



Significant outcomes
-
Persons with cocaine use disorder presented lower cingulate cortical thickness, and years of cocaine use was the variable most associated with cingulate thickness.
-
Negative correlations were found between early life stress and cingulate thickness.
-
A partial mediation effect of early life stress on cingulate was found in cocaine use disorder.
Limitations
-
The cross-sectional design cannot address the longitudinal developmental effects of exposure to early life stress.
-
We only measured one aspect of grey matter integrity: cortical thickness.
-
The results do not inform whether the observed cortical thinning found in cocaine use disorder could persist with successful treatment.
Introduction
Cocaine use disorder (CUD) is a severe, complex, and debilitating disease characterised by changes in reward and inhibitory systems (Volkow et al., Reference Volkow, Michaelides and Baler2019). There are four key interrelated brain circuits that are involved in or affected by CUD, including the reward circuit (e.g. nucleus accumbens and additional striatum regions), the learning/memory circuit (e.g. amygdala and the hippocampus), the motivation/drive circuit (e.g. orbitofrontal/subcallosal cortices and motor cortex), and the cognitive control circuit (e.g. dorsolateral prefrontal cortex and the cingulate gyrus) (Volkow et al., Reference Volkow, Koob and Mclellan2016). The cingulate is implicated with the neurobiology of impulsivity, cocaine craving, and attentional bias toward cocaine-related cues preceding relapse (Volkow et al., Reference Volkow, Wang, Fowler and Tomasi2012, Canterberry et al., Reference Canterberry, Peltier, Brady and Hanlon2016). In addition, findings suggest that persons with CUD have hypometabolism in the cingulate gyrus during the first months of withdrawal, suggesting that altered function, structure, and metabolism of specific cingulate cortices have clinical implications for the CUD treatment (Volkow and Fowler, Reference Volkow and Fowler2000, Volkow et al., Reference Volkow, Wang, Fowler and Tomasi2012).
Individual differences are highly relevant in the context of substance use disorders. Early-life stress (ELS) is an environmental factor that substantially increases the risk of developing several psychiatric disorders, including CUD (Andersen and Teicher, Reference Andersen and Teicher2009). Moreover, childhood maltreatment has been associated with worse clinical and treatment outcomes for CUD, as patients with a history of childhood physical neglect, for instance, exhibited higher levels of cocaine withdrawal symptoms during detoxification treatment when compared with patients with no such (Francke et al., Reference Francke, Viola, Tractenberg and Grassi-Oliveira2013). In addition to the clinical perspective, neuroimaging evidence points to the existence of altered brain development trajectories associated with ELS exposure (Teicher and Samson, Reference Teicher and Samson2016), a finding that could be implicated with the vulnerability to substance use disorders later in adulthood (De Bellis et al., Reference De Bellis, Morey, Nooner, Woolley, Haswell and Hooper2019). Consistent with that, studies have reported that ELS (Ross et al., Reference Ross, Sartin-Tarm, Letkiewicz, Crombie and Cisler2021, Lim and Khor, Reference Lim and Khor2022) and CUD are associated with alterations in structure, morphology, and function of brain regions involved in motivation, impulsivity, inhibitory control, and emotional regulation (Teicher and Samson, Reference Teicher and Samson2013, Irizar et al., Reference Irizar, Albein-Urios, Martínez-González, Verdejo-Garcia and Lorenzetti2020, Tondo et al., Reference Tondo, Viola, Fries, Kluwe-Schiavon, Rothmann, Cupertino, Ferreira, Franco, Lane, Stertz, Zhao, Hu, Meyer, Schmitz, Walss-Bass and Grassi-Oliveira2021), including the cingulate. For instance, structural and functional alterations in the cingulate cortices have been reported following traumatic stress exposure (Baker et al., Reference Baker, Williams, Korgaonkar, Cohen, Heaps and Paul2013, Calati et al., Reference Calati, Maller, Meslin, Lopez-Castroman, Ritchie, Courtet and Artero2018). However, little is known about whether a history of ELS could interact with CUD effects on the cingulate structure, providing further insights into the relationship between stress and addiction at the neuropathophysiological level.
Thus, this study had two main goals: 1) to compare the cortical thickness (CT) of four cingulate regions (rostral anterior, caudal anterior, posterior, and isthmus regions) between participants with CUD and healthy controls; and 2) to test a mediation model where the severity of exposure to ELS experiences would influence the association between lifetime cocaine consumption and cingulate CT alterations. As the cingulate gyrus has been associated with both ELS and cocaine addiction, we hypothesised that participants with CUD would have cingulate cortical thinning in comparison with controls. Moreover, a direct effect of lifetime cocaine use on cingulate CT was expected, as well as a mediation effect of ELS on this relationship. Therefore, we employed a hypothesis-driven region of interest approach to investigate CT alterations in cingulate subregions.
