


Energy drinks are consumed for many purposes, including boosting energy, improving mental alertness, enhancing athletic performance, satiating thirst and satisfying taste. Caffeine is especially common in these beverages, which may also contain various other ingredients, such as taurine, ginseng, herbs and amino acids(Reference Vercammen, Koma and Bleich1). Energy drinks are often sold in ready-to-drink formats (cans and shots) and classified as conventional foods/beverages or dietary supplements. Analysis of data collected in the 2003–2016 cycles of the National Health and Nutrition Examination Survey (NHANES), which is designed to be representative of the non-incarcerated population in the USA, found that 1·4 % of teenagers (ages 12–19 years), 5·5 % of young adults (ages 20–39 years) and 1·2 % of middle-aged adults (ages 40–59 years) consume energy drinks(Reference Vercammen, Koma and Bleich1). Sales of these drinks, including shots, in the USA are estimated to exceed $12 billion per year(2).
Despite intake across age groups and anticipated sales growth in the USA, studies have shown that energy drink consumption may be of public health concern, particularly among vulnerable groups such as children and young adults(Reference Markon, Jones and Punzalan3,Reference Wikoff, Welsh and Henderson4) . Previous analysis of adverse events reported to the US Food and Drug Administration (FDA) Center for Food Safety and Applied Nutrition’s Adverse Event Reporting System (CAERS) and exposure calls to the American Association of Poison Control Centers (AAPCC) National Poison Data System (NPDS) found consumption of energy drink products were correlated to adverse events including tachycardia, nausea, vomiting, as well as nervous system and gastrointestinal system alterations, among other negative physical outcomes(Reference Markon, Jones and Punzalan3). Other studies have also reported negative outcomes associated with energy drink consumption, including similar adverse events listed above as well as increased cardiac arrythmia, lower levels of sleep, increased stress, anxiety, anger, hepatic alterations, and other detrimental mental and physical effects(Reference De Sanctis, Soliman and Soliman5–Reference Levy, Santini and Capucci11). Additionally, some users mix energy drinks with alcohol, which can lead to further risky behaviours leading to adverse outcomes(Reference Doggett, Qian and Cole12–Reference Mallett, Scaglione and Reavy15). Energy drink has been found to be associated with other risky behaviours including drug use, poor dietary habits, sensation seeking and worse school performance(Reference Galimov, Hanewinkel and Hansen16). Finally, studies have tended to focus on either younger consumers(Reference Galimov, Hanewinkel and Hansen16–Reference Barrense-Dias, Berchtold and Akre18) or members of the military(Reference Pakkila, Anttonen and Patinen19–Reference Toblin, Adrian and Hoge21). Given these concerns, and relatively little data among non-military adults, we comprehensively assessed demographic and behavioural factors related to energy drink consumption, particularly high-risk behaviours such as alcohol and drug use, among participants in two large cohorts in the USA.
Methods
Study population
We conducted cross-sectional analysis using data from the Nurses’ Health Study 3 (NHS3) and Growing Up Today Study (GUTS)(Reference Bao, Bertoia and Lenart22). The NHS3 is an open, web-based prospective cohort study of female nurses and nursing students in North America. Enrolment started in 2010 and is ongoing. Participants complete a baseline questionnaire and follow-up questionnaires approximately every 6 months. As of 17 July 2020, 49 515 female participants have joined the study. GUTS is an ongoing prospective cohort study of young adults. The cohort was established in 1996 with the recruitment of 16 875 children, age 9–15 years (GUTS1) and expanded in 2004 with the enrolment of an additional 10 918 children aged 9–15 years (GUTS2). Participants complete follow-up questionnaires every 1–3 years. Because of age differences between the two enrolment cycles, these two groups were followed separately until 2013, when all participants were adults, and a common follow-up schedule and follow-up materials were used. For this study, we included NHS3 participants (age 20–55 years) who completed a diet assessment in the first follow-up questionnaire and GUTS participants (age 16–31 years) who completed a diet assessment in 2011, when intake of energy drinks was first assessed in this cohort. Eighty per cent of participants completed the follow-up questionnaire between 2010 and 2013. After excluding female participants who skipped the question on intake of energy drink and were pregnant at the time of diet assessment (excluded 9004) and males who did not skip the question about energy drinks (excluded 9601), the study included 37 198 participants from NHS3 and 8993 participants from GUTS. We combined the data from both cohorts for our analysis, in part, due to low overall levels of energy drink consumption, as described further in the discussion section. Participant selection flowcharts for GUTS and NHS3 are shown in Fig. 1 and 2, respectively.
