


The obesity pandemic is sweeping every age group. Children and adolescents are increasingly heavier than those of previous generations. In 1978, 3 % of the Canadian adolescents between the ages of 12 and 17 years were obese. The prevalence had increased to 9 % by 2004, the largest increase of all the Canadian age groups(Reference Canada1). The causes of obesity are numerous, and include environmental, cultural, familial, behavioural, metabolic and genetic factors. In the last 30 years, research on behavioural issues associated with obesity has expanded; yet, many questions remain unanswered and most conclusions are only tentative.
A number of research questionnaires are used to assess eating behaviour traits. One of the most widely used is the Three-Factor Eating Questionnaire (TFEQ)(Reference Stunkard and Messick2) that measures cognitive restraint, disinhibition and hunger in adults. In 1991, Westenhoefer(Reference Westenhoefer3) suggested that cognitive restraint, as measured by the TFEQ, could be divided into two subscales depending on its relationships with BMI and disinhibition: flexible and rigid control. The former, a more relaxed version of restraint, is associated with both low disinhibition and low BMI. The latter is a more severe restrictive state, and is associated with both high disinhibition and high BMI(Reference Westenhoefer, Stunkard and Pudel4). In addition to the control subscales, Bond et al. (Reference Bond, McDowell and Wilkinson5) expanded on the three main categories by defining more specific subscales for each behaviour trait, e.g. strategic dieting behaviour, emotional susceptibility and avoidance of fattening foods. These TFEQ subscales have been measured in adults(Reference Westenhoefer, Stunkard and Pudel4, Reference Drapeau, Provencher and Lemieux6–Reference Provencher, Drapeau and Tremblay11); however, to the best of our knowledge, they have never been assessed in adolescents.
The TFEQ has been shown to measure cognitive restraint and disinhibition independently(Reference Williamson, Lawson and Brooks10, Reference Van Strien12); yet, these behaviours work in combination as well. Studies have shown that high susceptibility to overeat (disinhibition) combined with low restriction is associated with higher body weight(Reference Westenhoefer, Broeckmann and Munch8, Reference Westenhoefer, Pudel and Maus13–Reference Dykes, Brunner and Martikainen15). These interactions have been studied in women using the TFEQ control subscales(Reference Williamson, Lawson and Brooks10), and in adolescent females, using the Dutch Eating Behaviour Questionnaire(Reference Van Strien12), with varying results concerning body weight. Thus, eating behaviour traits in adolescents have not been largely studied. The aim of the present study was to assess eating behaviours and their associations with body weight in adolescents.
Methods
The volunteers for the present study participated in the Québec Family Study, a prospective study which was started in 1978 and was continued until 2001 (phase 1, 1978–82; phase 2, 1989–95; phase 3, 1997–2001). All methods relevant to the present report are described elsewhere(Reference Provencher, Drapeau and Tremblay11). Sixty adolescents completed the TFEQ at the end of phase 2. Self-reported, 3 d dietary records(Reference Tremblay, Sévigny and Leblanc16) (two weekdays and one weekend day) were collected, and the Canadian Nutrient File(Reference Verdier and Beare-Rogers17) was used to estimate energy intake and diet macronutrient content. Body weight and height were measured using standardised laboratory methods. In addition to the original fifty-one-question TFEQ, subscales for disinhibition, hunger and cognitive restraint(Reference Bond, McDowell and Wilkinson5), as well as the rigid and flexible control subscales(Reference Westenhoefer3), were also measured. Lean and overweight/obese categories were determined by obesity cutoffs suggested by Cole et al. (Reference Cole, Bellizi and Flegal18) The adolescents were grouped into four categories defined by their levels of restraint (cognitive restraint, flexible control and rigid control) and disinhibition: (1) high disinhibition–high restraint; (2) high disinhibition–low restraint; (3) low disinhibition–high restraint (4) low disinhibition–low restraint. High and low scores were defined as being above or below the group median with equal group sizes. We selected this method of classification because there are currently no TFEQ score norms for adolescents by which to classify them.