Importantly, this study was performed with participants who predominantly consumed smoked cocaine (i.e. crack) instead of snorted cocaine (Bittencourt et al., Reference Bittencourt, Bampi, Sommer, Schaker, Juruena, Soder, Franco, Sanvicente-Vieira, Grassi-Oliveira and Ferreira2021). Crack cocaine is associated with shorter periods of sustained abstinence during treatment, greater propensity for dependence, higher plasmatic levels of the substance, greater intensity of psychotropic effects, easier administration, and lower costs when compared with intranasal and intravenous use of cocaine (Kiluk et al., Reference Kiluk, Babuscio, Nich and Carroll2013, Voon et al., Reference Voon, Ti, Dong, Milloy, Wood, Kerr and Hayashi2016). Moreover, crack cocaine users are often socioeconomically disadvantaged, and previous studies have shown that over 80% of female crack cocaine users reported lifetime victimisation, largely during childhood (Tractenberg et al., Reference Tractenberg, Viola, Rosa, Donati, Francke, Pezzi and Grassi-Oliveira2012, Perrenoud et al., Reference Perrenoud, Oikawa, Williams, Laranjeira, Fischer, Strang and Ribeiro2021), suggesting that this population of substance users possess a high risk for the long-term negative consequences of ELS and CUD.
Methods
Participants
We conducted a cross-sectional study with 78 participants with CUD and 53 healthy controls. We recruited the CUD group from public drug treatment inpatient facilities in southern Brazil. During hospitalisation, they followed a standardised cocaine detoxification protocol. The treatment consisted of psychoeducation and support groups, moderate physical activity, a balanced diet (2200 Kcal/day), nursing care, and psychological and medical treatments. As inpatients, they were in an abstinence-controlled environment with no access to any type of drug, including alcohol and nicotine. We recruited the HC from the same community by word-of-mouth advertising.
For inclusion, all participants had to (a) be right-handed; (b) self-declare as being of low or middle socioeconomic status; (c) be 18–50 years old; (d) have graduated middle school (>8 years of educational attainment) in Brazil; and (e) have an IQ > 80. Other criteria for inclusion in the CUD group were having (f) a mental disorder primarily diagnosed as CUD, confirmed via the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-IV) (Kübler, Reference Kübler2013); (g) undergone 7–14 days of inpatient treatment; and (h) tested positive for cocaine in a urine screening test during the first three days of hospitalisation (indicating they had used cocaine less than 1 week before the test). As previously mentioned, participants with CUD had a preference for smoking cocaine as a route of administration. Handedness was checked individually using the Handedness Inventory, with scores above nine indicating right-handedness (Briggs and Nebes, Reference Briggs and Nebes1975). Participants were excluded if they presented potential contraindications for magnetic resonance imaging (MRI) scanning (metallic implants, recent tattoos, claustrophobia), acute or unstable clinical illnesses, abuse of other substances 14 days or less before the study, neurologic disorders, HIV, or syphilis. Participants took a fast-track blood exam to test for the latter two conditions. Concurrent severe psychotic mental disorders were also an exclusion criterion; however, we accepted patients who had other substance use disorders into the CUD group.
For healthy controls, the exclusion criteria also included psychiatric or neurological disorders aside from tobacco use disorder. This sample was screened for major psychiatric disorders using the SCID-IV (Kübler, Reference Kübler2013) and administered by a trained member of the research staff before the date of the MRI exam. Use of psychotropic medications within 6 months before the study and use of alcohol within a week before the study were also exclusion criteria.
All participants tested negative for cocaine, cannabis, amphetamines, opiates, and benzodiazepines in a urine screening test on the date of the MRI. Whenever a crack cocaine user checked into the drug treatment centre and fulfilled the inclusion criteria, we invited them to participate in the study. After 1 week of hospitalisation, professional psychiatrists interviewed each participant using the SCID-IV. Participants underwent an MRI exam between the eighth and fifteenth days of hospitalisation.
All procedures were approved and carried out in accordance with the Ethics Committee of the Pontifical Catholic University of Rio Grande do Sul (PUCRS). After a complete description of the study, all subjects provided written informed consent.
Assessments
Sociodemographic characteristics and drug use patterns were obtained with the Addiction Severity Index – 6th version (ASI-6) (McLellan et al., Reference Mclellan, Luborsky, Woody and O'brien1980, Kessler et al., Reference Kessler, Cacciola, Alterman, Faller, Souza-Formigoni, Cruz, Brasiliano and Pechansky2012). This is a semi-structured interview that gathers information on recent and lifetime problems related to substance misuse - including information on licit (tobacco and alcohol) and illicit drug (cannabis, smoked or snorted cocaine). A pattern of use of at least three times per week during a year was considered a regular year of substance use. Data on both snorted and smoked cocaine were grouped into a single variable.
