


The value of human nutritional studies is largely dependent on the accuracy of the dietary information used. In particular, many epidemiological studies are evaluated by the accuracy of their assessment of an individual's habitual diet. Long-term dietary habits are often assessed using dietary questionnaires(Reference Willett1); however, given that food culture and dietary habits vary by country, these need to be developed specifically for each country(Reference Cade, Thompson and Burley2). In addition, because dietary questionnaires do not necessarily estimate true food intake, their validity needs to be evaluated. The most common way to do this is to assess actual intakes for a limited number of days using dietary records and a 24 h dietary recall(Reference Willett1–Reference Cade, Burley and Warm3).
Sasaki et al.(Reference Sasaki, Yanagibori and Amano4) developed a comprehensive self-administered diet history questionnaire (DHQ) that uses both food frequency methodology (consumption frequency and portion size) and diet history methodology (e.g. assessment of cooking methods and staple foods for each meal separately) to estimate the dietary intakes of 150 food and beverage items. This DHQ has been validated using the dietary record(Reference Sasaki, Yanagibori and Amano4), 24 h urine(Reference Sasaki, Yanagibori and Amano5), serum(Reference Sasaki, Ushio and Amano6) and doubly labelled water(Reference Okubo, Sasaki and Rafamantanantsoa7) methods, and has been used in many epidemiological studies(Reference Miyake, Sasaki and Tanaka8–Reference Okubo, Sasaki and Horiguchi12). However, although useful for epidemiological research, the DHQ takes about 45–60 min to answer, as a result of which shorter dietary assessment tools have been sought.
Recently, the DHQ was shortened to a brief-type self-administered DHQ (BDHQ) that requires approximately 15–20 min to answer. To our knowledge, however, the validity of the DHQ and BDHQ has not been compared. Further, although some studies have compared the validity of the long and short versions of the same questionnaire regarding nutrient intakes(Reference Potischman, Carroll and Iturria13–Reference Talegawkar, Johnson and Carithers15), no study has compared these in terms of food group intakes. Such information would aid in the selection of questionnaires that meet the requirements of the particular study design and information needed.
In the present study, we compared the relative validity of food group intakes derived from the DHQ and BDHQ among healthy men and women in Japan against 16 d semi-weighed dietary records (DR).
Methods
Participants
The present study was conducted in three areas in Japan, namely Osaka (urban), Nagano (rural inland) and Tottori (rural coastal), in consideration of survey feasibility and potential regional differences in food availability and dietary habits. From each area we recruited apparently healthy women aged 30–69 years who were willing to participate with a co-habitating husband, such that each of the 10-year age class strata (30–39, 40–49, 50–59 and 60–69 years) had eight women, without consideration of the age of men. Thus, a total of ninety-six women and ninety-six men were invited. None of the participants was a dietitian, nor were any of them currently receiving (or had recently received) dietary counselling from a doctor or dietitian, nor did they have a history of educational hospitalization for diabetes or nutritional education from a dietitian. Before the study, group orientations were held at which the study purpose and protocol were explained. Written informed consent was obtained from each participant. A total of ninety-two women aged 31–69 years and ninety-two men aged 32–76 years completed four 4 d DR, as well as four DHQ and BDHQ, once in each season, and were included in the present analysis. Body height and weight were measured to the nearest 0·1 cm and 0·1 kg, respectively, with participants wearing light clothing and no shoes. BMI was calculated as body weight in kilograms divided by the square of height in metres (kg/m2).
