

In December 1959, Hungary became one of the first countries in the world to begin nationwide mass vaccination with the Sabin polio vaccine. Though not often recognised as a player in the history of public health, this Eastern European state introduced the vaccine to its national immunisation programme four years before the United States – the country where the vaccine was developed. This campaign put Hungary at the frontline of polio vaccination along with the Soviet Union and Czechoslovakia, where the Sabin vaccine was tested. The Hungarian model of annual intensive mass vaccination campaigns became one of the bases on which the WHO built its global strategy of polio eradication in the late twentieth century.Footnote 1
The development and implementation of the live poliovirus vaccine in Hungary is in many ways an unusual Cold War story: one in which scientists all over the world, among them American and Soviet researchers, worked together and shared results that led to the immunisation of millions of children in national mass vaccination programmes. The scientific cooperation surrounding polio seems to have reached its climax in the development of the Sabin vaccine, revealing global cooperation that arched over conventional Cold War hostilities. Polio could clearly no longer be defined as ‘an American story’.Footnote 2
In order to plan and execute prevention methods, develop vaccines and provide state-of-the-art treatment for a new epidemiological phenomenon, scientific communities needed to be constantly in touch with each other, share new experiences and knowledge and cooperate in figuring out the next step. The lack of widely accepted standard procedures and the presence of intense debates in the fields of virology, medicine and public health ensured that a space for exchange and cooperation existed continuously, and it was one that ignored barriers erected after the Second World War between the East and West.
At the same time, the evaluation and introduction of this new vaccine was highly determined by the Cold War itself. Cold War frustrations and preconceptions permeated the scientific debate over the efficacy and safety of the new vaccine. The countries’ choices to introduce the new vaccine were largely shaped by the relations between the national public health structure, the government and its infrastructure and the vaccines, which, in turn, were mostly determined by being part of the ‘capitalist’ or ‘communist’ regime.
Hungary’s encounter with the Sabin vaccine presents a microcosm of global Cold War politics. Hungary’s choice of the Sabin vaccine over the Salk vaccine, and the country’s participation in the network of field trials, had much to do with being part of the Eastern Bloc and having a healthcare system that favoured mass vaccination programmes. Moreover, the particular ways in which the introduction of the Sabin vaccine and the success of eliminating polio from the country’s epidemiology reports gained political significance show the dynamic nature of the Iron Curtain. In an effort to prevent the epidemic, gaping holes opened through which the two sides connected, only to close again when the East and West realigned along conventional Cold War lines.
Drawing the Iron Curtain: Development of Live Poliovirus Vaccines
Hungary’s experiences with polio vaccines and the government’s decision to switch from Salk to Sabin were nested in a broader process of vaccine development. While the laboratory work of the development of live virus vaccines has a fascinating history in itself, it is the human experiments and field trials that provide the most compelling insights into the Cold War political context of vaccine development. Research groups headed by three different scientists tested three different vaccines across the globe, spanning South America to South East Asia and Africa to Eastern Europe. By 1959, according to the WHO’s report,Footnote 3 at least fifteen countries had conducted field trials with live poliovirus vaccines. The international cooperation in organising the trials and coordinating the evaluation of the new vaccines was unprecedented in this formative decade of international public health.
Although the live poliovirus vaccine, developed by Albert Sabin, made its official debut in national vaccination programmes in 1959 and 1960, its story in fact began much earlier. The concept of live virus vaccines had been known for decades before live poliovirus vaccine development started, and work on the live vaccine ran parallel to Salk’s research on the inactivated vaccine.
Live virus vaccines had been in use for more than 100 years in the case of smallpox and for over twenty years in the case of yellow fever.Footnote 4 The concept, therefore, was not new, and many thought that a live vaccine would be more effective than the killed one to begin with, in that it would work quicker and probably provide a more lasting protection since it followed the pattern of a natural infection.Footnote 5 Most importantly, those vaccinated would put the attenuated virus back into the environment through their stools, creating a chance to immunise others indirectly.Footnote 6 The challenge of the live, attenuated polio vaccine was to find a strain of virus that would not cause paralysis, but would provide immunity nonetheless. This method took considerably longer than Salk’s process of finding a way to kill the virus and preserve it.
It was Max Theiler, developer of the yellow fever vaccine, who introduced the idea of a live attenuated poliovirus. In 1946, after passing poliovirus continuously through mice, he reported having produced a strain that immunised monkeys without causing paralysis in them.Footnote 7 Theiler did not pursue this research further, but several of his peers did: in the 1950s Hilary Koprowski, Albert Sabin and Herald Cox took on live polio vaccine development.
Koprowski was born in Warsaw to a Jewish family and left Poland in 1939 after the Nazi occupation. From working with the Rockefeller Foundation in Brazil on yellow fever, he arrived at the Lederle Laboratories in the United States, where he started to work on the live polio vaccine. Albert Sabin, the most well-known of the three, was of Russian descent, also from a Jewish family, and worked on the polio vaccine at the University of Cincinnati. H. R. Cox, an American scientist, became head of the Virus and Rickettsial Research Department at Lederle Laboratories in 1946 and, for a while, worked with Koprowski there.