We assessed childhood maltreatment history with the Childhood Trauma Questionnaire (CTQ). The CTQ is a self-answered, five-point, Likert-type questionnaire with 28 items that evaluate the severity of exposure to ELS. The CTQ generates a total score (possible score range: 25–125) accounting for five types of maltreatment experiences (emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect) (Bernstein et al., Reference Bernstein, Fink, Handelsman, Foote, Lovejoy, Wenzel, Sapareto and Ruggiero1994, Grassi-Oliveira et al., Reference Grassi-Oliveira, Stein and Pezzi2006). In addition, there are quantitative scores for each type of maltreatment. Qualitatively, the presence of maltreatment was determined by using the suggested CTQ cut-off scores for cases of moderate severity.
MRI scanning
All MRI scans were performed in a 3.0T whole-body scanner (Signa, GE Healthcare, Milwaukee, USA). The three-dimensional, T1-weighted images were set to the following parameters: repetition time = 2400 ms, echo time = 15 ms, slice thickness = 1.6 mm, scan matrix = 512 × 512, voxel size = 1 mm3, field of view = 256 mm, and resolution = 256 × 256. All T1 images were visually inspected for the quality of the image and for the absence of apparent motion artefacts. All subjects were invited to undergo a mock scan in a fake MRI machine before the actual MRI scan. The objective was to allow them to familiarise themselves with the procedures of this study.
FreeSurfer pre-processing
To assess the subjects’ CT, we carried out cortical reconstructions using the FreeSurfer (version 5.3) image analysis suite (http://surfer.nmr.mgh.harvard.edu/). In short, the processing of cortical reconstructions involves motion correction and averaging (Reuter et al., Reference Reuter, Hd and Fischl2010) of volumetric T1-weighted images, removal of non-brain tissue using a hybrid watershed/surface deformation procedure, automated Talairach transformation, segmentation of the subcortical white matter and deep subcortical structures (Ségonne et al., Reference Ségonne, Dale, Busa, Glessner, Salat, Hahn and Fischl2004), intensity normalisation tessellation of the grey matter/white matter boundary (Sled et al., Reference Sled, Zijdenbos and Evans1998), automated topology correction (Ségonne et al., Reference Ségonne, Pacheco and Fischl2007), and surface deformation following intensity gradients to optimally place the grey/white and grey/cerebrospinal fluid borders at the location where the greatest shift in intensity defines the transition into the other tissue class (Fischl and Dale, Reference Fischl and Dale2000). Cingulate CT (rostral anterior, caudal anterior, posterior, and isthmus regions) was extracted by parcellation of the cortex using the Desikan–Killiany atlas (Desikan et al., Reference Desikan, Ségonne, Fischl, Quinn, Dickerson, Blacker, Buckner, Dale, Maguire, Hyman, Albert and Killiany2006). For each of the four cortical cingulate areas in both hemispheres, FreeSurfer calculates the average CT. Reconstructed images were visually inspected by three researchers with experience in neuroimaging and manually corrected for segmentation or processing mistakes in accordance with FreeSurfer’s troubleshooting guidelines. Thus, all T1 images were visually inspected for the quality of the image and for the absence of apparent motion artefacts. The edited exams were then reprocessed, and CT data were extracted from the corrected images.
Statistical Analyses
Descriptive analyses are presented as mean and standard deviation or absolute and relative frequencies. Differences involving continuous and categorical variables in sociodemographic clinical data were evaluated using independent t-tests, Yate’s correction for chi-square, or Fisher’s exact tests, respectively.
Analysis of covariance (ANCOVA) was used to estimate cingulate CT differences between groups adjusting by sex, age, and education. We estimated Cohen’s D effect sizes for the CT group comparisons. Pearson’s correlation was used to measure the association between sociodemographic/clinical variables and CT in the whole sample. Spearman’s correlation was used to measure the associations only in the CUD group due to less sample size.
The cingulate regions with significant differences between groups and significant associations with CTQ scores were inserted in a mediation model in which lifetime cocaine use, CTQ scores, and cingulate thickness were defined, respectively, as the independent variable, the intermediary variable, and the outcome. Within these models, the direct effect corresponds to the effect of cocaine use on CT in the absence of the mediating variable (CTQ). The indirect effect corresponds to the effect of cocaine use on CT through the mediating variable. Indirect effects were estimated using the bootstrap bias-corrected method that generates 95% confidence intervals (CIs). CIs that do not contain zero or both positive/negative values indicate statistically significant direct or indirect effects in mediation models with 10,000 bootstrap samples. The total effect equals the sum of both direct and indirect effects. The graphical model is displayed in Fig. 4. The covariates included in the mediation analyses were the same as in the ANCOVAs (i.e. sex, age, and education). Spearman’s correlation was performed to evaluate relationships involving CTQ scores and the mediation result between CUD participants.
All statistical analyses were performed using SPSS v. 26.0 (SPSS Inc., Chicago, IL, USA). Mediation analysis was performed using PROCESS v. 3.5 by Andrew Hayes (Hayes and Preacher, Reference Hayes and Preacher2014).