Four 4 d semi-weighed dietary records
Between November 2002 and September 2003, the participants completed a 4 d DR (covering four non-consecutive days) four times, once in each season, at intervals of approximately 3 months, namely November and December 2002 (autumn), February 2003 (winter), May 2003 (spring) and August and September 2003 (summer; Fig. 1). Each of the four recording days consisted of one weekend day and three weekdays. During the orientation session, local staff, who were registered dietitians, provided written and verbal instructions on how to maintain the dietary records and also provided the participants with a sample of a completed record. Each couple was given recording sheets and a digital scale (model KD-173, Tanita, Tokyo, Japan; ±2 g precision for 0–250 g and ±4 g precision for 251–1000 g), instructed on how to assign weights for each food and drink and asked to record and assign weights for all food and drinks consumed on the recording day. When assigning weights was difficult (e.g. eating out), they were instructed to record the size and quantity of food eaten using household measures in as much detail as possible. For each recording day, the participants were asked to fax the completed forms to the local staff, who reviewed the forms and where necessary asked the participants to add to or modify the record by telephone or fax. In some cases, the responses were handed over directly to the staff.
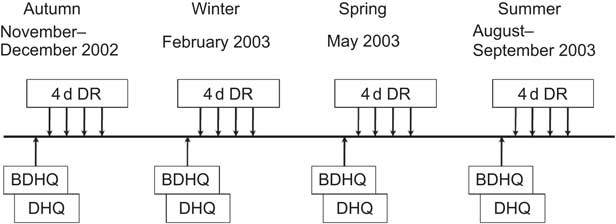
Fig. 1 Schedule for the present validation study (DR, semi-weighed dietary record; DHQ, self-administered diet history questionnaire; BDHQ, brief-type DHQ)
All collected records were checked by trained dietitians at each local centre and then at the data centre for dietary records. The coding of records and the conversion of other measurements of quantities into grams were performed by trained dietitians at the survey centre in accordance with uniform procedures. A total of 1299 food and beverage items appeared in the dietary records.
Self-administered diet history questionnaire
The participants answered the DHQ four times, once in each season, at intervals of approximately 3 months from November 2002 to September 2003 (Fig. 1). In each season, the DHQ was answered approximately 2 d before the start of the dietary recording period. Responses to the DHQ were checked at least twice for completeness by dietitians. When missing answers or logical errors were identified, the participants were asked to complete the questions again.
The DHQ is a sixteen-page semi-quantitative questionnaire that assesses dietary habits during the previous month. Participants are required to answer the questions themselves in principle; however, if self-completion is difficult, they are advised to seek help from the person who usually prepares their meals. The DHQ consists of the following seven sections: (i) general dietary behaviour, including preference for seasonings; (ii) usual cooking methods for fish and shellfish, meat, eggs and vegetables; (iii) consumption frequency and amount of six alcoholic beverages; (iv) consumption frequency and semi-quantitative portion size of selected food and non-alcoholic beverage items; (v) type, frequency and quantity of dietary supplements; (vi) consumption frequency and semi-quantitative portion size of staple foods (rice, other grains, noodles, bread and other wheat products), soup for noodles and miso (fermented soyabean paste) soup, assessed for each eating occasion (breakfast, lunch, dinner and snacks) separately, with questions on the size of the bowl or cup usually used for rice and miso soup; and (vii) open-ended items for foods consumed more than once weekly but not appearing in the DHQ. The food and beverage items were selected as foods commonly consumed in Japan, mainly from a food list used in the National Nutrition Survey of Japan, whereas standard portion sizes and sizes of bowls and cups for rice and miso soup were derived mainly from several recipe books for Japanese dishes(Reference Sasaki, Yanagibori and Amano4).
Estimates of dietary intake for a total of 150 food and beverage items were calculated using an ad hoc computer algorithm (including weighting factors) for the DHQ in accordance with the following procedures. For most items (145 items listed in sections 3, 4 and 6), dietary intake was calculated on the basis of the reported consumption frequency and portion size according to a semi-quantitative food frequency methodology. Dietary intakes of the remaining five items (four seasonings used during cooking and soya sauce) were estimated according to a diet history method, using the qualitative information in sections 1 and 2 and the quantitative information in section 4. Information on dietary supplements (section 5) and data from the open-ended questionnaire items (section 7) were not used in the calculation of dietary intake.
