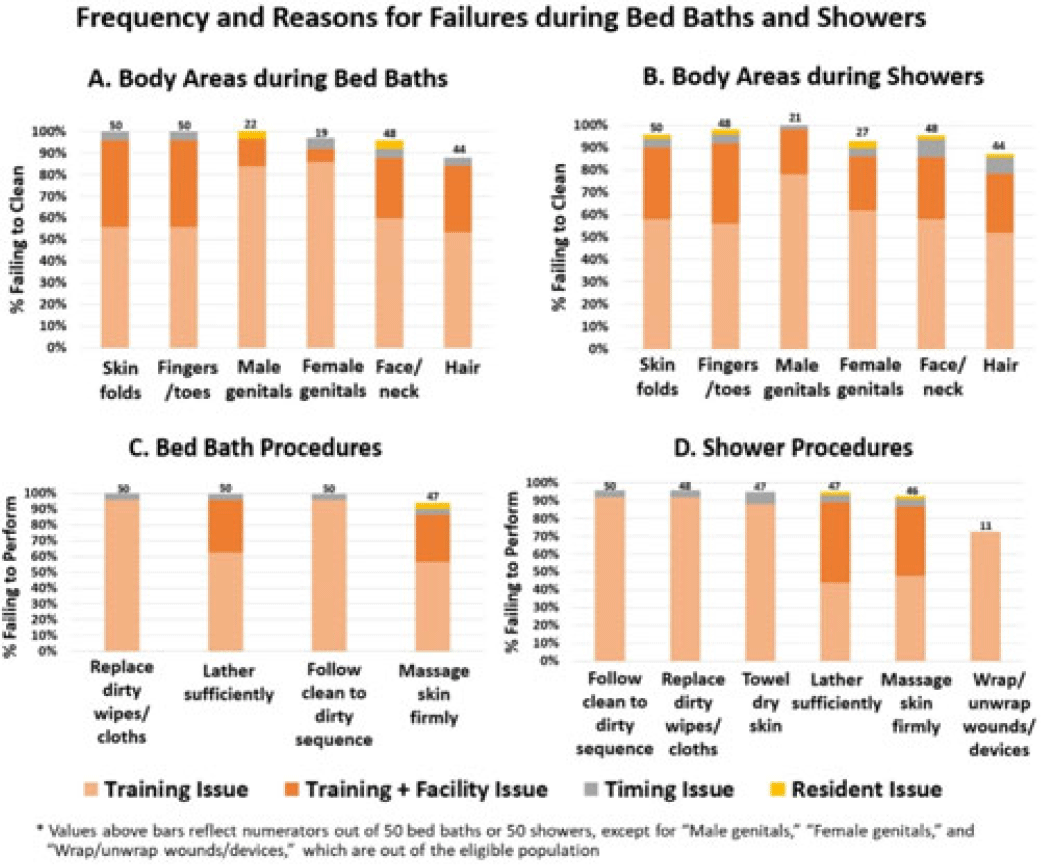
Background: Existing training for resident bathing in nursing homes (NHs) is brief and limited, likely because bathing is assumed to be intuitive. However, residents have complex skin issues, devices, dressings, and limited ability for self-care. We sought to assess bathing quality and to identify barriers to proper bathing techniques. Methods: We conducted a prospective observational study of bathing in 8 NHs in Orange County, California, involving a convenience sample of observed bed baths and showers conducted for quality improvement. NH staff were told that observation was occurring, and no feedback was given during or after bathing. Survey elements included cleansing of 6 specific body sites and adherence to bathing procedures (11 for bed baths and 17 for showers). Surveys also included queries to staff to further assess knowledge and perceived barriers. Observed lapses were documented, along with observer-determined reasons for noncompliance (ie, training issue, time pressure, facility issue (insufficient water temperature), resident refusal/behavior). Frequency of noncompliance with each element was tabulated for bed-baths and showers separately. Reasons for failure were displayed graphically. Results: In total, 50 bed baths (NH range, 5–8) and 50 showers (NH range, 4–7) were observed across 8 NHs. Lapses in bathing quality and process were extremely common for both bed baths and showers (Fig.). Inadequate body cleansing occurred for all observed body sites (88%–100% failure for bed baths, 58%–100% failure for showers). Most body areas were either skipped or sprayed with water without soaping. Procedural failures were high for both bed baths and showers (insufficient lather: 100% for bed bath and 40% for shower) lack of firm massage for cleaning (94% for bed bath and 90% for shower), failure to change wipes or cloths when dirty (100% for bed bath and 96% for shower), failure to follow clean-to-dirty sequence (100% for bed bath and 96% shower). In addition, failing to wrap or unwrap devices (73%) and failing to towel dry (94%) were common after showering. Reasons for failure were largely based on training or facility shortcomings (eg, insufficient hot water, inflexible showerhead attachment). Also, 86% of residents complained of being cold. Timing constraints and resident combativeness or refusal were rare. Staff-to-staff bathing advice most commonly involved competing for the “better shower” and “bathing early to get hot water.” Conclusions: Knowing how to appropriately bathe NH residents is not intuitive, and current training is brief and insufficient for high-quality resident care. Unacceptably high failures in proper bathing techniques in NHs necessitate re-evaluation of formal training and standardized practices to better cleanse residents. Moreover, common failures in facility processes for ensuring adequate water temperature and showerhead mobility for bathing or showering should be addressed.