Results
Sample characteristics
Demographic and clinical characteristics are shown in Table 1. The CUD group was older, had fewer years of education, had higher rates of unemployment, and had fewer participants self-declared as white. Furthermore, the CUD group had more severe exposure to ELS experiences than the control group, with higher CTQ scores among CUD participants than healthy controls. Similarly, the CUD group presented a significantly higher prevalence of physical abuse (p = .003), emotional abuse (p = .019), emotional neglect (p = .002), and physical neglect (p = .001), considering the quantitative scores for each type of ELS. Qualitatively, among the CUD group 27 participants (34%) presented childhood physical abuse history, 17 participants (22%) presented childhood sexual abuse history, 26 participants (33%) presented childhood emotional abuse history, 25 participants (32%) presented childhood emotional neglect history, and 24 participants (30%) presented childhood physical neglect history, while among the control group 6 participants (11%) presented childhood physical abuse history, 5 participants (9%) presented childhood sexual abuse history, 8 participants (15%) presented childhood emotional abuse history, 4 participants (7%) presented childhood emotional neglect history, and 4 participants (7%) presented childhood physical neglect history.
Table 1. Sample characteristics
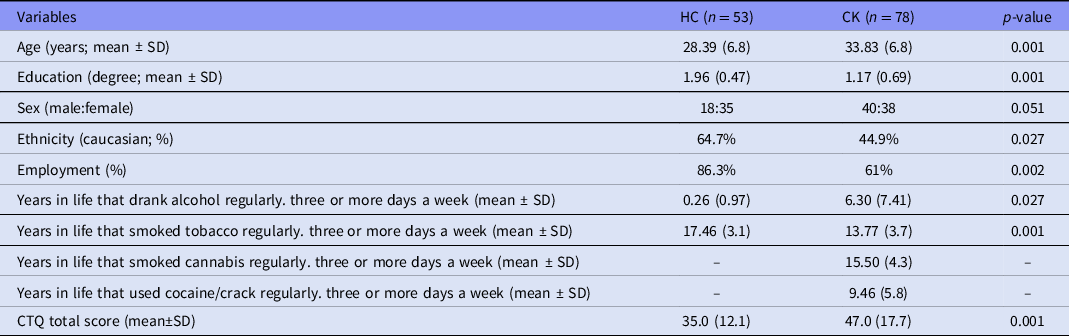
Legend. HC: healthy controls. CK: Crack-cocaine use disorder. Education: 0 – no formal education. 1 – elementary/middle school. 2 – high school. 3 – college.
Regular alcohol use was more common in the CUD group than in the control group, while regular tobacco use was more common in the control group than in the CUD group. No participant in the control group presented histories of regular cocaine/crack consumption.
Cortical thickness
Freesurfer analyses revealed cingulate regions with significant CT in CUD participants compared with healthy controls (Fig. 1). Group comparisons controlled for sex, age, and education revealed significant differences between groups in six regions out of eight (LH – left hemisphere / RH – right hemisphere), showing lower CT in the CUD group compared with the control group (p-values < 0.05). Compared with controls, the CUD group showed lower CT in the LH caudal anterior cingulate (p = 0.009, Cohen’s d = 1.01), LH rostral anterior cingulate (p < 0.001, Cohen’s d = 1.11), RH rostral anterior cingulate (p = 0.003, Cohen’s d = 0.76), LH posterior cingulate thickness (p = 0.018, Cohen’s d = 0.87), RH posterior cingulate (p = 0.007, Cohen’s d = 0.76), and RH isthmus cingulate (p = 0.003, Cohen’s d = 0.69). Groups did not differ in RH caudal anterior cingulate and LH isthmus cingulate thickness.
