



1. Introduction
A voluminous literature documents that the nutrition and environmental conditions in early-life can shape outcomes over the life-cycle [Kim et al. (Reference Kim, Deng, Fleisher and Li2014); Andalón et al. (Reference Andalón, Azevedo, Rodríguez-Castelán, Sanfelice and Valderrama-González2016); Groppo and Kraehnert (Reference Groppo and Kraehnert2016); Almond et al. (Reference Almond, Currie and Duque2017); Miller (Reference Miller2017); Hyland and Russ (Reference Hyland and Russ2019)]. More importantly, these conditions in utero can influence the likelihood of being born alive. Medical studies find that nearly $70\percnt$ of human conceptions do not result in live births [Boklage (Reference Boklage1990); Larsen et al. (Reference Larsen, Christiansen, Kolte and Macklon2013)]. In fact, the number of normal otherwise viable pregnancies which may end without live births could be as high as $50\percnt$
of human conceptions do not result in live births [Boklage (Reference Boklage1990); Larsen et al. (Reference Larsen, Christiansen, Kolte and Macklon2013)]. In fact, the number of normal otherwise viable pregnancies which may end without live births could be as high as $50\percnt$ [Hamoudi and Nobles (Reference Hamoudi and Nobles2014)]. Thus, given the relative importance of fetal health on the subsequent human capital formation, a growing number of studies have examined what factors affect the fetal survival rate [Hernández-Julián et al. (Reference Hernández-Julián, Mansour and Peters2014); Barreca and Page (Reference Barreca and Page2015); Sanders and Stoecker (Reference Sanders and Stoecker2015); Valente (Reference Valente2015); Nandi et al. (Reference Nandi, Mazumdar and Behrman2018)].
[Hamoudi and Nobles (Reference Hamoudi and Nobles2014)]. Thus, given the relative importance of fetal health on the subsequent human capital formation, a growing number of studies have examined what factors affect the fetal survival rate [Hernández-Julián et al. (Reference Hernández-Julián, Mansour and Peters2014); Barreca and Page (Reference Barreca and Page2015); Sanders and Stoecker (Reference Sanders and Stoecker2015); Valente (Reference Valente2015); Nandi et al. (Reference Nandi, Mazumdar and Behrman2018)].
Since it is very challenging to obtain fetal mortality data, a number of studies have used the likelihood of a live birth being male as a proxy measure of fetal survival rate [Hamoudi and Nobles (Reference Hamoudi and Nobles2014); Hernández-Julián et al. (Reference Hernández-Julián, Mansour and Peters2014); Barreca and Page (Reference Barreca and Page2015); Sanders and Stoecker (Reference Sanders and Stoecker2015); Valente (Reference Valente2015); Ahsan and Maharaj (Reference Ahsan and Maharaj2018); Nandi et al. (Reference Nandi, Mazumdar and Behrman2018)].Footnote 2 The reason for taking this approach lies in the inherent frailty of male fetuses. A seminal study by Trivers and Willard (Reference Trivers and Willard1973) hypothesizes that the reproductive success of a male offspring is more resource-sensitive and variable than that of a female offspring. Eriksson et al. (Reference Eriksson, Kajantie, Osmond, Thornburg and Barker2010) explain the biological mechanism behind these sex-specific differences. Given the weight of the placenta, the authors argue, boys tend to be bigger at birth than girls. As a result, the boys’ placentas are more efficient but may have less reserve capacity. In situations of environmental stress, this confers girls a pre-birth survival advantage.Footnote 3 Unsurprisingly, both fetal and neonatal mortality rates are higher among males than females [Naeye et al. (Reference Naeye, Burt, Wright, Blanc and Tatter1971); MacDorman and Kirmeyer (Reference MacDorman and Kirmeyer2007); Nilsson (Reference Nilsson2017)].Footnote 4 Moreover, mothers, pregnant with male children, are more likely to experience birth complications [Hall and Carr-Hill (Reference Hall and Carr-Hill1982); Sheiner et al. (Reference Sheiner, Levy, Katz, Hershkovitz, Leron and Mazor2004); Drevenstedt et al. (Reference Drevenstedt, Crimmins, Vasunilashorn and Finch2008)].Footnote 5
In this paper, we analyze the impact of a maternal health intervention program on sex ratios at birth to understand whether policies targeted toward improving maternal health also leads to a higher fetal survival rate.Footnote 6 Accordingly, we check if the likelihood of a live birth being male is impacted by the Village Midwife Program in Indonesia by using the first four waves of the Indonesian Family Life Survey (IFLS).Footnote 7 To counter high maternal mortality rates, the Government of Indonesia initiated this program in 1989 and was able to improve body mass index (BMI) for the reproductive age women [Frankenberg and Thomas (Reference Frankenberg and Thomas2001)].Footnote 8 Figure 1 shows that the communities with midwives have experienced an increase in the proportion of live male births as compared to communities with no midwives in our sample.

Figure 1. Changes in the probability of a live birth being male. Note: We calculate proportion of males among total live births for each community before and after a midwife is introduced. We define births from 1981 to 1988 as pre-program period, and births from 1989 to 2007 as post-program period. The communities which received a midwife between 1989 and 2007 are defined as program areas. We calculate kernel density with a bandwidth of 0.05.
To establish causality between the Village Midwife Program and the likelihood of a live birth being male in an empirical set-up is complicated because of the non-random nature of program placement. Frankenberg et al. (Reference Frankenberg, Suriastini and Thomas2005) point out that midwives are initially assigned to communities where health services are either non-existent or very limited and where health status is poor. The extensiveness of the program and phased-in nature over time and location through Indonesia allow us to employ a quasi-experimental method to determine program impacts. More specifically, we make use of the timing and placement information of the Village Midwife Program, available in the IFLS, and employ a difference-in-difference strategy to obtain causal estimates of the program impact. Our identifying assumption is that—conditional on community fixed effects, birth year fixed effects, and various household and time-varying community-level characteristics—the timing of midwife placement is exogenous.Footnote 9 Many of the program areas received the program within a short span of time. Given the rapid expansion within a short duration, it is plausible that the timing was not endogenous.Footnote 10
We find that the placement of a midwife in a community leads to an increase in the likelihood of a live birth being male by around 3 percentage point at any birth order. Given the proportion of males is 48.76 percent for the program communities before the program, this ratio moves to 51.65 percent after the program.Footnote 11 Our results are robust to adding a number of background variables and a rich set of relevant time-varying community characteristics available with the IFLS data set. A placebo test further confirms the validity of the research design. The program effect remains resoundingly similar when we include district-specific linear trend and community-specific linear trend and when we limit the sample within a few years around the arrival of a midwife in a community. Even while considering a mother fixed effects model, the estimate remains similar to our original estimate.Footnote 12 We also check a number of pathways that can explain our results and find significant increases in the likelihood of antenatal care check-up and skilled birth attendance for mainly less educated mothers. We also consider a number of possible alternative explanations for our results such as differential rates of attrition, changes in maternal mortality rate, fertility behavior, and son preference, but do not find any empirical support for these explanations.Footnote 13 Finally, we perform a series of tests to conclude that our main findings are robust to all these checks.