For men, intakes of foods categorized as meat, fish and shellfish, and eggs were calculated as the product of the reported consumption frequency and portion size multiplied by a factor of 1·2 for the following reasons(Reference Murakami, Sasaki and Takahashi16). First, standard portion sizes in the DHQ may be generally those for women, because the recipe books for Japanese dishes from which the standard portion sizes were derived generally show sizes for women, and also because the DHQ was originally developed for women(Reference Sasaki, Yanagibori and Amano4). Second, the possibility of gender differences in portion size is likely to be higher for foods used for the main dish (such as meat, fish and shellfish, and eggs) than for other foods(Reference Ogawa, Tsubono and Nishino17). Finally, intakes of meat, fish and shellfish, and eggs (and rice), but not of other foods, are generally higher in men than in women in Japan(18). Possible gender differences in rice portion size were accounted for by the question on rice bowl or cup size.
Brief-type self-administered diet history questionnaire
All participants were asked to complete the BDHQ at the same time as they completed the DHQ, in the order of BDHQ before DHQ (Fig. 1). Responses to the BDHQ were checked in the same way as those for the DHQ.
The BDHQ is a four-page structured self-administered questionnaire. Although participants are requested to answer the BDHQ themselves in principle, as for the DHQ, if self-completion is difficult, they are advised to seek help from the person who usually prepares their meals. The BDHQ assesses dietary habits during the preceding month, and consists of the following five sections: (i) intake frequency of forty-six food and non-alcoholic beverage items; (ii) daily intake of rice, including type of rice (refined or unrefined, etc), and miso soup; (iii) frequency of drinking alcoholic beverages and amount per drink for five alcoholic beverages; (iv) usual cooking methods; and (v) general dietary behaviour. Most food and beverage items were selected from the food list of the DHQ as those that are very commonly consumed in Japan, with some modifications using a food list used in the National Health and Nutrition Survey of Japan as additional information(Reference Sasaki, Yanagibori and Amano4, 18). Standard portion sizes, and adult sizes of bowls for rice and cups for miso soup, were derived from several recipe books for Japanese dishes.
Estimates of dietary intake for fifty-eight food and beverage items were calculated using an ad hoc computer algorithm (including weighting factors) for the BDHQ according to the following procedures: for most items (forty-six items listed in section 1), dietary intake was calculated on the basis of the reported intake or drinking frequency and the fixed portion size. Because the recipe books from which the standard portion sizes were derived generally showed portion sizes for women, they were used for women. Because no such information was obtained for men, the standard portion sizes for women were multiplied by 1·14 for men in consideration of the estimated energy requirement for men and women and on the basis of additional unpublished information on the differential intakes of rice and main dishes by sex. On the basis of a previous study that reported differential under-reporting of food intakes by food items(Reference Ogawa, Tsubono and Nishino17), as well as on the basis of other unpublished observations, portion sizes were weighted by 1·15 for chicken, pork and beef, squid, octopus, shrimp and clam, canned tuna, oily fish, non-oily fish, tofu and eleven vegetable items, including mushroom and seaweed; by 1·1 for eggs; and by 1·4 for potatoes. For rice and miso from miso soup, dietary intakes were calculated on the basis of the reported number of bowls of rice and cups of miso soup per day and the standard portion sizes of men and women separately. For five alcoholic beverages, dietary intakes were calculated on the basis of the reported drinking frequency and fixed portion size. Considering the possibility of over-reporting in a previous study(Reference Ogawa, Tsubono and Nishino17), the reported drinking frequency was weighted by 0·75 for all five alcoholic beverages. Dietary intakes of three food items usually added during cooking, namely salt, oil and sugar, were estimated according to the diet history method using the qualitative information in sections 4 and 5, together with the food intakes calculated above. Intakes of table salt and salt-containing seasoning at the table, such as soya sauce and soup consumed with noodles, were estimated from answers to the corresponding qualitative questions in section 5.