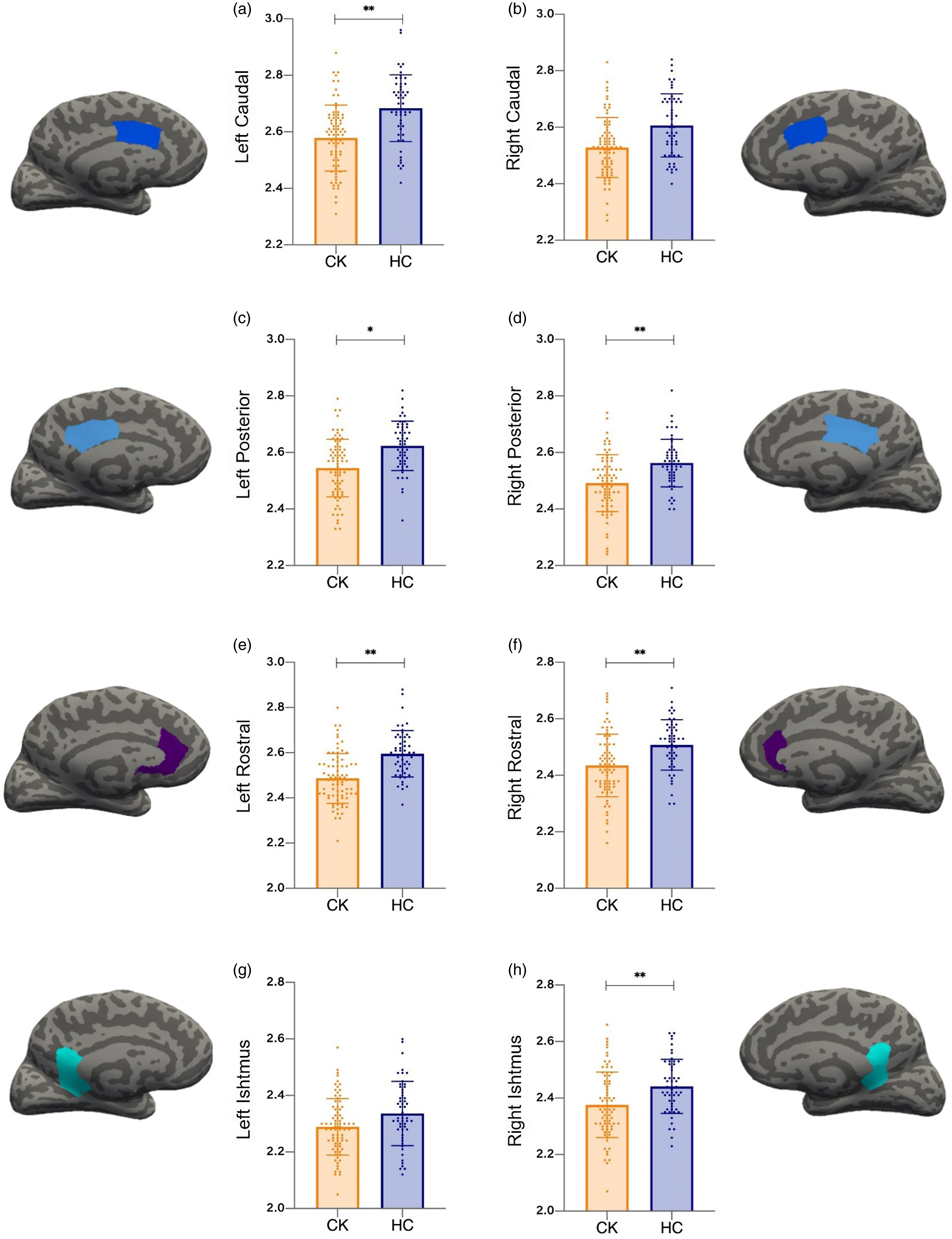
Fig. 1. HC: Healthy controls. CK: Crack-cocaine use disorder. Comparisons performed with ANCOVA adjusted for sex/age/education. Cingulate cortex regions: rostral anterior, caudal anterior, posterior, and isthmus. Y-axis of figures in millimetre scales. * represents a p-value 0.05. ** represents a p-value 0.01.
Correlation analyses
Fig. 2A shows the correlation matrix between substance use, sample characteristics, and cingulate CT. The correlation analysis between CTQ scores and cingulate thickness showed that CTQ scores were negatively correlated with RH isthmus cingulate and with LH rostral anterior cingulate thickness. At the same time, there were no significant associations with other cingulate regions. Furthermore, there were significant associations between cingulate thickness and age/education. Age was negatively correlated with almost all cingulate regions, except for the RH and LH isthmus cingulate. Similarly, education was positively correlated with almost all cingulate regions, except for the RH isthmus and the RH rostral cingulate. We also performed a scatter plot to show the association between CTQ scores and RH isthmus cingulate thickness (Fig. 2B).