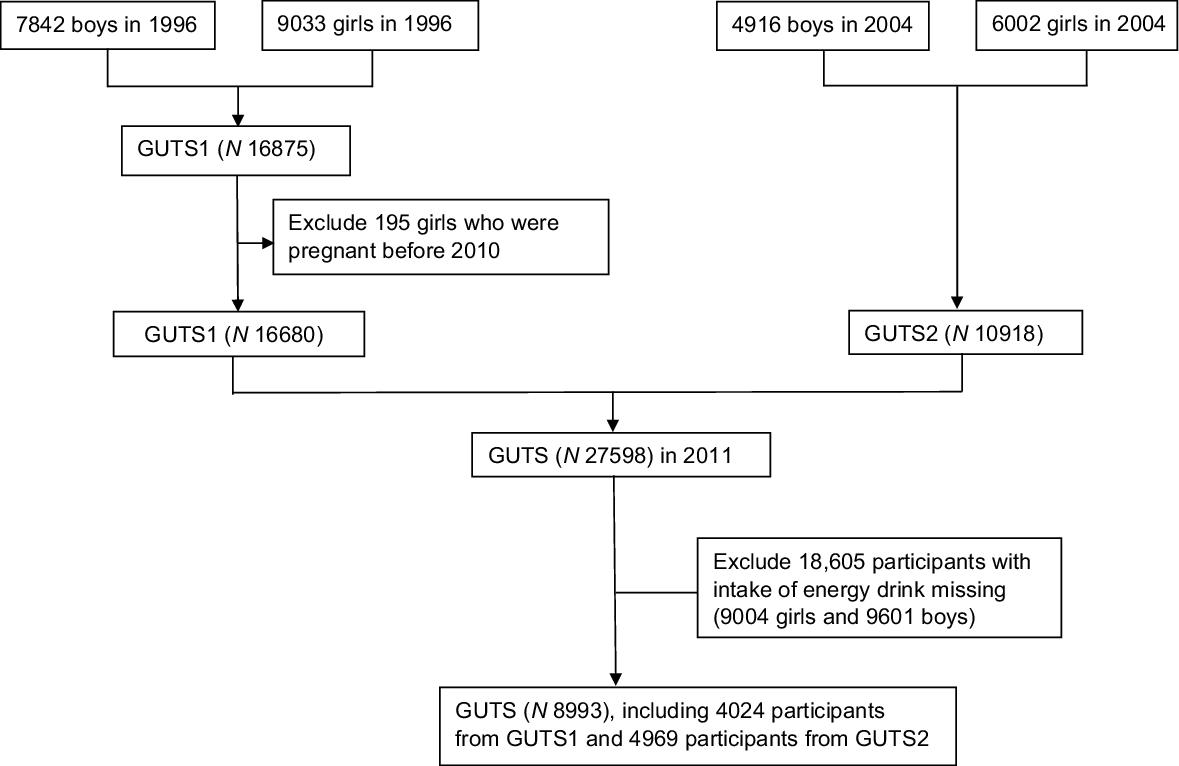
Fig. 1 A flow diagram of sample selection in the Growing Up Today Study (GUTS)

Fig. 2 Flow diagram of sample selection in the Nurses’ Health Study 3 (NHS3)
Assessment of energy drink use
Diet was assessed using an extensively validated FFQ(Reference Yuan, Spiegelman and Rimm23,Reference Yuan, Spiegelman and Rimm24) . Participants reported how often, on average, they consumed 131 foods and beverages listed in the questionnaire during the past year. Participants were asked to report their intake of ‘Energy drinks (e.g. Red Bull, Rock Star and Monster), 1 can’ in one of nine categories of increasing frequency of intake ranging from never or less than once per month to six or more times per d. For the purpose of this study, energy drink users were defined as those who reported consuming energy drinks at least once per month. The selected frequency category for each food item was then converted to daily intake. Food intake under each category was then combined to obtain the total intake of fruits, vegetables, fish and shellfish, red meat, sugar-sweetened beverages, etc. The FFQ used here has been previously shown to be of high validity(Reference Yuan, Spiegelman and Rimm23,Reference Yuan, Spiegelman and Rimm24) Finally, use of energy drinks was assessed in the second questionnaire in NHS3 and in 2011 in GUTS.