Disclosures: None
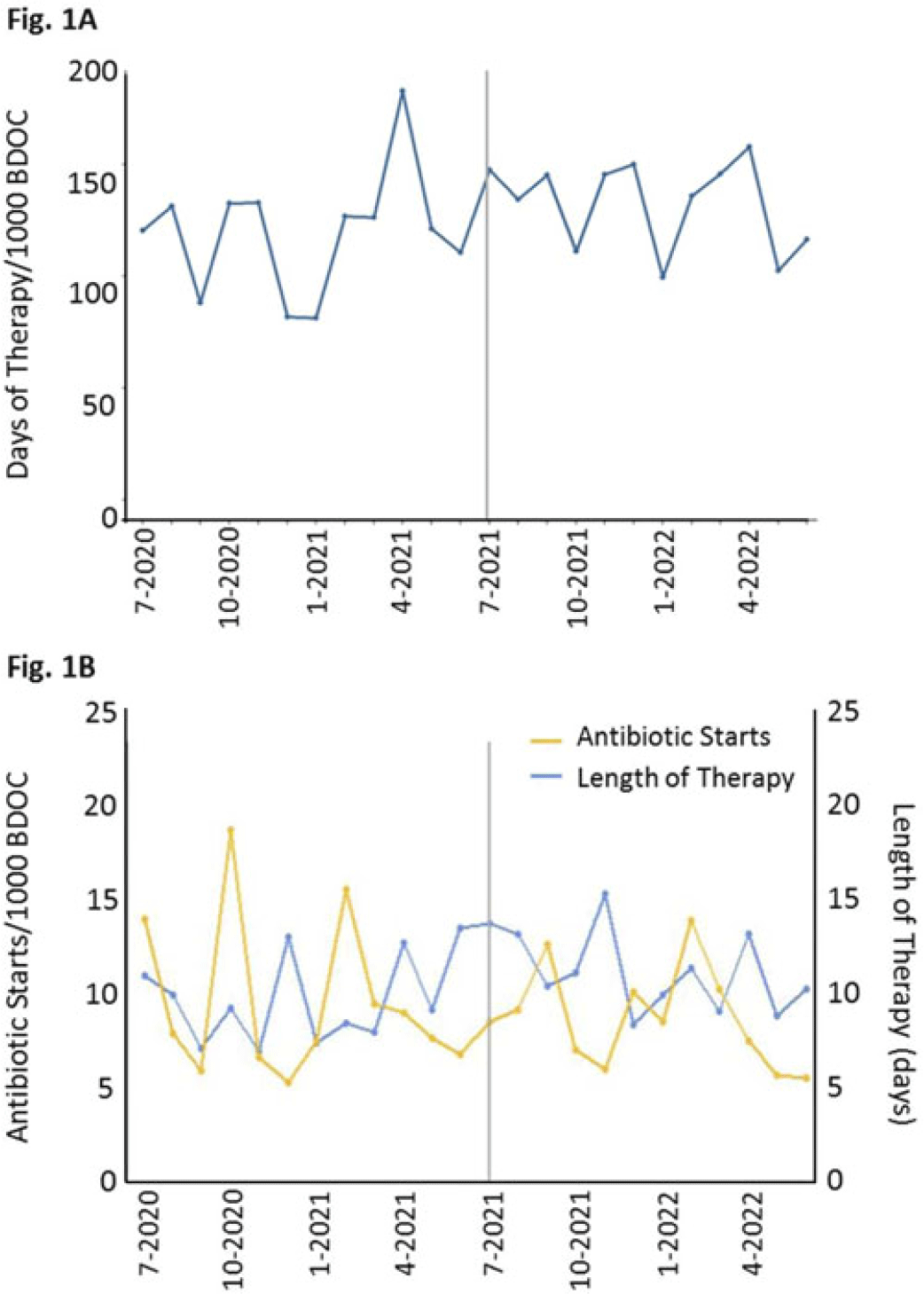
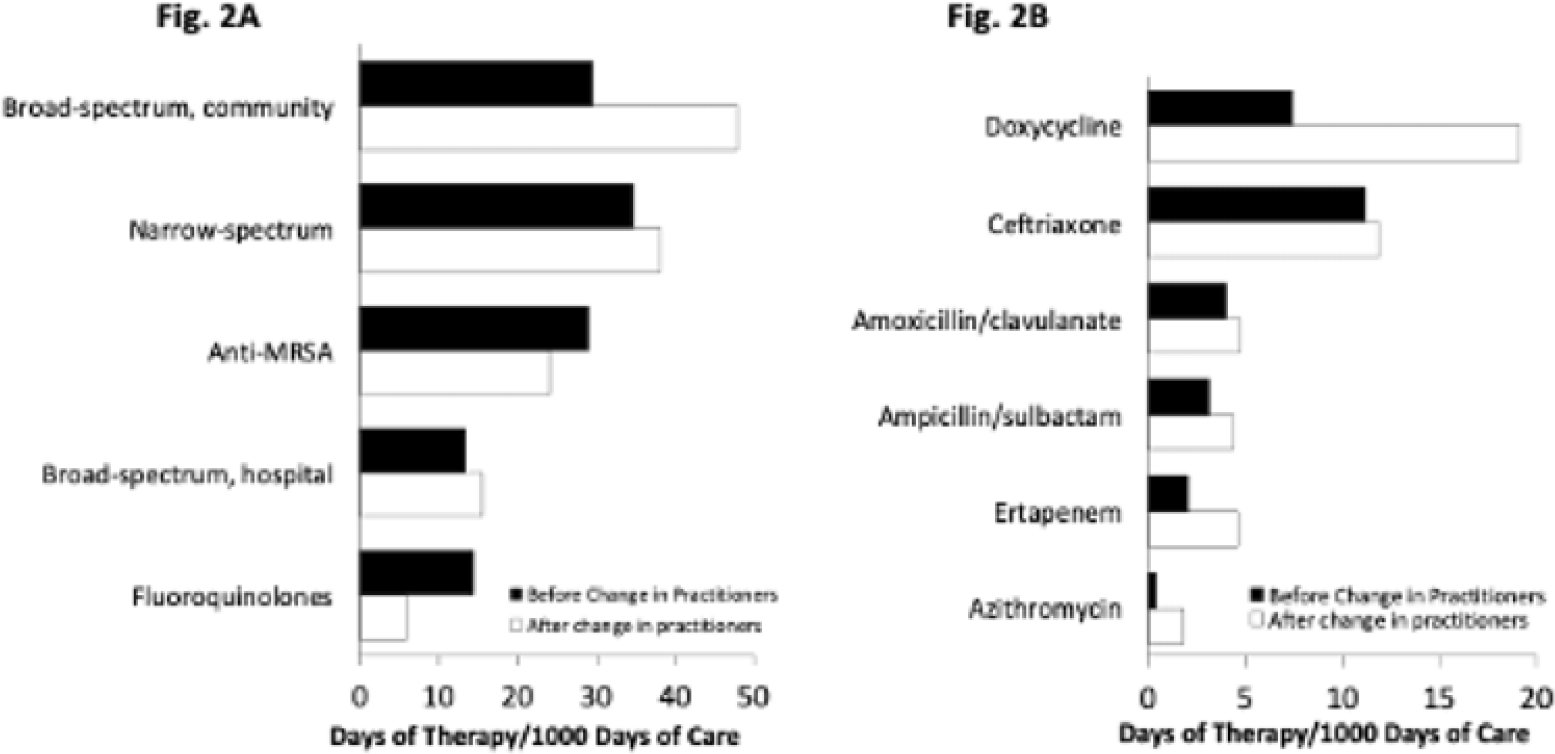
Background: In long-term care settings, practice patterns among practitioners are stronger determinants of antibiotic use than resident characteristics. In July 2021, hospitalists from the acute medicine service replaced geriatricians and assumed the care of residents in a 110-bed community living center (CLC) at a large academic Veterans Affairs (VA) medical center. We assessed changes in antibiotic use associated with that change of practitioners to guide stewardship efforts. We hypothesized that antibiotic use in the CLC would shift, reflecting the practice pattern of practitioners accustomed to treating patients in acute-care settings. Methods: We conducted a retrospective cohort study from July 1, 2020, through June 30, 2022, 1 year before and after the change of practitioners on July 1, 2021. We assessed resident characteristics and the following metrics of antibiotic use at monthly intervals: days of therapy (DOT) per 1,000 bed days of care (BDOC), antibiotic starts per 1,000 BDOC, and mean length of therapy (LOT) in days. We also compared the DOT per 1,000 BDOC for various antibiotics, in groups and individually. Results: In the years before and after the change of practitioners on July 1, 2021, the characteristics of CLC residents were comparable. Before and after July 1, 2021, monthly DOT per 1,000 BDOC (Fig. 1A), antibiotic starts per 1,000 BDOC, and mean LOT (Fig. 1B) were similar. After July 1, 2021, the use of fluoroquinolones decreased (14.31 vs 5.83 DOT per 1,000 BDOC; P < .01), and variations in anti-MRSA, narrow-spectrum, and broad-spectrum hospital agents were small, whereas the use of broad-spectrum community agents increased (29.42 vs 47.81 DOT per 1,000 BDOC; P < .01) (Fig. 2A). Within this group, there was increased use of doxycycline (7.42 vs 19.13 DOT per 1,000 BDOC; P < .01), ertapenem (2.03 vs 4.58 DOT per 1,000 BDOC; P < .01), and, modestly, azithromycin (0.40 vs 1.80 DOT per 1,000 BDOC) (Fig. 2B). Conclusions: The overall use of antibiotics, as measured by DOT, antibiotic starts, and LOT did not change after hospitalists assumed care of CLC residents. However, a notable decrease was observed in the use of fluoroquinolones, and an increase was observed in the use of doxycycline and ertapenem. Stewardship that is tailored to the type of provider and incorporates their practice patterns is needed to reinforce the prudent use of antibiotics.