The first researcher to conduct experiments with live poliovirus vaccine was Koprowski. In 1947, he was his own first experimental subject; three years later he moved on to experimenting on mentally disabled children in a state institution in New York’s Hudson Valley.Footnote 8 In light of the Nuremberg Code of 1947, this was an ethically dubious experiment at the least even by contemporary standards. Koprowski received much criticism when he presented his results in 1951 to a round table convened by the National Foundation of Infantile Paralysis. Reservations about his methods softened as time went on, and his experiment on ‘volunteers’ became represented as a brave first step in the development of a new and successful vaccine.Footnote 9
In 1956 a new opportunity presented itself for Koprowski to test his vaccine, this time in Belfast, Northern Ireland.Footnote 10 Koprowski, therefore, also became the first to take his vaccine abroad. The trial, however, turned out to be a disappointment for Koprowski’s Irish counterpart: the strain used by Koprowski proved to be unsuitable as a vaccine, since it regained its cytophatic power, turning virulent in the volunteers’ bodies. It was thus deemed unsafe.Footnote 11
Korpowski, Sabin and Cox turned to field trials outside the United States in part because the Cutter incident had raised suspicions against polio vaccines. In the spring of 1955, almost 200 patients in the United States (mostly children and family members) had contracted paralytic polio from a faulty batch of the Salk vaccine produced by the Cutter laboratories.Footnote 12 This incident had a tremendous impact: it shook public trust in the vaccine and changed vaccine regulation and control in the United States.Footnote 13 Furthermore, by the time Sabin’s vaccine required mass testing in order to establish its efficacy, the Salk vaccine had become widespread in the United States. Millions of children were now immunised with the killed-polio vaccine, making it impossible to test and evaluate a new vaccine against the same disease.
Not everyone shared the excitement over this international project, however. United States health officials did not uniformly accept vaccine testing on foreign ground. In a congressional hearing on polio vaccines in 1961, Alexander Langmuir, chief epidemiologist of the Department of Health, Education and Welfare and founder of the Epidemic Intelligence Service, found it important to note that ‘it is not as though they [Koprowski, Sabin and Cox] went elsewhere to test. They went to the place to test that would give the best tests, but all of the questions were started and worked on in this country before any overseas activity.’Footnote 14 In a scientific race between East and West, the fact that such an important vaccine was first widely tested and produced outside the United States needed explanation and emphasis that all, indeed, were first developed on American soil. Cooperation may have characterised live vaccine development, but Cold War frustrations gave context to its presentation.
From 1958, international live poliovirus trials accelerated, due to a report published by the World Health Organisation (WHO). That year, a severe polio epidemic outbreak in Singapore provided the first opportunity for a trial of Sabin’s vaccine. The WHO’s Second Expert Committee Report on Poliomyelitis recounted that eleven weeks into the epidemic, the Singapore government decided to introduce the vaccine.Footnote 15 The report stated that ‘there would appear to be sufficient justification for initiating at this time trials of the currently-available tested lots of attenuated poliovirus vaccine in increasingly large numbers of people.’Footnote 16 This was the green light for which live virus researchers had been waiting. Proponents of live vaccine field trials trumpeted the report’s recommendations that a large-scale trial of attenuated vaccine should be attempted in the face of an emerging epidemic, and in a place where polio was endemic. Sabin agreed to the trial on the condition that ‘adequate laboratory control could be assured’.Footnote 17 Almost 200,000 children were vaccinated on a voluntary basis.
Koprowski also kept working on his vaccine after he left the Lederle Laboratories and relocated to the Wistar Institute at the University of Pennsylvania. In early 1958, he conducted a mass-vaccination trial in the Ruzizi Valley in Belgian Congo.Footnote 18 The idea of an animal trial in the Congo came up in personal conversations during Koprowski’s participation in a rabies conference organized by the WHO in 1955 in Kenya. The trial, involving chimpanzees and their carers, was soon broadened to include a total of 244,596 people living in the Belgian Congo and Ruanda-Urundi.Footnote 19 It is not clear how volunteers were recruited, or if the people living under colonial rule had a choice about, or full understanding of, the trial for which they were enlisted. In any case, this time there was no protest by fellow scientists on ethical grounds.Footnote 20 In the end, the project was inconclusive, and was discontinued as efforts for independence from colonial rule generated political and social upheaval in the country.Footnote 21
Lederle Laboratories also continued with vaccine development and conducted field trials of their own in Central America in 1959, using a vaccine developed by Herald Cox in Colombia, Nicaragua and Costa Rica.Footnote 22 The mass immunisation campaigns in the latter two countries produced disappointing results, as the number of polio cases did not fall significantly after vaccination.Footnote 23 However, a controlled trial in MinnesotaFootnote 24 with the same vaccine reported ‘excellent antibody responses’.Footnote 25
Koprowski’s strains were later widely tested in Finland and Poland. In Poland, the introduction of Koprowski’s vaccine followed that of the Salk vaccine by one year.Footnote 26 During the five months between October 1959 and April 1960, more than 7 million children were immunised,Footnote 27 including roughly 80 per cent of the population between 6 months and 15 years of age.Footnote 28 In 1961, the country reverted to the Salk vaccine after an increase of polio cases following the oral vaccination with Koprowski’s Type III attenuated strain over the previous two years.Footnote 29
It is not clear how Koprowski was able to conduct such a large field trial behind the Iron Curtain. He was born in Poland, certainly, but as an immigrant living in the United States, his experimentation on Polish youth with American-made vaccines could easily have made him a suspect rather than a friend. Contemporary reports and articles never addressed the issue of Koprowski’s access to an Eastern European country’s children for field trials. Perhaps one of the reasons is that another influential and large field trial diverted attention from Koprowski’s endeavour: one that was not only conducted behind the Iron Curtain, but in the grounds of the arch enemy itself. This was Albert Sabin’s vaccine in the Soviet Union.