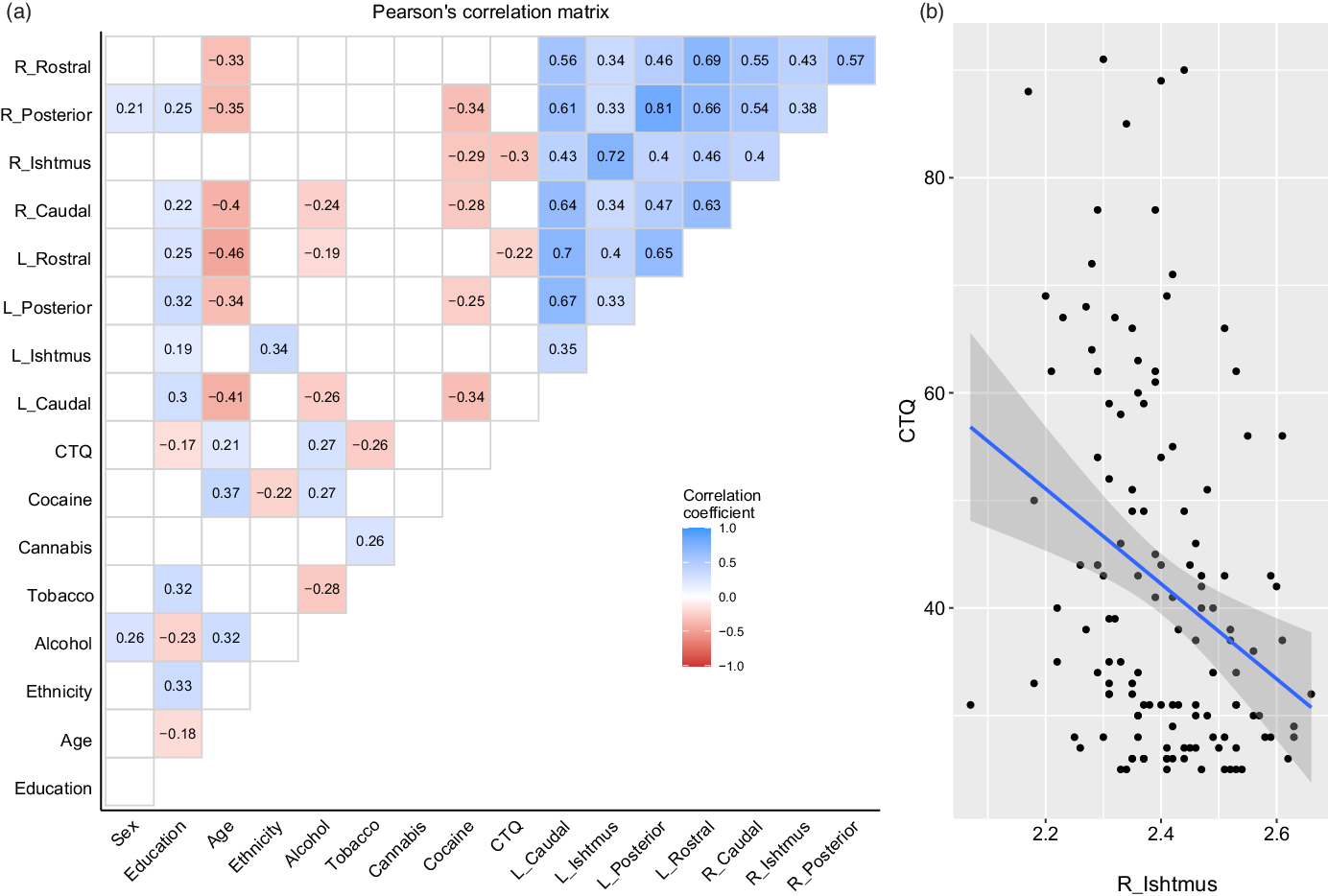
Fig. 2. A: Pearson’s correlation matrix, only significant correlations are depicted within the matrix. Ethnicity = 1, caucasian. Cocaine (both snorted/smoked), alcohol, cannabis, and tobacco represent years of regular consumption. CTQ, represents the total score. B: Correlation between CTQ total score and isthmus cingulate (right hemisphere) cortical thickness.
Regarding licit/illicit drugs, years of regular cocaine use was the variable most associated with cingulate thickness, negatively correlated with LH caudal anterior cingulate, LH posterior cingulate, RH caudal anterior cingulate, RH isthmus cingulate, and posterior cingulate thicknesses. Additionally, the correlational analysis revealed that years of regular alcohol use were negatively correlated with LH caudal anterior cingulate, RH caudal anterior cingulate, and LH rostral anterior cingulate thicknesses. There were no associations between tobacco/cannabis and cingulate thickness.
Mediation model
We ran mediation models in which years of regular cocaine use (if a control participant had never used cocaine, it was computed as zero years) was the predictor of cingulate thickness and tested whether CTQ scores could underlie this association. These analyses were controlled for age/education/sex and allowed us to identify the direct and indirect effects of cocaine use through childhood maltreatment. Thus, we tested the mediation effect only for the RH isthmus cingulate since this region was correlated with the total CTQ score in previous analyses.
In the mediation analysis, we found a negative significant direct effect of cocaine use on the RH isthmus cingulate (b = −0.005, 95%CI [−0.009, −0.002]) and an indirect effect mediated by CTQ scores on the RH isthmus cingulate (b = −0.001, 95%CI [−0.002, −0.0001]), suggesting partial mediation. The mediation model showed a significant improvement over a null model (R = 0.37; R-squared = S 0.14; Mean Square Error = 0.011; p = 0.0006. Specifically, 16.66% of the model’s total effect (b = −0.006, 95%CI [−0.010, −0.003]) was explained by the indirect effects mediated by ELS. Also, a marginal interaction effect was observed for sex (p = 0.055). The mediation model is shown in Fig. 3. Additionally, Spearman’s correlation analysis between the RH isthmus cingulate and CTQ scores for each type of maltreatment experience in the CUD group only showed a negative correlation with childhood physical abuse score (rho = −0.25, p = 0.024), while there were no significant associations between other CTQ scores and RH isthmus.
