



Introduction
People with HIV (PWH) are at increased risk for neurocognitive impairment (NCI) (Clifford & Ances, Reference Clifford and Ances2013; Heaton et al., Reference Heaton, Clifford, Franklin, Woods, Ake, Vaida, Ellis, Letendre, Marcotte, Atkinson, Rivera-Mindt, Vigil, Taylor, Collier, Marra, Gelman, McArthur, Morgello, Simpson, McCutchan, Abramson, Gamst, Fennema-Notestine, Jernigan, Wong and Grant2010), with HIV-associated neurocognitive disorders (HAND) evident in up to half of PWH (Heaton et al., Reference Heaton, Clifford, Franklin, Woods, Ake, Vaida, Ellis, Letendre, Marcotte, Atkinson, Rivera-Mindt, Vigil, Taylor, Collier, Marra, Gelman, McArthur, Morgello, Simpson, McCutchan, Abramson, Gamst, Fennema-Notestine, Jernigan, Wong and Grant2010; Heaton et al., Reference Heaton, Franklin, Deutsch, Letendre, Ellis, Casaletto, Marquine, Woods, Vaida, Atkinson, Marcotte, McCutchan, Collier, Marra, Clifford, Gelman, Sacktor, Morgello, Simpson, Abramson, Gamst, Fennema-Notestine, Smith and Grant2014; Saloner & Cysique, Reference Saloner and Cysique2017). Hispanics/Latinos/as/e/x, hereafter Hispanics, are the largest ethnic minority in the USA and at threefold risk for HIV infection compared to non-Hispanic Whites, hereafter Whites (HIV Surveillance Report, 2019). Hispanic PWH in the USA have worse disease outcomes including higher rates of acquired immunodeficiency syndrome (AIDS) and mortality compared to White PWH (McGinnis et al., Reference McGinnis, Fine, Sharma, Skanderson, Wagner, Rodriguez-Barradas, Rabeneck and Justice2003; Mindt et al., Reference Mindt, Miranda, Arentoft, Byrd, Monzones, Fuentes, Arias, Rentería, Rosario and Morgello2014). While Hispanics are at increased risk for NCI and neurocognitive decline, factors explaining this disparity are not clear (Marquine et al., Reference Marquine, Heaton, Johnson, Rivera-Mindt, Cherner, Bloss, Hulgan, Umlauf, Moore and Fazeli2018; Mindt et al., Reference Mindt, Miranda, Arentoft, Byrd, Monzones, Fuentes, Arias, Rentería, Rosario and Morgello2014; Watson et al., Reference Watson, Kamalyan, Tang, Hussain, Cherner, Rivera Mindt, Byrd, Franklin, Collier, Clifford, Gelman, Morgello, McCutchan, Ellis, Grant, Heaton and Marquine2022).
Emotional disorders characterized by negative affect such as depression and anxiety are prevalent in PWH. Rates of depression and anxiety are higher in PWH than the general population at approximately 20% and 50%, respectively (Ciesla & Roberts, Reference Ciesla and Roberts2001; Fazeli et al., Reference Fazeli, Marceaux, Vance, Slater and Long2011). Similarly, PWH report higher rates of loneliness, which may contribute to high rates of mood and substance use challenges (Edelman et al., Reference Edelman, Tetrault and Fiellin2014; Greene et al., Reference Greene, Hessol, Perissinotto, Zepf, Parrott, Foreman, Whirry, Gandhi and John2018; Grov et al., Reference Grov, Golub, Parsons, Brennan and Karpiak2010; Heywood & Lyons, Reference Heywood and Lyons2016) and have critical implications for the quality of life and disease progression of PWH. Depressive symptoms have been associated with worse medication adherence, which may lead to lower CD4 count and higher HIV plasma viral load and contribute to cognitive impairment (Heaton et al., Reference Heaton, Clifford, Franklin, Woods, Ake, Vaida, Ellis, Letendre, Marcotte, Atkinson, Rivera-Mindt, Vigil, Taylor, Collier, Marra, Gelman, McArthur, Morgello, Simpson, McCutchan, Abramson, Gamst, Fennema-Notestine, Jernigan, Wong and Grant2010; Scott et al., Reference Scott, Byrd, Rentería, Coulehan, Miranda, Fuentes and Mindt2018).
Some literature indicates that Hispanics are at increased risk for adverse emotional health (i.e, higher rates of depression and anxiety) in comparison to Whites (Hernandez et al., Reference Hernandez, Plant, Sachs-Ericsson and Joiner2005; Pratt & Brody, Reference Pratt and Brody2014), while other studies show Hispanic ethnicity is associated with positive emotional health including less loneliness (Gallegos & Segrin, Reference Gallegos and Segrin2021), better psychological well-being (Losada et al., Reference Losada, Robinson Shurgot, Knight, Márquez, Montorio, Izal and Ruiz2006) and life satisfaction (Calvo et al., Reference Calvo, Carr and Matz-Costa2017; Marquine et al., Reference Marquine, Maldonado, Zlatar, Moore, Martin, Palmer and Jeste2015). Yet, other research indicates comparable levels between groups (Breslau et al., Reference Breslau, Aguilar-Gaxiola, Kendler, Su, Williams and Kessler2006; Woodward et al., Reference Woodward, Taylor, Bullard, Aranda, Lincoln and Chatters2012). Using the NIH Toolbox Emotion Battery (NIHTB-EB), studies found that Hispanics reported better social satisfaction (emotional support, friendship, and loneliness) and psychological well-being (life satisfaction, meaning and purpose) than Whites (Zahodne et al., Reference Zahodne, Sharifian, Kraal, Sol, Zaheed, Manly and Brickman2021; Zahodne et al., Reference Zahodne, Watson, Seehra and Martinez2018). Yet, comprehensive studies evaluating ethnic differences in emotional health among diverse PWH are lacking.