The new vaccine was the result of an exceptional cooperation between Russian and American scientists, Mikhail Chumakov and Albert Sabin, at a particular moment of the Cold War. The slight thaw that followed Stalin’s death opened up new opportunities for exchange. Khrushchev’s secret speech against Stalin’s rule had significant effects for the biomedical sciences as well.Footnote 30 Historian Saul Benison argues that it was the increase in the incidence of polio that convinced Soviet authorities that ‘it was costly socially and economically not to take advantage of the great breakthroughs in American biomedical research vis-à-vis polio’.Footnote 31 For the first time since the Second World War, medical cooperation between the two superpowers started to become a reality.
In early 1956, a Soviet medical mission arrived in the United States, led by Mikhail Chumakov, his wife and colleague Marina Voroshilova and Anatoli Smorodintsev.Footnote 32 This visit was significant enough for Hungarian newspapers to keep the public informed about it, from the arrival of the Soviet scientists to their engagement with American colleagues.Footnote 33 The delegation studied the production of the Salk vaccine and ongoing research in epidemiology. During the trip, they also visited the laboratory of Albert Sabin. This visit turned out to be the beginning of a decade-long exchange. Sabin returned the favour in June 1956, spending a month touring the Soviet Union for talks and laboratory visits. Scientists, specimens and vaccine vials crossed the Iron Curtain in both directions as cooperation intensified between American and Soviet virologists, especially between Sabin’s and Chumakov’s groups. This cooperation had the blessing of both the FBI and the State Department, despite warnings from the Department of Defense that the materials and research involved could be used in making biological weapons.Footnote 34 Scientists’ foreign travel was not strictly controlled only on the Eastern side of the Iron Curtain. In the 1950s, many American scientists in other fields ran into difficulties or were denied passports for political reasons when applying (600 passport applications were rejected on political grounds in the 1950s up until 1958).Footnote 35 Sabin’s relative freedom in travelling, therefore, was not entirely typical of his time.
In the broader context of scientific cooperation between the two sides in the Cold War, the exchange of knowledge and specimens among Sabin and Chumakov was a rare, albeit not unique, phenomenon. While the American and Russian virologists shared virus strains, production and testing methods in developing the live polio vaccine, the post-Stalin era gave way to various collaborative projects. The International Geophysical Year (IGY), held between 1957 and 1958, and the Antarctic Treaty proclaiming Antarctica to be a ‘continent dedicated to peace and science’ were heralded as symbolising the universality of science and international cooperation.Footnote 36 At the same time, the IGY and the Treaty reflected deeply ingrained Cold War hostility and the concerns over the Space Race.Footnote 37 Attenuated poliovirus strains were also not the only biomedical specimens to circulate the globe in the 1950s. From the immediate post-war years onwards, blood samples were collected around the world to determine the frequency of blood groups,Footnote 38 and with the rise of serological epidemiology, serum banks were organised under the auspices of the WHO to collect and freeze blood for epidemiological surveillance and ‘for as yet unknown’ uses.Footnote 39
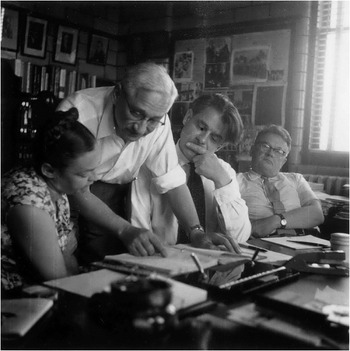
Figure 5.1 From left to right: Marina K. Voroshilova, Albert B. Sabin, Mikhail P. Chumakov, Anatolii A. Smorodintsev. Undated. Miscellaneous, Assorted Letters and Photographs. Box 01. File 05 (Assorted Professional Photographs, 1950s–1960s). University of Cincinnati. Hauck Center for the Albert B. Sabin Archives.
The exceptional quality of the scientific exchange between Sabin and Chumakov was that it resulted in a tangible product that would be widely used and considered successful in both the East and West: the polio vaccine used today in eradication efforts. Their cooperation led to the largest field trial in the history of polio, involving over 16.5 million people across the Soviet Union.Footnote 40 As soon as Sabin finished selecting the optimal strain for creating the vaccine, he sent samples to Smorodintsev in Leningrad. Field trials with the strain started in 1957 on a very small scale, with the vaccination of sixty-seven children. This number gradually grew to 150, then to 2,010, and finally to 20,000 in 1958.Footnote 41 Parallel to Smorodintsev’s trials, another field trial, initiated by Chumakov, then director of the Poliomyelitis Research Institute in Moscow, took off in greater proportions. Chumakov asked Sabin to send him ‘the greatest possible amount’ of vaccine for testing and producing. Sabin sent enough to vaccinate 300,000 children.Footnote 42 Chumakov started the trial with 20,000 and, following its initial success, was able to conduct the largest field trial to date in the history of polio vaccines.