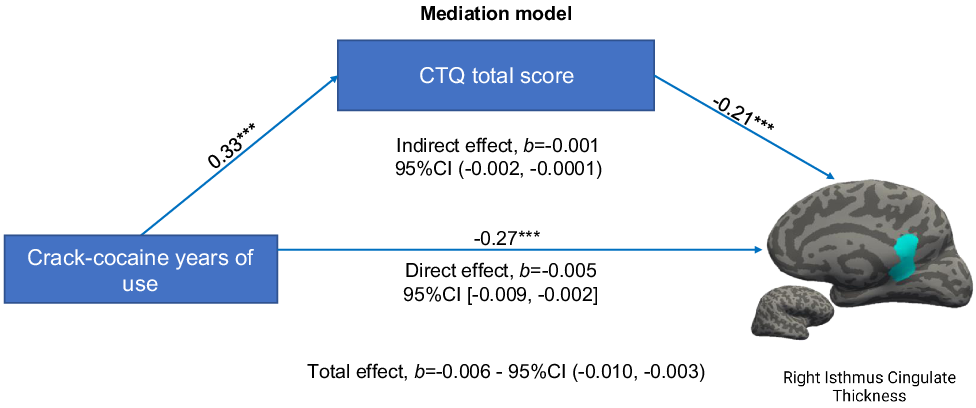
Fig. 3. The direct effect means the effect of cocaine use on CT when the mediating variable (CTQ) is not included. The indirect effect means the effect of cocaine use on CT through the mediating variable. 95% confidence intervals (CIs) that do not include zero, or both positive/negative values, indicate statistically significant effects. The total effect is the sum of the indirect/direct effect in the mediation model. A pattern of crack-cocaine use at least three times per week during a year was considered as a regular year of crack-cocaine consumption. Univariate standardized regression coefficients are presented above lines, showing a positive association between the predictor and the mediator, and negative associations between the predictor/mediator with the outcome.
Since we also found a negative correlation between alcohol use and LH rostral anterior cingulate thickness, we also tested the mediation model with alcohol instead of cocaine use as the main predictor. Neither a direct effect of alcohol (b = −0.0009, 95%CI [−0.004, 0.002]) nor an indirect effect of ELS/alcohol (b = −0.0004, 95%CI [−0.001, 0.0004]) were detected.
Discussion
Using structural MRI data, we compared cingulate CT between CUD patients and healthy control subjects. Group comparisons revealed significant differences in LH caudal anterior cingulate, LH rostral anterior cingulate, RH rostral anterior cingulate, LH posterior cingulate, RH posterior cingulate, and RH isthmus cingulate thicknesses, with a significantly lower CT in the CUD group than in the control group. We also observed higher CTQ scores in the CUD group than in the control group. Significant negative correlations were found between CTQ scores and CT of the RH isthmus cingulate and the LH rostral anterior cingulate. The mediation analysis showed a negative significant direct effect of cocaine use on isthmus cingulate CT and an indirect effect mediated by CTQ scores on isthmus cingulate CT, suggesting partial mediation. Particularly, 16,66% of the model’s total effect was explained by the indirect effects mediated by ELS. We demonstrated that ELS is related to CUD and, in conjunction with it, mediates the effect of CUD on decreased isthmus cingulate thickness in the right hemisphere. This supports the role of ELS as a key environmental stressor that influences brain developmental trajectories associated with drug addiction.
Previous neuroimaging studies observed that the cingulate cortex of cocaine users has abnormalities in perfusion (Childress et al., Reference Childress, Mozley, Mcelgin, Fitzgerald, Reivich and O'brien1999), white matter fractional anisotropy (Tondo et al., Reference Tondo, Viola, Fries, Kluwe-Schiavon, Rothmann, Cupertino, Ferreira, Franco, Lane, Stertz, Zhao, Hu, Meyer, Schmitz, Walss-Bass and Grassi-Oliveira2021), and grey matter density compared with controls (Ersche et al., Reference Ersche, Jones, Williams, Turton, Robbins and Bullmore2012). Similar to our findings, Connolly et al., observed a negative association between years of cocaine use and grey matter volume of the cingulate gyrus (Connolly et al., Reference Connolly, Bell, Foxe and Garavan2013). More specifically, the anterior cingulate cortex is involved in reward processing and motivational salience and governs cognitive control processes such as attention and inhibition (Bubb et al., Reference Bubb, Metzler-Baddeley and Aggleton2018, Zhao et al., Reference Zhao, Sallie, Cui, Zeng, Du, Yuan, Li, De Ridder and Zhang2021). Consistent with these observations, the rostral anterior cingulate cortex has been previously linked to encoding aversive emotional states (Rainville et al., Reference Rainville, Duncan, Price, Carrier and Bushnell1997) and uncertainty in the decision-making framework (Bush et al., Reference Bush, L.U.U. and Posner2000), and particularly in the suppression of task-irrelevant emotional information (Davis et al., Reference Davis, Taylor, Hutchison, Dostrovsky, Mcandrews, Richter and Lozano2005). The posterior cingulate cortex is a primary node of the default mode network and is related to drug abuse (Li et al., Reference Li, Yang, Wang, Huang, Li, Zhu, Zhang, Zhao, Qin, Yuan, Von Deneen, Wang and Tian2013). Thus, the cingulate cortex serves not only as a crucial neural substrate characterising the neurobiological mechanisms of addiction but also has the potential of a therapeutic target and neuroimaging-based biomarker of CUD (Zhao et al., Reference Zhao, Sallie, Cui, Zeng, Du, Yuan, Li, De Ridder and Zhang2021). Indeed, given that the cingulate cortex is also implicated in the modulation of cue-induced cocaine craving (Kilts et al., Reference Kilts, Gross, Ely and Drexler2004), evidence suggests that bilateral transcranial stimulation over the prefrontal cortex changes the drug-cued reactivity in the cingulate cortex in patients with CUD (Conti and Nakamura-Palacios, Reference Conti and Nakamura-Palacios2014).
