



Introduction
Primary laryngeal chondrosarcoma and its benign counterpart chondroma are extremely rare. Only 0.2 per cent of laryngeal malignancies originate from laryngeal cartilage, of which most derive from cricoid cartilage (72–75 per cent), followed by thyroid cartilage and arytenoid cartilage.Reference Chin, Dubal, Sheikh, Unsal, Park and Baredes1 Hoarseness, dyspnoea, neck mass and dysphagia are the most common presenting symptoms.Reference Chin, Dubal, Sheikh, Unsal, Park and Baredes1 Laryngeal carcinoma can be locally invasive, but rarely metastasises. Prognosis is therefore better compared to other laryngeal cancers such as squamous cell carcinoma, with estimated five-year survival rates around 90 per cent.Reference Chin, Dubal, Sheikh, Unsal, Park and Baredes1 Therefore, treatment with local resection, whilst preserving a functional larynx, is a viable option.
Endotracheal intubation may be hampered by intralaryngeal malignancies or stenosis. In addition, a tube obstructs the surgical field during laryngeal surgery and a (temporary) tracheostomy may be necessary. In patients with benign or low-grade malignant laryngeal tumours such as laryngeal carcinoma, a tracheostomy may be avoided if adequate ventilation can be achieved through an ultrathin endotracheal tube (ETT), which allows surgical visibility. The Tritube (Ventinova Medical, Eindhoven, the Netherlands) is a new tracheal tube (outer diameter, 4.4 mm), which consists of three lumina: a ventilation lumen (2.4 mm diameter), a cuff lumen and a pressure measurement lumen (Figure 1). Because of this small lumen, ventilation is achieved using flow-controlled ventilation with the Evone system (Ventinova Medical). It actively manages the inspiration and expiration, and is able to measure the intratracheal pressure using the extra lumen. Multiple articles have described its advantages over other ventilating methods.Reference Schmidt, Günther, Weber, Wirth, Brandes and Barnes2,Reference Schmidt, Günther, Weber, Kehm, Pfeiffer and Becker3
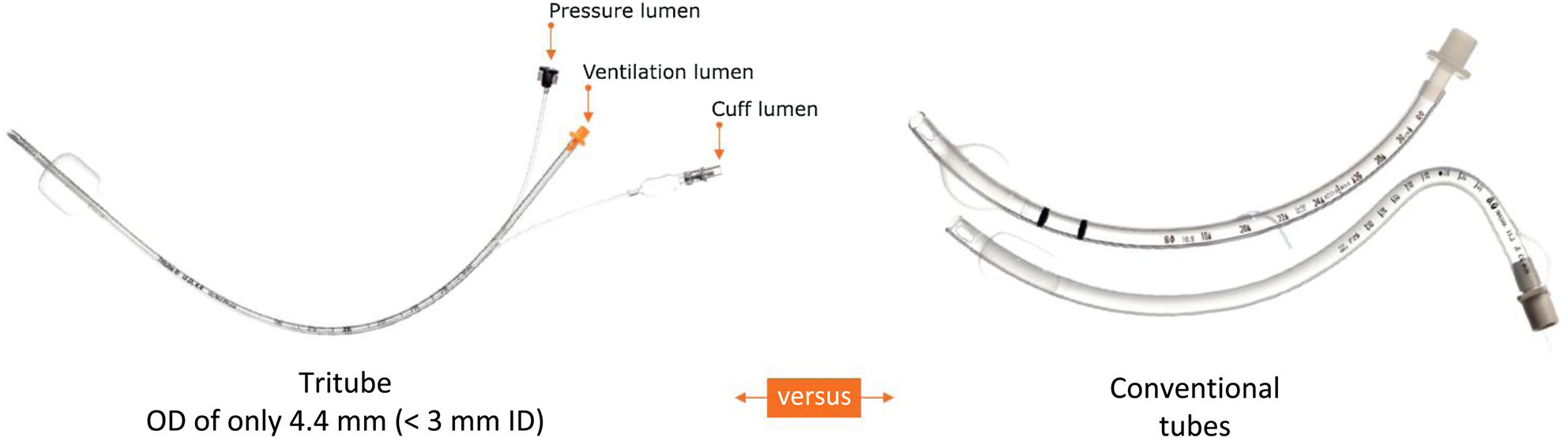
Fig. 1. The Tritube in comparison to conventional endotracheal tubes. Reproduced with permission from Ventinova Medical. OD = outer diameter; ID = inner diameter
We present a patient with a chondrosarcoma deriving from the left arytenoid cartilage that was resected via an anterior laryngofissure. The patient was successfully intubated with the Tritube. Airway surgery was performed whilst keeping this thin tube in situ, thus eliminating the need for a (temporary) tracheostomy.