Social and emotional health has important implications for neurocognition. Worse depressive symptoms, anxiety, discrimination, acculturative and perceived stress have been linked to worse neurocognition in Hispanics (Camacho et al., Reference Camacho, Tarraf, Jimenez, Gallo, Gonzalez, Kaplan, Lamar, Khambaty, Thyagarajan, Perreira, Hernandez, Cai, Daviglus, Wassertheil-Smoller and González2018; Estrella et al., Reference Estrella, Durazo-Arvizu, Gallo, Tarraf, Isasi, Perreira, Zeng, Marquine, Lipton, González, Daviglus and Lamar2021; Marquine et al., Reference Marquine, Gallo, Tarraf, Wu, Moore, Vásquez, Talavera, Allison, Muñoz, Isasi, Perreira, Bigornia, Daviglus, Estrella, Zeng and González2022; Muñoz et al., Reference Muñoz, Gallo, Hua, Sliwinski, Kaplan, Lipton, González, Penedo, Tarraf, Daviglus, Llabre and Isasi2019). Other studies show lower loneliness, greater purpose of life, social, and familial support are linked with better neurocognitive and mental health outcomes in Hispanics (Chavez-Korell et al., Reference Chavez-Korell, Benson-Flórez, Rendón and Farías2013; Estrella et al., Reference Estrella, Durazo-Arvizu, Gallo, Tarraf, Isasi, Perreira, Zeng, Marquine, Lipton, González, Daviglus and Lamar2021; Mulvaney-Day et al., Reference Mulvaney-Day, Alegría and Sribney2007; Valdivieso-Mora et al., Reference Valdivieso-Mora, Peet, Garnier-Villarreal, Salazar-Villanea and Johnson2016). A cross-sectional study among older community-dwelling adults of diverse backgrounds utilizing the NIHTB Emotion and Cognition batteries showed differential ethnic associations between emotion and cognition (Zahodne et al., Reference Zahodne, Watson, Seehra and Martinez2018). In this study, greater emotional support and higher purpose in life were associated with worse working memory in Hispanics, but not among non-Hispanics (Zahodne et al., Reference Zahodne, Watson, Seehra and Martinez2018). Greater friendship was associated with better working memory in Whites, but this association was non-significant among Hispanics. Yet, a similar longitudinal study using the NIHTB revealed that higher friendship was associated with less neurocognitive decline across Hispanics and Whites (Zahodne et al., Reference Zahodne, Sharifian, Kraal, Sol, Zaheed, Manly and Brickman2021). In contrast to Zahodne’s studies with healthy diverse older adults, our study including middle-aged adults with HIV might provide further insight into the effects of age and health status on emotional and neurocognitive health.
Emotional difficulties such as stress and trauma have also been associated with increased risk for HIV-associated neurocognitive impairment (Rubin et al., Reference Rubin, Cook, Weber, Cohen, Martin, Valcour, Milam, Anastos, Young, Alden and Gustafson2015; Watson et al., Reference Watson, Sundermann, Hussain, Umlauf, Thames, Moore, Letendre, Jeste, Morgan and Moore2019). Relatedly, loneliness and social isolation in adults with and without HIV have been associated with worse neurocognition (Han et al., Reference Han, Adeyemi, Wilson, Leurgans, Jimenez, Oullet, Shah, Landay, Bennett and Barnes2017; Kelly et al., Reference Kelly, Duff, Kelly, McHugh Power, Brennan, Lawlor and Loughrey2017; Wilson et al., Reference Wilson, Krueger, Arnold, Schneider, Kelly, Barnes, Tang and Bennett2007). Yet, investigations of ethnic differences in emotional health among PWH, and the link between emotional health and neurocognition among Hispanic PWH are limited.
The current study aimed to (1) characterize and compare emotional health in Hispanic and White PWH and (2) investigate the associations between emotional health and neurocognition across Hispanic and White PWH utilizing the NIHTB Emotion and Cognition batteries. Considering the heterogeneity within the US Hispanic population, we also examined whether there were differences within Hispanics on our main outcomes of interest based on primary language (English/Spanish), which is closely linked to other culturally relevant factors (e.g., acculturation, country of birth, years living in the USA). Increased understanding of emotional health and its link to neurocognition among diverse PWH might shed light on mechanisms of HIV-associated neurocognitive dysfunction that are most relevant for different cultural groups. This is an important initial step towards the development of culturally-relevant interventions that consider culture specific mechanisms of HIV-associatated neurocognitive dysfunction, and addressing neurocognitive disparities (Thomas et al., Reference Thomas, Quinn, Butler, Fryer and Garza2011).
Methods
Participants
Participants included 323 (107 Hispanic and 216 White) PWH recruited from the San Diego area and enrolled in observational cohort studies at the UCSD HIV Neurobehavioral Research Program (HNRP) from 2014 to 2020. Exclusion criteria for these cohort studies include history of head injury with loss of consciousness greater than 30 min or other severe neuromedical comorbidities that may affect cognitive functioning (i.e., stroke, epilepsy, opportunistic CNS infection). Participants who tested positive on urine toxicology or breathalyzer tests on the day of neuropsychological testing were rescheduled. Detailed descriptions of these studies can be found in prior reports (Doyle et al., Reference Doyle, Morgan, Morris, Smith, Little, Iudicello, Blackstone, Moore, Grant, Letendre and Woods2013; Heaton, Franklin, et al., Reference Heaton, Franklin, Deutsch, Letendre, Ellis, Casaletto, Marquine, Woods, Vaida, Atkinson, Marcotte, McCutchan, Collier, Marra, Clifford, Gelman, Sacktor, Morgello, Simpson, Abramson, Gamst, Fennema-Notestine, Smith and Grant2014). All data were obtained in compliance with the Helsinki Declaration and approved by the ethics committee of the UCSD Institutional Review Board. Participants demonstrated decisional capacity to consent, provided written informed consent, and were compensated for their participation. Inclusion criteria for present analyses were self-identifying as Hispanic or White, available National Institute of Health Toolbox Cognition Battery (NIHTB-CB) data, and at least two of the three National Institute of Health Toolbox Emotion Battery (NIHTB-EB) summary T-scores (e.g., negative affect, psychological well-being, and social satisfaction) and their component scales administered at the same visit. Data from the first visit that the NIHTB was administered were used for this cross-sectional study.
Materials and procedures
Participants completed comprehensive neurocognitive, neuromedical, and psychiatric assessments. Sociodemographic information (age, sex, years of education, sexual orientation, employment status) was ascertained via self-report. Language of test administration was determined based on participants self-reported fluency in English and Spanish, and language preference. Specifically, participants reported how well they spoke English and Spanish using a Likert-type scale (0 = not well to 3 = very well), and were tested in the language that they reported having greater fluency on. Participants reporting equal fluency in both languages were tested in their preferred language (Cherner et al., Reference Cherner, Suarez, Lazzaretto, Fortuny, Mindt, Dawes, Marcotte, Grant and Heaton2007; Mungas et al., Reference Mungas, Reed, Crane, Haan and González2004). Spanish-speaking participants were evaluated by trained English-Spanish bilingual and bicultural staff.
Neurocognitive assessment
The NIHTB-CB was used to assess neurocognition (Heaton, Akshoomoff, et al., Reference Heaton2014; Weintraub et al., Reference Weintraub, Dikmen, Heaton, Tulsky, Zelazo, Bauer, Carlozzi, Slotkin, Blitz, Wallner-Allen, Fox, Beaumont, Mungas, Nowinski, Richler, Deocampo, Anderson, Manly, Borosh, Havlik and Gershon2013; Weintraub et al., Reference Weintraub, Dikmen, Heaton, Tulsky, Zelazo, Slotkin, Slotkin, Carlozzi, Bauer, Wallner-Allen, Fox, Havlik, Beaumont, Mungas, Manly, Moy, Conway, Edwards, Nowinski and Gershon2014). One of the NIHTB-CB composite scores is Fluid Cognition, which measures attention, executive function, episodic memory, working memory, and processing speed. These cognitive domains are most likely to be impacted by HAND (Akshoomoff et al., Reference Akshoomoff2013; Heaton, Franklin, et al., Reference Heaton, Franklin, Deutsch, Letendre, Ellis, Casaletto, Marquine, Woods, Vaida, Atkinson, Marcotte, McCutchan, Collier, Marra, Clifford, Gelman, Sacktor, Morgello, Simpson, Abramson, Gamst, Fennema-Notestine, Smith and Grant2014). The primary outcome of our analyses was demographically-adjusted Fluid Cognition T-scores that correct for age, gender, education, and ethnicity/race with different norms for English and Spanish-speakers (Casaletto et al., Reference Casaletto, Umlauf, Beaumont, Gershon, Slotkin, Akshoomoff and Heaton2015; Casaletto et al., Reference Casaletto2016).
