



Breast-feeding is one of the fifteen viable, effective and low-cost preventive interventions that can reduce infant mortality(Reference Jones, Steketee and Black1). Evidence has shown that breast-feeding provides substantial benefits beyond infant survival and women’s health in high-, medium- and low-income countries(Reference Victora, Bahal and Barros2–Reference Schliever, Kilgore and Seo4). Considering all these benefits, the WHO recommends exclusive breast-feeding (EBF), without offering water, teas and other liquids, until 6 months of age(5). Over the past two decades, the prevalence of EBF slowly increased worldwide, from 24·9 % in 1993 to 35·7 % in 2013 and to 41 % in 2018(Reference Victora, Bahal and Barros2).
In Brazil, the EBF prevalence is similar to the global context. Despite an increase over time from 3·1 % in 1986 to 41·3 % in 2008(Reference Venâncio, Saldiva and Monteiro6), recent data indicated stabilisation of EBF prevalence between 2006 (37·1 %) and 2013 (36·6 %)(Reference Boccolini, Boccolini and Monteiro7). Furthermore, there are heterogeneities in the EBF prevalence among regions of the country and within the 5570 Brazilian municipalities. An example is the difference found in the duration (in d) of EBF prevalence among regions of the country comparing data from the first and second Breastfeeding Prevalence Survey (conducted in 1999 and 2008, respectively). For instance, while a significant increase was observed in the Centre-west region (19·5–66·5 d), not so favourable performance was observed in the Northeast region (26·3–34·9 d).
Evidence has shown that multiple factors may interfere in EBF discontinuation, such as unplanned pregnancy(Reference Finnie, Peréz-Escamilla and Buccini8), pacifier use and bottle-feeding(Reference Buccini, Perez-Escamilla and Venancio9,Reference Parizoto, Parada and Venâncio10) , pre-lacteal feeding(Reference Finnie, Peréz-Escamilla and Buccini8), early use of infant formulas and other types of milk(Reference Mendes, Lobo and Sousa11), maternal primiparity(Reference Parizoto, Parada and Venâncio10), C-section(Reference Finnie, Peréz-Escamilla and Buccini8,Reference Boccolini, Pérez-Escamilla and Giugliani12) , low birth weight(Reference Ortelan, Neri and Benicio13), not being born in a Baby-Friendly Hospital(Reference Parizoto, Parada and Venâncio10), or lack of qualified support during childbirth(Reference Monteiro, Buccini and Venâncio14), maternal obesity(Reference Monteiro, Buccini and Venâncio14), and the absence of maternity leave(Reference Boccollini, Carvalho and Oliveira15). In Brazil, a recent systematic review identified thirty-six factors associated with EBF discontinuation. These factors were organised within the hierarchical model, where distal factors included mother’s place of residence, age and education, and proximal factors included mother’s employment, child’s age and pacifier use(Reference Boccollini, Carvalho and Oliveira15).
This evidence supports the importance of gathering local data in order to better inform policies that support, promote and protect breast-feeding tailored with needs of each municipality/locality(Reference Venâncio, Escuder and Saldiva16). However, the Brazilian monitoring system of breast-feeding and infant feeding practices (SISVAN ‘Sistema de Vigilância Alimentar e Nutricional’) has not been fully adopted by all municipalities and lacks quality information. Thus, municipalities should conduct surveillance to monitor progress and then analyse these data. Robust analysis such as pooled data analysis from multiple surveys can facilitate more precise estimation and lead to better decision-making processes(Reference Bravata and Olkin17). Nevertheless, the use of pooled analysis using EBF data has not been well explored. By using a pooled data analysis from three methodologically similar data sets of cross-sectional surveys on breast-feeding practices, this paper describes an innovative way to identify determinants of EBF discontinuation in the municipality of Marília, São Paulo, Brazil, between 2008 and 2013.