Case report
A 49-year-old otherwise healthy male teacher presented to a general hospital with hoarseness and stridor that had slowly progressed over 12 months. On digital flexible laryngoscopy, a supraglottic submucosal mass was seen at the site of the left arytenoid (Figure 2). A magnetic resonance imaging scan showed enlarged left arytenoid cartilage with calcifications, indicative of a chondral tumour (Figure 3).
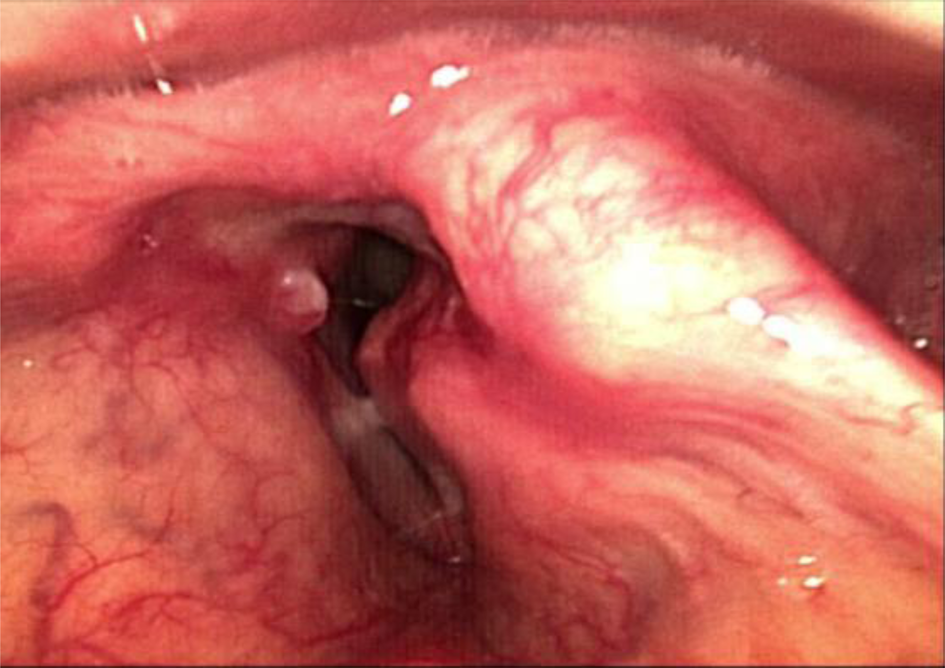
Fig. 2. Diagnostic laryngoscopy: a tumour is seen on the left side. The lumen is narrow and deviated.