Statistical analyses were performed using JMP 7.0 Statistical Software from Statistical Analysis Systems (SAS Institute, Cary, NC, USA). Means, standard error and interquartile ranges were calculated, and Student's t tests were used to test for sex and weight category differences in mean TFEQ values with the significance level set at P ≤ 0·05. Pearson's correlation coefficient was used to quantify linear relationships. When appropriate, correlations were adjusted for confounding factors such as age and BMI (reported energy intake). As the median split method has been criticised(Reference MacCallum, Zhang and Preacher19), full-factorial multiple regression analysis using the continuous variables restraint and disinhibition was also used to test for variable interaction. An ANOVA was used to compare BMI z-scores between various TFEQ categories. When the ANOVA was significant, a post hoc Tukey–Kramer test was used to detect which conditions were statistically different from each other. To account for the variation in growth rate observed at adolescence, values were transformed into BMI z-scores using the US Centre for Disease Control and Prevention 2000 growth charts for children, aged 2–20 years(Reference Berkey and Colditz20). The present study was approved by the Medical Ethics Committee of Université Laval.
Results
Characteristics of the study population are given in Table 1. There were no significant sex differences either in physical characteristics or in mean TFEQ scores, except for avoidance of fattening foods which was higher in females than in males (P < 0·05). Rigid control, disinhibition and emotional susceptibility to overeat were all positively related to BMI z-scores (Table 2). Among females, but not among males, there was a positive relationship between rigid control and BMI z-scores (P ≤ 0·04). Among males, but not among females, emotional susceptibility and disinhibition were significantly correlated with BMI z-scores (P ≤ 0·02 and 0·03, respectively). Mean values of rigid control, disinhibition and the disinhibition subscales were all higher among the overweight/obese adolescents (Table 3). In the total sample, rigid and flexible control were positively correlated after adjusting for age and BMI (r 2 0·11, P < 0·01).
Table 1 Physical characteristics of the study population by sex
(Mean values and interquartile ranges (IQR))
Table 2 Correlations between eating behaviours and BMI z-scores* in adolescents
TFEQ, Three-Factor Eating Questionnaire.
* BMI z-scores were calculated from the Center for Disease Control and Prevention 2000 growth charts.
Table 3 Three-Factor Eating Questionnaire (TFEQ) scores with corresponding subscales for adolescents
(Mean values and interquartile ranges (IQR))

Mean values were significantly different from those of lean adolescents: *P < 0·05, **P < 0·01.
The adolescents were grouped into four categories according to their levels and type of restriction (flexible and rigid) and disinhibition. Mean TFEQ scores were all significantly different between low and high categories (P < 0·05; Table 4). Sex distributions within the TFEQ categories were not significantly different, and for this reason, we did not separate the categories by sex. Full-factorial multiple regression analysis revealed no significant effect of the interaction between disinhibition and cognitive restraint, flexible control or rigid control on BMI z-scores (data not shown). However, adolescents characterised by high cognitive restraint–high disinhibition had significantly higher BMI z-scores than those characterised by low disinhibition–low cognitive restraint (Fig. 1(A)), as did those characterised by high disinhibition–high rigid control when compared with the group characterised by low disinhibition–low rigid control (Fig. 1(B)). There were no significant differences between BMI z-scores for the flexible control categories (Fig. 1(C)).
Table 4 Three-Factor Eating Questionnaire (TFEQ) scores for high and low categories of cognitive restraint, its subscales and disinhibition
(Mean values and interquartile ranges (IQR))
* Mean values were significantly different from each other for all high–low pairs (P < 0·05).
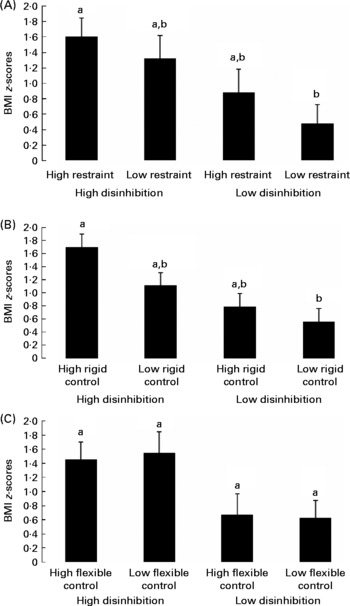
Fig. 1 BMI z-scores for (A) cognitive restraint, (B) rigid control and (C) flexible control–disinhibition eating behaviour categories for male and female adolescents. Data are represented as means with their standard errors. Mean values were significantly different as per one-way ANOVA (P ≤ 0·05). a,b Mean values with unlike letters were significantly different from each other as per post hoc Tukey–Kramer test (P ≤ 0·05).