By the end of 1959, over 15 million people, spanning fourteen republics of the Soviet Union, were vaccinated in the trial. Smorodintsev and his team immunised more than 1.5 million of the subjects; the rest received the vaccine from Chumakov’s lab in the Institute for Poliomyelitis Research in Moscow. The Soviet Union’s Minister of Health issued an order on 16 December 1959 for the mass immunisation of the whole population between the ages of 2 months and 20 years by July 1960. This meant vaccinating 77 million people in a matter of months.Footnote 43 The British Medical Journal deemed this campaign a ‘Blitzkrieg against poliomyelitis’.Footnote 44
Parallel to the Soviet campaign, smaller but equally important trials were conducted in Czechoslovakia and Hungary. Both countries had seen severe outbreaks of polio in the 1950sFootnote 45 and already had a strong interest in live poliovirus vaccines. Moreover, the use of live poliovirus vaccine and its potential to eliminate the wild virus from the environment fitted well with socialist medicine’s emphasis on prevention and an interventionist approach to the environmental causes of illness and disease, as heralded by CzechoslovakianFootnote 46 and HungarianFootnote 47 public health professionals.
Collaboration in the trials and mass vaccination with the Sabin strain did not occur in Eastern Europe suddenly, nor did it come through the Soviet Union. Sabin had been in touch with Hungarian and Czechoslovakian scientists for years by the end of the 1950s, sharing views, data and methods, mostly on vaccine production and efficacy. His impressive correspondence attests to an extensive professional network that fostered scientific exchange and personal ties within and across the Iron Curtain. Scientists from East and West met not only at international conferences, but collaborated in laboratory work, shared publication drafts,Footnote 48 circulated specimens,Footnote 49 advised each other on methods and kept each other up to date on the latest results. Sabin’s own research no doubt benefited from this intensive exchange, as he had direct and instant access to work conducted in laboratories across Eastern Europe. Conversely, Hungarian and Czechoslovakian virologists gained easier access to publication opportunities in international journalsFootnote 50 and later received help, through invitations and scholarships, in facilitating study trips to the United States.Footnote 51
This collaboration and the personal connections between virologists in the East and West rested on long-standing ties. Hungarian publications on polio, published between the world wars, demonstrate an extensive knowledge of contemporary epidemiological research and place findings in the context of up-to-date data and theories published by German, French, Romanian, Swedish, American and British colleagues.Footnote 52 Many further ties were established in the interwar era. The Rockefeller foundation had a significant role in setting up public health institutions and providing fellowships for study in the United States for researchers and public health officials in both countries.Footnote 53 Grants from the Rockefeller Foundation continued to be available to individual researchers due to its shift from public health to grants in medical research and education in the immediate post-war years;Footnote 54 it greatly fostered connections in polio vaccine development, and, indirectly, affected the politics of polio research in the United States. For instance, returning from one of his Eastern European trips, Sabin served as an intermediary for the Czechoslovakian Dionyz Blaskovic, who had worked closely with Jonas Salk and Thomas Francis on a Rockefeller Grant in obtaining freeze-dried blood serum specimens.Footnote 55
The relatively large field trials in Czechoslovakia were organised by the Hygiene and Epidemiological Service in 1958 and 1959, with vaccines prepared from the Sabin strains by the Institute of Sera and Vaccines in Prague and additional batches acquired from Chumakov in the Soviet Union.Footnote 56 While personal relationships provided the basis for the endeavour, the Czechoslovakian scientists requested Sabin’s assistance through the WHO.Footnote 57 Sabin personally aided the bureaucratic process of shipping the strains from Cincinnati to Prague in the spring of 1958 and kept a close eye on the trials.Footnote 58 The trials were conducted in four regions (Ústi nad Labem, Liberec, Juhlava and Ostrava)Footnote 59 and in total 140,000 children between 2 and 6 years of age were vaccinated.Footnote 60
Finding the serological results favourable, Vilem Skovranek, head of the Hygienic Services, had already laid out a potential plan to extend the vaccination to a broader, national scale in early 1959, but was discouraged by the uncertainty of the vaccine supply at the time.Footnote 61 Based on studies by mostly Soviet scientists,Footnote 62 the vaccination programme was eventually extended to a nationwide campaign in 1960. By the use of domestically produced vaccine from Sabin strains and also vaccine imported from the Soviet Union,Footnote 63 93 per cent of Czechoslovakia’s child population was vaccinated, totalling roughly 3.5 million children between the ages of 2 months and 14 years.Footnote 64 The mass vaccination was deemed to be an instant success: no confirmed poliomyelitis cases developed in the territory of Czechoslovakia in the first two epidemic seasons after the beginning of the campaign.Footnote 65
Although less widely known than the field trials and early mass immunisation programmes in the Soviet Union and Czechoslovakia, Hungary was also among the Sabin vaccine pioneers. Hungarian virologists and public health authorities had been following oral vaccination trials closely throughout the year. They met with Chumakov, Sabin and Smorodintsev in Moscow in May, along with virologists from Czechoslovakia and Poland.Footnote 66
A turning point in the development of serious interest came with the epidemic of the summer of 1959. In September the State Hygienic Institute hosted an international congress on microbiology, at which one of the focus points was the issue of live polio vaccines. Chumakov delivered the keynote address about the Russian findings,Footnote 67 while Albert Sabin’s presentation was read in his absence. Vilem Skovranek, deputy minister of health in Czechoslovakia and a key player in the Czechoslovakian field trials, also presented a paper on the live polio vaccine.Footnote 68 He soon recounted his experiences at the conference to Sabin in a letter, and added that ‘both in Hungary and [Czechoslovakia] a mass vaccination with live vaccine is planned for the beginning of 1960’.Footnote 69