Assessment of demographic and behavioural data
Sociodemographic and behavioural data were obtained from responses to follow-up questionnaires completed closest to the time of energy drink consumption assessment when available, and otherwise from each participant’s demographic information collected at baseline (online Supplementary Table 1). Participants reported their race and ethnicity using categories defined by the US Census Bureau (Non-Hispanic White, Non-Hispanic Black, Hispanic, Asian and Other). Other demographic characteristics reported by participants included highest level of education achieved (< Bachelor’s, Bachelor’s, ≥ Master’s degree), geographical region of residence (Northeast, Midwest, West and South), marital status (never married, married, divorced, separated, widowed and domestic partnership) and sexual orientation (completely heterosexual, mostly heterosexual, bisexual, mostly homosexual, completely homosexual and not sure).
We decided to assess behaviours that could be harmful to human health based on findings from existing literature such as drug/alcohol use(Reference Mallett, Scaglione and Reavy15–Reference Barrense-Dias, Berchtold and Akre18,Reference Dawodu and Cleaver25–Reference Peacock, Bruno and Ferris27) , as well as other potentially risky behaviours identified by the authors that were already collected as part of the GUTS/NHS 3 questionnaires. Data on health-related behaviours and behavioural risk factors included smoking status (current or past smoker), e-cigarette use (yes/no), usual duration of overnight sleep (< 7, 7–9, > 9 h specifically, we asked about hours of sleep on work-free days without obligations in NHS3), tanning bed use (yes/no), use of birth control among female participants (Depo Provera, Other hormonal contraception, Vasectomy, Tubal Ligation, Oral Contraceptive, Foam/Jelly/Sponge, Diaphragm/Cervical Cap, Condom, Rhythm/Natural Family Planning, Intrauterine Device and yes/no), preventive physical exam/doctor’s visit in the past 2 years (yes/no), lifetime number of sexual contacts/partners, marijuana use (yes/no), use of illegal drugs besides marijuana (cocaine, heroin, ecstasy, lysergic acid diethylamide (LSD/acid)), mushrooms (shrooms) or any other hallucinogen, crystal meth (methamphetamine, crank, tweak), other amphetamines (uppers, speed)), binge drinking (yes/no), use of multivitamin supplements (yes/no), and use of muscle enhancing products (yes/no, protein powder or shake, creatine, weight loss shakes/drinks, amino acids, hydroxymethylbutyrate /HMB, dehydroepiandrosterone/DHEA, growth hormone, anabolic/injectable steroids). The most recent self-reports of height and weight, which have been previously found to be validly reported in GUTS and other cohorts of nurses(Reference Rimm, Stampfer and Colditz28), were used to calculate the BMI as weight (kg) divided by height squared (m2) and then grouped into WHO reference categories (< 25 kg/m2, 25–30 kg/m2, ≥ 30 kg/m2).
Participants’ physical activity was assessed by means of self-report questionnaires in 2015 in GUTS and the second questionnaire in NHS3. Participants were asked about the amount of time that they spent per week, on average, in each of the following physical activities: walking; jogging; running; bicycling; playing tennis; other aerobic exercise (aerobic, dance, ski or stair machine, etc.), lower intensity exercise (yoga, stretching and toning) and other vigorous activities (e.g. lawn mowing). The amount of total reported physical activity was calculated as energy expenditure in hours per week.
A single diet score (based on criteria of the American Heart Association (AHA)) was defined using a priori cut-offs(Reference Arvizu, Stuart and Rich-Edwards29), looking at consumption quantities for various foods, including: fruits/vegetables, fish and shellfish, Na, sugar-sweetened beverages (SSB), and whole grains, as well as nuts/legumes/seeds, processed meat, and saturated fat. For healthy foods, such as fruits and vegetables or fish, participants received a score ranging from 0 to 10 points based on consumption level – where a score of 0 indicated they did not consume the food at all and 10 indicated that they consumed the optimal level of said food according to the AHA. For unhealthy foods (e.g. processed meats, SSB), a score of 0 indicated intake higher than that of the 80–90th percentile among US adults, while a score of 10 meant that the food was consumed at or below the target intake level(Reference Arvizu, Stuart and Rich-Edwards29).
Statistical analysis
We conducted both basic descriptive and quantitative analyses to characterise demographic and behavioural factors in relation to energy drink consumption. Descriptive analysis addressed the distributions of demographic and behavioural factors by reported energy drink use among each cohort. Univariate/multivariable logistic models were used for bivariate analyses. We examined associations between demographic and behavioural factors and the odds of energy drink consumption using logistic regression. We applied both univariable and multivariable logistic regression models. As to multivariable analysis, we simultaneously included all demographic and behavioural factors into the regression model and used missing indicators for variables with missing values. As for pooled analysis, we combined individual data in NHS3 and GUTS into one dataset and conducted regression analyses in the pooled dataset. We tested for heterogeneity in associations between cohorts by including interaction terms of each covariate and cohort into the model, and Pfor interaction was obtained using likelihood ratio test comparing models with and without interaction terms. Given the multiple demographic and behavioural factors considered, we corrected for multiple testing using Bonferroni correction and considered results significant or significant heterogeneity in associations across cohorts with P value<0·05/37 (=0·001), where 37 was the number of tests performed.