Disclosures: None
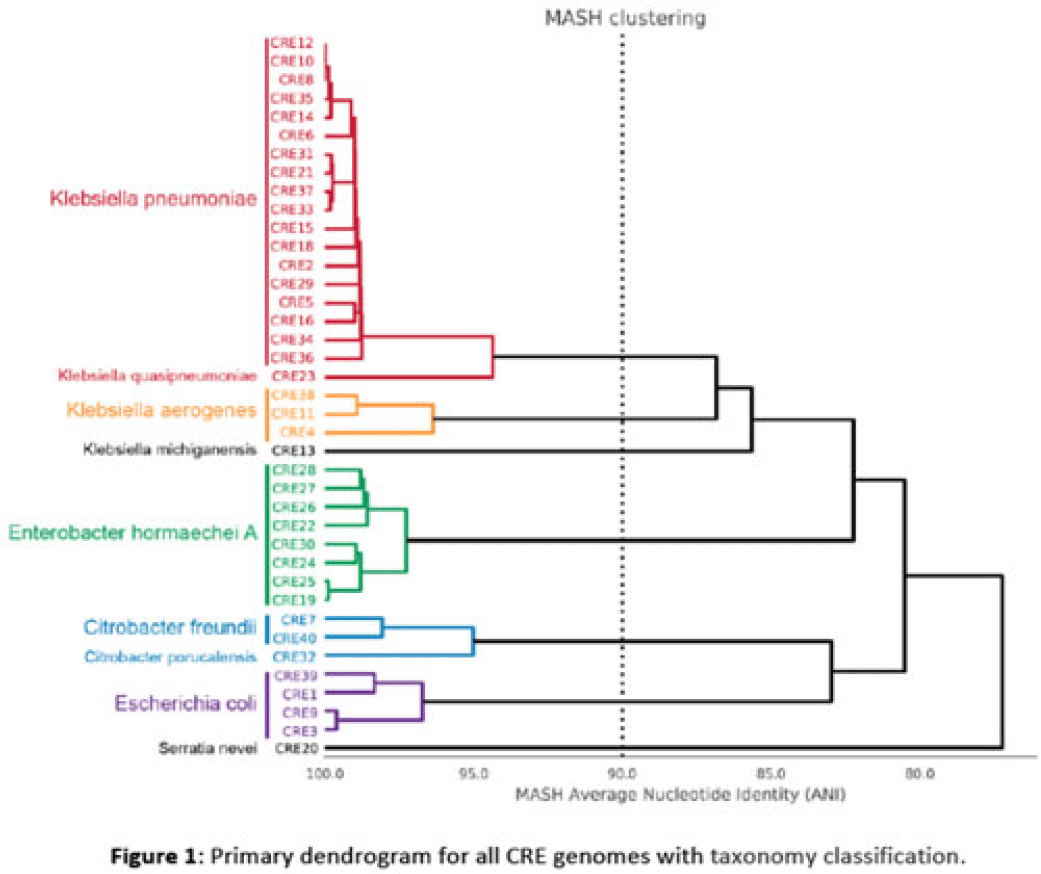
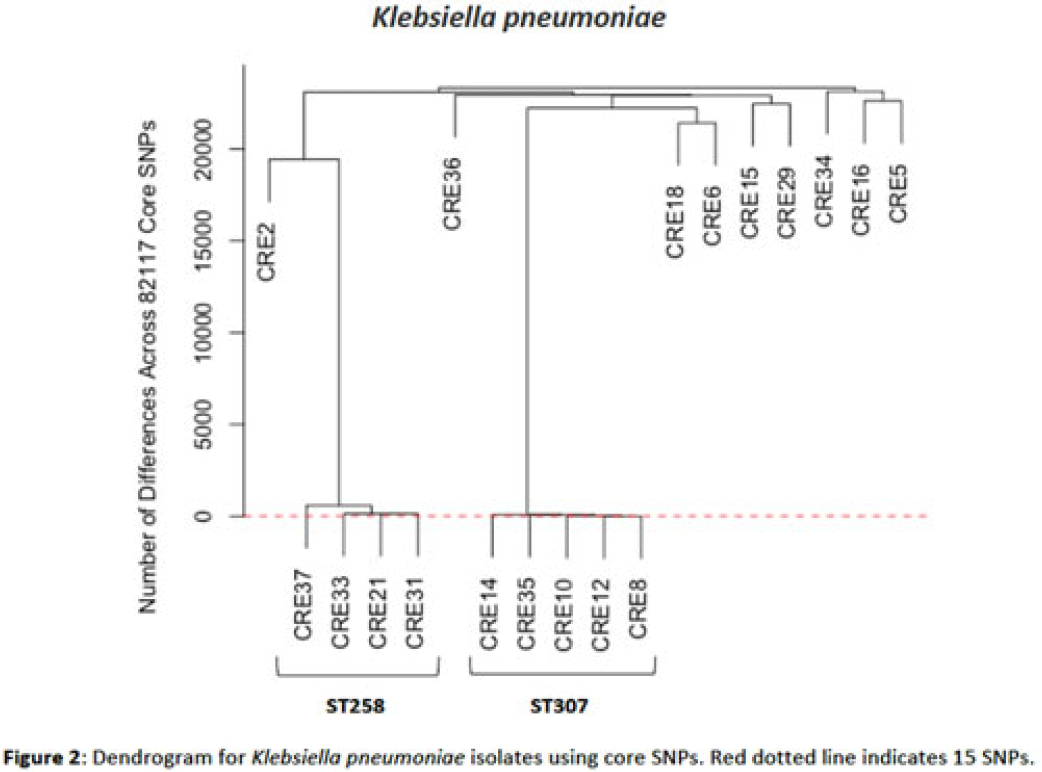
Background: Multidrug-resistant organisms (MDROs) are increasingly implicated in nosocomial outbreaks worldwide. We evaluated whole-genome sequencing (WGS) as an adjunctive epidemiological tool to identify infection clusters and MDRO transmission in the healthcare setting. Methods: Clinical isolates of carbapenem-resistant Enterobacterales (CRE) from July 1, 2021, to June 30, 2022, underwent Illumina WGS. Assembled genomes were taxonomically classified with GTDB-Tk software and were typed using multilocus sequence typing (MLST). Average nucleotide identity (ANI) was calculated between genomes. Numbers of differences among core single-nucleotide polymorphisms (SNPs) were calculated for pairs within taxonomic groups, and the data were evaluated in the context of patient dates and locations of care obtained from the electronic medical record. Results: In total, 39 CRE isolates underwent WGS (Fig. 1). Klebsiella pneumoniae represented the largest number of isolates (n = 18). Using MLST, 2 distinct groups of K. pneumoniae were identified (ST307 and ST258) with 5 and 4 isolates, respectively (Fig. 2). Within ST307, SNP differences ranged between 8 and 115. 3 isolates (CRE8, CRE10, and CRE12) were collected within 4 weeks of each other and had ≤26 pairwise SNP differences. Notably, CRE8 and CRE10 were located on the same unit at the same time and used the same MRI scanner on the same day. CRE35 had >95 SNP differences and was admitted 8 months prior to others in ST307 but had surgery in the same OR as CRE8. Within ST258, pairwise comparison of samples revealed 139–588 SNP differences. CRE21, CRE31, and CRE33 had SNP differences of ≤150. These patients were in the same hospital room (CRE33 and CRE21) and unit (CRE31 and CRE33), but they did not overlap temporally. CRE37 had >580 SNP differences, with no overlap in hospitalization dates or locations with other patients. Conclusions: Two closely related K. pneumoniae isolate populations were identified using WGS. Strong temporal and spatial commonalities were identified among isolates with few SNP differences. Isolate pairs with intermediate SNP differences shared spatial commonalities, suggesting possible indirect transmission between patients. No common exposures were identified for pairs with large numbers of SNP differences. WGS is an evolving tool to detect outbreak clonal populations of MDRO not identified through traditional epidemiologic techniques. WGS can provide insight into transmission patterns and the role of environmental contamination in propagating these nosocomial infections. More studies are needed to define the role and clinical significance of isolates with intermediate SNP differences in transmission of these pathogens between hosts and the healthcare environment.