In fact, Hungarians did not wait until the following year to introduce the Sabin vaccine. György Ivánovics, a virologist, informed Sabin in October that they were intending to begin vaccination in a limited section of the country in November and would later extend it to the whole of Hungary.Footnote 70 Trials began in Győr-Moson-Sopron County in 1959 on 3 and 4 November, during which the population between the ages of 3 months and 15 yearsFootnote 71 was vaccinated. Virologists reported the average acceptance rate of the vaccine to be 96 per cent.Footnote 72 The trial was short, and little time was spent on the evaluation of the results. The State Hygienic Institute analysed 127 stool samples before and after the trial to investigate the presence of the attenuated virus after vaccination, but the overall evaluation of the vaccine and the decision to introduce it nationally were based on the large-scale field trials conducted by the Soviet Union, as well as the experiences of Czechoslovakia and Singapore with the Sabin, and Poland and the Belgian Congo with the Koprowski strains.Footnote 73
‘There Is No Cold War’
While international meetings gave a frame to scientific collaboration and served as a venue to discuss problems and display trial results, national policies regarding science funding and research directions also contributed to collaboration in polio research. The moment of political thaw that made the global cooperation of live poliovirus vaccine development possible coincided with several turning points in scientific research conditions on both sides of the Iron Curtain. The United States had recently increased federal financial support for scientific research, and Washington became more receptive to international cooperation in the field.Footnote 74 American scientists had more resources and support to work together with foreign colleagues. In fact, research opportunities widened on a massive scale for both superpowers, fuelled by intense political, economic and military rivalry.Footnote 75 Ironically, then, antagonistic Cold War objectives helped open opportunities for cooperation across the Iron Curtain.
At the same time, in the Soviet Union, scientific discourse was changing, gradually breaking with Stalinist concepts of the superiority of a particularly Soviet form of science and medicine.Footnote 76 According to Sabin, the vice president of the Soviet Academy of Sciences made this change clear when, in defence of Sabin at a lecture in the Soviet Union, he stated, ‘[W]e have now reached a stage in Soviet science where we cannot and should not any more speak of Soviet genetics, Western genetics or American genetics. There is just one kind of genetics, the kind that gives reproducible results.’Footnote 77
As shown in Chapter 1, polio began to create a unique space in Cold War politics preceding the thaw, mainly due to the involvement of children’s health and the threat of disabling future generations amid post-war recovery. The internal changes and new avenues in both American and Soviet scientific environments, together with a more general thaw in Cold War policies, further widened this space to produce a hitherto unprecedented medical cooperation between the two arch-enemies.Footnote 78
The global effort to put a stop to polio epidemics created a community of scientists who transcended Cold War barriers and defied the world order. Scientists and national public health authorities shared results of field trials from all over the world with three different live virus vaccines, along with updates on vaccine use and epidemiological data, in the pages of major scientific journals and at international conferences.
For instance, at a symposium and conference in Moscow in May 1960, in addition to the 300 specialists from the Soviet Union, 73 foreign scientists from 19 countries took part in eight working sessions. During the three days of the conference, ‘23 reports and communications results were summarized of the mass application of live poliovirus vaccine in 9 republics of the Soviet Union, as well as in Poland, Hungary, China, Bulgaria, Sweden and the USA.’Footnote 79
The success of the new vaccines ignited a scientific euphoria, strengthening the sense that science, as putatively objective and universal, could serve as a tool to stop the Cold War and unite humanity in a common bond. Opening the Sixth Symposium of the European Association of Poliomyelitis in 1959 in Munich, the organisation’s president referred to the participating scientists, from twenty-five different countries, as ‘members of our polio family’.Footnote 80 Going a step further, at the Fifth International Poliomyelitis Conference in 1960 in Copenhagen, Basil O’Connor (who was president of the American National Foundation for Infantile Paralysis) celebrated the achievements of the cooperation in his opening speech:
This is a council, not of war, but of victory. Together we have successfully created weapons against a common enemy that bring within our reach a triumph for all mankind, the coming elimination of epidemic-paralytic poliomyelitis. We meet now to compare notes on what we have created, to report our experiences and help each other in reaching decisions on the most effective use of those weapons. Your very presence here, from the East, from the West, is proof to the world that in your high calling, in search for the truth that frees man from disease, there is no cold war.Footnote 81
This feeling of unity marked the end of a decade in which other domains of public health had been hindered by Cold War tensions. For much of the 1950s, the Soviet Union, along with most Eastern European countries, remained outside the WHO as a sign of protest against the agency’s politics. Since the founding document of the WHO did not permit the unjoining of the agency, the Eastern European countries were termed inactive. The Soviet Union returned to the international agency in 1957 along with Bulgaria, Albania, Poland and Romania.Footnote 82 Other states rejoined later, with Hungary being one of the last countries from the Eastern Bloc to rejoin in 1963.