Emotional health assessment
Emotional health was assessed using the NIHTB-EB (Salsman et al., Reference Salsman, Butt, Pilkonis, Cyranowski, Zill, Hendrie, Kupst, Kelly, Bode, Choi, Lai, Griffith, Stoney, Brouwers, Knox and Cella2013), comprised of 13 individual scales grouped into three summary scores based on prior confirmatory factor analyses: negative affect (i.e., anger affect, anger hostility, sadness, fear affect, and perceived stress), social satisfaction (i.e., friendship, emotional support, instrumental support, and reverse-coded loneliness and perceived rejection), and psychological well-being (i.e., meaning and purpose, life satisfaction, and positive affect) (Babakhanyan et al., Reference Babakhanyan, McKenna, Casaletto, Nowinski and Heaton2018). Raw scores for each individual scale were converted to normalized T-scores reflecting an individual’s emotional characteristic in relation to the average English or Spanish-speaker in the USA. T-scores for English-speakers are based on Census-weighed normative data, whereas T-scores for Spanish-speakers are based on sample-weighted norms (Babakhanyan et al., Reference Babakhanyan, McKenna, Casaletto, Nowinski and Heaton2018). Main predictors were negative affect, social satisfaction, and psychological well-being summary T-scores. To aid in the clinical interpretation of emotional health summary T-scores, those beyond one SD in the direction of distress (i.e., negative affect T-scores > 60, psychological well-being T-scores < 40, and social satisfaction T-scores < 40) were categorized as “problematic” (Babakhanyan et al., Reference Babakhanyan, McKenna, Casaletto, Nowinski and Heaton2018). Notable average T-scores that were at least 4 scores from the normative mean of 50 were identified as lower or higher emotional health than either census weighted or sample weighted normative sample. The 13 individual scales that comprise the summary scores were similarly evaluated.
Neuromedical assessment
Neuromedical assessments included a structured medical interview, neurological examination, blood draw, and urine sample collection. AIDS status, estimated years of HIV disease, antiretroviral therapy (ART) regimen, and months of exposure to ART were obtained via self-report. Laboratory measurements consisted of clinical chemistry panels, blood counts, rapid plasma reagin (screen for syphilis), Hepatitis-C (HCV) antibody, CD4+ T cells (flow cytometry), and urine toxicology. Procedures were performed at a Clinical Laboratory Improvement Amendments (CLIA)-certified, or CLIA-equivalent, laboratory. HIV disease diagnosis was confirmed by enzyme-linked immunosorbent assay with Western blot confirmation. HIV RNA levels in plasma were measured by reverse transcriptase polymerase chain reaction (Roche Amplicor, v. 1.5, lower limit of quantitation 50 copies/milliliter) to ascertain detectability of plasma HIV RNA.
Psychiatric and substance use assessments
Participants completed the Composite International Diagnostic Interview (Version 2.1) (Kessler et al., Reference Kessler, Andrews, Mroczek, Ustun and Wittchen1998; Wittchen Reference Wittchen1994). Diagnoses for current (within past 12 months) and lifetime Major Depressive Disorder and Substance Use Disorders for alcohol, cannabis, opioids, methamphetamine, cocaine, sedatives, and hallucinogens were assigned based on the Diagnostic and Statistical Manual-Fourth Edition (DSM-IV).
Statistical analyses
Sample characteristics were examined for and met parametric assumptions. Differences in demographics, HIV disease and psychiatric characteristics, and Fluid Cognition T-scores were compared between Hispanics and Whites (and between primarily Spanish- or English-speaking Hispanics) using Chi 2 (or Fisher’s exact) and independent sample t-tests as appropriate.
For our first aim, we compared NIHTB-EB summary and individual scale T-scores by ethnicity (and language group within Hispanics) via a series of independent sample t-tests. For summary and individual scale T-scores that differed by group, we conducted separate linear regression models, using ethnicity (or language group within Hispanics) as the predictor, adjusting for covariates (i.e., demographic, HIV, psychiatric, and substance use characteristics that significantly differed between groups at α <.10).
For our second aim, we ran three separate multivariable linear regression models examining the association between each of the three Emotion summary T-scores on Fluid Cognition T-scores by ethnicity. Each model included terms for (1) ethnicity; (2) the Emotion summary T-scores of interest; (3) the two-way interactive effects between these two variables; and (4) significant covariates (demographic, HIV, psychiatric, and substance use characteristics that differed between ethnicity and/or were univariably associated with Fluid Cognition at α < .10 among the overall sample). Variables and interaction terms that were not significant at α > .10 were removed and models rerun. Significant interaction effects were followed up with stratified models by ethnicity. For Emotion summary T-scores that showed a significant link with Fluid Cognition T-scores, we examined the association between the individual scales comprising the summary score and Fluid Cognition T-scores. We additionally examined interaction effects between Emotion summary T-scores and Hispanic language group on Fluid Cognition T-scores using similar procedures for models by ethnicity described above. Analyses were conducted using JMP software package (version 14.0) and α<.05 was used to determine significance in final models. R version 3.5.0 was used to create all figures.
Results
Sample characteristics
Demographic, HIV disease, psychiatric, and substance use characteristics for the overall sample and stratified by ethnicity are summarized in Table 1. Among demographic, HIV disease, psychiatric and substance use characteristics, Hispanics were significantly younger, had fewer years of education, fewer estimated years of HIV infection, fewer months of exposure to ART, fewer gay or bisexual individuals, lower prevalence of lifetime MDD, lifetime cannabis, and cocaine use disorder than Whites. All other sample characteristics did not significantly differ by ethnicity (Table 1). There were no significant differences on Fluid Cognition T-scores (p = .42) between Hispanics (M = 45.48, SD = 9.91) and Whites (M = 46.44, SD = 10.91), but Hispanics scored lower on the Flanker Inhibitory Control and Attention Test (Hispanics: M = 40.73, SD = 12.27; Whites: M = 43.64, SD = 9.30; p = .03); and the Picture Sequence Memory Test (Hispanics: M = 47.34, SD = 8.76; Whites: M = 49.69, SD = 10.13; p = .03), with no significant ethnic differences on other tests (ps >.14). Within Hispanics, 44 were tested in Spanish and 63 were tested in English, and the majority (80%) were of Mexican origin/descent (i.e., country that participant or family immigrated from).