Disclosures: None
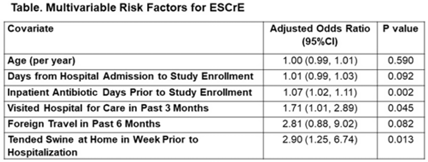
Background: The epidemiology of extended-spectrum cephalosporin-resistant Enterobacterales (ESCrE) in hospitalized patients in low- and middle-income countries (LMICs) is poorly described. Although risk factors for ESCrE clinical infection have been studied, little is known of the epidemiology of ESCrE colonization. Identifying risk factors for ESCrE colonization, which can predispose to infection, is therefore critical to inform antibiotic resistance reduction strategies. Methods: This study was conducted in 3 hospitals located in 3 districts in Botswana. In each hospital, we conducted ongoing surveillance in sequential units hospitalwide. All participants had rectal swabs collected which were inoculated onto chromogenic media followed by confirmatory testing using MALDI-TOF MS and VITEK-2. Data were collected via interview and review of the inpatient medical record on demographics, comorbidities, antibiotic use, healthcare exposures, invasive procedures, travel, animal contact, and food consumption. Participants with ESCrE colonization (cases) were compared to noncolonized participants (controls) using bivariable and multivariable analyses to identify risk factors for ESCrE colonization. Results: Enrollment occurred from January 15, 2020, to September 4, 2020, and 469 participants were enrolled. The median age was 42 years (IQR, 31–58) and 320 (68.2%) were female. The median time from hospital admission to date of sampling was 5 days (IQR, 3–12). There were 179 cases and 290 controls (ie, 38.2% of participants were ESCrE colonized). Independent risk factors for ESCrE colonization were a greater number of days on antibiotic, recent healthcare exposure, and tending swine prior to hospitalization. (Table). Conclusions: ESCrE colonization among hospitalized patients was common and was associated with several exposures. Our results suggest prior healthcare exposure may be important in driving ESCrE. The strong link to recent antibiotic use highlights the potential role of antibiotic stewardship interventions for prevention. The association with tending swine suggests that animal husbandry practices may play a role in community exposures, resulting in colonization detected at the time of hospital admission. These findings will help to inform future studies assessing strategies to curb further emergence of hospital ESCrE in LMICs.
Disclosures: None
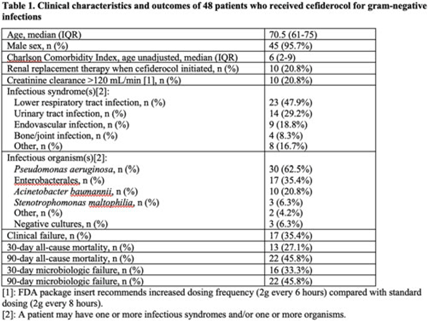
Background: Cefiderocol is a novel siderophore cephalosporin with broad-spectrum activity. In the CREDIBLE-CR phase 3 clinical trial examining treatment of carbapenem-resistant gram-negative infections, cefiderocol had similar clinical and microbiological efficacy compared to the best available therapy, but the mortality rate was unexpectedly higher in the cefiderocol group. We investigated the postapproval, real-world clinical outcomes of cefiderocol therapy. Methods: We conducted a prospective, observational study of patients who received cefiderocol for at least 2 days within the Veterans’ Health Administration (VHA) between the date of approval by the US Food and Drug Administration (FDA), November 14, 2019, and August 31, 2022. Types of infections were defined by NHSN criteria. Clinical failure was a composite outcome based on type of infection including survival (30- and 90-day mortality) and resolution of signs and symptoms of infection. Microbiologic failure was defined as culturing the same organism, as defined by the CDC NHSN, at least 7 days after the start of cefiderocol. Structured data were sourced from the VHA Corporate Data Warehouse, and each eligible episode underwent manual chart review. Results: During the study period, 8,763,652 patients across 132 VA medical centers received 1,142,940,842 prescriptions (not limited to antibiotics). Overall, 48 unique individuals had received cefiderocol, with 48 cefiderocol courses prescribed. Patients had a median age of 70.5 years (range, 61–75), and a median Charlson comorbidity score of 6 (range, 2–9). The most common infectious syndromes were lower respiratory tract infection in 23 (47.9%) of these 48 patients and urinary tract infection in 14 (29.2%) of these patients. The most common pathogens cultured were P. aeruginosa in 30 patients (62.5%), Enterobacterales in 17 patients (35.4%), and A. baumannii in 10 patients (20.8%). The clinical failure rate was 35.4% (17 of 48), and 15 (88.2%) of these 17 patients died within 3 days of clinical failure. The 30-day and 90-day microbiologic failure rates were 33.3% (16 of 48) and 45.8% (22 of 48), respectively. The 30-day and 90-day all-cause mortality rates were 27.1% (13 of 48) and 45.8% (22 of 48), respectively (Table 1). Conclusions: Our study cohort included older individuals with multiple comorbidities who were treated with cefiderocol mainly for lower respiratory tract and urinary tract infections, with Pseudomonas aeruginosa as the main causative pathogen. Clinical and microbiologic failure were seen in>30% of patients, and >40% of these patients died within 90 days. These data contribute to the growing body of literature on the real-world use of cefiderocol and provide outcome data on clinical failure, microbiologic failure, and mortality.
Financial support: This study was supported by the Department of Veterans Affairs Clinical Science Research and Development (VA CSRD grant no. IK2 CX001981).