Although the development of the live vaccine was the result of intensive cooperation that reached across the Iron Curtain, its implementation followed Cold War fault lines. Several major points of conflict emerged, all of which had significant effects on polio prevention in Hungary and worldwide. Convictions and reservations about the efficacy and safety of the Sabin vaccine divided the East and West, while varying healthcare and economic structures had a direct effect on the choice of the vaccine (i.e. to stick with the hitherto-used Salk vaccine or change to Sabin), as well as the speed of introduction and licensing. Furthermore, differences in welfare systems and socialised medicine, a sensitive point in Cold War concerns, influenced the efficiency of vaccine application.
National Mass Vaccination
The introduction of the Sabin vaccine in Hungary in 1959 could not have been more different from that of the Salk vaccine two years before. In the case of the killed-virus vaccine, the state was slow to move in vaccine production. In addition, it faced challenges in its acquisition and ran into significant problems in the vaccination campaigns. Meanwhile, in the introduction and dissemination of the brand-new Sabin vaccine, Hungary was quick to adopt it following field trials and became the first country in the world to organise a nationwide mass vaccination with the oral vaccine. While countries like the Soviet Union and Czechoslovakia had immunized millions of children through their trials, introducing a vaccine in a national programme with the aim of protecting each and every one of a nation’s children was a significant step, regardless of population size.
Shortly after the vaccine trial in Hungary, the national weekly newsreel quickly broke the news about the live poliovirus vaccine and the experiences of children in Győr-Moson-Sopron County.
A new polio vaccine has arrived from the Soviet Union, the Sabin vaccine … Its protective effect is stronger than that of the Salk vaccine … The new vaccine was warmly welcome all throughout Győr county … and will make its way to every part of the country and we hope that with it we will take another step forward in preventing polio.Footnote 83
Barely two weeks after the Hungarian field trials started, the government announced a nationwide vaccination campaign starting in mid-December 1959.Footnote 84 A year later, an estimated 2.4 million children had been immunised with the live vaccine imported from the Soviet Union.Footnote 85
This quick acceptance of the brand-new vaccine in Hungary was very different from the scepticism voiced about the Salk vaccine back in the mid-1950s. In connection with the Cutter incident, a Hungarian newspaper article in 1955 (based on an article in the French newspaper L’Humanité) had argued: ‘The effectiveness of a new vaccine can be established only after a long time and numerous experiments. It is a dramatic fact that due to such negligence many thousands of children became the guinea pigs of the savage protectors of free enterprise.’Footnote 86 Four years, two epidemics and a revolution later, the Hungarian press was not so squeamish about time and the number of experiments. There was a greater need for vaccination that actually worked.
Concern over the safety of the Salk vaccine was ameliorated over the years by the growing number of success stories from Europe and the United States. While knowledge about the rate of efficacy and recommended dosage remained in flux, by 1957 the Hungarian government could rely on a wide-ranging international experience of two years, reported in the pages of medical journals and at international polio conferences.
In the case of the Sabin vaccine, the context could not have been more different. There were no comparable international experiences or clear success stories that could reassure Hungarian scientists and the political leadership. Not one country had begun national mass vaccination in the autumn of 1959, and due to the novelty of the vaccine, there were no long-term observations to determine the percentage of the population who would be protected against the three polio strains. It was just two large-scale trials, albeit involving millions of vaccinees, that provided evidence of the efficacy and safety of the new product.
However, this time the trials were all conducted on home ground, that is to say, on the ‘right’ side of the Iron Curtain. Intensive scientific cooperation among the Eastern European countries and the Soviet Union, fostered greatly during the years of inactive membership of the WHO between 1949 and 1957,Footnote 87 made it possible for Hungarian scientists to keep an eye on live polio vaccine trials in the Eastern Bloc from the very beginning, and to gain direct information about the results from participating scientists on personal visits.Footnote 88
While proximity and the role of the East in the vaccine trials played a large part in the quick adaptation of the Sabin vaccine, these cannot serve as the sole explanations. As the story of the introduction of the Salk vaccine demonstrates, Hungarian scientists had access to onsite visits to manufacturing labs in the West and were participants in the increasingly intensive circulation of scientific knowledge about polio. Also, by the late autumn of 1959, Salk vaccine production in Hungary had already started for the following year.
Moreover, as Hungarian paediatrician Domokos Boda’s memoirFootnote 89 shows, the Cold War divide could have surprising effects: namely, trust in Western and distrust in Eastern technology. Boda was part of the delegation sent to Moscow to investigate the new vaccine and to inform the Hungarian government’s choice between the Salk and Sabin vaccines and saw that enthusiasm over the new Sabin vaccine was not shared by everyone in the Soviet Union. He recounted meeting a group of Soviet virologists on his arrival; they were ardently against the introduction of the new vaccine to the Soviet Union. They argued that the Salk vaccine could be considered safe, since the Americans tested it on their own people. The Sabin vaccine was a solution with which the Americans did not wish to experiment on their own society; therefore, it must be potentially dangerous. As Boda remembered, some even went so far as to consider the introduction of the Sabin25 vaccine part of a scheme by the Americans to destroy millions of Soviet children, cutting future generations short and thereby weakening the nation.Footnote 90 With these sentiments, the Soviet scientists were expressing the general frustrations that often arise with the appearance of new vaccines: the potential to cause disease and harm.