Table 1. Participant characteristics for the overall sample and stratified by ethnicity
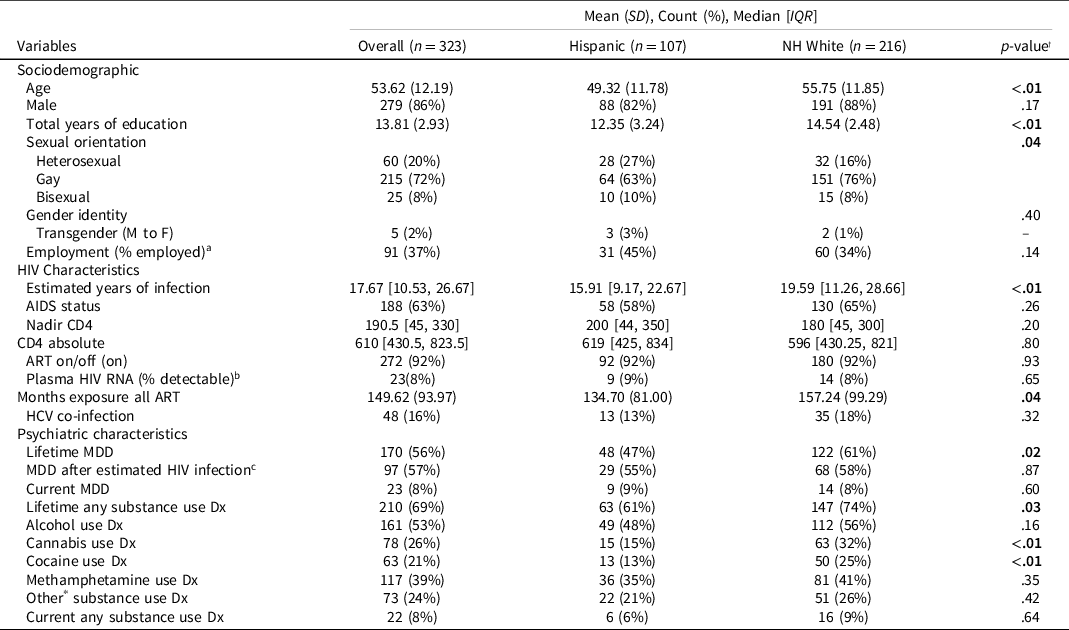
Note. IQR = interquartile range; SD = standard deviation; NH = Non-Hispanic; ART = antiretroviral therapy; HCV = Hepatitis-C; MDD = Major Depressive Disorder; Dx = disorder; NCI = neurocognitive impairment.
† Comparisons of ethnic group (e.g. Hispanic vs Non-Hispanic (NH) White) are calculated using χ2-tests or independent sample t-tests as appropriate.
a Indicates n = 246 (69 Hispanics and 177 NH Whites).
b Indicates n = 277 (96 Hispanics and 181 NH Whites).
c Indicates n = 172 (51 Hispanics and 121 NH Whites).
* Other category included hallucinogen, inhalant, opioid, PCP, and sedative substance use.
Table 2 shows descriptive characteristics of the Hispanic sample by primary language. Spanish-speakers were significantly older, more likely to be female, had fewer years of education, and more likely to be of Mexican origin/descent (93.2%), compared to English-speaking Hispanics (73.8% Mexican origin/descent). Spanish-speakers were more likely to present with MDD after HIV disease infection, had significantly longer estimated duration of HIV disease, more months of exposure to ART, were significantly less likely to have a lifetime diagnosis of any substance use disorder, specifically, less likely to have a lifetime diagnosis of methamphetamine or “other” substance use disorder (hallucinogen, inhalant, opioid, PCP, and sedative) than English-speaking Hispanics. All other sample characteristics in Hispanics did not significantly differ by language group (Table 2). There were no significant differences in Fluid Cognition T-scores by primary language group (Spanish-speakers: M = 46.93, SD = 8.07; English-speakers: M = 44.47, SD = 10.97; p = .18), but English-speaking Hispanics scored significantly lower on the Flanker Inhibitory Control and Attention Test (English-speakers: M = 37.78, SD = 13.82; Spanish-speakers: M = 44.97, SD = 8.01; p < .01) and the Picture Sequence Memory Test (English-speakers: M = 45.85, SD = 9.27; Spanish-speakers: M = 49.47, SD = 7.57; p = .03), with no significant differences by language group on other tests (ps>.66).
Table 2. Participant characteristics for Hispanics stratified by primary language
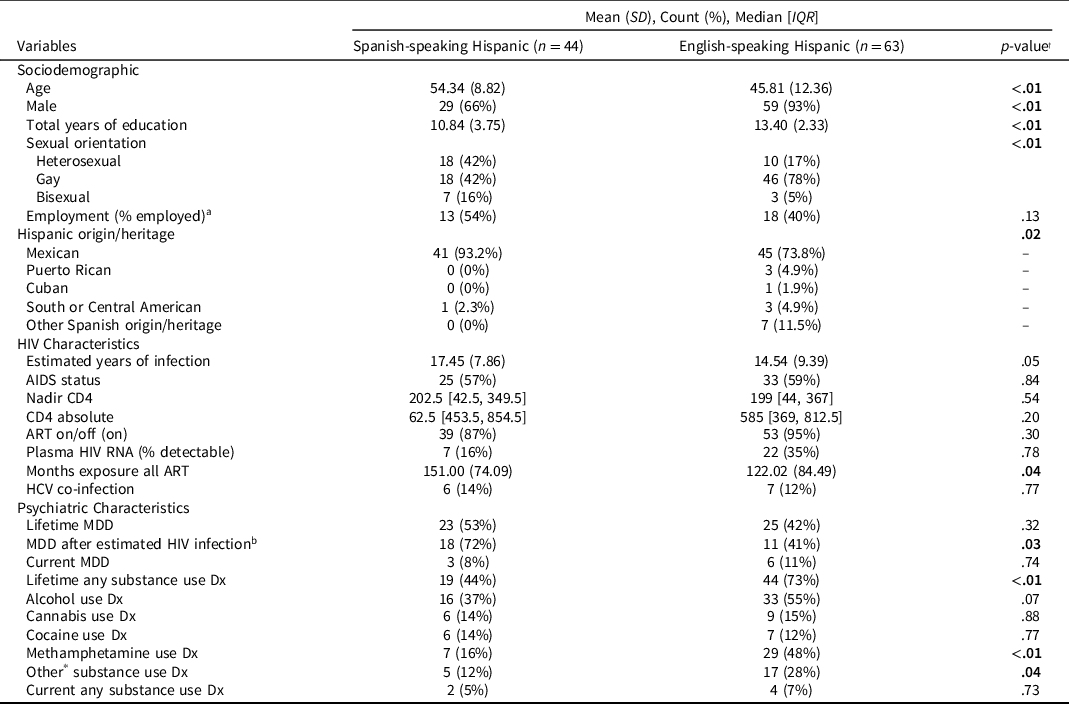
Note. IQR=interquartile range; SD = standard deviation; ART = antiretroviral therapy; HCV = Hepatitis-C; MDD = Major Depressive Disorder; Dx = disorder.
† Comparisons of language group (e.g. primarily Spanish-speaking vs primarily English-speaking) are calculated using χ2-tests or independent sample t-tests as appropriate.
a Indicates n = 51 (24 Spanish speakers and 45 English speakers).
b Indicates n = 51 (26 Spanish speakers and 25 English speakers)
* Other category included hallucinogen, inhalant, opioid, PCP, and sedative substance use.