We also verified a mediation effect of ELS severity within the relationship between lifetime cocaine consumption and cingulate CT, suggesting that adverse experiences during childhood, such as abuse and neglect, could aggravate the effects of CUD later in life regarding thinning of the right isthmus cingulate CT. Importantly, the mediation model suggested that some percentage of the total model effect was due to the influence of a history of ELS (i.e. indirect effect), showing that years of substance consumption is not the only factor associated with altered brain CT. Indeed, evidence suggests that additional psychosocial factors (e.g. childhood maltreatment, adversity, poverty) account for a proportion of the detrimental effects of substance use disorders in the brain (De Bellis et al., Reference De Bellis, Morey, Nooner, Woolley, Haswell and Hooper2019). For instance, it has been shown that highly traumatised Kurdish male refugees and repatriated French citizens from Algeria presented reduced bilateral isthmus cingulate cortex volume in comparison with healthy non-traumatized controls (Calati et al., Reference Calati, Maller, Meslin, Lopez-Castroman, Ritchie, Courtet and Artero2018), suggesting that stressful experiences may increase the risk to the isthmus cingulate of the adverse effects of lifetime cocaine consumption.
The results of this study should be interpreted by taking some limitations into account. First, it must be pointed out that our findings suggest only a partial mediation effect of ELS on the relationship between lifetime cocaine use and decreased isthmus cingulate thickness. It suggests that other pathophysiological mechanisms underlie the association between lifetime cocaine use and cingulate thickness. Second, the CUD group was older and had lower educational attainment than the control group, which is important because age and education are associated with differences in brain structure. However, all statistical analyses were controlled for age and education. Third, our study is cross-sectional, so it cannot address the longitudinal developmental effects of exposure to childhood maltreatment on CT. Despite the cross-sectional design, we used mediation analysis to investigate this relationship. Therefore, with all due caution, given the nature of our data, the statistical method can facilitate an understanding of the relationships between these factors. Fourth, the results also do not inform whether the observed cortical thinning found in CUD subjects could persist with successful treatment and long abstinence periods. Thus, prospective studies also need to explore the relevance of these findings to the progression of drug addiction, prediction of relapse, and treatment outcomes. Lastly, we only measured one aspect of grey matter integrity: CT. Therefore, we cannot rule out the existence of other anatomical alterations associated with CUD. Future studies using other measures and analysis methods should help elucidate these functional changes to the underlying brain structure.
Conclusion
Our results provide evidence of the interactive effects of both childhood maltreatment and lifetime cocaine use on the cingulate gyrus among persons with CUD, suggesting putative mechanisms by which exposure to ELS may create a vulnerable brain substrate for the effects of CUD later in life. This finding is important for our understanding of the effects of trauma, stress, and CUD on the grey matter structure of the brain. Because the cingulate gyrus is implicated in cognitive, emotional, and behavioural control processes, the effects of CUD on the cingulate cortex may reflect a progressive loss of control related to addictive behaviours. Future longitudinal studies should build on the groundwork established by the analyses presented in this study to examine both structure and function of grey matter in clinical groups and to identify a clinical usage for these neuroimaging markers.
Author contributions
The study was designed by Bittencourt, Viola and Grassi-Oliveira. MRI acquisition and FreeSurfer analyses were carried out by Bittencourt, Tondo, Rothman, Belmonte, and Ferreira. Statistical analyses were carried out by Viola. Bittencourt wrote the first draft of the manuscript, which was subsequently revised for important intellectual content by the remaining authors. Grassi-Oliveira designed the original protocol and got the funding. All authors approved the final version of the manuscript before submission.
Financial support
This study was supported by NIDA and the Fogarty Foundation (RGO) (R01DA044859) and by CNPq (RGO) (466802/2014-5) and SENAD (RGO) (822647/2015).
Statement of interest
The authors have no conflicts of interest to declare.