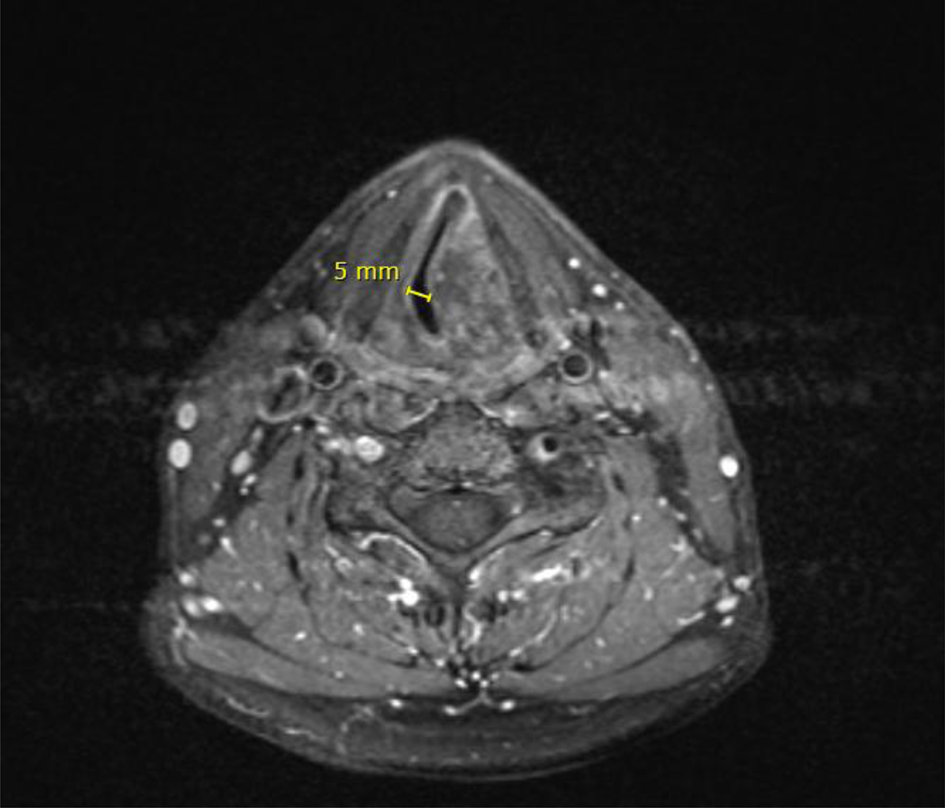
Fig. 3. Axial magnetic resonance imaging scan showing a maximum airway diameter of under 5 mm.
The patient was then referred to our tertiary head and neck centre. The patient underwent direct laryngoscopy with biopsies under general anaesthesia. The mass was hard and fixed in the larynx. Pathology showed a chondral tumour. It was decided that curative local resection should be performed through an anterior laryngofissure.
Because of the fixed intralaryngeal obstruction with a diameter of less than 5 mm, a Tritube was used for intubation. This small tube could just be passed through the narrowed airway with some resistance. There were no complications during or after intubation.
An anterior laryngofissure approach was used to obtain access to the endolarynx and the tumour. A clear view of the submucosal mass and the Tritube in the airway lumen was achieved (Figure 4). The tube did not obstruct the view of, or access to, the tumour. The tumour was resected, including the left arytenoid cartilage. Histology showed a grade I chondrosarcoma.