Emotional health among ethnically and linguistically diverse PWH
Figure 1 presents data on the NIH TB Emotion summary and individual scale T-scores by ethnicity and language group within Hispanics, and comparisons between these groups based on independent sample t-tests.
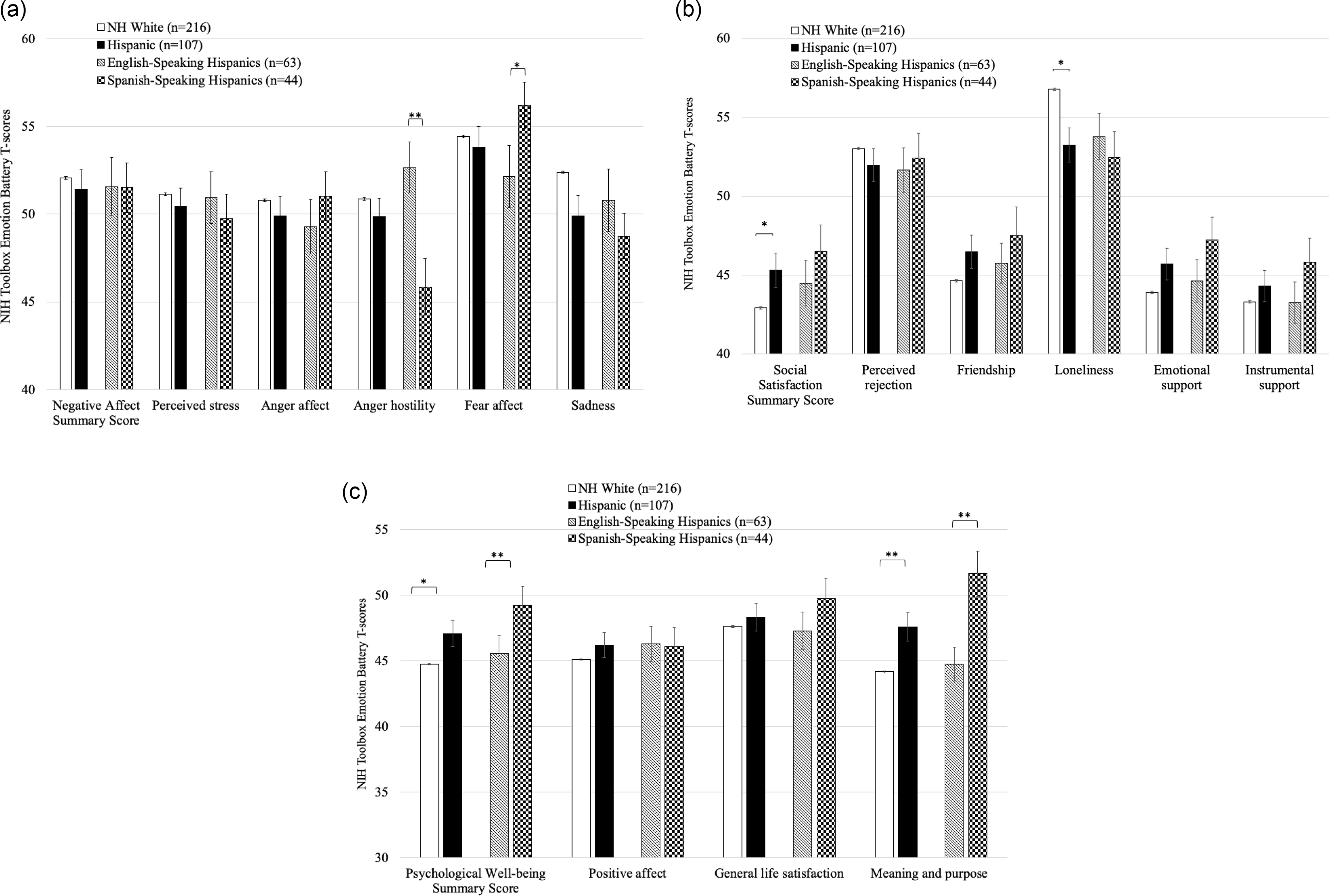
Figure 1. Comparisons on the NIH Toolbox Emotion Battery summary T-scores (Figure 1a: negative affect; Figure 1b: social satisfaction; Figure 1c: psychological well-being) and individual scales comprising these summary scores, by ethnicity (Hispanic vs Non-Hispanic White) and language group within Hispanics (English-and Spanish-speaking) based on independent sample t-tests (unadjusted for covariates). *p < .05, **p < .01.
Regarding negative affect (Figure 1a), there were no significant group differences between Hispanic and White PWH on the summary score or the individual scales. Within Hispanic PWH, Spanish-speakers reported significantly lower anger hostility (Cohen’s d =−.62), but higher fear affect (Cohen’s d = .34) than English-speakers. After controlling for significant covariates (i.e., age, gender, education, sexual orientation, estimated years of infection, months of exposure to ART, lifetime alcohol, cannabis, cocaine, methamphetamine, and other substance use diagnoses), Spanish-speaking Hispanics still had significantly lower anger hostility (β = −6.82, 95% CI = −10.88 to −2.76, p = .001) and higher fear affect (β = 5.72, 95% CI =.88 to 10.56, p = .02). Group mean T-scores of negative affect were generally within five T-score points of the normative mean of 50 for White and Hispanic PWH. Twenty-seven percent of the overall sample showed problematic negative affect scores, with no significant differences between Whites (28%) and Hispanics (23%, p = .35). Within Hispanic PWH, 26% of English-speakers and 17% of Spanish-speakers showed problematic negative affect scores (p = .42), with Spanish-speaking Hispanics showing significantly low anger hostility (M = 45.84, SD = 10.66) but elevated fear affect (M = 56.22, SD = 8.76).
Regarding social satisfaction (Figure 1b), Hispanic PWH had significantly higher summary T-scores than White PWH (Cohen’s d = .22). Both groups showed average scores more than half a SD below the normative mean, and 39% of the overall sample showed problematic social satisfaction scores (42% in Whites and 34% in Hispanics, p = .14). Hispanics reported significantly less loneliness than Whites (Cohen’s d=.31). After controlling for significant covariates, there were no longer significant ethnic differences on social satisfaction summary T-scores (β = 2.47, 95% CI = −.18 to 5.11, p = .068). However, Hispanics continued to show significantly lower loneliness (β = −3.91, 95% CI = −6.68 to −1.15, p = .006) than Whites. There were no significant differences in social satisfaction summary T-score or individual scales by language group within Hispanic PWH, and proportions of problematic social satisfaction scores were notable in both language groups (40% in English- and 25% in Spanish-speaking Hispanic PWH, p =.15).