Our results contribute to a greater understanding of fetal survival differences by sex through a policy targeted toward improving maternal health. Andersson and Bergström (Reference Andersson and Bergström1998) report short maternal stature and obesity to be related to a low sex ratio at birth for a town in the Central African Republic. In another study by Cagnacci et al. (Reference Cagnacci, Renzi, Volpe, Alessandrini and Arangino2004), non-optimal reproductive/metabolic conditions among mothers (defined as low pre-pregnancy weight and/or a greater weight gain during pregnancy) are associated with a reduced sex ratio at birth for a data on 10,239 children born in the period 1997–2001 from an institute in Modena, Italy.Footnote 14 Some other studies which analyze the association between maternal characteristics and sex-ratios at birth include Almond and Edlund (Reference Almond and Edlund2007); Hamoudi and Nobles (Reference Hamoudi and Nobles2014); Ahsan and Maharaj (Reference Ahsan and Maharaj2018). A number of animal studies have also examined associations between maternal health and sex ratios at birth. For instance, Rosenfeld and Roberts (Reference Rosenfeld and Roberts2004) find that maternal age and maternal diet, play directive roles in controlling sex ratio among mice. In particular, a diet high in saturated fats but low in carbohydrate leads to the birth of significantly more male than female offspring in mature laboratory mice. We contribute to this literature by examining the possible role of a maternal health intervention in affecting the sex ratios at birth among humans. To the best of our knowledge, our paper is one of the first studies in the economics literature that studies the effects of maternal health intervention on fetal loss as measured by sex ratios, using a quasi-experimental design.Footnote 15
Moreover, consistent with Hatt et al. (Reference Hatt, Stanton, Makowiecka, Adisasmita, Achadi and Ronsmans2007); Frankenberg et al. (Reference Frankenberg, Buttenheim, Sikoki and Suriastini2009), the effect of the program is driven by mothers with low levels of education.Footnote 16 It is well documented that the socio-economic status of mothers affects health care utilization [Hatt et al. (Reference Hatt, Stanton, Makowiecka, Adisasmita, Achadi and Ronsmans2007); Ahmed et al. (Reference Ahmed, Creanga, Gillespie and Tsui2010)]. Since maternal education is an important indicator of socio-economic status, our second finding indicates that the improvement in fetal survival is largest for the socio-economic groups, who are also the greatest beneficiaries of the Village Midwife Program (although the difference is not statistically significant at conventional levels). We also find that the program effect is mostly concentrated among mothers with short height and who live far from a health facility. Our results thus add to the evidence of the Village Midwife program serving to reduce socio-economic disparities in Indonesia as far as health outcomes are concerned.
Overall, our results contribute to a large public health literature that examines the impact of midwives on fetal survival rates [see for review Lassi and Bhutta (Reference Lassi and Bhutta2015); Sandall et al. (Reference Sandall, Soltani, Gates, Shennan and Devane2016); Ota et al. (Reference Ota, Silva Lopes, Middleton, Flenady, Wariki, Rahman, Tobe-Gai and Mori2020)].Footnote 17 We contribute to the existing literature in four ways. First, the studies, in those aforementioned review articles, focus on neonatal mortality, still births, birth weight, height-for-age, preterm birth, fetal loss, etc. as outcomes of interest. Our results show that sex-ratio at birth can be also be an outcome of interest to measure the effectiveness of a midwife program on fetal health in settings where sex-selective abortions are not prevalent. Second, in many cases, these studies are designed and implemented by researchers with the help of non-government entities. In contrast, we evaluate a program that was initiated by the government. Third, these studies can only evaluate the program's effectiveness in limited geographic areas,Footnote 18 whereas we provide an evaluation of a program that was rolled out nationally based on a dataset that covers overwhelming majority areas of the country.Footnote 19 Finally, based on the reviews of Lassi and Bhutta (Reference Lassi and Bhutta2015), Sandall et al. (Reference Sandall, Soltani, Gates, Shennan and Devane2016), and Ota et al. (Reference Ota, Silva Lopes, Middleton, Flenady, Wariki, Rahman, Tobe-Gai and Mori2020), we have not found any other study, which examined the impact of midwife programs on the likelihood of fetal survival in Indonesia. Our study, therefore, complements these studies.
The results have important implications for developing countries. In the last three decades, many developing countries—including Indonesia—have experienced a substantial decline in maternal mortality [Hogan et al. (Reference Hogan, Foreman, Naghavi, Ahn, Wang, Makela, Lopez, Lozano and Murray2010); WHO (2012)]. Global initiatives leading to the adoption of better family planning and maternal health policies have contributed to this decline [Hogan et al. (Reference Hogan, Foreman, Naghavi, Ahn, Wang, Makela, Lopez, Lozano and Murray2010); Ahmed et al. (Reference Ahmed, Li, Liu and Tsui2012)]. Moreover, birth weight data is often missing in developing countries [Currie and Vogl (Reference Currie and Vogl2013)]. In those circumstances, sex-ratios at birth can be used as a measure to gauge benefits to the next generation from policies which improve the health of reproductive-age women.Footnote 20
2. The Village Midwife Program in Indonesia
Indonesia suffered from high rates of maternal and neonatal mortality around the time the Village Midwife Program was launched [Shankar et al. (Reference Shankar, Sebayang, Guarenti, Utomo, Islam, Fauveau and Jalal2008)]. According to Shiffman (Reference Shiffman2003)], Indonesia's first national seminar on safe motherhood was held in 1988, where President Suharto delivered the keynote address. This was held following the 1987 international safe motherhood conference in Nairobi. The primary objective behind the introduction of the Village Midwife Program (also known as Bidan di Desa (BDD)) in the late 80 s, as stated by the Indonesian Ministry of Health (DepKes), was to improve maternal health with a particular emphasis on reducing maternal mortality in rural areas [Frankenberg and Thomas (Reference Frankenberg and Thomas2001)].
The World Bank provided financial support to the program through its fifth population loan to Indonesia, covering the period 1991 to 1996, for an amount of USD 104 million [Shiffman (Reference Shiffman2003).Footnote 21 Within a decade, 96 percent of all locales in the country had access to midwives as the number of midwife villages increased five-fold–from nearly 5,000 workers in 1987 to 80,000 in 2009 [Weaver et al. (Reference Weaver, Frankenberg, Fried, Thomas, Wheeler and Paul2013); WHO (2013)]. According to the Ministry of Health, 40 percent of the 68816 villages in Indonesia had midwives in 2005. This accompanied an increase in skilled delivery from 34 to 64 percent by 1998 along with the percentage of women receiving antenatal increasing from 57 percent in 1987 to 88 percent by 1998. Figure 2 shows the cumulative number of all IFLS villages where a midwife was present each year between 1989 and 2007.