Missing data for all variables were presented in Supplementary table 2. Given that we included all variables simultaneously into the model for multivariable regression, we used missing indicators for variables with missing values to avoid issues of model convergence. In sensitivity analysis, for variables that have skewed distributions, we imputed missing values as the value that has the highest percentage, i.e. ‘no’ for smoking status, use of tanning bed, binge drinking, marijuana use, and multivitamin use, married/partner for marriage status, and completely heterosexual for sexual orientation. We fitted multivariable logistic regression including those imputed variables to obtain OR of these variables with energy drink intake and then added the rest of the variables into the multivariable model one by one to obtain OR of that variable. All statistical tests were two-sided and performed using SAS version 9.2 for UNIX (SAS Institute Inc).
Results
Our study included 46 390 individuals, with 9088 (19·5 %) participants from the GUTS and 37 302 (80·5 %) were from the NHS3. The overall levels of energy drink consumption are shown in Table 1. 40 269 participants (86·8 %) reported that they consumed fewer than one energy drink product per month, while 3540 (7·6 %) reported consuming 1–3 energy drinks per month and 2581 (5·6 %) reported consuming more than three energy drinks per month. Of those 2581 individuals, 8·4 % (0·5 % of the total study sample) reported daily consumption of energy drinks and 3·9 % (0·2 % of the total sample) reported consuming more than one energy drink per d.
Table 1 Distribution of intakes of energy drink in Nurses’ Health Study 3 (NHS3) and Growing Up Today Study (GUTS)

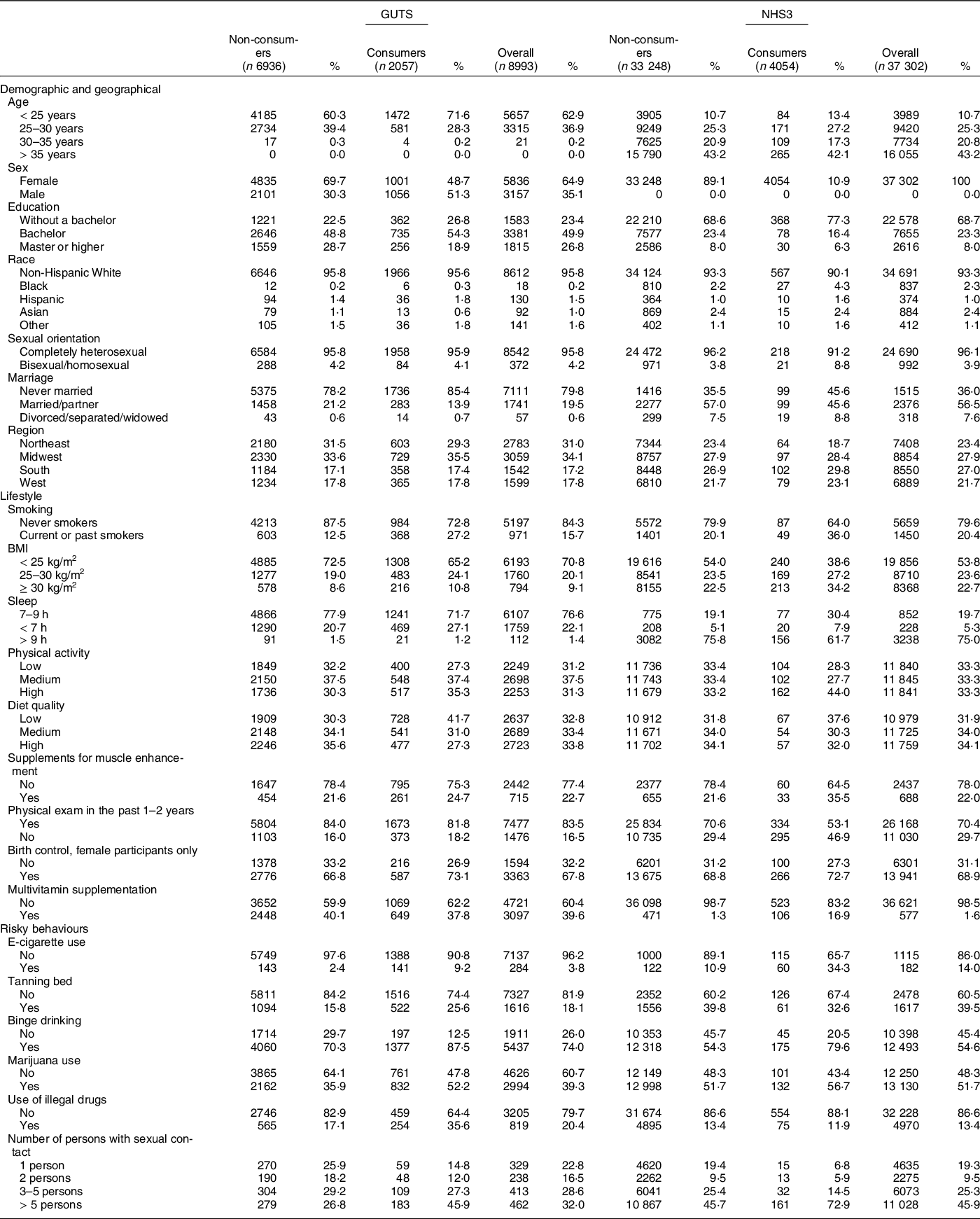