Statistical analysis
All statistical analyses were conducted for women and men separately using the SAS statistical software package version 9·1 (SAS Institute Inc., Cary, NC, USA). We also conducted the analysis described below for each of the three areas separately (data not shown). Because the results were similar not only to each other but also to the result derived from all three areas combined, we show only the combined group result.
Intakes of energy were estimated on the basis of the intakes of food items obtained using the DR or with the respective questionnaire and the corresponding food composition list in the Standard Tables of Food Composition in Japan (19). In the previous validation study of the DHQ, the correlation coefficients of nutrient intakes between the DR and DHQ improved when energy-adjusted values, rather than crude values, were used(Reference Sasaki, Yanagibori and Amano4). Therefore, energy-adjusted values were calculated using the density method, which involved computing the amount of each food group consumed daily per 10 MJ of daily energy intake. We assessed the relative validity of the DHQ and BDHQ in terms of the ability to estimate median values of food intake and the ability to rank the individuals in a population according to food intake. The ability to estimate represented values was evaluated by comparing median intakes, and ranking ability was evaluated using Spearman's correlation coefficients. We examined the relative validity of food group intakes derived from the first DHQ (DHQ1) and the first BDHQ (BDHQ1) by comparison with those from the four 4 d DR. Although the reference period differed between the DHQ1 or BDHQ1 (previous month in autumn) and the 4 d DR conducted in each season (which can be considered as representative of habitual intake during the year), we intended to examine whether a single DHQ or BDHQ for dietary habits during the previous month can represent habitual dietary intakes over a longer period (e.g. several months or 1 year). In addition, the mean values of the four DHQ and BDHQ (mDHQ and mBDHQ) were also examined using the same method as above to match the evaluation period with that of the DR.
The food groups used in the present study are shown in Table 1. Food group intakes are presented as medians and interquartile ranges for DR, DHQ1, BDHQ1, mDHQ and mBDHQ. Statistically significant differences in food group intakes between the two questionnaires and the DR were determined using the Wilcoxon signed-rank test using two-sided values, with P < 0·05 considered to indicate a significant difference from the DR. Spearman's correlation coefficients between the DR and DHQ1, BDHQ1, mDHQ or mBDHQ were then calculated. We used these non-parametric tests as they require no assumption of data following a particular parametric distribution, such as the Gaussian, while remaining robust against single gross outliers. Correlation coefficients obtained from the DHQ and BDHQ were compared using the Meng–Rosental–Rubin method to compare overlapping correlation coefficients(Reference Meng, Rosenthal and Rubin20). Tested correlation coefficient pairs were considered to be statistically different when Z > 1·96, with a significance level of 5 %. In addition, agreement for food group intakes between the DR and the questionnaire at the individual level was examined using Bland–Altman plots(Reference Bland and Altman21). We plotted the food intake difference between the DR and the questionnaire against mean values noted in the DR and the questionnaire for typical primary components of a Japanese diet, including rice, total vegetables and fish and shellfish. The limits of agreement were set as 1·96 times the standard deviation of the difference.
Table 1 Definitions of food groups

DHQ, self-administered diet history questionnaire (150 items); BDHQ, brief-type DHQ (fifty-eight items).
†The following food items included in the DHQ (thirteen items) or BDHQ (three items) were not categorized: tomato ketchup; non-oil dressings; table salt; salt used during cooking; soya sauce; curry or stew roux and meat sauce; corn soup; Chinese soup; soup consumed with noodles; water for miso soup; nutritional supplement bars; artificial sweeteners; and drinking water in the DHQ; and table salt and salt-containing seasonings used at the table such as soya sauce; salt used during cooking; and soup consumed with noodles in BDHQ.
‡No food item is included in BDHQ.