Disclosures: None
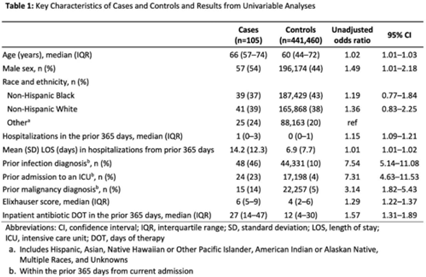
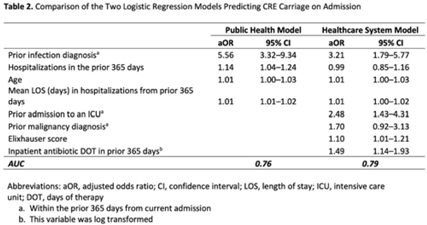
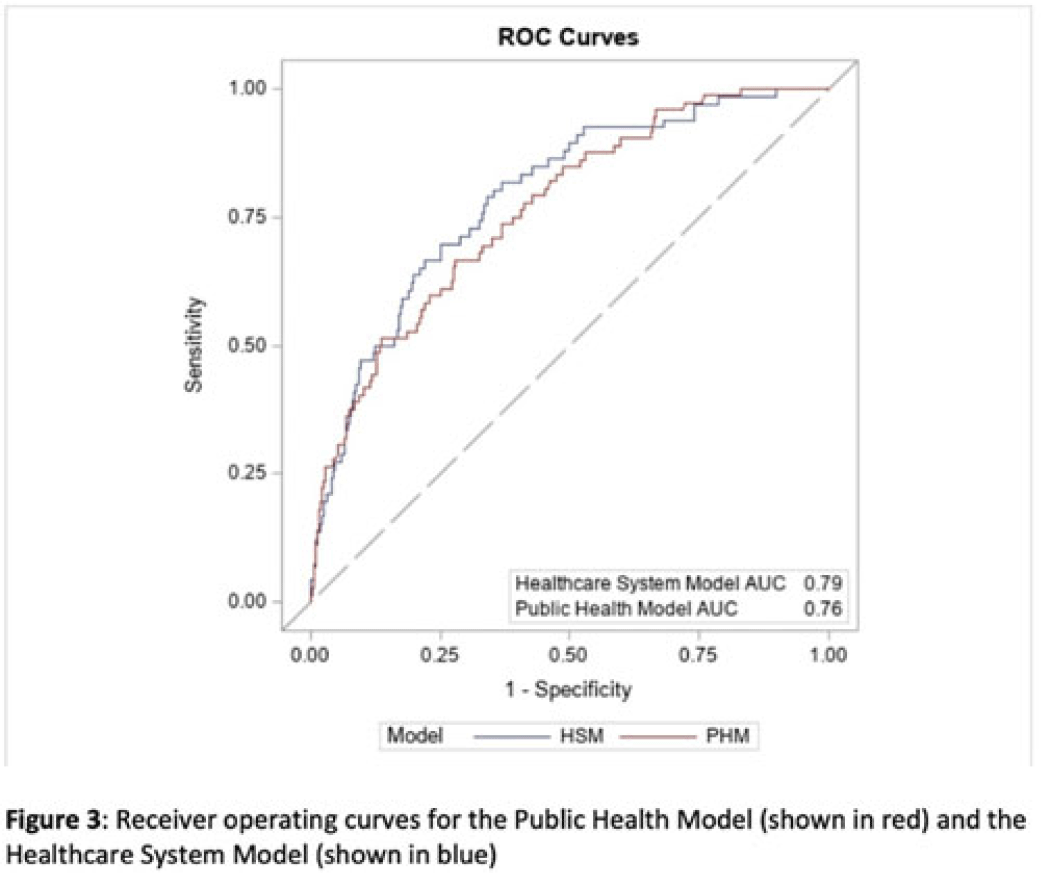
Background: Prompt identification of patients colonized or infected with carbapenem-resistant Enterobacterales (CRE) upon admission can help ensure rapid initiation of infection prevention measures and may reduce intrafacility transmission of CRE. The Chicago CDC Prevention Epicenters Program previously created a CRE prediction model using state-wide public health data (doi: 10.1093/ofid/ofz483). We evaluated how well a similar model performed using data from a single academic healthcare system in Atlanta, Georgia, and we sought to determine whether including additional variables improved performance. Methods: We performed a case–control study using electronic medical record data. We defined cases as adult encounters to acute-care hospitals in a 4-hospital academic healthcare system from January 1, 2014, to December 31, 2021, with CRE identified from a clinical culture within the first 3 hospital days. Only the first qualifying encounter per patient was included. We frequency matched cases to control admissions (no CRE identified) from the same hospital and year. Using multivariable logistic regression, we compared 2 models. The “public health model” included 4 variables from the Chicago Epicenters model (age, number of hospitalizations in the prior 365 days, mean length of stay in hospitalizations in the prior 365 days, and hospital admission with an infection diagnosis in the prior 365 days). The “healthcare system model” added 4 additional variables (admission to the ICU in the prior 365 days, malignancy diagnosis, Elixhauser score and inpatient antibiotic days of therapy in the prior 365 days) to the public health model. We used billing codes to determine Elixhauser score, malignancy status, and recent infection diagnoses. We compared model performance using the area under the receiver operating curve (AUC). Results: We identified 105 cases and 441,460 controls (Table 1). CRE was most frequently identified in urine cultures (46%). All 4 variables included in the public health model and the 4 additional variables in the healthcare system model were all significantly associated with being a case in unadjusted analyses (Table 1). The AUC for the public health model was 0.76, and the AUC for the healthcare system model was 0.79 (Table 2; Fig. 1). In both models, a prior admission with an infection diagnosis was the most significant risk factor. Conclusions: A modified CRE prediction model developed using public health data and focused on prior healthcare exposures performed reasonably well when applied to a different academic healthcare system. The addition of variables accessible in large healthcare networks did not meaningfully improve model discrimination.
Disclosures: None
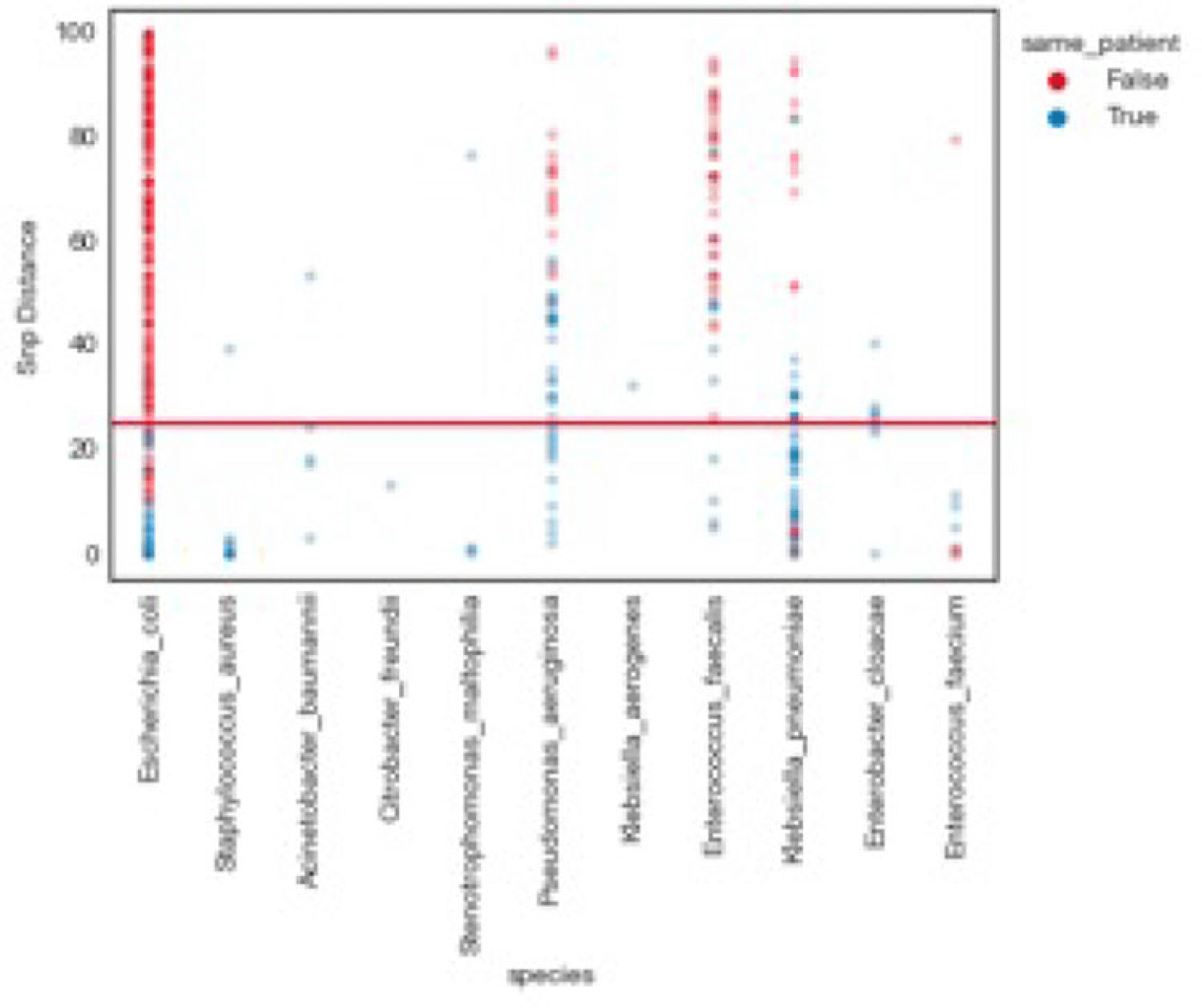
Background: Traditional hospital outbreak-detection methods are typically limited to select multidrug-resistant pathogens in a single unit, which can miss transmission of many medically important healthcare-transmissible pathogens. Whole-genome sequencing (WGS) enables comprehensive genomic resolution for accurate identification of clonal transmission. Previously, lack of scalability limited the use of WGS for hospital surveillance. Methods: We conducted prospective surveillance of select bacteria from all inpatient clinical cultures plus all bacteria from clinical cultures from ICUs and oncology units at the University of California Irvine (UCI) Clinical Microbiology Laboratory from September 2021 to February 2022. Due to pandemic stressors, this pilot test was a prelude to a real-time demonstration project. Its goal was to demonstrate the efficiency and scalability of the WGS platform when receiving samples monthly and analyzing results quarterly without the intent for real-time response. Bacterial isolates slated for discard were collected weekly and sent monthly to Day Zero Diagnostics for sequencing. In total, 1,036 samples from 926 patients