Regarding psychological well-being (Figure 1c), Hispanics showed significantly higher summary T-scores than Whites (Cohen’s d = .29), the latter had average scores more than five T-scores below the normative mean (M = 44.73, SD = 10.11). Thirty percent of the overall sample showed problematic psychological well-being scores (Whites = 32%, Hispanics = 25% in, p = .20). Hispanics showed significantly higher meaning and purpose than Whites (Cohen’s d = .64). After controlling for significant covariates, Hispanics continued to have significantly higher psychological well-being (β = 2.53, 95% CI = .008 to 5.06, p = .0492) summary T-scores, and significantly higher meaning and purpose T-scores (β = 3.10, 95% CI = .48 to 5.71, p = .02) than Whites. Spanish-speaking Hispanics scored significantly higher on the psychological well-being summary T-score, and on meaning and purpose, than English-speakers, even after controlling for significant covariates (psychological well-being: β = 4.99, 95% CI = .60 to 9.38, p = .03; meaning and purpose: β = 9.30, 95% CI = 4.31 to 14.29, p = 0.0004). There were no significant language group differences in proportions of problematic psychological well-being sumary scores within Hispanic PWH (English-speakers = 26%; Spanish-speakers=25%; p = .93).
Associations between emotional health and cognition among ethnically and linguistically diverse PWH
Table 3 shows results of final models examining the association between NIHTB-EB summary T-scores and Fluid Cognition T-scores by ethnicity, after adjusting for significant covariates. Table 3, Model A depicts the final model results for negative affect, showing a significant interaction (p = .02) between ethnicity and negative affect T-scores on Fluid Cognition T-scores. Follow-up models stratified by ethnicity indicated a significant association between higher negative affect T-scores and worse Fluid Cognition T-scores among Whites (β = −.17, 95% CI = −.32 to −.03, p = .02), but no significant association in Hispanics (β = .16, 95% CI = −.06 to .37, p = .15).
Table 3. Results of final multivariable models depicting associations between NIHTB Emotion Battery summary T-scores (negative affect, social satisfaction, and psychological well-being) and Fluid Cognition T-scores among PWH

a Represents NIHTB-EB summary TS entered as predictor in each of three separate linear regression analyses: Negative Affect (Model A), Social Satisfaction (Model B), and Psychological Well-Being (Model C). NH = Non-Hispanic; EB = Emotion Battery; TS = T-score; ART = Antiretroviral therapy; β = estimate; CI = Confidence Interval.
There was no significant ethnicity and social satisfaction interaction on Fluid Cognition T-scores (p = .26). Thus, we removed the interaction term and re-ran the model. Table 3, Model B shows results of the final model for social satisfaction T-scores, such that there was a positive association between social satisfaction and Fluid Cognition T-scores in the overall sample (p = .01).
We did not find a significant interaction of ethnicity and psychological well-being on Fluid Cognition T-scores (p = .58), therefore we removed the interaction term and re-ran the model. Table 3, Model C shows no significant association between psychological well-being and Fluid Cognition T-scores in the final model (p = .54).
To further understand factors driving the interaction between negative affect and ethnicity on neurocognition, we investigated the individual scales which comprise this summary score as predictors of Fluid Cognition, using separate models comparable to those run using the negative affect summary T-score. Figure 2 depicts an interaction, showing higher fear affect (β = −.15, 95% CI = −.29 to −.008, p = .04; Figure 2a), perceived stress (β = −.20, 95% CI = −.34 to −.06; p = .01; Figure 2b), and sadness (β = −.14, 95% CI = −.26 to −.02, p = .03; Figure 2c), were significantly associated with lower Fluid Cognition T-scores in Whites, but not Hispanics (perceived stress: β = .13, 95% CI = −.06 to .31, p = .18; fear affect: β = .15, 95% CI = −.007 to .31, p = .06; sadness: β = .08, 95% CI = −.08 to .25, p = .33). The respective interactions of ethnicity with anger affect and anger hostility on Fluid Cognition T-scores were not significant, and there were no significant main effects of these individual scale T-scores on Fluid Cognition (Figures 2d and 2e; ps >.05).
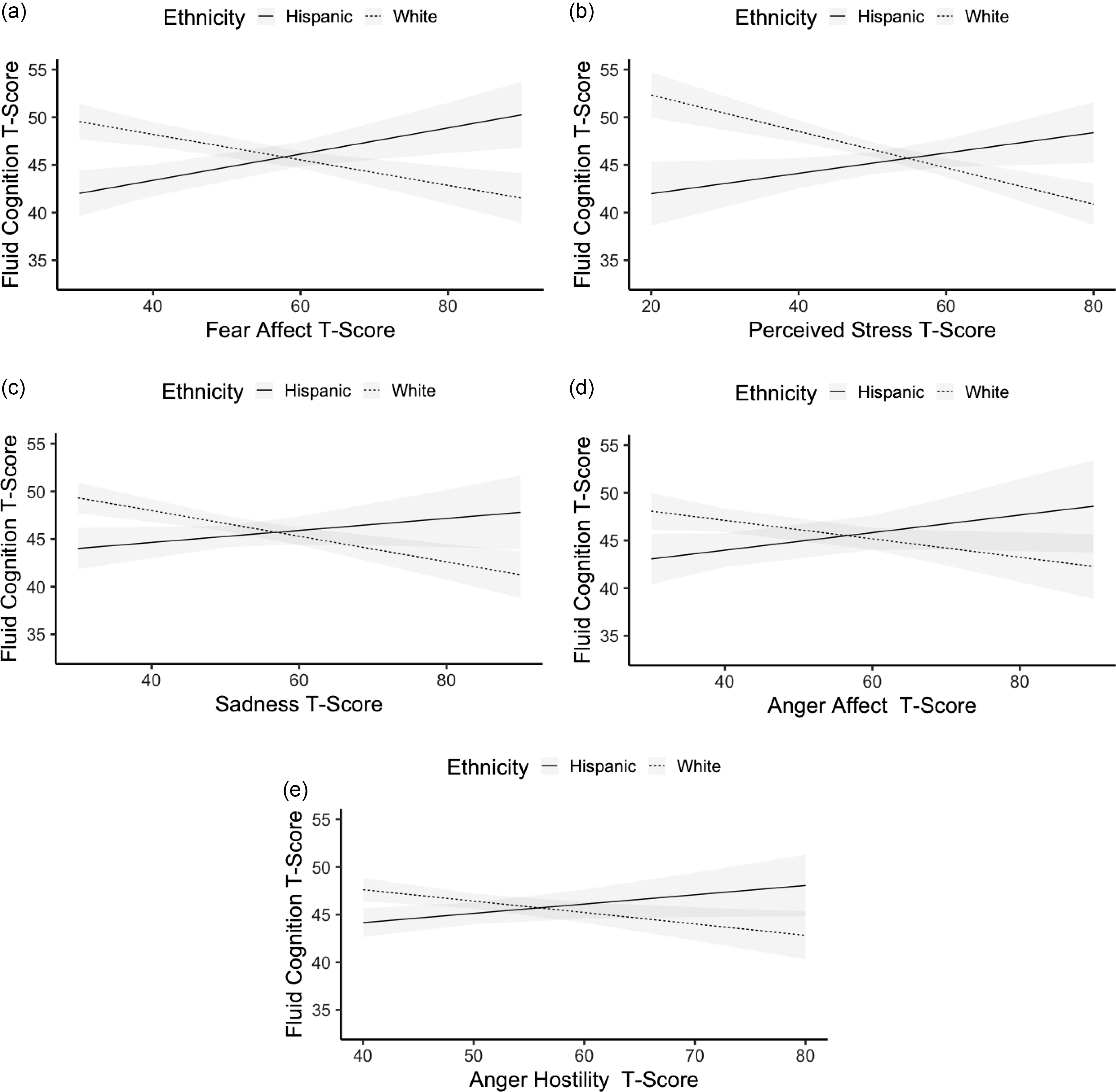
Figure 2. Results from linear regression models examining modifications in associations between scales comprising the NIHTB-EB negative affect summary scores and Fluid Cognition by ethnicity, adjusting for significant covariates. Results from interaction terms for each of the models were as follows:
Fig.2a. Ethnicity X Fear Affect: β = .28; SE = .11; CI = .05 to .50; p = .02. Fig.2b. Ethnicity X Perceived Stress: β = .33; SE = .12; CI = .09 to .58; p = .008. Fig.2c. Ethnicity X Sadness: β = .22; SE = .11; CI = .001 to .44; p = .049.Fig.2d. Ethnicity X Anger Affect: β = .21; SE = .15; CI = -.09 to .50; p = .17. Fig.2e. Ethnicity X Anger Hostility: β = .22; SE = .13; CI = -.04 to .47; p = .09.