Results
Characteristics of participants have been reported elsewhere(Reference Murakami, Sasaki and Takahashi16). The mean ages of women and men were 49·6 (sd 11·4) and 52·8 (sd 12·1) years, respectively. The mean estimated daily energy intakes for women were 7809 (sd 1144) kJ with the DR, 8000 (sd 1538) kJ with the DHQ1, 7364 (sd 1747) kJ with the BDHQ1, 7859 (sd 1387) kJ with the mDHQ and 7139 (sd 1396) kJ with the mBDHQ. The corresponding values for men were 9953 (sd 1788), 9606 (sd 2409), 9237 (sd 2443), 9785 (sd 2053) and 9252 (sd 2028) kJ, respectively.
Medians and interquartile ranges of energy-adjusted food group intakes derived from the DR, DHQ and BDHQ are shown in Table 2 for women and in Table 3 for men. These values were estimated well by the DHQ1 and BDHQ1 for about half of the food groups. No significant differences between the DR and the DHQ1 or between the DR and the BDHQ1 were observed in fifteen (44 %) and fifteen (52 %) foods for women and in fourteen (41 %) and sixteen (55 %) foods for men, respectively. For food group intakes estimated by mDHQ and mBDHQ, no significant differences between the DR and the mDHQ or between the DR and the mBDHQ were observed in twelve (35 %) and sixteen (55 %) foods for women, or in eleven (32 %) and fourteen (48 %) foods for men, respectively.
Table 2 Comparison of energy-adjusted food group intakes (g/10 MJ) estimated using a 16 d DR, DHQ1 and mDHQ and BDHQ1 and mBDHQ among ninety-two women

DR, semi-weighed dietary records; DHQ, self-administered diet history questionnaire; DHQ1, first DHQ; mDHQ, mean of four DHQ; BDHQ1, first brief-type DHQ; mBDHQ, mean of four BDHQ; IQR, interquartile range.
Significantly different from the DR at *P < 0·05, **P < 0·01 and ***P < 0·001 (Wilcoxon signed-rank test).
†In the DHQ, the following two items are available: ‘green and oolong tea’ and ‘black tea’, whereas in the BDHQ, the following two items are available: ‘green tea’ and ‘black and oolong tea’.
Table 3 Comparison of energy-adjusted food group intakes (g/10 MJ) estimated using a 16 d DR, DHQ1 and mDHQ and BDHQ1 and mBDHQ among ninety-two men
DR, semi-weighed dietary records; DHQ, self-administered diet history questionnaire; DHQ1, first DHQ; mDHQ, mean of four DHQ; BDHQ1, first brief-type DHQ; mBDHQ, mean of four BDHQ; IQR, interquartile range.
Significantly different from the DR at *P < 0·05, **P < 0·01 and ***P < 0·001 (Wilcoxon signed-rank test).
†In the DHQ, the following two items are available: ‘green and oolong tea’ and ‘black tea’, whereas in the BDHQ, the following two items are available: ‘green tea’ and ‘black and oolong tea’.
Spearman's correlation coefficients between energy-adjusted food group intakes estimated by the DR and questionnaires are shown in Table 4. Median correlation values for women were 0·43 (range: −0·09 to 0·77) for DHQ1 and 0·44 (range: 0·14 to 0·82) for BDHQ1, with respective values of 0·44 (range: 0·08 to 0·87) and 0·48 (range: 0·21 to 0·83) for men. The correlation coefficients between DR and DHQ1 differed with statistical significance from values between DR and BDHQ1 for some food groups. No statistically significant differences in coefficient values were noted for other food groups. Correlation coefficients of most food groups between the DR and the mDHQ and between the DR and the mBDHQ were improved compared with the respective DHQ1 and BDHQ1 values for both men and women. Median correlation values for women were 0·52 (range: 0·09–0·87) for mDHQ and 0·54 (range: 0·18–0·87) for mBDHQ, with respective values of 0·59 (range: 0·05–0·91) and 0·55 (range: 0·26–0·90) for men. The correlation coefficients between DR and mDHQ differed with statistical significance from values between DR and mBDHQ for several food groups. No statistically significant differences in coefficient values were noted for other food groups. DHQ and BDHQ thus showed comparable correlations for food group intakes.