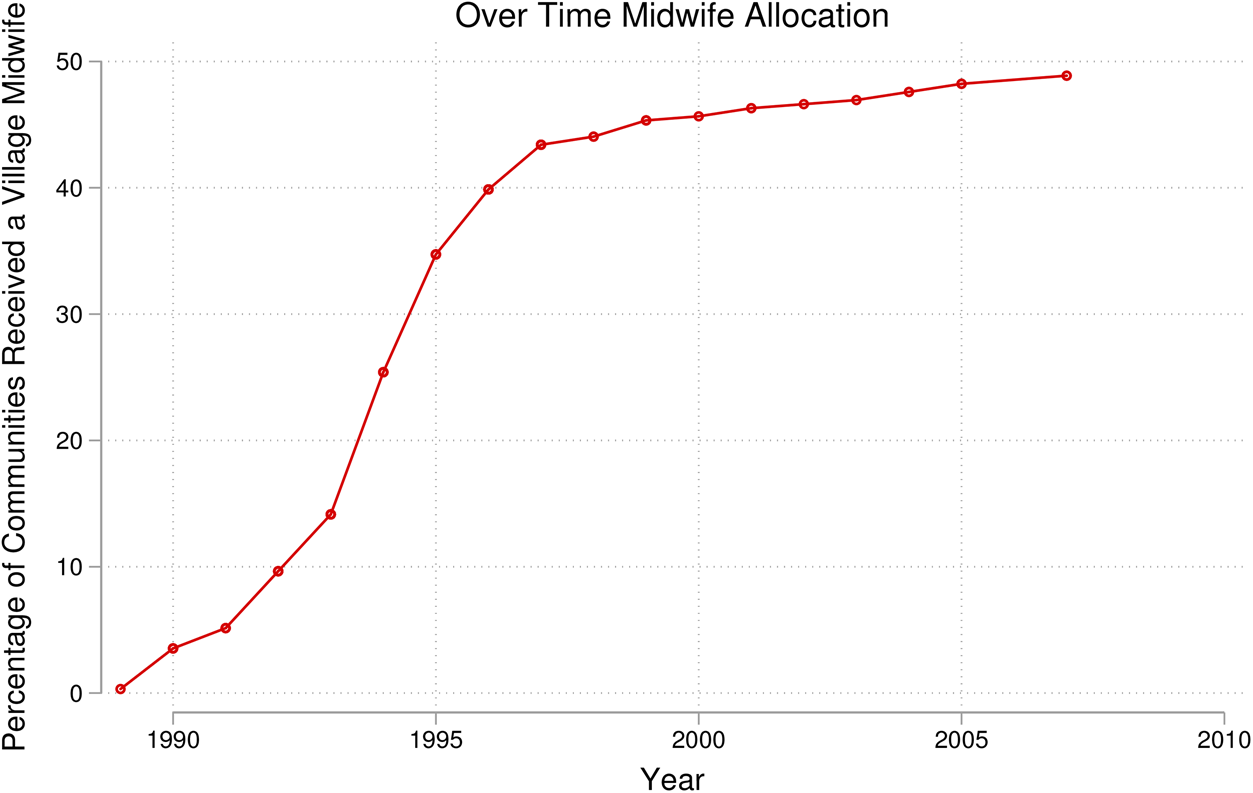
Figure 2. Cumulative number of communities with a midwife
In the beginning, village midwives were typically recruited from nursing programs with one additional year of training in midwifery. Later, this was changed to require that village midwives attend a three-year midwifery academy. These village midwives are largely in their early twenties and single at the entry-level and are usually placed in their province of origin. The practices of a midwife are initially stationed at village delivery post. If no such station exists in the village, home of the village leader acts as the delivery post [Weaver et al. (Reference Weaver, Frankenberg, Fried, Thomas, Wheeler and Paul2013)]. After assignment to a community, village midwives are guaranteed a government salary for at least three years. They should engage in public practice during normal working hours, while they can have their own private practice after duty hours. The goal was to help the midwives sustain their practice without a government salary, once the government contract ends [Frankenberg and Thomas (Reference Frankenberg and Thomas2001)].
The primary goal of a village midwife includes improving the reproductive health of women by providing a variety of health and family planning services. She should work with traditional birth attendants, and act as a link to formal health care delivery systems (e.g., by referring complicated obstetric cases to health centers and hospitals). Unlike the formal health delivery systems, a midwife should pro-actively seek out for patients and visit their homes. As is evident from a number of studies, she acts as a general health resource in a community: advising different health-promoting behaviors including sanitation and nutrition, dispensing medications, immunizations, well-child care, and a variety of acute-care services such as sick-patient visits, administering of antibiotics, attending to wounds, etc. [Frankenberg and Thomas (Reference Frankenberg and Thomas2001) and Weaver et al. (Reference Weaver, Frankenberg, Fried, Thomas, Wheeler and Paul2013)].
As is evident from a number of studies, the Village Midwife Program has met with considerable success. Frankenberg and Thomas (Reference Frankenberg and Thomas2001) find that reproductive-age women in communities which have received village midwives between 1993 and 1997 have experienced a significant increase in body mass index in 1997 relative to 1993. Other successes include higher usage of antenatal care during the first trimester of pregnancy among low educated women, increases in receipt of iron tablets, less reliance on traditional birth attendants for birth delivery [Frankenberg et al. (Reference Frankenberg, Buttenheim, Sikoki and Suriastini2009)], increased usage of injectable contraceptives while the decreased incidence of oral contraceptive and implant use [Weaver et al. (Reference Weaver, Frankenberg, Fried, Thomas, Wheeler and Paul2013)]. Children exposed to the program in early life have also benefited in better nutrition status (as measured by height for age) [Frankenberg et al. (Reference Frankenberg, Suriastini and Thomas2005)].
3. Data and measurements
We use the first four waves of the IFLS, conducted in 1993, 1997, 2000, and 2007, respectively.Footnote 22 We define the communities which were sampled in the first wave of the IFLS in 1993 as the original IFLS communities. There are in total of 311 original communities in the data. During the first survey (1993–94), the sample drawn was representative of $83\percnt$ of the population residing in 13 out of 27 provinces in Indonesia. Within each of these 13 provinces, the enumeration areas (EA) have been randomly selected for inclusion in the final survey. In the first wave, 7,224 households have been interviewed, and detailed individual-level information (including the age and education of the household members) has been collected. The later waves sought to follow up on the same set of households. If any household migrated from its original location, it is usually successfully traced to its new location by the IFLS investigators. The re-contact rates of households from the first wave have been $94.4\percnt$
of the population residing in 13 out of 27 provinces in Indonesia. Within each of these 13 provinces, the enumeration areas (EA) have been randomly selected for inclusion in the final survey. In the first wave, 7,224 households have been interviewed, and detailed individual-level information (including the age and education of the household members) has been collected. The later waves sought to follow up on the same set of households. If any household migrated from its original location, it is usually successfully traced to its new location by the IFLS investigators. The re-contact rates of households from the first wave have been $94.4\percnt$ , $95.1\percnt$
, $95.1\percnt$ and $93.6\percnt$
and $93.6\percnt$ in the second, third, and fourth waves, respectively [Strauss et al. (Reference Strauss, Witoelar and Sikoki2016)].
in the second, third, and fourth waves, respectively [Strauss et al. (Reference Strauss, Witoelar and Sikoki2016)].
For the present study, we use data from pregnancy histories of women which include information on (i) birth date, (ii) sex of the child, (iii) age of the mother, (iv) child alive or not at the time of survey, and (v) if not alive–then age of death. Regarding the placement information of midwives, please note that about 152 communities of the original 311 IFLS communities have received a midwife between the year 1989 and 2007. While IFLS provides data on the start year of a midwife in each of these communities, the information on start month is unavailable. Another difficulty lies in the fact that some of the sampled households and respondents have later moved to other communities. Since migrants could be different from non-migrants along both observable and unobservable dimensions, attrition of the households due to migration could be a concern [Thomas et al. (Reference Thomas, Witoelar, Frankenberg, Sikoki, Strauss, Sumantri and Suriastini2012)]. However, Weaver et al. (Reference Weaver, Frankenberg, Fried, Thomas, Wheeler and Paul2013) argue that conditional on select individual and community characteristics, the receipt of the midwife of a community is not significantly related to a woman's migration out of the study communities or loss to follow up over the study period. The rate of migration in our data is $18\percnt$ —we later show that migration is not systematically related to the placement of a midwife in our data as well.
—we later show that migration is not systematically related to the placement of a midwife in our data as well.