were analyzed for genomic relatedness, a scalable and automated analysis pipeline already in use for rapid (days) characterization of genomic-relatedness in small and large sets of isolates. Mapping and SNP calling was performed against high-quality, best-match reference genomes. Sets of samples with pairwise distance of 2 persons with genomically related isolates and were denoted as “clusters.” Separately, we also investigated within-patient diversity by quantifying the genomic relatedness of isolates collected from individual patients. Results: Isolates represented 28 distinct species. We identified 10 Escherichia coli clusters (range, 2–4 patients; median, 2 patients), 2 Klebsiella pneumoniae clusters (range, 2–4 patients), and 1 Enterococcus faecium cluster (3 patients). All but 1 involved genomically matched isolates from multiple hospital locations. There were 4 Escherichia coli ST131 clusters spanning 4 months, including 1 with 4 patients across 3 different hospital locations. At a species level, there were distinct differences between the observed SNP distances between samples isolated from the same versus different patients (Fig. 1). All identified clusters had not been flagged by routine outbreak detection methods used by the UCI infection prevention program. Conclusions: Comprehensive WGS-based surveillance of hospital clinical isolates identified multiple potential transmission events between patients not in the same unit at the time cultures were taken. Combining WGS detection and real-time epidemiologic investigation may identify new avenues of transmission risk and could provide early warnings of clonal transmission to prevent larger outbreaks. High-volume surveillance of hospital isolates can also provide species- and context-specific clonality.
Financial support: This study was funded by Day Zero Diagnostics.
Disclosures: None
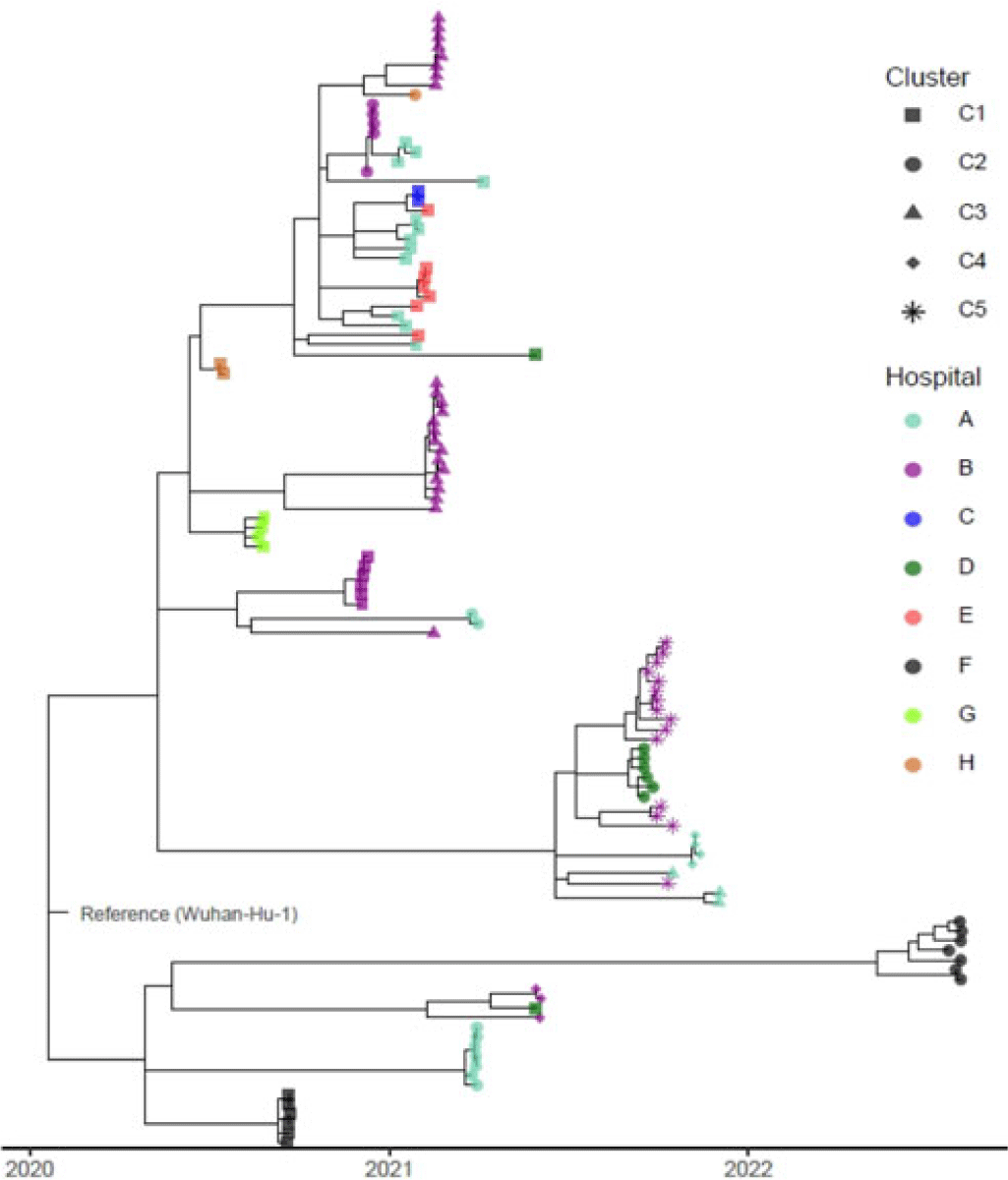
Background: Identifying and interrupting transmission of severe acute respiratory syndrome coronavirus 2 and resulting disease (COVID-19) in acute-care settings can be challenging due to incubation period, asymptomatic infection, and prevalent community disease. To elucidate routes of infection and interrupt COVID-19 outbreaks with uncertain epidemiological chains of transmission, UPMC utilized reactive whole-genome sequencing (WGS) of viral specimens. Methods: UPMC infection prevention teams identified healthcare-associated COVID-19 clusters with uncertain transmission pathways among patients and/or healthcare personnel (HCP) in acute-care hospitals. Nasopharyngeal samples preserved in viral transport media were obtained for genetic analyses. Nucleic acids were extracted and WGS libraries were prepared by targeted enrichment or multiplex PCR methodologies. Resulting sequencing reads were aligned to the Wuhan-1 reference genome, followed by identification of single-nucleotide polymorphisms (SNPs) among the genomes and construction of a phylogenetic tree. Specimens were considered genetically similar if there were ≤2 SNP differences between viral genomes within a cluster. Results: Between May 2020 until August 2022, infection prevention teams requested WGS for 17 healthcare-associated clusters of COVID-19 involving 182 individuals across 8 UPMC facilities (median outbreak size, 9 individuals; range, 2–26). Of the 182 individuals, 36 lacked clinical specimens and 30 did not pass WGS quality-control criteria of ≥95% of the reference genome with a minimum of 10× coverage. Of the 116 sequenced genomes, 94 (81%) had virus genetically similar to ≥1 other specimen, including 87 (83.6%) of 104 patient viruses and 7 (58.3%) of 12 HCP viruses, comprising 22 clusters (Fig. 1). The remaining 22 (20.6%) specimens were genetically unrelated. In total, 16 (94.1%) of the 17 epidemiologically identified clusters had 2 or more individuals with a genetically similar virus. Also, 7 (41.1%) of these clusters had genetically similar viral genomes for every individual within each cluster. Also, 9 (52.9%) clusters contained both genetically related