To examine whether specific scales might be driving the main effect of social satisfaction on neurocognition in the overall sample, we ran models comparable to the final model on social satisfaction with each individual scale within this summary score as the predictor. Results revealed that higher emotional support (β = .14, 95% CI = .03 to .25, p = .02), higher friendship (β = .19, 95% CI = .08 to .31, p < .01) and lower perceived rejection (β = −.13, 95% CI = −.24 to −.02, p = .02) were significantly associated with higher Fluid Cognition T-scores in the overall sample, while associations with instrumental support (β = .02, 95% CI = −.10 to .14, p = .75; Figure 2c) and loneliness (β = −.09, 95% CI = −.20 to .02, p = .11) were not significant.
We further assessed if primary language modified the influence of each emotional health summary score on neurocognition among Hispanic PWH. Results showed no significant interaction, such that primary language did not significantly modify the association of negative affect (β = .30, 95% CI = −.28 to .88, p = .31), social satisfaction (β = −.06, 95% CI = −.27 to .14, p = .55), nor psychological well-being (β = −.40, 95% CI = −.86 to .06, p = .09) on Fluid Cognition T-scores among Hispanic PWH.
Discussion
The first aim of this study was to characterize and compare emotional health in Hispanic and White PWH. Importantly, findings reveal that 27%-39% of the present cohort showed problematic scores in at least one aspect of emotional health. Analyses of continuous Emotion summary T-scores showed that Hispanic PWH reported better scores in some aspects of emotional health (i.e., social satisfaction summary, loneliness, psychological well-being summary, and meaning and purpose), though some of these scores were still normatively poor. Within Hispanics, Spanish-speakers reported better scores in some aspects of emotional health (i.e. psychological well-being, meaning and purpose, anger hostility) but worse scores in others (i.e., fear affect) than English-speakers. Our second aim was to investigate the association between emotional health and neurocognition among Hispanic and White PWH. We found that worse negative affect was associated with worse neurocognition in White, but not Hispanic PWH. As for other aspects of emotional health, worse social satisfaction was linked to worse neurocognitive performance across ethnicity, while there was no significant association between psychological well-being and neurocognition.
We also found that there were no significant ethnic group differences on global fluid cognition, but that Hispanics with HIV obtained lower T-scores on some of the individual tests comprising this composite compared to non-Hispanic Whites with HIV. Neurocognitive scores were demographically-adjusted (i.e., accounted for the influence of age, gender, and years education on normal variations on test performance within different ethnic/racial and language groups. Thus, these neurocognitive differences are likely due to factors associated with the experience of living with HIV and being Hispanic, and are in line with prior findings indicating neurocognitive disparities among Hispanics with HIV (e.g., Watson et al., Reference Watson, Kamalyan, Tang, Hussain, Cherner, Rivera Mindt, Byrd, Franklin, Collier, Clifford, Gelman, Morgello, McCutchan, Ellis, Grant, Heaton and Marquine2022).
A notable proportion of both White and Hispanic PWH showed problematic negative affect, though there were no significant ethnic differences on this summary score nor its individual scales. Yet, Spanish-speakers showed decreased anger hostility (feelings of antagonism or animosity), but increased fear affect (anxiety over perceptions of threat) than English-speaking Hispanics. Primary language among Hispanics in the USA is closely linked to other factors (e.g., acculturation, country of birth, years living in the USA, socioeconomic status) (Fujii, Reference Fujii2017; Hazuda et al., Reference Hazuda, Stern and Haffner1988), which might help explain these differences. For example, it might be the case that increased fear affect among Spanish-speakers is related to increased immigration status anxieties in this group, whom are more likely to have been born in a country other than the USA. Future studies directly assessing these factors would be best suited to explain the observed differences. Yet, the present findings underscore the importance of considering Hispanic heterogeneity to best understand emotional health among diverse PWH.
Social support and perceptions of social relationships were notably poor in our sample of PWH, relative to normative expectations. Hispanics showed less severe difficulties in this aspect of emotional health, particularly as it related to feelings of loneliness and social isolation. This is congruent with previous findings showing less loneliness among older Hispanics without HIV than their White counterparts (Zahodne et al., Reference Zahodne, Watson, Seehra and Martinez2018). This prior study also showed higher emotional support, friendship, and instrumental support among Hispanics. As we did not replicate this finding in our sample of PWH, living with HIV might be linked to decreased social support. Additional research should include Hispanics and Whites with and without HIV to best elucidate whether social support is particularly impacted among White PWH.
Psychological well-being was also quite low in our cohort, particularly among White and English-speaking Hispanic PWH. Spanish-speaking Hispanic PWH showed a relative strength in psychological well-being, particularly in feeling that their lives were meaningful. If English language use is interpreted as a dimension of acculturation, these results suggest that greater adherence to Hispanic culture might be linked to higher psychological well-being, particularly higher meaning and purpose. This is in line with prior findings showing higher meaning and purpose in older Hispanics than Whites without HIV (Zahodne et al., Reference Zahodne, Watson, Seehra and Martinez2018).
Worse negative affect was associated with worse neurocognition among White PWH, but not among Hispanic PWH. Analyses within individual negative affect scales showed similar associations by ethnicity related to fear affect, perceived stress, and sadness. This contrasts with another NIHTB study of predominantly White healthy older adults in which negative affect was not associated with neurocogntion (Zahodne et al., Reference Zahodne, Nowinski, Gershon and Manly2014). Our differing findings might be due to greater prevalence of NCI in PWH relative to the general population. Alternatively, our results suggest that factors specific to Hispanic ethnicity may buffer the adverse impact of negative affect on neurocognition in PWH. For example, less feelings of loneliness could be indicative of a more active social life, and greater socialization could expose individuals to more cognitively stimulating activities.