Methods
Study settings
The data presented in this manuscript refer to the municipality of Marília, a medium-sized municipality (216 745 inhabitants) located in the state of São Paulo, in the southeastern region of Brazil, with a maternal–child health network composed of fifty primary healthcare units, three maternity hospitals and one Human Milk Bank. Marília is one of the few municipalities in Brazil that surveyed breast-feeding and child feeding practices in three waves 2008, 2011 and 2013, in an effort by its political administration to effectively monitor breast-feeding practices. The first author is the municipal health manager, who facilitated the logistics of the research and translation of the findings into evidence-informed decisions.
Semi-structured interviews on child feeding practices (Supplementary Material) were conducted with children’s caregivers (among which 73 % were mothers) in the first stage of the National Immunization Campaign. The interviews were conducted by trained undergraduate and graduate students, and health providers. Interviewers were trained and supervised by the Director of the Human Milk Bank and by professors from partner universities. The child feeding questionnaires were stored in the administration of the Human Milk Bank. Data were collected in the years 2008, 2011 and 2013, totalling a sample of 1645 children under 6 months old.
Outcome variable
In this study, the WHO recommendation for EBF was followed to define the outcome, that is, children under 180 d old who received only breast milk in the last 24 h with no other food or liquids(5).
EBF was determined from the question, ‘Did the child receive breast milk between yesterday morning until this morning?’ This information was confirmed with questions about intake in the previous 24 h of tea, juice, water or other type of milk/infant formula and questions about intake of other foods like fruit or savoury food. For all questions, the options for answers were ‘yes’ or ‘no’ (Supplementary Material).
For data analysis purpose, the dependent variable of the study was the discontinuation of EBF (not being EBF at the time of the data collection). The use of current status, recommended by the WHO, aims to minimise possible biases resulting from the informant’s memory, which is particularly suitable for the characterisation of EBF(18).
Covariates
A conceptual hierarchical model was used to guide the selection of covariates (Fig. 1). Conceptual hierarchical frameworks are particularly appropriate to study determinants of childhood health outcomes such as breast-feeding(Reference Victora, Huttly and Fuchs19), as in the case of our analysis. Specifically, in Brazil, a recent literature review indicates the hierarchical model as the approach to organise a range of factors at varying levels of proximity to determine EBF determinants(Reference Boccollini, Carvalho and Oliveira15). This method of organising and determining relevant risk factors is appropriate for grouping inter-related factors in a hierarchical way to elucidate relationships between variables and inform analytical decisions. Thus, considering the set of data collected in the years 2008, 2011 and 2013, a conceptual model of determinants for discontinuation of EBF adapted from the literature(Reference Finnie, Peréz-Escamilla and Buccini8,Reference Buccini, Perez-Escamilla and Venancio9) was used to guide the selection of ten explanatory variables (Fig. 1).

Fig. 1 Conceptual model: description of hierarchical interrelationship between explanatory and outcome variables
The variables selected were: maternal education (0–8 years, >8 years), maternal age (<20 years old, ≥20 years old), maternal employment situation (does not work outside the home/on maternity leave, works outside the home), primiparity (yes, no), birth in a Baby-friendly hospital in the municipality of Marília (yes, no), C-Section (yes, no), child’s sex (male/female), low birth weight (yes, no), pacifier use (yes, no) and well-child visits (public, not-public). The child’s age (0–2 months old, 2–4 months old and 4–6 months old) was included as a control variable in all stages of data analysis.
Statistical analyses
To analyse the determinants of EBF discontinuation between 2008 and 2013, the statistical analysis was conducted by survey wave and for the pooled sample. For the pooled analyses, data were weighted to adjust for the differences in the sample size across survey waves. As proposed by Buccini et al. (Reference Buccini, Perez-Escamilla and Venancio9), for all analyses of the pooled sample, data were weighted to adjust for the differences in sample size across survey waves. The sample size weight was created from equation 1/(2 × [n C /n T ]), where n C is the sample size for each survey and n T is the sample size for the pooled data.