and unrelated specimens: 5 of these had more complex genomic profiles (including 4 clusters containing 2 distinct subclusters of ≥2 genetically related viruses) and 1 cluster contained 3 subclusters of ≥2 genetically related viruses. In the outbreak with 3 clusters, 3 SNPs separated specimens from 2 temporally proximal clusters, suggesting possible propagation between clusters (cluster B-3 in Fig. 1). Conclusions: WGS can complement traditional epidemiological investigations of healthcare-associated COVID-19 outbreaks, revealing complex transmission dynamics. Future investigations will characterize the impact of WGS on determining specific transmission pathways in acute-care facilities.
Disclosures: None
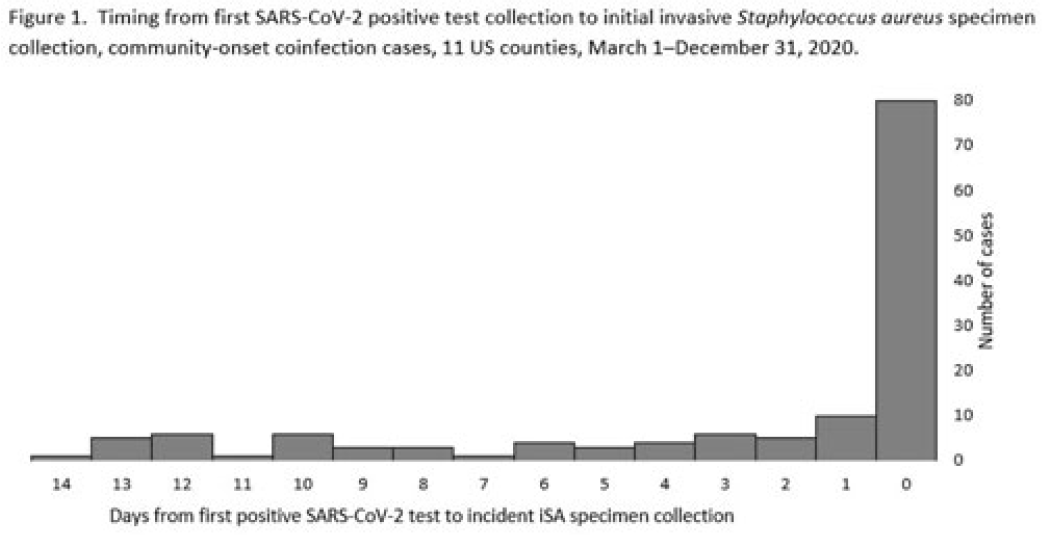
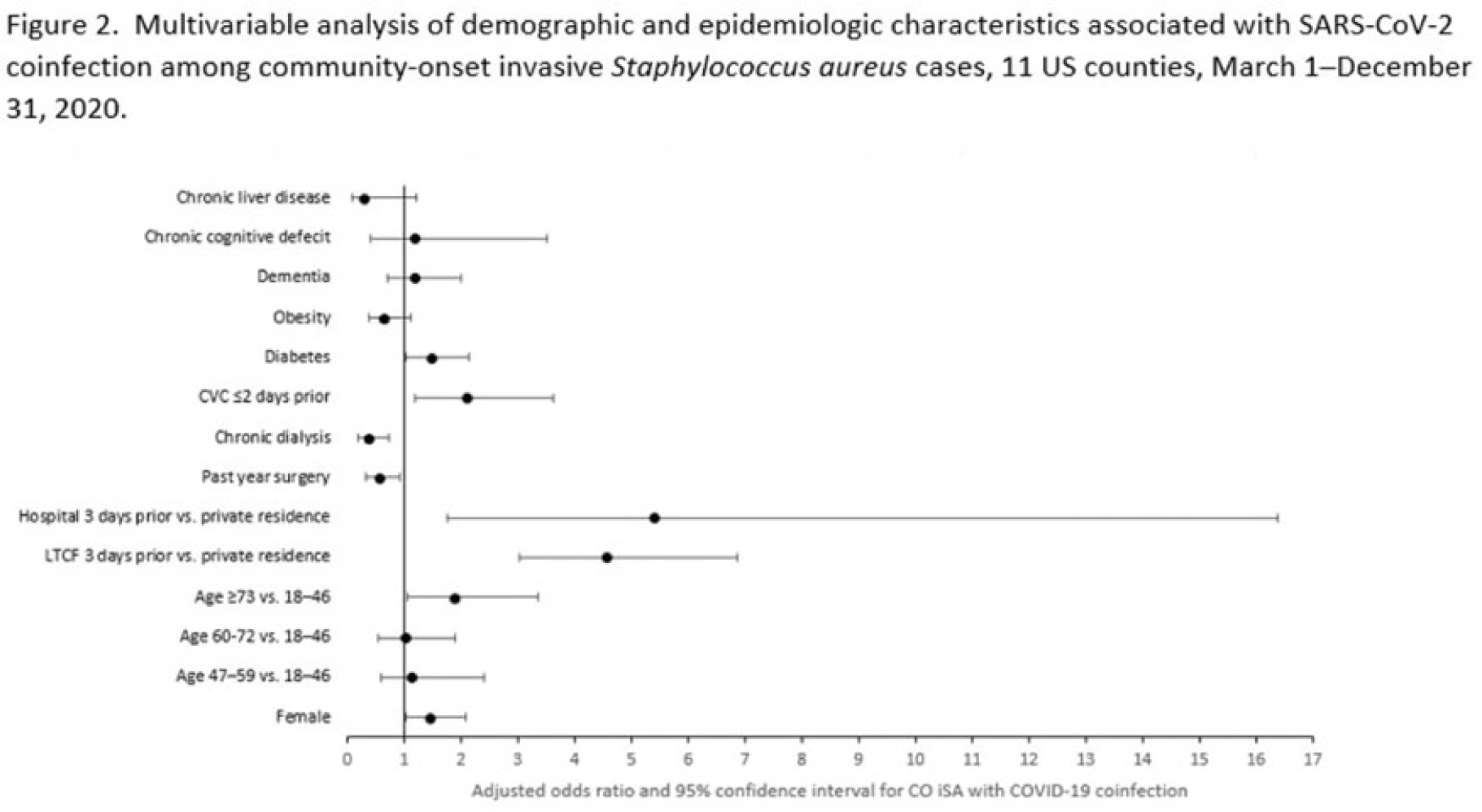
Background: Previous analyses describing the relationship between SARS-CoV-2 infection and Staphylococcus aureus have focused on hospital-onset S. aureus infections occurring during COVID-19 hospitalizations. Because most invasive S. aureus (iSA) infections are community-onset (CO), we characterized CO iSA cases with a recent positive SARS-CoV-2 test (coinfection). Methods: We analyzed CDC Emerging Infections Program active, population- and laboratory-based iSA surveillance data among adults during March 1–December 31, 2020, from 11 counties in 7 states. The iSA cases (S. aureus isolation from a normally sterile site in a surveillance area resident) were considered CO if culture was obtained <3 days after hospital admission. Coinfection was defined as first positive SARS-CoV-2 test ≤14 days before the initial iSA culture. We explored factors independently associated with SARS-CoV-2 coinfection versus no prior positive SARS-CoV-2 test among CO iSA cases through a multivariable logistic regression model (using demographic, healthcare exposure, and underlying condition variables with P<0.25 in univariate analysis) and examined differences in outcomes through descriptive analysis. Results: Overall, 3,908 CO iSA cases were reported, including 138 SARS-CoV-2 coinfections (3.5%); 58.0% of coinfections had iSA culture and the first positive SARS-CoV-2 test on the same day (Fig. 1). In univariate analysis, neither methicillin resistance (44.2% with coinfection vs 36.5% without; P = .06) nor race and ethnicity differed significantly between iSA cases with and without SARS-CoV-2 coinfection (P = .93 for any association between race and ethnicity and coinfection), although iSA cases with coinfection were older (median age, 72 vs 60 years , P<0.01) and more often female (46.7% vs 36.3%, P=0.01). In multivariable analysis, significant associations with SARS-CoV-2 coinfection included older age, female sex, previous location in a long-term care facility (LTCF) or hospital, presence of a central venous catheter (CVC), and diabetes (Figure 2). Two-thirds of co-infection cases had ≥1 of the following characteristics: age > 73 years, LTCF residence 3 days before iSA culture, and/or CVC present any time during the 2 days before iSA culture. More often, iSA cases with SARS-CoV-2 coinfection were admitted to the intensive care unit ≤2 days after iSA culture (37.7% vs 23.3%, P<0.01) and died (33.3% vs 11.3%, P<0.01). Conclusions: CO iSA patients with SARS-CoV-2 coinfection represent a small proportion of CO iSA cases and mostly involve a limited number of factors related to likelihood of acquiring SARS-CoV-2 and iSA. Although CO iSA patients with SARS-CoV-2 coinfection had more severe outcomes, additional research is needed to understand how much of this difference is related to differences in patient characteristics.
Disclosures: None
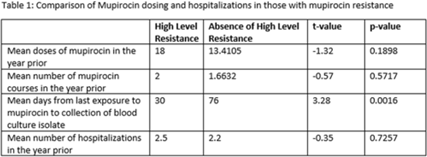