The present analysis is primarily based on the birth cohort born between 1981 and 2007, while the analysis for underlying mechanisms (antenatal care, skilled birth attendance, and birth at a facility) are based on birth cohort born within last five years of the survey.Footnote 23 In our paper, the birth information for children born between 1981 and 1993 comes from the first wave, for children born between 1994 and 1997 comes from the second wave, for children born between 1997 and 2000 comes from the third wave, and finally the birth information for children born between 2001 and 2007 comes from the fourth wave. By constructing the sample this way, we avoid repetition of birth reporting for situations where, a mother, say, in the second wave may report a birth in 1992 which has been reported already in the first wave. For the 1981-2007 birth cohort, birth month information is missing for 1368 births. Rather than dropping these births from the analysis, we randomly impute the birth months from a uniform distribution. Moreover, maternal education information is missing for 177 births, which are dropped entirely from the analysis.
Table 1 presents the summary information of the different samples used in this paper. In panel A, we show the information for the birth cohort 1981-2007. It indicates that about 51 percent of all the live births are male, which is close to the natural biological ratio [Shifotoka and Fogarty (Reference Shifotoka and Fogarty2012)]. The women in the sample, on average, has received at least primary education, as is evident from the mean education of 6 years. The mean age at birth is 26.7 years. In panel B, we show the descriptive statistics for the live births within the last five years of the survey. Again, the proportion of male births is $51\percnt$ . We also find that $60\percnt$
. We also find that $60\percnt$ of the live births were assisted by a skilled attendant, $44\percnt$
of the live births were assisted by a skilled attendant, $44\percnt$ of the births took place in a facility, and $91\percnt$
of the births took place in a facility, and $91\percnt$ received any antenatal care.
received any antenatal care.
Table 1. Summary statistics

Note: Panel A is based on the birth cohort born between 1981 and 2007, and Panel B is based on the cohort born within last five years of the survey and are born between 1989–1999 and 2003–2007. Skilled birth attendance takes a value of 1 if the mother received care from any of the following sources: physician, midwife, and nurse; and 0 otherwise. Birth at facility takes a value of 0 if the birth took place at own home, family member's home, or at the traditional midwife's house (office) and 1 otherwise. Antenatal care takes the value 1 if the mother has received any antenatal care during pregnancy, and 0 otherwise.
In Table 2, we further explore the difference in the incidence of male birth along with maternal and household head characteristics before and after the program, separately for the program and non-program areas. The pre-program period is 1981–1988, and the post-program period is 1989–2007 as the program started in 1989. Here, we find that the baseline incidence of male births is 48.76 percent in the program areas, and in the post-program period, this value changes to 51.65 percent–a 2.9 percent increase. In non-program areas, the incidence of male births is almost identical between the pre-program and post-program periods–the difference is statistically indistinguishable from zero. In both the program and non-program areas, we also observe significant change in maternal years of education, age at menarche, age at first marriage, maternal age at birth, the incidence of the household head being male, and household head years of education. But the magnitudes of the changes are very similar.
Table 2. Comparison of summary statistics before and after the initiation of the program
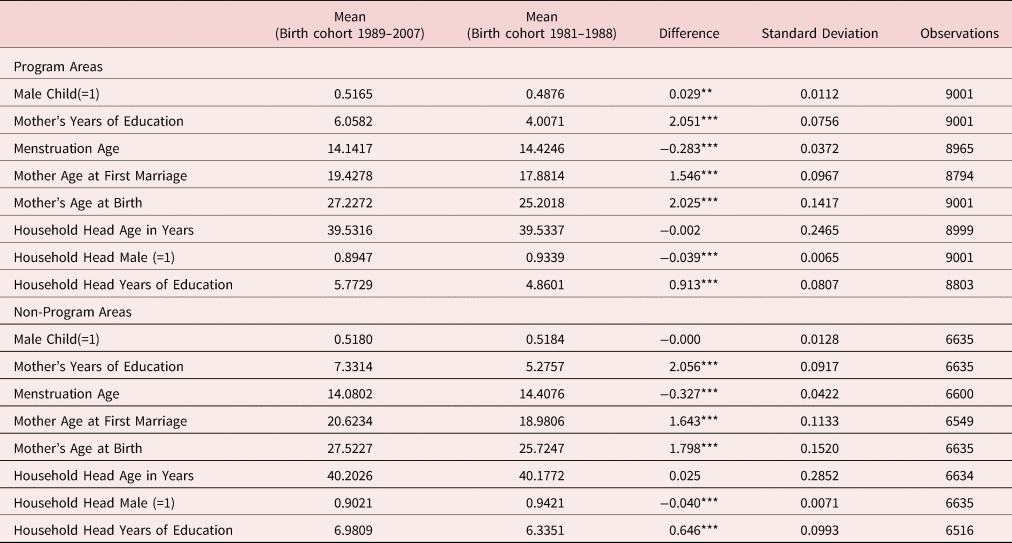
Note: This table compares samples for children born before the start of the program (1981–1988) and children born after the start of the program (1989–2007). Panel A presents summary statistics of program areas and Panel B presents summary statistics of non-program areas. Program areas are communities which have received a midwife between 1989 and 2007 and non-program areas are the communities which have not received a midwife during the same time period.
In panel A of Table A1 in the Online Appendix, we compare the mean of the community characteristics of the program and non-program areas during the first wave. The program communities are different from non-program communities in a number of ways–the former is more likely to be a rural area, less likely to have paved road or public phone or electricity. Also, they are farther from the nearest health facility, market, and district capital center, and have fewer health posts. We compare the maternal and household characteristics for the birth cohort 1981–1988 between the program and non-program communities in Panel B. These births took place before the midwife program started. For the program areas, the likelihood of a live birth being male is lower, the mothers are less educated and marry earlier. The household head characteristics are also dissimilar between the two sets of communities.
4. Empirical framework and results
4.1. Effect of a midwife on the likelihood of a live birth being male
To examine the impact of the midwife program on the likelihood of a live birth being male, we estimate the following linear probability model with community fixed effects for child i who is born in month m, birth order d, year t in community j:

The dependent variable M takes the value of 1 if the child is a male and 0 otherwise. The variable T takes a value of 1 if the community has a midwife in the year of birth, else takes a value of 0. It is important to highlight that T is set equal to zero for children from non-program communities. Thus the source of variation for the discrete version of the treatment variable is the variation in treatment status across communities over time. The coefficient for T is β 1, which captures the treatment effect of the midwife program on the likelihood of a live birth being male. To the extent that the placement of the midwives is not based on any unobserved time-varying characteristics which also affect the dependent variable, the coefficient β 1 will produce causal estimates of a midwife placement.Footnote 24
X ijt is a set of mother level observables, such as maternal education and mother age at the time of the survey. These variables are defined as linear spline functions–for maternal years of education splines, the knots are taken at 6, 9, and 12 while for maternal age splines, the knots are taken at 20, 25, 30, 35, 40, and 45. The results presented in Table A1 in the Online Appendix suggest that a number of community characteristics, including the availability of health infrastructure and remoteness, influence whether it received a village midwife. If the characteristics that influence receiving a midwife also influence sex ratio at birth, the cross-sectional program estimates will be biased unless the specifications include suitable controls. Accordingly, we include a number of controls. θ jt includes a set of time-varying community characteristics such as: if the community has a paved road, the urban status of the community, whether it has a public phone, distance to the market, distance to the district capital center, number of health posts, community electricity status, and distance to the nearest health facility. The inclusion of this broad set of variables substantially mitigates concerns that other simultaneously occurring relevant changes do not confound the program effect. The inclusion of θ j controls for various community-level time-invariant observables and unobservables, while δ t controls for various observable and unobservable shocks during the year of birth at the national level. Moreover, γ m is birth month fixed effects, which control for seasonality, and λ d is birth order fixed effects, which control for any relationship between birth order and sex-ratio [James (Reference James1987)].