The analyses were conducted in three stages. First, each explanatory variable was described by comparing its distribution in each survey wave (i.e. 2008, 2011 and 2013) using the χ 2 analyses. The P value < 0·05 was the criterion of significant changes in the distribution of the variable across the three surveys. Second, bivariate analysis was conducted within each survey and the pooled sample to compare the prevalence of EBF discontinuation across explanatory variables using χ 2 analysis. Third, multivariable Poisson regressions with robust variance adjusted by the child’s age were conducted on each survey wave and on the pooled sample to investigate the independent association between the EBF discontinuation and the explanatory variables. To estimate the adjusted prevalence ratio of each explanatory variable associated with the outcome, a multivariable model guided by the hierarchical model was used (Fig. 1). The distal level (1) included mother’s education (proxy of socio-economic status), which was the first to be included in the analytical model and remained as a control for the hierarchically inferior blocks. The intermediate level (2), which corresponds to the variables related to mother’s characteristics, was included in the model after the adjustment by the distal block and remained as a control for the subsequent block. Analogous procedure was adopted to the proximal level (3), which corresponds to the variables related to the characteristics of the child and their birth. Proximal level (4) corresponds to the variables related to child’s health care follow-up. All the analyses were conducted in Stata version 14.1.
Results
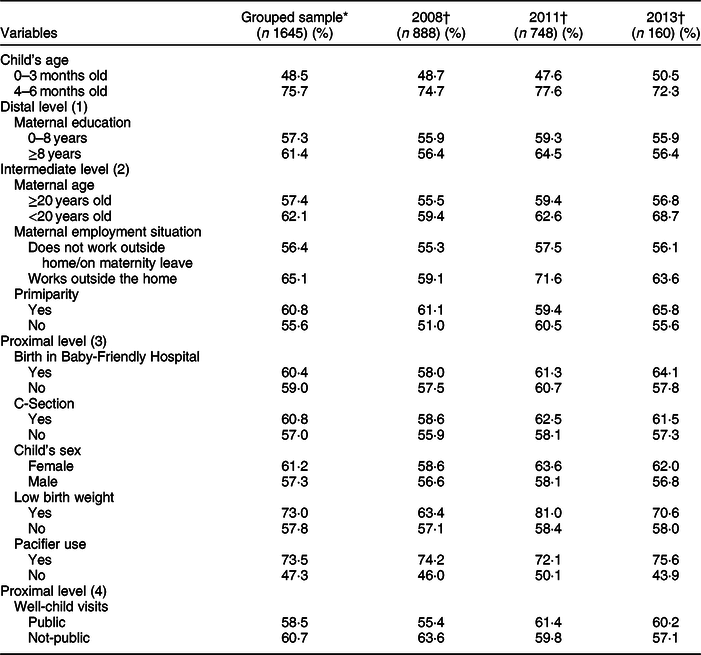
A total of 1645 mothers with children under 6 months old participated in the three survey waves. The average prevalence of EBF between 2008 and 2013 was of 40·7 % (Table 1). The prevalence of EBF across survey waves slightly decreased, from 42·3 in 2008 to 39·2 % in 2011, and to 40·6 % in 2013. The prevalence of C-section and pacifier use significantly increased between 2008 and 2013 (Table 1).
Table 1 Descriptive characteristics of children under six months old and their mothers by research wave, AMAMUNIC, 2008–2013

* Adjusted by grouped sample weight.
† Adjusted by individual survey sample.
In the pooled sample, the prevalence of EBF discontinuation was higher in mothers with more education, younger, primipara and those working outside the home (Table 2). The characteristics of childbirth, birth in a Baby-Friendly Hospital, not using pacifiers and not being born with low weight favoured continuation of EBF (Table 2). Except for maternal education, the same determinants increased the prevalence of EBF discontinuation in 2008, 2011 and 2013. Whereas in 2011, high maternal education increased the EBF discontinuation compared with less educated women, in 2008 and 2013, no difference between mothers’ educational levels was observed.
Table 2 Prevalence of exclusive breast-feeding discontinuation by mother–child characteristics, AMAMUNIC, 2008–2013
* Adjusted by grouped sample weight.
† Adjusted by individual survey sample.