Methicillin-resistant Staphylococcus aureus (MRSA) is a common etiology of hospital-acquired infections (HAIs). One strategy to reduce HAIs due to MRSA involves a multistep decolonization process. This often involves nasal application of mupirocin 2% ointment. In our institution, when individuals meet criteria for decolonization, we recommend 5 days of treatment given twice daily. High levels of mupirocin resistance have been reported in some hospital systems, with >80% of tested isolates being resistant. To better understand our resistance levels, we selected 238 MRSA isolates from blood cultures to be tested for mupirocin resistance to correlate the presence of resistance and use of mupirocin for decolonization. We choose to assess MRSA blood isolates rather than nasal swabs given that we aim to prevent invasive MRSA infections, including blood stream infections, with decolonization. The blood cultures were collected from 11 acute-care facilities within our system from March 2021 through June 2022. High-level resistance was defined as an MIC >1,024 μg/mL according to Clinical and Laboratory Standards Institute guidelines. Of those, 7.14% showed high level resistance, and 76.47% occurred in those who were exposed to mupirocin and 23.53% occurred in those without mupirocin exposure (P = .0094). On average, those with high-level resistance had had more recent exposure to mupirocin compared to those without resistance, which was statistically significant. Also, those with high resistance, on average, received more doses of mupirocin, although this was not statistically significant. Conclusions: More recent and higher number of doses of mupirocin were associated with the development of resistance, which is consistent with what we know from pharmacodynamics of antibiotic resistance with other agents. These findings may be particularly important for those patients who have frequent hospitalizations and often require decolonization. Understanding baseline mupirocin resistance levels in an institution can assist with determining decolonization strategies.
Disclosures: None
Background: Directing COVID-19 diagnostic testing to healthcare workers (HCWs) who are likely to be infected has potential to reduce staffing shortages and decrease opportunity for in-hospital transmission; however, HCWs with COVID-19 may exhibit a range of symptoms. We assessed the burden of symptoms in relation to cycle threshold (Ct) values as a surrogate for viral shedding in vaccinated healthcare workers. Methods: We retrospectively reviewed employee health records of COVID-19–vaccinated employees who tested positive for SARS-CoV-2 between December 2020 and January 2022 at 2 academic hospital systems. We reviewed demographic data, reasons for testing including symptoms, exposure history, medical history, vaccination dates, Ct values, and genotypes when available. We compared mean Ct values between symptomatic and minimally symptomatic cases using independent sample t tests. Patients were defined as minimally symptomatic if they had no symptoms or a single symptom that is not cough, fever, or anosmia at the time of testing. Patients were defined as more symptomatic if they reported >1 symptom or cough, fever, or anosmia. Results: In total, 298 HCWs tested positive for COVID-19. Most positive cases were female (73%), white (78%), and had patient-facing roles (77%). Genotypic testing (n = 109) revealed that most genotypes belonged to the SARS-CoV-2 delta variant (AY lineages, B1.617.2). More cases were minimally symptomatic (62%) than were more symptomatic (38%). None required hospitalization during the study period. Mean Ct values (n = 141) showed no significant difference between more symptomatic and minimally symptomatic cases (19.8 vs 20.6; P = .40) (Fig. 1). Also, there was no significant difference in mean Ct value, comparing those with vaccination 90 days prior to positive (20.52 vs 19.88; P = .537). Conclusions: Our study shows no significant difference in cycle threshold values between minimally symptomatic and more symptomatic infections in vaccinated HCWs. In addition, HCWs exhibit high viral load even when infected within 90 days after vaccination. When considering whether to attend work, HCWs should be aware that mild symptoms and recent vaccination do not necessarily reflect low transmissibility and that they should follow CDC guidance regarding when to return to work.
Disclosures: None