We report the effects of the Village Midwife Program on the likelihood of a live birth being male in Table 3 for three different linear probability models— the first is a parsimonious regression specification which excludes mother level observables as well as time-varying community characteristics; the second one includes mother level observables; and the third specification includes both mother level observables and community time-varying characteristics. For all these models, we report the coefficient for the binary specification of midwife exposure. The impact of a midwife in a community is quite large under all the specifications for the entire sample. A child born in a community with a midwife at the time of birth is about 2.8 to 3.1 percentage points more likely to be a male. If we add the impact to the pre-program mean proportion of male child in the program areas of 0.4876, it comes close to the biologically normal ratio of 0.5156 to 0.5186 [Kevane and Levine (Reference Kevane and Levine2000); Almond and Edlund (Reference Almond and Edlund2007); Ahsan and Maharaj (Reference Ahsan and Maharaj2018)].
Table 3. Impact of the village midwife program on the likelihood of a live birth being male: birth cohort 1981–2007
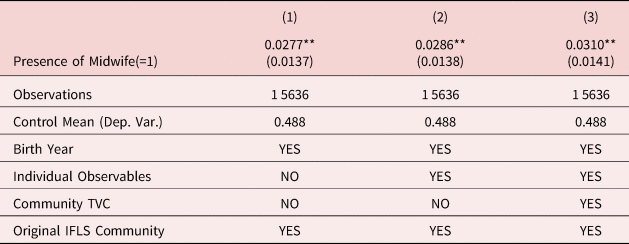
Notes: Standard errors are clustered at the community level (***p<0.01, **p<0.05, *p<0.1). The dependent variable is the likelihood of a live birth being male which takes a value of 1 if the child is male, and 0 otherwise. The variable Presence of Midwife is a dummy for the presence of a midwife during the birth year of a child. The individual controls include maternal years of education (splines with knots at 6,9, and 12) and maternal age at survey (splines with knots at 20, 25, 30, 35, 40, and 45). Community controls include time-varying characteristics at the community level: paved road status, electricity status, number of health posts, urban status, public phone status, distance to market, distance to the district capital center, and distance to the nearest health facility. All regressions include birth month fixed effects, birth year fixed effects, birth order fixed effects, and community fixed effects.
Alternative Specifications
Birth month interacted with birth year—Recall that in regression equation (1), we have included birth month and birth year fixed effects additively. While such a specification controls for seasonality and yearly shocks, it can not absorb month by year changes such as prices of pregnancy inputs (transportation costs, medicine prices, etc.). To explore the robustness of our results, we now control for the interaction of birth month and birth year. Column (1) of the Table 4 reports the results. The coefficient estimate remains similar to our main estimates in Table 3 and is statistically significant at the 5 percent level.
Table 4. Impact of a midwife on the likelihood of a live birth being male–alternative specifications
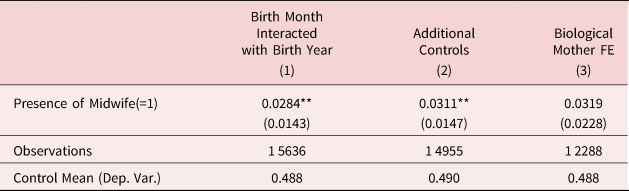
Notes: Standard errors are clustered at the community level (***p<0.01, **p<0.05, *p<0.1). The dependent variable takes a value of 1 if the child is male, and 0 otherwise. The variable Presence of Midwife is a dummy for the presence of a midwife during the birth year of a child. The individual controls include maternal years of education (splines with knots at 6,9, and 12) and maternal age at survey (splines with knots at 20, 25, 30, 35, 40, and 45). Community controls include time-varying characteristics at the community level: paved road status, electricity status, number of health posts, urban status, public phone status, distance to market, distance to the district capital center, and distance to the nearest health facility. All regression specifications also include birth order fixed effects, and interaction of birth month and birth year fixed effects. In column (2), additional controls at the individual and household level include maternal years of education fixed effects, maternal age at survey fixed effects, maternal age at first marriage, maternal age at the onset of menstruation, mother's number of siblings, natural log of per capita expenditure in household, household head years of education, household head age, and whether household head is male.
Additional controls—We also explore if our results are robust to the inclusion of additional mother-level observables, information about the household head and household income. From the IFLS, we can obtain mother age at menarche, mother age at first marriage along with the information on age, sex, and years of education of the household head. Moreover, we control for per capita household expenditure—a proxy for household income. If program communities over time have faster economic growth than non-program areas, the program communities may experience greater fetal survival, and in the absence of any income measure, we might falsely attribute this as a program effect. In column (2) of Table 4, we show the results when we include these controls while controlling for fixed effects for maternal age and years of education instead of splines as was done in the main regression equation specification. The results show that the coefficient estimate does not change even after including these additional controls.
Biological mother fixed effects–Finally, we consider a regression specification with biological mother fixed effects. Biological mother fixed effects control for the observed and unobserved time-invariant mother level variables, including the preference for fertility and sex-composition of children. In Table A2 in the Online Appendix, we first report how the biological mother fixed effects sample compares with the main sample. Not surprisingly, the mothers who are in the fixed effects sample are different in many dimensions; however, the outcome of our study, the likelihood of a live birth being male, is not statistically different between these two samples. Column (3) of Table 4 shows that the impact estimate remains similar even after the inclusion of biological mother fixed effects. However, the estimate is not statistically significant due to large standard errors.
Placebo Test and Robustness Checks
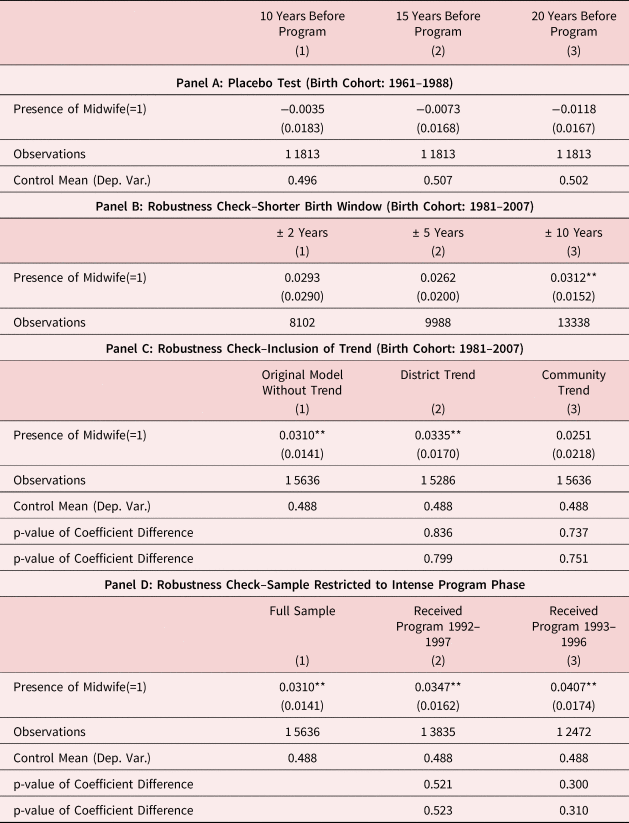
A standard concern in any difference-in-difference analysis is whether pre-trends and mean-reversion drive the treatment effects, rather than the program in question. To address this concern, we perform a placebo program implementation where we try to obtain the program impact if the midwife arrives in a community ten/fifteen/twenty years prior the actual year. We then re-estimate our main specification on this sample for these three situations separately. In the absence of pre-trends and mean-reversion, the impact estimate should be zero for placebo treatments. For this purpose, we limit our sample to the birth cohort born between 1961 and 1988–they were not exposed to the midwife program in utero or before. In Panel A of Table 5, we report the results–the estimated placebo effects are almost zero and statistically insignificant in all three situations, as expected in the absence of any pre-trends in the pre-program period or mean-reversion.