The determinants of EBF discontinuation between 2008 and 2013 were maternal employment status (mothers working outside of the home) (adjusted prevalence ratio (APR) = 1·10, 95 % CI 1·00, 1·21); first-time mothers (APR = 1·10, 95 % CI 1·01, 1·20); low birth weight (APR = 1·17, 95 % CI 1·05, 1·32) and pacifier use (APR = 1·48, 95 % CI 1·36, 1·61) (Table 3). For maternal employment status, first-time mothers and low birth weight, the individual prevalence ratios were not significant within all the survey waves but in the same direction (attesting higher power of pooled analysis). Thus, whereas in 2008 and 2013, working outside the home and low birth weight were not significantly associated with EBF discontinuation, in 2011 working outside the home and low birth weight were associated with 18 and 33 % higher prevalence for EBF discontinuation, respectively. Similarly, in 2011 and 2013, first-time mothers were not associated with EBF discontinuation, whereas in 2008, first-time mother was associated with an 18 % higher prevalence for EBF discontinuation. For pacifier use, similar results were observed within each survey wave where multivariable analyses indicated that pacifier use was strongly associated with the risk of EBF discontinuation in 2008, 2011 and 2013 (APR = 1·55 v. 1·36 v. 1·71, respectively).
Table 3 Multivariable Poisson regressions used to estimate the adjusted prevalence ratios of exclusive breast-feeding discontinuation according to mother–child characteristics controlled for child’s age, AMAMUNIC, 2008–2013
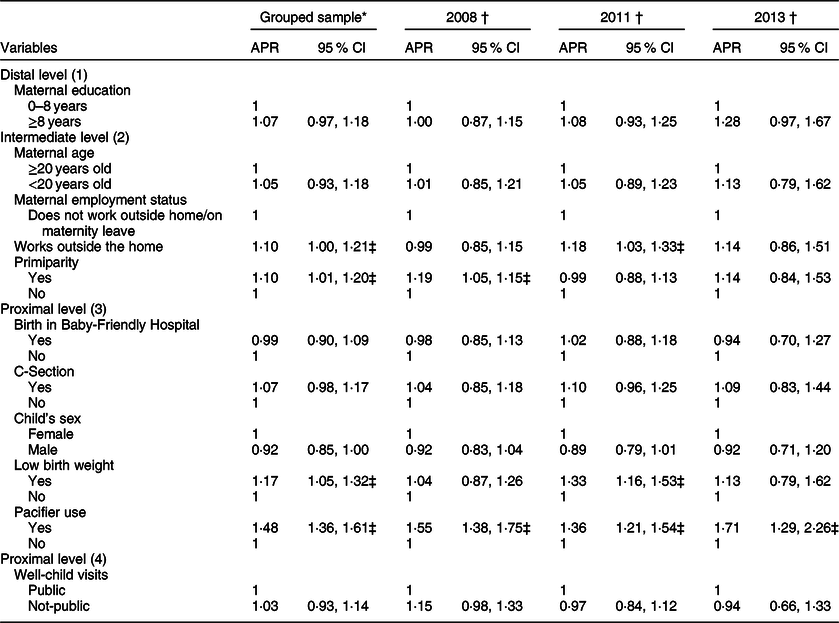
APR, adjusted prevalence ratio.
* Adjusted by grouped sample weight.
† Adjusted by individual survey sample.
‡ Variables P < 0·05.
Discussion
EBF prevalence in Marília is slightly higher (40·7 %) than the national average (36·6 %)(Reference Boccolini, Boccolini and Monteiro7), and for the state of São Paulo in southeastern Brazil (39·1 %)(Reference Venâncio, Escuder and Saldiva16). EBF prevalence in Marília is slightly lower than Colombia (43 % in 2005)(Reference Ferreira, Parada and Carvalhaes20) and higher than Mexico (16 % in 2016)(Reference González de Cosío, Ferre and Mazariegos21). Results from EBF prevalence in Marília are low compared with findings from 127 countries that found an EBF prevalence of 53 % in low-income countries, 61 % in medium-income countries and 63 % in high-income countries(Reference Victora, Bahal and Barros2). The heterogeneity of EBF prevalence, within the Brazilian context and globally, highlights the relevance of monitoring breast-feeding practices at the local level and the key role of having a robust analysis such as pooled analysis focused on the understanding of EBF determinants over time, as we did in our study.