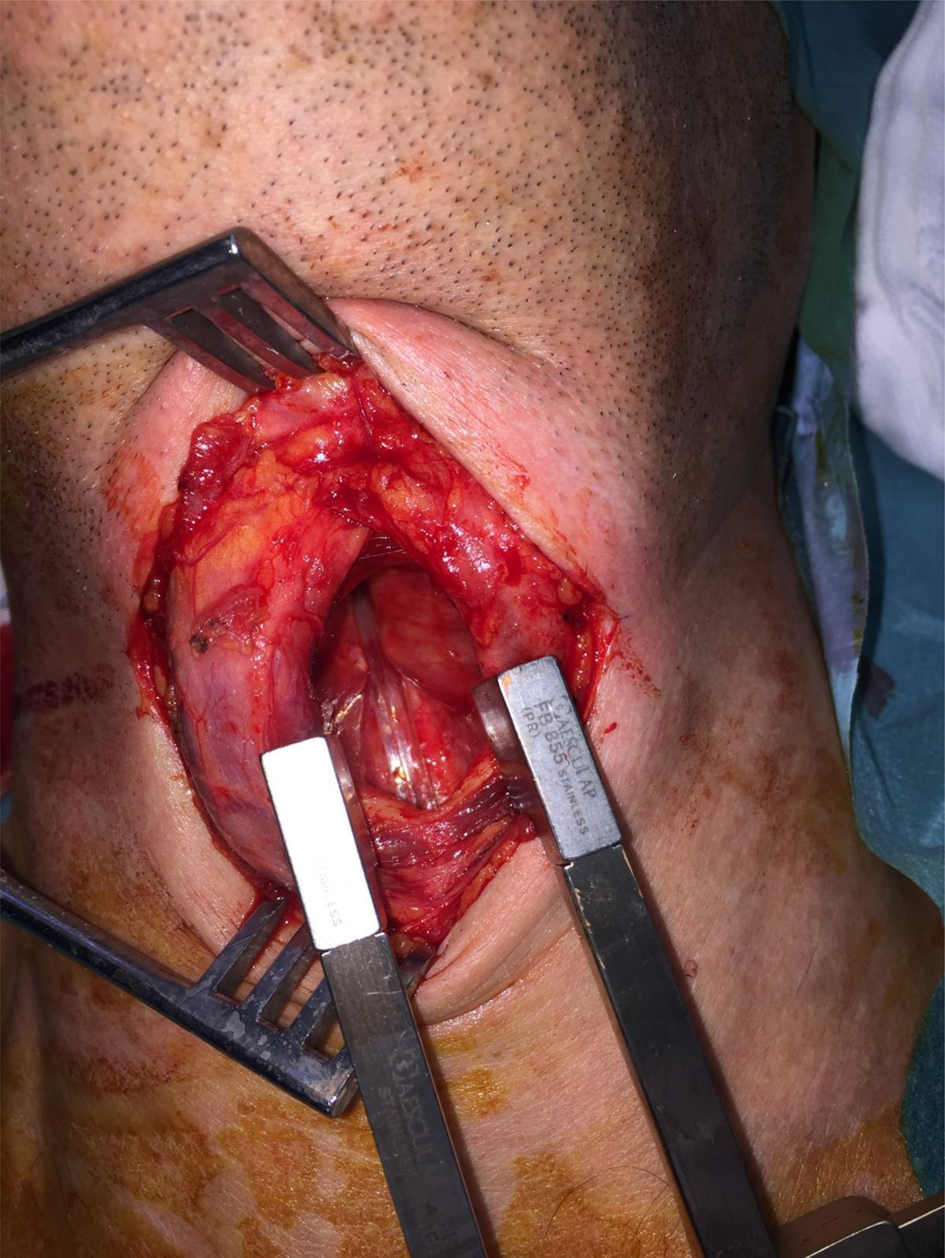
Fig. 4. Opening of the laryngofissure with inspection of the endolarynx. The Tritube is seen in situ. The tumour is seen on the left side. The left vocal fold was stretched over the tumour and the vestibular folds were pushed up cranially.
After the resection, direct laryngoscopy showed some oedema of the vocal folds due to surgical manipulation, but the patient was successfully extubated in the operating theatre. The oedema decreased after a few days (Figure 5). After the procedure, the patient did not experience dyspnoea and had no problems swallowing, and his voice improved. After 5 days, the patient was discharged home and he is now teaching again.
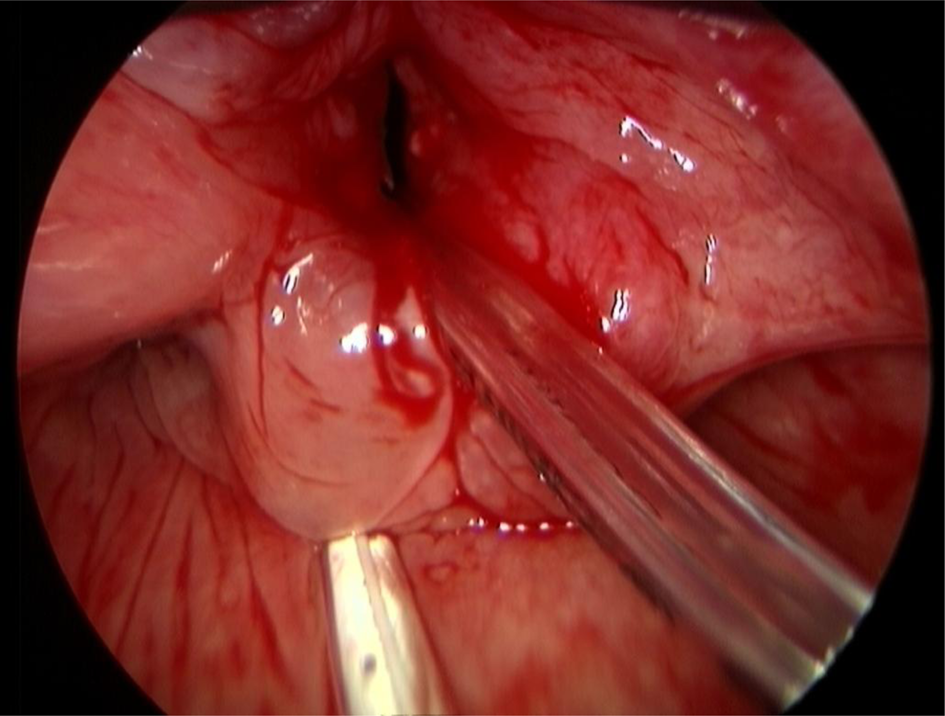
Fig. 5. Post-operative laryngoscopy: there is still some oedema caused by the manipulation during the procedure. The tumour has been removed. The Tritube is seen through the lumen.