Hunger was positively correlated to self-reported energy intake for the entire sample (r 2 0·1, P ≤ 0·02). No other TFEQ scales were related to either energy intake or macronutrient content estimated from the dietary records.
Discussion
To our knowledge, the present study was the first to assess the TFEQ, and its subscales, on an adolescent population of both sexes. The results showed that the rigid control trait was positively related to BMI z-scores in females, while emotional susceptibility and disinhibition were associated with BMI z-scores in males. In addition to individual TFEQ associations with body weight, eating behaviour categories were also associated with BMI z-scores. When the cognitive restraint scale is divided into the restraint subscales (rigid and flexible), the deleterious effect of rigid control on body weight is observed. Although there was no interaction effect of rigid control and disinhibition on BMI z-scores, those with both high restraint and high disinhibition had significantly higher BMI z-scores than those with low eating behaviour scores, with the negative effect deriving from high rigid control. These behaviours had significant and independent effects on BMI z-scores, and a trend towards an additive effect was visible.
Disinhibition, or overeating, is known to be associated with increased body weight(Reference Bryant, King and Blundell21), whereas the relationship between body weight and dietary restraint varies in adults; some show an inverse relationship(Reference Shearin, Russ and Hull9, Reference Williamson, Lawson and Brooks10, Reference Lawson, Williamson and Champagne14), while others show no relationship(Reference Dykes, Brunner and Martikainen15, Reference Schubert and Randler22–Reference Harden, Corfe and Richardson24). A positive relationship between restrained eating and body weight has been found among adolescents(Reference Lluch, Herbeth and Mejean25, Reference de Lauzon, Romon and Deschamps26) and children(Reference Vogels, Posthumus and Mariman27). In the present study, there was no linear relationship between cognitive restraint per se and BMI z-scores, but the heavier the adolescents were, the higher their rigid control towards eating was, a result concordant with previous findings in adults(Reference Westenhoefer, Stunkard and Pudel4, Reference Drapeau, Provencher and Lemieux6, Reference Timko and Perone7, Reference Provencher, Drapeau and Tremblay11, Reference Schubert and Randler22, Reference Stewart, Williamson and White28). The conflicting results of dietary restraint in the literature coupled with data emerging regarding rigid dietary control show the importance of using the restraint subscales. In the present study, flexible control did not seem to affect body weight as it is not related to BMI z-scores.
In accordance with the results obtained in adult men(Reference Provencher, Drapeau and Tremblay11), there was a positive relationship between disinhibition and BMI z-scores among adolescent males, a relationship not found among females in the present study. Male adolescent eating behaviour studies are rare. One study has shown that male adolescents exhibit higher uncontrolled eating, a derivative of the disinhibition measure in a revised TFEQ (TFEQ-R18)(Reference de Lauzon, Romon and Deschamps26), and another study has shown higher external hunger, which is eating in the absence of hunger according to the Dutch Eating Behaviour Questionnaire(Reference Snoek, van Strien and Janssens29). Not only was disinhibition related to body weight in the present study, but the male adolescents had higher mean disinhibition scores when compared with adult norms(Reference Timko30). Restrained eating seems to be more prevalent in adolescent females(Reference Lluch, Herbeth and Mejean25, Reference de Lauzon, Romon and Deschamps26, Reference Snoek, van Strien and Janssens29), whereas overeating may play an important role in both sexes. Accordingly, a large adolescent study showed that 7·8 % of boys and 17·3 % of girls reported objective overeating, revealing its effects on both sexes(Reference Ackard, Neumark-Sztainer and Story31). A recent review(Reference Bryant, King and Blundell21) has confirmed the poor health associations of disinhibited eating, and stressed the importance of including young males in eating behaviour/disorder research as the problem is now being observed in young males(Reference Muise, Stein and Arbess32).