Table 2 shows available demographic and risk factor data for comparison by energy drink consumer status across the cohorts. Over 75 % of individuals reported having at least a bachelor’s degree, with 8405 (22·6 % of those reporting) indicating a master’s degree or higher education. Energy drink consumption was less likely among higher education levels compared to the lowest ones. Most participants (about 90 %) self-identified as Caucasian across the cohorts. Most participants were non-smokers, with the lowest rates of smoking seen in GUTS2; smokers were more likely to be energy drink consumers. Less than 1 % of NHS3 participants reported e-cigarette use, but data on e-cigarette use were not collected in the other cohorts. E-cigarette use was also more common among those who reported energy drink use. GUTS1 and GUTS2 participants were more likely than NHS3 members to report binge drinking, defined as four or more alcoholic drinks over a few hours. More than half (51·5 %) of GUTS1 participants reported marijuana use, exceeding use indicated by data from the two other cohorts. GUTS1 participants also were more likely to report use of illegal drugs (20·0 %) compared to NHS3 participants (13·3 %); GUTS2 did not collect data on this exposure.
Table 2 Distribution of exposure according to intake of energy drinks in Growing Up Today Study (GUTS) and Nurses’ Health Study 3 (NHS3)
We present the associations of demographic and behavioural factors with odds of being an energy drink consumer in Table 3. For GUTS-only participants, being female, and for both GUTS and NHS3 participants, higher education levels, were consistently associated with lower odds of energy drink consumption in multivariable logistic regressions (Table 3). Black study participants were more likely to consume energy drinks compared to Caucasian participants (pooled OR (pOR: 2·10. 95 % CI: 1·41, 3·14)). Marital status was not associated with energy drink consumption. Those self-identifying with bisexual/homosexual orientation were statistically significantly more likely to consume energy drinks based on results from the NHS3 univariable analyses (OR: 2·43, 95 % CI: 1·54, 3·82), but sexual orientation was not significantly associated with energy drink intake in the other cohort or pooled analyses.