Table 5. Placebo tests and robustness checks
Notes: Standard errors are clustered at the community level (***p<0.01, **p<0.05, *p<0.1). The dependent variable is the likelihood of a live birth being male which takes a value of 1 if the child is male, and 0 otherwise. The variable Presence of Midwife is a dummy for the presence of a midwife during the birth year of a child. The individual controls include maternal years of education (splines with knots at 6,9, and 12) and maternal age at survey (splines with knots at 20, 25, 30, 35, 40, and 45). Panel B and C also include time-varying community characteristics: paved road status, electricity status, number of health posts, urban status, public phone status, distance to market, distance to the district capital center, and distance to the nearest health facility. All regressions include birth month fixed effects, birth year fixed effects, birth order fixed effects, and community fixed effects. Reported p-values reported in Panels C and D refer to the tests for coefficient difference in columns (2) and (3) with respect to column (1). See the text for greater details.
Now we explore if our results are robust to including only births that occur within a short window around the introduction of the midwife. We consider three-time windows: ±2 years, ±5 years, and finally ±10 years around the introduction of the midwife.Footnote 25 The idea behind this exercise is that the shorter the window around the event, the more plausibly exogenous the variation is (less reflective of underlying pre-existing trends, less likely to be affected by attrition, etc.). Panel B of Table 5 reports the results. The estimates remain remarkably similar to our main estimates in all three samples, further validating our research design.
Next, we consider district-specific and community-specific linear trends separately in our regression model. If differential trends in program and non-program areas are driving the results, the inclusion of such trends will cause the estimated program effects to be almost zero. In panel C of Table 5, we report the program estimates after including district-specific and community-specific trends in column (2) and column (3) respectively and then compare the estimates of our original model in column (1). We find that the program effects remain resilient to the inclusion of trends–the values with or without the trend are not statistically different. On a related note, our results are also statistically indistinguishable from our main estimates if we limit the sample only to the communities which eventually received a midwife (not shown in the paper).
Finally, we check how the results change if we only consider program areas which have received a midwife during the intense program implementation phase. Figure 2 indicates that the program expansion was rapid between 1992 and 1997. Among communities which received a midwife between 1989 and 2007, while only 10 percent of IFLS communities had a midwife at the beginning of 1992, 90 percent of these communities had a midwife at the end of 1997. If we consider a shorter time frame, the expansion looks even more drastic–20 percent at the beginning of 1993 versus 82 percent at the end of 1996. Please recall that our identifying assumption is that the timing of program placement is exogenous, conditional on community and year fixed effects and some other observables. Since the Village Midwife Program is rolled out over a number of years, any violation of the identifying assumption is less serious if we restrict our treatment communities only to the ones who have received a midwife during this (short) rapid expansion period. Also, such an approach reduces the concern that other factors, and not midwives, are responsible for the improvement in the likelihood of a live birth being male in the treated communities. In panel D of Table 5, we consider two alternative specifications of rapid program expansion phase–column (2) denotes the period 1992–1997 and column (3) denotes 1993–1996.Footnote 26 In these two columns, we include all non-program communities, while keeping only those program communities which received the program during the intense program expansion phase. In other words, we drop the program communities which received the program outside 1992-1997 (column (2)) or 1993-1996 (column (3)). For both specifications, we find the program effects to be mildly stronger (although statistically similar to our original estimate in column (1)) and statistically significant.
4.2. Pathways
What are the different mechanisms through which the presence of a midwife explains the higher likelihood of live births being male? We discuss two different explanations in this section. First, we check if a midwife is associated with greater usage of antenatal care and modern birth amenities.Footnote 27 Second, we examine whether maternal health improves due to midwives as male children are more sensitive to maternal nutrition in utero.
4.2.1 Use of antenatal care, skilled birth attendance, and birth at facility
In this section, we test the impact of the program on the likelihood of using antenatal care, skilled birth attendance, and births in a facility. WHO (2016) recommends antenatal care for identifying pregnancy risks as well as preventing any disease during pregnancy. Skilled birth attendance is also recommended to address complications during the childbirth [Adegoke and Van Den Broek (Reference Adegoke and Van Den Broek2009)]. As mentioned earlier, male pregnancy is more likely to experience complications than female pregnancies [Hall and Carr-Hill (Reference Hall and Carr-Hill1982); Sheiner et al. (Reference Sheiner, Levy, Katz, Hershkovitz, Leron and Mazor2004); Drevenstedt et al. (Reference Drevenstedt, Crimmins, Vasunilashorn and Finch2008)]. Therefore, all these measures may increase the likelihood of inclusion in the live birth sample for male children compared to female children.
In Table 6, we report the results along with uncorrected p-values for each coefficient, as well as False Discovery Rate corrected marginal “q-values” as in Anderson (Reference Anderson2008). We consider two variants of regression specifications: one with community fixed effects and another with biological mother fixed effects.
Table 6. Impact of the Village Midwife Program on antenatal care, skilled birth attendance, and birth in facility: birth cohort last five years from survey

Notes: Standard errors are clustered at the community level (***p<0.01, **p<0.05, *p<0.1). The sample is restricted to children who are born within last five year of the survey. Skilled birth attendance is a dummy if the mother received care from any of the following sources at child birth: physician, midwife, and nurse. Birth at facility dummy takes a value of 0 if the birth took place at own home, family member's home, or at the traditional midwife's house (office), and 1 otherwise. The variable Presence of Midwife is a dummy for the presence of a midwife during the birth year of a child. The individual controls include maternal years of education (splines with knots at 6,9, and 12) and maternal age at survey (splines with knots at 20, 25, 30, 35, 40, and 45). Community controls include time-varying characteristics at the community level: paved road status, electricity status, number of health posts, urban status, public phone status, distance to market, distance to the district capital center, and distance to the nearest health facility. All regressions include birth month fixed effects, birth year fixed effects, birth order fixed effects, and community fixed effects. Reported q-values are calculated following Anderson (Reference Anderson2008).
In regression specifications with community fixed effects, we find a significant impact of midwife placement on the use of antenatal care.Footnote 28 The impact on skilled birth attendance is also positive but not statistically significant. In contrast, we find the program impact on birth at a facility is negative but again, not statistically significant. The last result points to the possibility of midwives substituting for birth facilities to some extent.Footnote 29
In regression specifications with biological mother fixed effects, we find the impact on antenatal care is even stronger, but it is not statistically significant at 5 percent level due to a larger standard error.
4.2.2 Improvement in maternal health
Improvement in maternal health and nutrition can also increase the likelihood of a live birth being male [Eriksson et al. (Reference Eriksson, Kajantie, Osmond, Thornburg and Barker2010)]. Since we do not have maternal health information during pregnancy, we consider BMI of the reproductive age women at the time of the survey. In Table A4 in the Online Appendix, we show a positive association between midwife exposure and maternal BMI at the time of survey (significant at 10 percent level).
Our results, however, should be interpreted carefully. If current BMI reflects pre-pregnancy BMI, this result implies that a midwife increases BMI of women who have given birth following the program. However, this pattern is also possible if the midwives encouraged women with higher BMI to get pregnant or encouraged women with lower BMI to avoid pregnancy. Another possibility is that the midwife has helped the mothers gain BMI after childbirth. However, Frankenberg and Thomas (Reference Frankenberg and Thomas2001) also find that the addition of a village midwife to a community is associated positively with a change in BMI for women of reproductive age between the first and second waves of the IFLS. We thus conclude by noting that an improvement in maternal health is a likely pathway to increase the likelihood of a live birth being male in our sample, but the evidence is not definite.