The EBF prevalence in Marília remained relatively stable between 2008 and 2013, unlike what was observed in other municipalities in southeastern Brazil(Reference Parizoto, Parada and Venâncio10,Reference Ferreira, Parada and Carvalhaes20) . For instance, in Bauru, a medium-sized municipality with similar characteristics as Marília also located in southeastern Brazil has increased EBF prevalence from 8·5 % (1999) to 24·2 % (2006), a growth of 184·7 %, which was due to investment in actions that promote breast-feeding, in training health professionals (community-based/Primary Health Care and hospital-based) as well as in reducing pacifier use(Reference Ferreira, Parada and Carvalhaes20). Likewise, in Botucatu, the prevalence of EBF moved from 13·0 % (1995) to 29·6 % (2004), as a result of the improvement of the care practices provided to mothers and newborn children in maternity hospitals, the creation of a Human Milk Bank, the creation of Family Health Units in the Primary Health System and the increase in the number of health professionals to provide breast-feeding support in the municipality(Reference Ferreira, Parada and Carvalhaes20). These data reinforce the importance of a municipal strategic plan based on evidence and tailored to the municipality needs.
Among the determinants of EBF discontinuation identified in our study, mothers currently working outside the home were a major risk factor. Mothers who were working outside of the home at the time of the survey included those who did not have maternity leave due to informal employment or those who returned to work before the baby reached 6 months. Evidence shows that mothers who work outside home, without maternity leave, had three times the chance of interrupting EBF(Reference Queluz, Pereira and Santos22). The analysis of the Brazilian national data confirmed that not having maternity leave increased the chances of EBF discontinuation in 23 % of women(Reference Monteiro, Buccini and Venâncio14). Likewise, analysis of data from thirty-eight countries found that the extension of paid maternity leave promotes breast-feeding(Reference Chai, Nandi and Heymann23). Maternity leave for formal and informal workers can be a potential mechanism for reducing barriers in EBF. Among mother’s characteristics, maternal primiparity has also been associated with EBF discontinuation in prior studies(Reference Monteiro, Buccini and Venâncio14,Reference Martins, Vieira and Vieira24,Reference Almeida, Ribeiro and Rodrigues25) including ours. First-time mothers have 41 % more risk of interrupting EBF than multiparous mothers(Reference Martins, Vieira and Vieira24). This result confirms the importance of training health providers to develop actions to manage and support breast-feeding tailored to the needs of first-time mothers(Reference Almeida, Ribeiro and Rodrigues25).
In our study, infants with low birth weight were more susceptible to EBF discontinuation. Studies showed that the weight at birth greatly influences breast-feeding outcomes, especially EBF(Reference Sanches, Buccini and Gimeno26). Low birth weight children may have difficulty sucking mother’s breast(Reference Medoff-Cooper, Verklan and Carlson27). In addition, they may stay hospitalised for longer time, and the separation from their mothers may negatively impact breast-feeding outcomes. Recent study showed that infants with low weight are likely to be breastfed when being born in a Baby-Friendly Hospital(Reference Serra and Scochi28). Although the birth in a Baby-Friendly Hospital was not associated with EBF discontinuation in this study, prior evidence found that local investments in the adherence of the Baby-Friendly Initiative can improve breast-feeding rates among the most vulnerable children(Reference Serra and Scochi28,Reference Silva, Rea and Venâncio29) . For instance, in Marília, only one of the three maternity hospitals of the municipality is certified as Baby-Friendly; thus, there is a window of opportunity with strong evidence of high impact on the increase of EBF rates(Reference Serra and Scochi28,Reference Silva, Rea and Venâncio29) .