Social satisfaction had a positive association with neurocognition across ethnicity. This is consistent with prior research showing the benefits of social networks, social support, (Atkins et al., Reference Atkins, Rubenstein, Sota, Rueda, Fenta, Bacon and Rourke2010; Bateganya et al., Reference Bateganya, Amanyeiwe, Roxo and Dong2015), higher emotional support, higher friendship and less perceived rejection on neurocognition (Kelly et al., Reference Kelly, Duff, Kelly, McHugh Power, Brennan, Lawlor and Loughrey2017; Zahodne et al., Reference Zahodne, Nowinski, Gershon and Manly2014). Our findings underscore the potential neurocognitive benefit of interventions to improve social satisfaction among PWH across ethnicity.
Though previous research has indicated significant associations between psychological well-being and neurocognition in adults without HIV (Zahodne et al., Reference Zahodne, Watson, Seehra and Martinez2018), we did not replicate this finding in our sample of PWH. Perhaps the impact of HIV disease on the nervous system or other socioemotional factors (e.g. discrimination, stigma) not presently assessed may help explain our lack of a positive association between psychological well-being and neurocognition among diverse PWH. Future research incorporating people with and without HIV might aid in discerning differing links between positive affect and neurocognition.
Our study has several limitations. First, it was cross-sectional in design, and therefore we cannot attribute causation to the associations observed. Although poor socioemotional health may negatively affect neurocognition, the link between emotional functioning and neurocognition may be in the reverse direction. For example, lower neurocognitive functioning, steeper neurocognitive decline, and living with a chronic medical condition may contribute to a decline in the quantity and enjoyment of social interactions, resulting in worse emotional health. A longitudinal study would be best suited to address causality between emotional and neurocognitive change over time.
Given differences in age and education across ethnic groups, we considered matching groups one-on-one based on these demographics. However, matching for age would drastically reduce our NH White sample size by more than 50%, and matching based on education would exclude an important segment of the Hispanic population, limiting generalizability of our findings for this group. Thus, we opted for multivariable models adjusting for differences in demographic characteristics as covariates, as this analytical approach allowed us to maximize sample sizes and preserve statistical power (Vittinghoff et al., Reference Vittinghoff, Glidden, Shiboski and McCulloch2006). Future studies focused on analyzing emotion-cognition associations via a health disparities framework (Hill et al., Reference Hill, Pérez-Stable, Anderson and Bernard2015; National Institute on Minority Health and Health Disparities, 2017) could benefit from recruitment efforts to match participants on key variables.
The generalizability of our results is limited to White and Hispanic PWH living in Southern California. Future research should include other ethnic groups underrepresented in research and/or living in other US regions. While Hispanics other than of Mexican origin/heritage comprised the minority of our Hispanic sample, our Hispanic sample is typical of the US-Mexico border region of Southern California. While there is vast heterogeneity within the Hispanic population in the US, Hispanics in this borderland region share important characteristics (e.g. language use, regional culture). Future larger multisite studies might investigate whether country of origin, US geographic region, and other factors of heterogeneity among US Hispanics modify present findings. While language use is a dimension of acculturation, it is important to recognize the multidimensionality of acculturation was not assessed in our study. As such, measuring Hispanic-specific multidimenstional acculturation factors not included in this study such as cultural values, social affiliations, cultural customs or traditions (Schwartz et al., Reference Schwartz, Unger, Zamboanga and Szapocznik2010) may help expound differential emotion-neurocognition associations by ethnicity.
The present study also has several strengths. The NIHTB-EB assesses a spectrum of detailed positive and negative emotional health variables providing a comprehensive view of emotional health. Additionally, the composite summary scores used in our analyses were based on psychometrically-supported standards using normative samples with English and Spanish speakers (Babakhanyan et al., Reference Babakhanyan, McKenna, Casaletto, Nowinski and Heaton2018). Importantly, our study captures the complexity of emotional health outcomes above and beyond psychiatric diagnoses such as depression and anxiety, which are often times stigmatized, even more so in Hispanic than White groups (Wong et al., Reference Wong, Collins, McBain, Breslau and Audrey2021). Our study goes beyond analyzing potential emotion-neurocognition differences between Hispanics and Whites by also assessing Hispanics by primary language, thus, recognizing the linguistic heterogeneity of Hispanics in the USA.
Overall, present findings indicate that PWH show notable problems in several domains of emotional health. Yet, some Hispanics, particularly those that are primarily Spanish-speaking, appear to have relative strengths in certain aspects of emotional health. These results are an important step towards developing culturally relevant interventions for diverse PWH. For example, treatments aimed at improving social satisfaction might help promote neurocognitive health among diverse PWH. Interventions focused on ameliorating negative affect, while helpful in their own right to improve emotional health, might be less impactful on neurocognition among Hispanics than Whites. Future studies incorporating assessments of culturally relevant constructs potentially linked to emotional and neurocognitive health may inform the development of adequate treatment of HIV-associated neurocognitive impairment in diverse populations of PWH.
Acknowledgements
This work was supported by grants from the National Institutes of Health (The HIV Neurobehavioral Research Center (HNRC): P30MH62512, R01MH57266, K23MH105297, P30AG059299, T32MH019934, R01MD013502, P01DA012065, Traning in Research on Addictions in Interdisciplinary NeuroAIDS (TRAIN): T32DA031098, Alcohol Research Traiing Grant: T32AA013525, and Mentorship for Advancing Diversity in Undergraduate Research on Aging Program (MADURA) Program: R25 AG06650401).
The HIV Neurobehavioral Research Center (HNRC) is supported by Center award P30MH062512 from NIMH. The San Diego HNRC group is affiliated with the University of California, San Diego, the Naval Hospital, San Diego, and the Veterans Affairs San Diego Healthcare System, and includes: Director: Robert K. Heaton, Ph.D., Co-Director: Igor Grant, M.D.; Associate Directors: J. Hampton Atkinson, M.D., Ronald J. Ellis, M.D., Ph.D., and Scott Letendre, M.D.; Center Manager: Jennifer Iudicello, Ph.D.; Donald Franklin, Jr.; Melanie Sherman; NeuroAssessment Core: Ronald J. Ellis, M.D., Ph.D. (P.I.), Scott Letendre, M.D., Thomas D. Marcotte, Ph.D., Christine Fennema-Notestine, Ph.D., Debra Rosario, M.P.H., Matthew Dawson; NeuroBiology Core: Cristian Achim, M.D., Ph.D. (P.I.), Ana Sanchez, Ph.D., Adam Fields, Ph.D.; NeuroGerm Core: Sara Gianella Weibel, M.D. (P.I.), David M. Smith, M.D., Rob Knight, Ph.D., Scott Peterson, Ph.D.; Developmental Core: Scott Letendre, M.D. (P.I.), J. Allen McCutchan; Participant Accrual and Retention Unit: J. Hampton Atkinson, M.D. (P.I.) Susan Little, M.D., Jennifer Marquie-Beck, M.P.H.; Data Management and Information Systems Unit: Lucila Ohno-Machado, Ph.D. (P.I.), Clint Cushman; Statistics Unit: Ian Abramson, Ph.D. (P.I.), Florin Vaida, Ph.D. (Co-PI), Anya Umlauf, M.S., Bin Tang, M.S.
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, nor the US Government.
Funding statement
None
Conflicts of interest
The authors have nothing to disclose.