Table 3 OR of consuming energy drinks characteristics related to intake of energy drinks in Growing Up Today Study (GUTS) and Nurses’ Health Study 3 (NHS3)
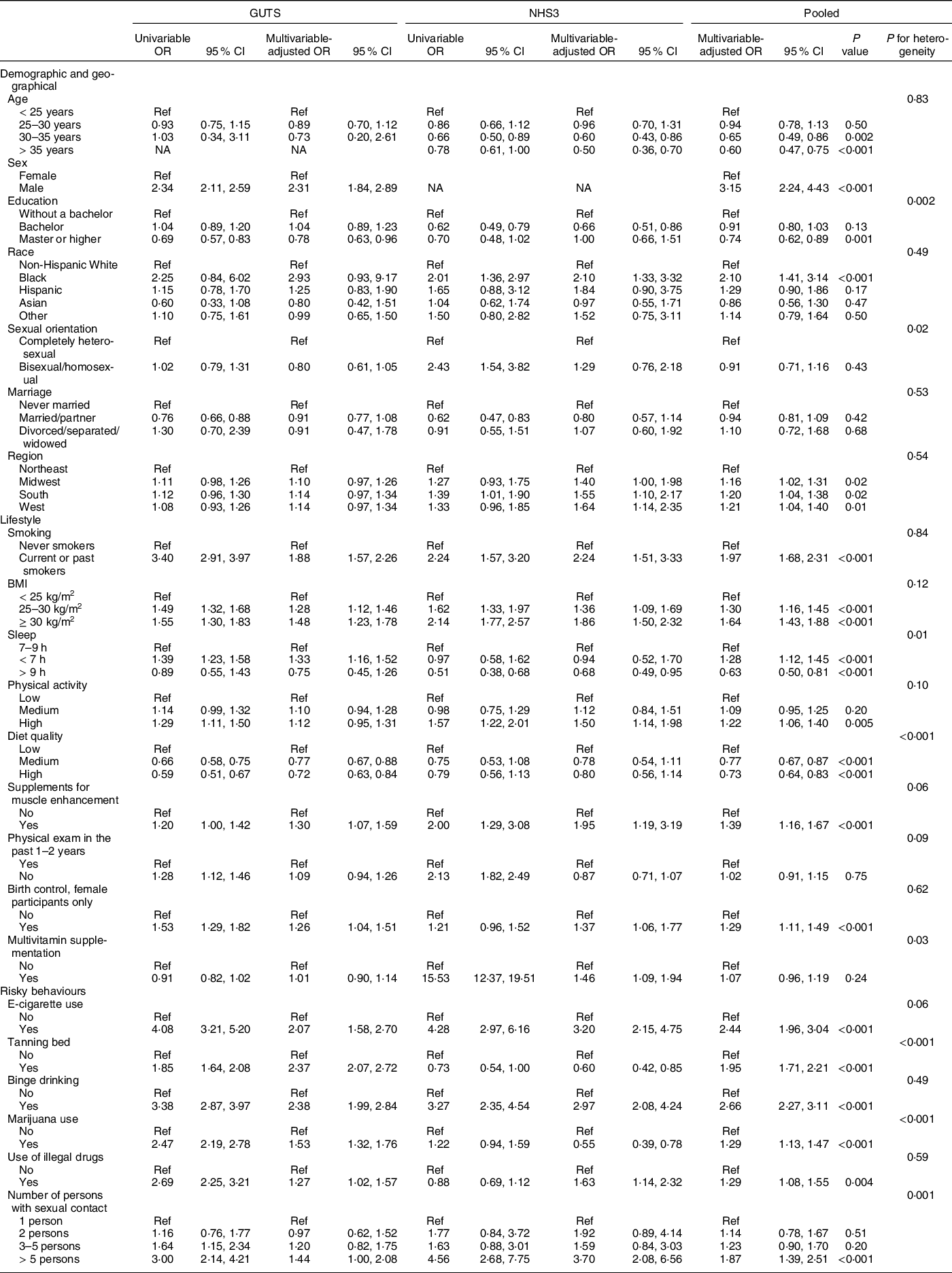
Univariate analysis used a logistic model.
Multivariate analysis used a logistic model that simultaneously included all variables in the model.
Pooled analysis combined individual data from NHS3 and GUTs into a single dataset and conducted regression analysis in the pooled dataset. We tested for heterogeneity in association between cohorts by including interaction terms of each covariate and cohort into the model, and P for interaction was obtained using likelihood ratio test comparing models with and without interaction terms.
Several behavioural factors were also associated with energy drink consumption as seen in Table 3. Smokers were more likely within and across cohorts to consume energy drinks than non-smokers (pOR: 1·97. 95 % CI: 1·68, 2·31). Higher BMI levels (25–30 kg/m2 and ≥ 30 kg/m2 compared to < 25 kg/m2) were, overall, also associated with consumption; those with lower, healthier BMI levels were less likely to consume energy drinks. The pooled model showed that those with high-quality diets were statistically significantly less likely to consume energy drinks compared to those with lower-quality diets; however, the individual cohort models revealed that high-quality diet was not associated with energy drink consumption in the NHS3. Similarly, results for the relationship between physical activity and energy drink intake varied across and within cohorts, including statistically significant associations between high physical activity and energy drink consumption. Additionally, individuals who reported that they used supplements for muscle enhancement were statistically significantly more likely to consume energy drinks based on the GUTS1 age- and sex-adjusted and multivariable models, as well as the pooled multivariable model, but the relationship between muscle enhancement supplements and energy drink intake was not statistically significant in either of the NHS3 models. E-cigarette use (as-aOR: 2·44, 95 % CI: 1·96, 3·04), tanning bed use (pOR: 1·87, 95 % CI: 1·73, 2·24), binge drinking (pOR: 2·66, 95 % CI: 2·27, 3·11), marijuana use (pOR: 1·29, 95 % CI: 1·13, 1·47) and illegal drug use (pOR: 1·29, 95 % CI: 1·08, 1·55) were all strongly significantly associated with energy drink consumption in the pooled analysis.