Pacifier use was significantly associated with the discontinuation of EBF, corroborating previous studies(Reference Buccini, Perez-Escamilla and Venancio9,Reference Vogel, Hutchison and Mitchell30,Reference Buccini, Perez-Escamilla and Paulino31) . Data from the first and the second Breast-feeding Prevalence Survey in the Brazilian capitals and the Federal District, conducted in 1999 and 2008, also found that the use of pacifier was the strongest risk factor to the EBF discontinuation(Reference Buccini, Perez-Escamilla and Venancio9). Buccini et al. (Reference Buccini and Venancio32) outlined three hypothesis (which do not exclude each other) to explain the influence of pacifier use on the EBF discontinuation: (1) The introduction of pacifiers may cause EBF discontinuation; pacifier use may discourage breast-feeding, by interfering in the oral dynamics of the baby and the demand for mother’s breast, which reduces the frequency of breast-feeding. (2) The introduction of pacifiers occurs due to problems in breast-feeding; thus, pacifier use would be a consequence and not a cause of a lower duration of EBF; it is based on this premise that pacifier can be considered an indicator of breast-feeding difficulty. (3) The introduction of pacifiers occurs due to baby’s behaviour, mother–baby interaction and mother’s profile (and their families’); thus, breast-feeding and pacifier use are influenced by the behaviour of the baby during breast-feeding and by the way the interaction mother–baby–family is established (e.g. a combination of a fussy baby and an anxious mom may increase the chances of introducing a pacifier). Pacifier are often used by mothers to relieve the infant’s crying; thus, health providers must be educated about the topic to be able to counsel parents on the pros and cons of pacifier use. Actions with parents should address strategies to handle the infant’s crying behaviour instead of introducing pacifiers(Reference Buccini and Venancio32), as well as information about the potential negative interference of pacifier use on breast-feeding. For the groups with more risk to use pacifier (e.g. first-time mothers and mothers working outside the home), it is recommended to offer practical help in dealing with the difficulties in breast-feeding, listening to the mothers concerning the need for a pacifier, and offering support for the cases where the habit of using pacifier has already begun(Reference Buccini33).
This research has some strengths and limitations. First, due to its cross-sectional nature, we cannot establish the temporal sequence of events between the determinants and EBF outcomes; thus, reverse causality cannot be ruled out. On the other hand, this is the first study analysing the prevalence of EBF discontinuation and its determinants in the municipality of Marília using pooled analysis. Our findings may be generalised to urbanised areas in Brazil, which correspond to more than 85 % of the Brazilian population(34). Second, despite the high coverage of immunisation campaign for children under 5 years old in the municipality of Marília in the three survey waves (in 2008 was 88·67 %; in 2011 was 98·25 % and in 2013 was 93·87 %), in 2013, there were changes in the national guidelines of immunisation making the convocation of children under 6 months old non-mandatory. Yet, during the campaign, some caregivers of children under 6 months old went to the Primary Health Care Units to update their immunisation booklets and participated in the research. Due to this change in the national immunisation strategy, the number of children under 6 months old who participated in the campaign was smaller than 2008 and 2011, and as a consequence, the sample size for that year was also smaller. To avoid bias related to sample size for the pooled analysis, data were weighted to adjust the differences in the sample size across survey waves. In spite of these limitations, these findings are innovative as they raise hypotheses that can be tested by future studies, for example, the evaluation of the degree of adherence to breast-feeding promotion strategies such as Baby-Friendly Hospital Initiative, Human Milk Banks and the Brazilian Strategy to promote breast-feeding and complementary feeding in the primary care settings. The fact that our findings are based on three survey waves that are representative of urban samples in a large country like Brazil and that both the individual and pooled regression analyses point to the same conclusions makes our study a unique contribution to the literature.
Finally, the determinants of EBF discontinuation in Marília can inform the formulation of tailored public policies. These findings can indicate the outlining of local actions and in others that have a similar epidemiological profile focused on groups who are most vulnerable to early weaning and strengthen the implementation of public policies in the mother–child healthcare network.
Acknowledgements
Acknowledgements: The authors acknowledge the Marília Human Milk Bank and the Municipal Health Secretary of Marília for their support in the data collection. Financial support: None. Conflict of interest: None. Authorship: E.N.N. and G.B. formulated the research question, analysed the data and interpreted the findings; E.N.N. conducted the data collection and wrote the first draft of the article; C.L., L.C.A. and G.B. revised and contributed substantially throughout the writing process. The final version of the article was approved for all co-authors. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the Ethics Committee of the Public Health School of the University of São Paulo (protocol no. 1,077,981/2015).
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020003110