‘My colleagues and I were in a difficult situation,’ Boda wrote. ‘It would be impossible to use the Sabin vaccine in Hungary if the official Soviet view was known. After agonising, we recommended the Sabin vaccine and kept quiet about the controversy.’Footnote 91 The fact that the Sabin vaccine arrived from the East, therefore, cannot alone explain the speedy implementation and fast decision-making of the Hungarian government. A more plausible explanation is that the communist government could not afford another demonstration of the limits of its power by a new epidemic that would be decidedly out of their control. After the summer of 1959, it became clear that Salk vaccination did not fulfil the hopes of curbing polio in the country. The government needed to act fast. To this end, rapidly introducing a new vaccine that promised to eradicate polio seemed the only choice.
There were changes not only compared to 1955, but compared to the previous discourse of the Salk vaccination as well. In this new rhetoric of polio vaccination, the state rehabilitated parents as allies in the fight against polio and appealed to them for cooperation in a very different tone compared to just a few months previously. ‘Certainly there would be no negligent parents who would endanger children to be exposed to illness by missing vaccination,’ wrote Népszava, in a friendlier voice, in its first article informing the public about the upcoming Sabin vaccination.Footnote 92
Parents received a letter along with the details of the vaccinating site and time, explaining that the outbreak that summer was due to the inadequate protection the Salk vaccine provided: ‘in [the] long run the protection yielded by the Salk vaccine did not prove to be satisfactory’, but researchers had ‘finally succeeded in preparing a material of higher protective value’, the Sabin vaccine. The Public Health and Epidemiology Centre also made it clear that the cooperation of parents was essential in bringing polio under control. ‘Every parent’s duty is to protect children from the eventual illness. Make sure to take your child (or send your older ones) on the date fixed for vaccination to the vaccination centres’, the letter instructed.Footnote 93
Official communications in newspapers re-evaluated the state’s role in vaccine procurement. In the case of the Salk vaccine, the government was portrayed as a hero, which, in spite of all hardships and even debt, had managed to go out and attain much-needed protection for children. This time, Father Russia decidedly stole the show: according to daily newspaper Népszava, the Hungarian government ‘asked for the help of the Soviet Union and not without result: we were granted 2.5 million doses of vaccine.’Footnote 94 There was no talk of cost or debt or the achievement of the state required to import the vaccine.
National mass vaccination started on the same day, 14 December 1959, throughout the whole country, and immunisation with each type of virus had to be completed within one week. Type I virus vaccine was distributed from 14 to 19 December 1959, Type III strain from 21 to 27 January 1960 and Type II from 23 to 27 February 1960.Footnote 95 Vaccination with the Sabin vaccine in the form of drops was mandatory for children between three months and two years; for all other age groups up to the age of 14, immunisation was voluntary.Footnote 96 Vaccination was organised in Mother and Infant Protection Offices by district paediatricians. Parents received leaflets informing them about the Sabin vaccine and the campaign, which also served as their registration document. Children were also vaccinated in day-care centres, kindergartens and schools,Footnote 97 which renders the term voluntary dubious.
There were also clear differences in the level of organisation between the Salk and Sabin campaigns. The Ministry of Health seemed to have learnt a lesson from resistance among physicians to the Salk vaccination method, and now took care to inform the medical profession of the vaccination programme well in advance. In November the Ministry of Health organised a conference for the counties’ chief hygienists, the directors and epidemiologists of the Public Health and Epidemiological Stations, and the leading paediatricians of the country, in order to acquaint them with the details of the mass vaccination. Later in the month, similar conferences involved physicians and health experts at the local level.Footnote 98
Notifying the public and disseminating information about the vaccine began well in advance of the campaign. This time, Hungarians could read about the research on the new polio vaccines of Koprowski and Sabin in the newspaper by August 1959,Footnote 99 three months in advance of the campaign, while parents were provided with detailed news about the approaching campaign a month before it started. The above-mentioned news broadcast portrayed the swift and painless vaccination more than a month prior to the start of the national campaign on 14 December 1959. Red Cross and trade union activists, the Communist Youth Association and the Women’s Council all took part in informing the public about the new vaccine, its benefits and its painless application method.Footnote 100 Nor did their activities stop at public education in advance of the campaign. Once vaccinations started, every evening Red Cross activists visited the homes of those who had failed to appear before the vaccination brigades.Footnote 101
The vaccine administration also seemed to have gone more smoothly in the Sabin campaign. The Sabin drops definitely required less technical knowledge to administer than the Salk injections, in terms of administration. The faulty needles addressed in Tóth’s letter were in the past: all that was needed this time was a spoon. Parents were called on to bring their own spoons in order to facilitate the vaccination process.Footnote 102
‘Many of the little ones still get scared of the doctor; but see, no need to be afraid of the horrible needle, because they can take the vaccine against polio with sweet tea’,Footnote 103 news broadcasters soothed the to-be-vaccinated children – and their parents – in advance of the campaign. A ministerial report from 1959 remarked that parents did not usually have a problem with the number of vaccinations: it was the number of injections that kept them away from vaccination.
Of course, in practice, the campaign still had its hiccups. Interestingly, we can identify these problems from a newspaper article titled ‘Sabin vaccination in the capital is progressing in a fast and well-organised manner’.Footnote 104 Many parents failed to bring their vaccination cards, and many had lost their ‘invitation’, the written request by the city council to appear for vaccination. The article also mentions ‘distrustful’ mothers who claimed that their children had a fever in order to avoid having to take the vaccine.