Finally, we examined potential associations of all variables with energy drink intake, accounting for missing values. As shown in Supplementary Table 3, the findings are nearly identical to those in the main analysis. Male participants were more likely to consume energy drinks (aOR: 2·86, 95 % CI: 2·56, 3·21), as were Black participants (pOR: 2·08, 95 % CI: 1·44, 3·01). Higher BMI were also associated with energy drink intake (for both higher BMI categories compared to < 25 kg/m2), as were e-cigarette use (pOR: 4·56, 95 % CI: 3·63, 5·74), tanning bed use (pOR: 2·37, 95 % CI: 2·11, 2·67), binge drinking (pOR: 1·23, 95 % CI: 1·11, 1·36) and illegal drug use (pOR: 1·49, 95 % CI: 1·25, 1·77).
Discussion
This study shows that energy drink intake is associated with risky behaviours and suboptimal physical status, such as obesity, e-cigarette use, smoking, binge drinking, and use of illicit drugs, and highlights the complexity of the public health problems related to consumption of these products. Our results are also consistent with previously reported associations between energy drink intake and risky behaviours, especially among teenagers and young adults, including illicit drug use, alcohol dependence and binge drinking, prescription drug misuse, and other harmful outcomes(Reference Galimov, Hanewinkel and Hansen16,Reference Arria, Caldeira and Bugbee17,Reference Dawodu and Cleaver25,Reference Meredith, Sweeney and Johnson26,Reference Al-Shaar, Vercammen and Lu30) . For example, Buja et al. (2017)(Reference Buja, Gallimberti and Chindamo31) found that caffeinated energy drink consumption was associated with negative impacts on digital well-being, revealed by problematic social network site usage among young teenagers in North-eastern Italy. An Icelandic study additionally showed that adolescent caffeine consumption was associated with self-reported physically aggressive behaviours towards others, including punching and kicking other individuals(Reference Kristjansson, Kogan and Mann32). Finally, researchers have also reported significant associations between increased energy drink consumption and suicide attempts among teenagers in South Korea and Ontario, Canada(Reference Kim, Sim and Choi7,Reference Masengo, Sampasa-Kanyinga and Chaput33) . Overall, energy drink consumption has been correlated with risky behaviours that can have short-term, long-term, and/or permanent negative effects, especially among youth.
Much of the current literature on caffeinated energy drinks focuses on teenagers and younger/college-age adults(Reference Arria, Caldeira and Bugbee17,Reference Barrense-Dias, Berchtold and Akre18) , as well as military personnel who may be of a similar age as many enlist or are conscripted as young adults(Reference Pakkila, Anttonen and Patinen19–Reference Toblin, Adrian and Hoge21). Few studies, however, appear to assess the effects of caffeinated energy drinks among adults who are older than college age, and even fewer look together at risky behaviours among them and their offspring. Lieberman et al. analysed 2007–2012 NHANES data for adults aged 19+ years, primarily looking at demographic factors, as well as some health status characteristics and risky behaviours associated with all caffeine intake (not just caffeinated energy drink consumption); they found that smoking, higher calorie intake and alcohol consumption (when adjusted for employment factors) were associated with increased caffeine usage(Reference Lieberman, Agarwal and Fulgoni34). In a study of energy drink intake among illicit drug users who participated in the online 2014 Global Drug Survey of individuals aged 16 years or older, Peacock et al. (2017)(Reference Peacock, Bruno and Ferris27) found that over two-thirds of participants reported ever consuming energy drinks and higher levels of energy drink use were associated with several risky health behaviours, including use of tobacco, marijuana, amphetamine, 3,4-methylenedioxymethamphetamine (MDMA/ ecstasy) and cocaine.
Given the general dearth of energy drink consumption and risky behaviour data among adults, and the potential for adverse health outcomes from these behaviours, we believe that our study provides a unique opportunity to assess the behaviours that may accompany energy drink consumption among slightly older adults – study participants were generally older than those considered in much of the literature, with participant mean baseline ages ranging from a college student age common in the literature of 19·61 years (GUTS non-consumers) to a much older 33·96 years (NHS3 non-consumers). Furthermore, our study found several risky behaviours associated with energy drink consumption in a large, robust sample size. Additionally, we assessed certain risky behaviours related to energy drink use that have not often been assessed in the literature, including tanning bed use, lifetime number of sexual partners and use of muscle enhancement supplements. These findings help shed light on health issues and activities of concern to both the general public and, perhaps, also serve as a warning sign for medical and other health practitioners to look for other unsafe behaviours as well.