Table 4 Spearman's correlation coefficient between energy-adjusted food group intakes estimated using a 16 d DR and those estimated using the DHQ1, mDHQ, BDHQ1 and mBDHQ among ninety-two women and ninety-two men

DR, semi-weighed dietary records; DHQ, self-administered diet history questionnaire; DHQ1, first DHQ; mDHQ, mean of four DHQ; BDHQ1, first brief-type DHQ; mBDHQ, mean of four BDHQ.
Significant difference between correlation coefficients of DHQ1 and BDHQ1, or between mDHQ and mBDHQ, at *P < 0·05 and **P < 0·01 (see ‘Method’ section).
†In the DHQ, the following two items are available: ‘green and oolong tea’ and ‘black tea’, whereas in the BDHQ, the following two items are available: ‘green tea’ and ‘black and oolong tea’.
The Bland–Altman plots for rice, total vegetables and fish and shellfish for both DHQ1 and BDHQ1 are illustrated in Fig. 2. In general, examination at group level showed moderate agreement, but poor agreement at individual levels. Similar results were observed in mDHQ and mBDHQ (data not shown).

Fig. 2 Bland–Altman plots for agreement between energy-adjusted intakes (g/10 MJ) of selected food groups (rice, total vegetables and fish and shellfish) estimated using a 16 d DR and that estimated using the DHQ1 or the BDHQ1 in ninety-two women (a–f) and ninety-two men (g–l; DR, semi-weighed dietary records; DHQ1, first self-administered diet history questionnaire; BDHQ1, first brief-type DHQ)
Discussion
We examined the relative validity of food group intakes estimated by the DHQ and BDHQ, which were developed to assess dietary habits in Japanese populations, using a 16 d DR as reference. Compared with the DR, both DHQ1 and BDHQ1, as well as mDHQ and mBDHQ, estimated intakes well for about half of the food groups. Thus, in terms of the ability to estimate the representing value, these questionnaires were relatively useful. Correlation coefficient values were >0·40 for many food groups, showing that DHQ and BDHQ had reasonable ranking ability. Further, correlation coefficients between DR and DHQ1 and between DR and BDHQ1 did not differ with statistical significance for most food groups, nor were statistically significant differences noted between values for DR and mDHQ and between those of DR and mBDHQ. Thus, the DHQ and BDHQ showed similar ranking ability in terms of food intake estimates. Although the correlation coefficients of mDHQ and mBDHQ were higher than those of DHQ1 and BDHQ1, even DHQ1 and BDHQ1 had reasonable validity for food group intakes. On the basis of these results, we determined that DHQ and BDHQ were valid at the group level, although Bland–Altman plots showed poor agreement at the individual level. However, the differences may be too small to be of practical importance, at least in some situations.
In their review of dietary assessment questionnaires validated in Japan, Wakai(Reference Wakai22) reported correlation coefficients between the DR and questionnaires by food group, and found that medians from previous studies ranged from 0·19 to 0·73. The performance of both the DHQ and BDHQ in the present study was thus comparable with these other extensive(Reference Tokudome, Imaeda and Tokudome23, Reference Ishihara, Sobue and Yamamoto24) and short dietary questionnaires(Reference Ogawa, Tsubono and Nishino17, Reference Lee, Uchida and Shirota25, Reference Tsubono, Kobayashi and Sasaki26).
To our knowledge, the present study is the first validation study to compare food group intakes obtained from long and short versions of the same questionnaire. Although the BDHQ has only fifty-eight food items, the results showed that this short questionnaire, which was developed from the DHQ (i.e. the long comprehensive questionnaire), showed a reasonable ranking ability to estimate food group intakes. Although no other study has investigated food group intakes, several studies have compared long and short versions of the same questionnaire with regard to nutrients(Reference Potischman, Carroll and Iturria13–Reference Talegawkar, Johnson and Carithers15), all of which also showed that both the long questionnaire and the short questionnaire derived from it have reasonable ranking ability.