Analyses by high and low eating behaviour categories revealed that having both high disinhibition and high restraint, specifically high rigid control, were related to higher BMI z-scores. The individuals in the high disinhibition–high rigid control category may be characterised as being unsuccessful in their restrained attempts, which could explain their increased body weight. The fundamental purpose of the rigid control subscale was to show that some individuals are so severely controlled that this behaviour is unable to be maintained, and uncontrolled eating episodes occur(Reference Westenhoefer3). It was shown that young females with high dietary restraint in combination with other eating behaviours, specifically disinhibition, were more likely to fail at their restrained efforts and had more eating disorder symptoms, such as binging(Reference Van Strien12). Disinhibition and rigid control towards eating are the strongest distinguishing factors for obesity in this group of adolescents, since only those with both high disinhibition and high rigid control had significantly higher BMI z-scores than those with low levels of both behaviours. As there were no significant differences between the flexible control categories, flexible control may have a moderating effect on BMI. This is not surprising as flexible control is known to be a more successful approach to weight loss(Reference Westenhoefer, Stunkard and Pudel4). Several studies have found that restraint has a moderating effect on the interaction between disinhibition and body weight(Reference Lawson, Williamson and Champagne14, Reference Dykes, Brunner and Martikainen15, Reference Hays, Bathalon and McCrory23); yet, these studies did not use the restraint subscales. Using the restraint subscales may shed more light on the potential moderating effect of restraint.
Various factors could explain the trends observed herein. The categories were formed on the basis of the study sample means. The lack of TFEQ research on adolescents limits comparisons. However, when comparing these values with US adult TFEQ norms(Reference Timko30) and with results obtained in children (12 years)(Reference Vogels, Posthumus and Mariman27), overall high disinhibition scores among these adolescents were observed, specifically among the males. In contrast, cognitive restraint, rigid control and flexible control scores were all lower in this population than in adults(Reference Westenhoefer, Stunkard and Pudel4, Reference Drapeau, Provencher and Lemieux6, Reference Provencher, Drapeau and Tremblay11) and children(Reference Vogels, Posthumus and Mariman27). Thus, the high disinhibition scores coupled with the low restraint scores may be largely responsible for the lack of significant differences between restraint and disinhibition categories.
In the present study, hunger was the only TFEQ score which was associated with absolute energy intake. One study also reported a similar lack of associations between TFEQ scores and energy intake(Reference Goulet, Provencher and Piche33); however, most studies have reported these associations(Reference Westenhoefer, Pudel and Maus13, Reference Harden, Corfe and Richardson24, Reference Lluch, Herbeth and Mejean25, Reference Provencher, Drapeau and Tremblay34). Discrepancies could be explained in part by under-reporting in adolescents, which has been found to be as much as 34 %(Reference Rennie, Jebb and Wright35). BMI values(Reference Vance, Woodruff and McCargar36) and eating restraint scores (for females) are also positively correlated with under-reporting in dietary analysis in adolescent populations(Reference Babio, Canals and Fernandez-Ballart37, Reference Ventura, Loken and Mitchell38). The lack of associations between the TFEQ scores and self-reported energy intake could in part be explained by these phenomena; yet, further research is needed in this area.
There are other limitations with the present study. The lack of high and low norms for eating behaviours resulted in the use of group-specific separations, and this should be taken into account when interpreting the present results. A larger sample size would be needed to generate more definitive tests of the trends observed herein. Finally, because of the cross-sectional nature of these associations, it is impossible to establish cause and effect relationships.
In conclusion, eating behaviours in adolescents are associated with body weight, similar to what is observed in adult studies. The TFEQ is able to identify relevant eating behaviour traits associated with higher BMI in this mixed-sex age group. Disinhibition and rigid control should be targeted in adolescents in order to characterise youth at risk for obesity, and to implement proper weight control strategies or to predict success or failure in weight-loss participants.
Acknowledgements
The present work was funded by the Canadian Institutes of Health Research (MCG-15187). A. R. G. is a recipient of the Richard J. Schmeelk Fellowship. The authors specially thank G. Fournier, L. Allard, M. Chagnon and C. Leblanc for their contributions to the recruitment and data collection of the Québec Family Study. Québec Family Study was supported over the years by multiple grants from the Medical Research Council of Canada and the Canadian Institutes for Health Research (PG-11811, MT-13960 and GR-15187) as well as other agencies. There are no conflicts of interest for the present study. The authors' contributions are as follows: A. R. G. carried out the literature review, data extraction and interpretation of the data, and drafted the manuscript. V. D. participated in the conceptualisation, data extraction and interpretation of the data, and helped to draft the manuscript. A. T., L. P., C. B. and J.-P. D. contributed to the conceptualisation and data interpretation. All the authors revised the manuscript.