A potential limitation with our study is that the two cohorts are fundamentally very different in terms of their sample source. However, we believe that the benefits of pooling the cohorts outweigh this limitation. First, although population characteristics are different between the two cohorts, we found similar associations for many variables, showing the robustness of our findings. Second, the heterogeneity in associations for some variables allows us to have a better understanding of the associated patterns of energy drink intake. Third, by combining the NHS3 and GUTS, our study has ample power to achieve a strong conclusion of our research question, particularly in the presence of overall low energy drink consumption. Another limitation is that some of the data used for the GUTS analysis is from 2011, meaning that behaviours and other relevant information may have changed since the data were collected.
Limitations of addressing different study periods and exposure windows notwithstanding, as previously mentioned, an analysis of CAERS and NPDS data found that consumption of caffeinated energy drinks could lead to a variety of serious and life-threatening events, including tachycardia and other cardiac disorders, nervous system irregularities, nausea/vomiting and even death(Reference Markon, Jones and Punzalan3). A recent systematic review of thirty-two studies found that insomnia was frequently associated with energy drink consumption, both among children and adults(Reference Nadeem, Shanmugaraj and Sakha35). Other studies have also reported associations between energy drink consumption and cardiac outcomes, including life-threatening arrhythmias(Reference Piccioni, Covino and Zanza10,Reference Levy, Santini and Capucci11) , and possibly hepatic and kidney damage(Reference Al Yacoub, Luczkiewicz and Kerr36). While most consumption of caffeine can be generally considered safe(Reference McGuire37), use of caffeinated energy drinks can present health-threatening risks(Reference Markon, Jones and Punzalan3) that warrant consideration in conjunction with the other unhealthy behaviours addressed in this analysis.
Certain limitations constrained this study, which nevertheless identified several characteristics and risky behaviours correlated with energy drink use in adults. First, even though the study used data from longitudinal cohort studies, the cross-sectional analysis restricted our ability to assess temporality between consumption of energy drinks and behaviours(Reference Arria, Caldeira and Bugbee17); therefore, we are unable to determine if consumption of energy drinks actually led to the risky behaviours, if the risky behaviours simply happened concurrently with energy drink use, and/or if the behaviours actually preceded energy drink intake. Furthermore, we are unable to see if and/or how energy drink consumption may have changed over time and whether such variability would affect the associations detected in the cross-sectional analysis. When data from future iterations of questionnaires among the same cohorts become available, conducting longitudinal analysis will be possible, which in turn will help further elucidate these potential relationships and provide better insight to potentially inform consumer outreach and education and public health interventions going forward. Finally, we could not analyse the relationship between the specific products (e.g. individual brands) and the behaviours assessed, because user characteristics and health outcomes can vary by product(Reference Markon, Jones and Punzalan3).
Conclusion
Findings from this study indicate that energy drink consumption is associated with high BMI (25–30 kg/m2 and ≥ 30 kg/m2) and poor diet quality. Furthermore, findings from this study suggest that any potential health problems due to high BMI and poor diet could be further impacted by several risky behaviours, including smoking and/or e-cigarette use, binge drinking, and illegal drug use that are associated with use of energy drinks, leading to increased risk of morbidity and mortality. Our findings are important to help public health practitioners develop population-level targeted and effective interventions, including education and outreach, to reduce and prevent adverse health outcomes stemming from risky behaviours related to use of energy drinks. Finally, clinicians should be made aware of these relationships to better identify potentially vulnerable patients to provide specific health advice and care.
Acknowledgements
Acknowledgements: N/A. Authorship: Design and Formulation of Research: A.O.M., M.D., J.E.C., B.J.W.; Analysis of data: M.D.; Writing: A.O.M., M.D.; Responsible for Final Content: A.O.M., M.D., J.E.C., B.J.W. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the The Institutional Review Board of the Brigham and Women’s Hospital in Boston, Massachusetts. Written consent was obtained from all study participants.
Financial support:
This study was funded via contracts from the Food and Drug Administration (FDA) and by Nationals Institutes of Health (NIH) grants R24-ES028521 and U01-HL145386.
Conflict of interest:
The authors declare that there are no conflicts of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S1368980022001902








 Open access
Open access