Discussion
There are multiple ways to ensure pulmonary ventilation during airway surgery, including the use of a standard ETT, a microlaryngeal tube and high-frequency jet ventilation. The relatively large diameter of a standard ETT leads to obstruction of the surgical field during airway surgery. It needs to be used in combination with a tracheostomy, resulting in a period(s) of apnoea. This is associated with risks of hypoventilation, desaturation and atelectasis formation.Reference Schmidt, Günther, Weber, Kehm, Pfeiffer and Becker3 It may also cause direct mucosal damage. In addition, a temporary tracheostomy severely affects patients’ comfort post-operatively.
• Endotracheal intubation may be hampered by intralaryngeal malignancies or stenosis
• During open surgery for intralaryngeal pathology, a conventional orotracheal tube obstructs the surgical field, thus a (temporary) tracheostomy is usually necessary
• The Tritube is a new ultrathin tracheal tube which may be advantageous over other ventilating methods during laryngeal surgery
• This paper presents a case in which local resection of a chondrosarcoma through a laryngofissure was accomplished without the need for tracheostomy
• The Tritube allowed safe intubation, efficient ventilation and good surgical visibility
High-frequency jet ventilation is regularly used for endoscopic endolaryngeal surgery. High-frequency jet ventilation uses a very thin catheter placed in the airway that propels air under high pressure; therefore, it cannot be used for open laryngeal surgery as the air would leak away through the surgical field.
The main advantages of the Tritube are related to its small total diameter of 4.4 mm, combined with a pressure measurement that protects against barotrauma and a cuff that protects the airway from aspiration.Reference Schmidt, Günther, Weber, Wirth, Brandes and Barnes2,Reference Schmidt, Günther, Weber, Kehm, Pfeiffer and Becker3 Surgeons may operate freely under an acceptable view (Figure 4), and tracheostomy or intermittent apnoea may be avoided. After surgery, the patient will be able to breathe and speak normally, and use of the Tritube may result in less soreness and pain in the throat compared to a thicker tube.Reference Kristensen, de Wolf and Rasmussen4 Narrow airways may also be more easily accessed. Other advantages include avoiding direct damage during the procedure.
Possible disadvantages of the Tritube include the risk of dislocation or occlusion, and not being able to remove secretions from the airway or flush after suctioning. In addition, it cannot be used in laser surgery as it is not laser resistant.Reference Schmidt, Günther, Weber, Wirth, Brandes and Barnes2 The Evone system might also have unfamiliar settings, and it is not possible to switch to conventional ventilation without exchanging the tube for a standard ETT.Reference Schmidt, Günther, Weber, Wirth, Brandes and Barnes2
The Tritube can be used for other laryngeal procedures as well. At our hospital, the Tritube has also been used in more than 10 cases for tracheal resection and reconstruction, eliminating the need for cross-field intubation and a period of apnoea during placement of the anastomotic sutures. Difficult or narrow airways could be an indication for using the Tritube as well. Because of the Tritube's size, intubation can be achieved more easily compared to a standard ETT in difficult or narrow airways. The tube might also be less uncomfortable for patients during or after (awake) intubation.
Conclusion
This paper describes a case in which local resection of a chondrosarcoma through a laryngofissure was accomplished without the need for tracheostomy. The Tritube with the Evone system allowed efficient ventilation and good surgical visibility.
Competing interests
None declared






 Open access
Open access