4.3. Alternative explanations
4.3.1 Changes in maternal characteristics of the live birth sample
From earlier studies, we know that maternal characteristics (like health and education) may influence the likelihood of a live birth being male [Almond and Edlund (Reference Almond and Edlund2007); Ahsan and Maharaj (Reference Ahsan and Maharaj2018)]. Therefore, it is important to analyze whether the placement of midwives is associated with a change in the distribution of mothers of the live birth sample in the treatment and control communities. We discuss some reasons why this distribution can change in the presence of midwives. First, there could be differential rates of attrition due to migration in the treatment and control communities. Some residents may choose to stay in their communities because of the presence of a midwife or may choose to migrate from non-program communities to program communities. Calculating program effects then becomes difficult even in a randomized control design study.Footnote 30
Second, the provision of a midwife may also affect the maternal mortality rate in the program communities. Please note that the pregnancy outcomes are obtained only if a mother is alive at the time of the survey. Moreover, the provision of a midwife may affect the mortality rates of women differently for different socio-economic characteristics (SES), as educated and wealthy households enjoy favorable mortality outcomes [Galama et al. (Reference Galama, Lleras-Muney and van Kippersluis2018)]. Naturally, the observed parental characteristics of the birth sample will change.
Finally, another concern in evaluating the impact of a health intervention program on pregnancy outcomes is that a health intervention may affect fertility behavior. Frankenberg and Thomas (Reference Frankenberg and Thomas2001) document that a village midwife also provides contraceptives to reproductive-age women. Moreover, they may also offer suggestions regarding family size or birth timing. Again, the provision of a midwife may affect the fertility rates of women differently for different socio-economic characteristics (SES), as educated and wealthy households have lower fertility levels [Handa (Reference Handa2000)]. We can thus expect the observed parental characteristics of the birth sample to change.
We first check the issue of selective migration in the sample. In Table A5 in the Online Appendix, we compare the maternal characteristics between the migrant and non-migrant sample. We find migrant mothers, on the average, to be more educated, younger, getting married at an older age, and experience menstruation at a younger age. This is not surprising: Thomas et al. (Reference Thomas, Witoelar, Frankenberg, Sikoki, Strauss, Sumantri and Suriastini2012) also note that the migrants are generally different from non-migrants in observable characteristics in Indonesia. However, this would be a concern if the midwife program placement has changed the migration behavior of mothers. In Table A6 in the Online Appendix, we report the impact of the midwife placement on the likelihood of migration. For migrants, the treatment variable is assigned based on the origin communities. This means that the variable is based on whether the community of origin has received a midwife or not. We find that the midwife placement has not changed the migration behavior, which is consistent with the findings in Weaver et al. (Reference Weaver, Frankenberg, Fried, Thomas, Wheeler and Paul2013). Thus, we would like to argue that our results are internally consistent.
We now check if the maternal characteristics like maternal years of education, age at birth, age at first birth, marriage age, age at menarche, the likelihood of being married, and height (in centimeter) change between treatment and control communities after the arrival of midwives.Footnote 31 We also compare household head characteristics like age, the likelihood of being a male, and years of education between treatment and control communities. We report the results in the first eleven columns of Table A7 in the Online Appendix. Our results indicate that the placement of a midwife is not associated with any of these mother characteristics—the magnitude of coefficients is small and they are also statistically insignificant.Footnote 32
Moreover, we also examine if the midwife program has any impact on cohort size—this would again mean that the mothers who gave birth to children after the arrival of a midwife in a community would be different from those in our sample who gave birth in control communities.Footnote 33 In order to check this, we aggregate the number of births in community at a year level and then use this community-year panel to regress midwife placement on the total number of births that year. The results are reported in column (11) of Table A7 in the Online Appendix. Reassuringly, the midwife coefficient is not significant, offering no evidence of selective fertility.Footnote 34, Footnote 35
In addition to analyzing the cohort size, we explore whether the program has had any impact on the proportion of women who had at least one child in a given community in a given year. Column (12) of Table A7 in the Online Appendix reports the impact of midwife placement on the proportion of reproductive age women who have given birth in the sample period. We find that the program has not changed that proportion.
4.3.2 Miscarriage/Stillbirths
Please recall that we use sex ratio at birth as a proxy for fetal survival rates in this paper. Measurement of miscarriage or stillbirth is difficult and suffers from misreporting problems in developing and developed countries alike [Sanders and Stoecker (Reference Sanders and Stoecker2015)]. According to Larsen et al. (Reference Larsen, Christiansen, Kolte and Macklon2013), 60 percent of all conceptions naturally get aborted during pre-implantation even before what is known as a miscarriage. Out of the remaining 40 percent conceptions, 30 percent experience live births, and 10 percent experience miscarriage. Thus, for every 3 live births, we should expect 1 miscarriage on an average. In total, we have about 15,636 live births in our sample. The estimate of Larsen et al. (Reference Larsen, Christiansen, Kolte and Macklon2013) suggests that there should be about 5,212 miscarriages/stillbirths in our sample. However, in our data, we only observe 1,573 self-reported miscarriages/stillbirths. This discrepancy in miscarriage number shows that the self-reported miscarriages are far from accurate in our sample.Footnote 36 Also, please note that the Village Midwife Program can have opposing impacts on miscarriages, which may cancel each other out. On the one hand, a midwife could reduce the incidence of miscarriages/stillbirths by providing better maternal nutrition in utero. On the other hand, the reporting of miscarriage/stillbirth could increase because of the midwives; for example, the midwives can help reproductive age women with early detection of pregnancy and termination if it can lead to a miscarriage/stillbirth. Thus, even if the midwife services could lead to a lower incidence of miscarriage, they could also entail a higher incidence of reporting of miscarriage. The possibility that these two opposing effects could cancel out can not be easily ruled out. We report the impact of midwife placement on the incidence of miscarriage/stillbirth in Table A8 in the Online Appendix. The impact of a midwife is almost zero and insignificant. However, lack of detailed relevant data prevents us from determining whether it is measurement error of miscarriages/stillbirths or the above-mentioned cross-cancellation effects of a midwife that can explain the nil impact of midwives on miscarriage or stillbirths in our sample.
Here, it is important to emphasize that a large number of studies find that the provision of skilled birth attendants leads to a decrease in stillbirth incidence [Bhutta et al. (Reference Bhutta, Yakoob, Lawn, Rizvi, Friberg, Weissman, Buchmann, Goldenberg and steering committee2011)]. Therefore, one should not conclude that the provision of midwives did not affect still birth. We are unable to find an impact due to the lack of quality data.
4.4. Additional robustness checks
4.4.1 Starting month of midwives
As was mentioned earlier, we do not have the starting month of midwifery services in a community. To circumvent this problem, we have assumed that midwives started working at the beginning of a year. We now examine if our main results are robust to this assumption. To address this issue, we have assigned start month of midwives randomly from a uniform distribution across these 152 program communities and estimated the program impact for 299 simulations.Footnote 37 We plot the density of such coefficient estimates from the 299 regressions in Figure A2 in the Online Appendix–the mean of the distribution is the same with the coefficient estimate reported in column (3) of Table 3 of the paper.