In the present study, not only the DHQ but also the BDHQ estimated food group intakes well. Several explanations for the similar ranking ability of the fifty-eight-item BDHQ and 150-item DHQ can be suggested. First, the food and beverage items in the BDHQ may well reflect foods commonly consumed in Japan. Second, the DHQ takes more time to complete than the BDHQ, which may hamper the accuracy of responses. Third, the BDHQ differs from the DHQ in not asking portion sizes. Some participants in the present study might have answered at least some of the DHQ portion size questions inaccurately. Portion size misestimation has been shown to be a source of error in answering these questionnaires(Reference Di Noia and Contento27). Further, typical portion size varies among individuals and is affected by BMI and other factors(Reference Burger, Kern and Coleman28). Further study is needed to investigate the accuracy of participants' responses to portion size in the DHQ.
Although median food group intakes and correlations obtained from the BDHQ were comparable to those from the DHQ, there were several food groups that neither the DHQ nor the BDHQ estimated well. In particular, potatoes and seaweeds had low correlation between the DHQ and DR and between the BDHQ and DR. Results of epidemiological studies based on the DHQ- or BDHQ-assessed intakes of these foods should be interpreted carefully. In addition, although our results showed that the DHQ and BDHQ were useful in both men and women, a considerable number of men (32 %) answered with their wives’ help; therefore, the validity of the two questionnaires may be lower when the questionnaires are answered by men only.
Several limitations of the present study warrant mention. First, dietary habits are subject to seasonal variation(Reference Ogawa, Tsubono and Nishino29, Reference Tokudome, Imaeda and Nagaya30). Here, we dealt with this issue by using a 4 d DR conducted in each of the four seasons over 1 year as the reference method. This use of a multiple-day DR minimizes the effect of daily and seasonal dietary intake variation on dietary assessment and is therefore the preferred way of validating dietary assessment questionnaires(Reference Willett1). Further, we also examined the validity of not only a single DHQ and BDHQ (autumn) but also the mean of four DHQ and BDHQ, one in each of the four seasons. Second, although we assumed that food group intakes derived from the DR were the gold standard and the present study on relative validity relied on the extent to which DR is accurate, a DR is also susceptible to measurement error because of erroneous recording and potential changes in eating behaviour. Nevertheless, errors in the DR are thought to have lower correlation with errors in the DHQ and BDHQ compared with those in a 24 h dietary recall or other instruments that rely on memory(Reference Willett1). Moreover, biomarkers cannot be used to examine the validity of most food group intakes. Third, the information used to write the algorithm that was used to calculate food intake from data obtained from the BDHQ had insufficient reliability. Further, because information on variables such as portion size and dietary behaviour was not available for use in calculating food intakes from questionnaire data, the BDHQ algorithm was written using previous information(Reference Ogawa, Tsubono and Nishino17) and other unpublished observations. Finally, the participants may not be representative of the general Japanese because they were not randomly sampled from the general Japanese population. In addition, they might have been highly health conscious, given that nearly all of them completed the study despite its strict design.
In conclusion, we found reasonable relative validity of food group intakes estimated by the DHQ and BDHQ compared with those using a DR among adult Japanese men and women with regard to their ability to estimate median values of food intake and their ability to rank individuals in a population according to food intake. The validity of the BDHQ was similar to that of the DHQ. These findings support the use of not only the DHQ but also the BDHQ in large-scale epidemiological studies in Japan.
Acknowledgements
The present study was supported by grants from the Japanese Ministry of Health, Labour and Welfare. The authors have no conflict of interest to declare. S.K. performed statistical analyses and wrote the manuscript; K.M. assisted in writing and editing the manuscript; S.S. contributed to the concept and design of the study, study protocol and data collection, and assisted in writing and editing the manuscript; H.O. assisted in manuscript preparation; N.H., A.N., M.F. and C.D. were involved in study design, data collection and data management. All the authors have read and approved the final manuscript. We thank all participants and local staff for their participation in the study.