4.4.2 Missing birth months
Please recall that the information about the month of birth is missing for about 10 percent of the birth cohort 1981–2007. Table A9 in the Online Appendix compares the maternal characteristics of children with missing birth months and non-missing birth months. The table shows that maternal characteristics, including her education, are important predictors of birth month. For missing birth months, we have imputed the missing birth months from a uniform distribution and run the main regression with birth month fixed effects for the whole sample. However, it is important to explore how the estimates change when we drop the births with missing birth months. We report the results in Table A10 in the Online Appendix. The results show that the program effects do not change if we exclude the births with missing birth months from the sample.
4.4.3 First birth order
Our main regression tables include birth order fixed effects. However, the results for the restricted sample of first-order births can still be useful in ruling out son preference as a potential confounder. Previous studies have found no evidence of sex-selection at first birth.Footnote 38 Table A11 in the Online Appendix reports the results for the first birth order. We find that the magnitude of the program coefficient remains comparable, although it is not precisely estimated.
4.4.4 Wantedness of additional children and son preference
The IFLS asks the mothers in the sample whether they want additional children and the desired number of sons and daughters. Although there is no record for son preference in Indonesia [Palloni (Reference Palloni2017)], it might be helpful to learn whether the placement of midwife influenced the wantedness of additional children and son-preference. Column (1) of Table A12 in the Online Appendix estimates whether the placement of midwife has affected the wantedness of additional children–the impact is almost zero and statistically insignificant.
Next, we analyze the impact of the program on son preference. Following Palloni (Reference Palloni2017), we define son preference as a dummy variable which takes the value 1 if the mother wants more sons than girls. In column (2), we find, if anything, the program has a negative impact on son preference. This result is not surprising. An influential study by Jayachandran and Lleras-Muney (Reference Jayachandran and Lleras-Muney2009) finds that parents invest more in girls following the midwife programs in Sri Lanka because parents expect that the girls are less likely to experience maternal mortality. Therefore, it is possible that parents want more girls because girls are now more likely to survive. We can conclude that a greater number of boys following the program is less likely to be associated with changing son-preference.
4.4.5 Recall bias
Recall bias would lead to an overestimation of the program effects if, for example, mothers living in program areas are more (less) likely to report the birth of their daughters (sons) before the start of the program. Unfortunately, we are not aware of any direct way to test this. However, recall bias would be more pronounced if mothers are asked to recall a birth that took place long before the survey. Therefore, restricting the sample to more recent births might be a way to evaluate whether recall bias is overestimating the impacts.
In Table A13 in the Online Appendix, we restrict the sample to children born from 1988 to 2007.Footnote 39 We find the coefficient is 0.028 which is close to the estimates based on full sample reported in Table 3. Therefore, it is unlikely that systematic recall bias is leading to an overestimation of impacts.
4.5. Heterogeneity
In this section, we explore how the impact of a midwife varies by three important determinants of fetal survival, proxied by the likelihood of a live birth being male. We expect mothers who are less educated, less healthy, or live in remote areas are more likely to benefit from the program. Therefore, we re-estimated the models for different sub-samples. These sub-samples are formed by splitting the entire sample at the median level of the various determinants of fetal survival. Using the universe of US linked births and infant deaths, Almond and Edlund (Reference Almond and Edlund2007) tested the Trivers and Willard (TW) hypothesis, which states that the parents in good condition would have more sons and parents in poor condition would have more daughters. They find that better-educated mothers are more likely to bear male children in the US.
In Panel A of Table A14 in the Online Appendix, we show the results when we divide the sample by the median maternal educational attainment. Some of the earlier studies find that the effectiveness of a midwife is mostly driven by low educated mothers. Hatt et al. (Reference Hatt, Stanton, Makowiecka, Adisasmita, Achadi and Ronsmans2007) report that the Indonesian Village Midwife Programme dramatically reduced socioeconomic inequalities in professional attendance at birth. Frankenberg et al. (Reference Frankenberg, Buttenheim, Sikoki and Suriastini2009) find that access to village midwives has a stronger effect on receipt of antenatal care among women with relatively low levels of education than among their better-educated counterparts. In this exercise, we check if the midwives have been able to provide effective care in reducing fetal deaths among the disadvantaged mothers, where disadvantaged mothers are defined as the ones with low levels of education. We find the less educated mothers to be heavily impacted by the program—they are about three percentage points more likely to give birth to a male child in the presence of a midwife in the community. The impact is much smaller for educated mothers. However, we cannot rule out the impacts to be significantly different for the two education groups (p-value for the difference in coefficients is 0.58).
A recent study by Ahsan and Maharaj (Reference Ahsan and Maharaj2018) finds that maternal height can be an important predictor of the likelihood of a live birth being male in India as maternal height is a long term marker of maternal nutrition. Accordingly, we check if the impact of a midwife is greater among the shorter mothers. Panel B of Table A14 in the Online Appendix reports the estimates for the entire sample as well as for the splits by lower and higher than the median height. We find that the program is more successful for shorter mothers than for taller mothers–the estimate for shorter mothers is close to 1.8 times larger than that of the taller mothers. However, the difference in program estimates between the shorter and taller mothers is not statistically significant because of large standard errors.
Another potentially important determinant of fetal survival is access to health care. One of the most substantial economic costs in accessing health care in developing countries is related to traveling to the care [Adhvaryu and Nyshadham (Reference Adhvaryu and Nyshadham2015)] so that the distance to health facilities from a pregnant mother can be an important factor. We thus obtain the program estimates separately for lower and greater than the median distance to the nearest health facility in Panel C of Table A14 in the Online Appendix. Mothers residing farther to a health facility are more likely to be in a more remote area and belong to a more disadvantaged socio-economic group. Moreover, they have fewer chances to visit such facilities during pregnancy on a regular basis and be benefited from such visits. We find that the program estimate is greater among women who live far from a health facility. On the other hand, the impact for the mothers residing closer to a health facility is almost zero. This is reasonable as the former set of mothers are most likely to be the greatest beneficiary of the program, as midwives visit patients in their abode rather than making them to come to the health center.
5. Conclusion
Epidemiological research indicates that males in utero are more susceptible to changes in maternal health as compared to females. Using that insight, we analyze whether a maternal health intervention would influence sex ratio at birth. We consider the Village Midwife Program in Indonesia for this purpose; the program was targeted toward improving the health of the reproductive age women. Our results show that the presence of midwives during pregnancy is associated with an increase in fetal survival rate, as measured by the likelihood of a live birth being male. The effects are greater among disadvantaged mothers. We also find an increase in antenatal care and skilled birth attendance among children who are born alive, suggesting these inputs along with an improvement in maternal health, lead to a greater survival for them.
The results have important implications for evaluating maternal health interventions. Despite the global decline in overall maternal mortality rate, countries in Sub-Saharan Africa and South Asia, still have a long way to go [WHO (2012)]. Based on the evidence of this paper, we would like to argue that maternal health interventions in those countries should improve fetal survival rates, especially among mothers from the lower socio-economic background who are also the greatest beneficiaries from such programs. Our study also underscores the importance of using sex-ratio as an effective metric for evaluation of such maternal health policies, even if routine measures like infant mortality do not change.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/dem.2022.30
Acknowledgments
We thank John Strauss, Jeffrey Nugent, Neeraj Sood, Tridib Banerjee, Amar Hamoudi, Claus Portner and conference and seminar participants at Econometric Society North American Summer Meeting, American Society of Health Economists, UNU-WIDER Human Capital and Growth, Development Economics and Policy (Germany), Economic Demography Workshop, Western Economic Association International, and Southern Illinois University Carbondale. All errors are our own.