While the organisation of the Sabin vaccination was by far more effective than the previous years’ attempts with the Salk vaccine, the result was well below the expectations of the government. For instance, in Budapest alone, they planned to vaccinate half a million children in three days.Footnote 105 However, they only managed to vaccinate 300,000. According to Népszava, many of the ‘invitations’ did not arrive with families in time because of the high workload of the Hungarian Post with the approach of Christmas and New Year’s Eve. Furthermore, they also blamed the foggy, cold weather for making many children ill with colds, who could not take the vaccine while they had a fever. For these reasons, the city extended the vaccination period by three extra days.Footnote 106
One of the reasons for the quick response to the problem of the low vaccination rate and for the relatively intensive campaign was the particularity of the Sabin vaccine. Although the Sabin drops were easier to administer, their expiration time was significantly shorter than that of the Salk vaccine. Hungary received the shipment frozen, and the vaccine was thawed in the State Institute of Hygiene, where they tested it before distributing it to the vaccination points.Footnote 107 Once the vaccine had been thawed, it needed to be used in the space of about a week.Footnote 108 This small window of usage might explain why the government (the Health Ministry and the SHI) invested such effort into the organisation of the Sabin vaccination.
While the acceptance and application of the vaccine was remarkably fast, the Health Ministry did wish to evaluate the vaccine. For this reason, the minister ordered every hospital director to report any confirmed or potential polio cases and all cases of any contagious disease that attacked the central nervous system, whether accompanied by paralysis or not. These cases were to be reported via telephone to the PHCED as well.Footnote 109
By February 1960, 92.4 per cent of the population under 14 years of age had received immunisation with the Sabin vaccine.Footnote 110 In a matter of three months, Hungary had vaccinated 2.5 million people, more than the total number in two years of Salk vaccination.Footnote 111 The country thus joined the Soviet Union and Czechoslovakia in being among the first countries in the world to organise national mass vaccination with the new, live poliovirus vaccine.
Cold War Fault Lines
Mass vaccination with live polio vaccine quickly spread in Eastern Europe. In Bulgaria in 1960, around 2 million children between 2 months and 14 years of age were targeted;Footnote 112 in Romania in 1961, the vaccine was administered to the whole population under 30 years of age, around 10 million people.Footnote 113 Yugoslavia carried out a small field trial with the Sabin vaccine from January to May 1960, involving about 8,000 pre-school children in the city of Kragujevac, and, following a relatively severe epidemic in 1960, began mass vaccination in 1961.Footnote 114
East Germany conducted a field trial of the Sabin vaccine in April 1960, citing the favourable results of the Soviet Union, Czechoslovakia, Hungary and Poland as the basis for their own trial. The vaccination was free and voluntary, and German virologists reported a very favourable acceptance from the population, with around 86 per cent of people between the ages of 2 months and 20 years immunised. Vaccination with the oral vaccine became compulsory in 1961, reaching 43 per cent of the total population by 1962.Footnote 115 Other European countries started using the live vaccine in the years 1962 and 1963.Footnote 116
The introduction of the Sabin vaccine was peppered with controversies, rivalries and delays in the case of the United States. While it took American authorities an incredible two hours to license the Salk vaccine in 1955,Footnote 117 it took over three years for the United States Public Health Service to do the same for the live vaccine.Footnote 118 The Ad Hoc Committee on Live Poliovirus Vaccines, organised under the Division of Biologics Standards in 1958, repeatedly met until 1962, when Sabin’s vaccine was finally licensed. The deliberations surrounding the live poliovirus vaccine had to do in part with the widespread use of the Salk vaccine, its cultural significance in a society that marched, danced and collected its dimes for research against polio and the all too recent memories of the Cutter incident.
Reservations over the new vaccine also threw light on underlying fault lines in international vaccine research. While cooperation in live vaccine development reached over the Iron Curtain and forged cooperation that was untypical of its time and celebrated as a triumph over political dividing lines, Cold War rhetoric had the upper hand when it came to the evaluation of its results. The words of virologist David Dane from 1959 encapsulate the pervasiveness of Cold War rhetoric in live vaccine development, as he discussed the potential perils of attenuated strains:
It may be that the brain washing which these polioviruses have had in the laboratories of Drs Sabin, Cox and Koprowski have cleansed them of all their potential of indulging in un-American neurotropic activities and that they will remain as stable as the coelacanth. It may be that they will replace all deviationist particles throughout the whole world and we shall all be infected with a common but stable and harmless virus which will occupy and pass peacefully from alimentary tract to alimentary tract for ever more under the auspices of the WHO.Footnote 119
What Dane is referring to here is the growing role of the WHO in coordinating the evaluation and validation of the trials. While the trials were mostly the result of the networks of individual researchers, combined with mostly state funds and ‘volunteer’ subjects, the WHO became an arena in which Cold War tensions could find relief and professional agendas could be pushed through.
Considering the potential harm that live polio vaccines could cause, trust became central to the evaluation of the Eastern European Sabin trials. However, in an era of suspicion of the enemy within and without, trust did not come easily in the Cold War. Therefore the most pressing questions about this Cold War scientific feat, primarily for the Americans, were: could the Russians be trusted? Would their numbers lie? Did the new vaccine actually work?
To resolve the issue of scientific trustworthiness and to bridge Cold War suspicions, the WHO, already highly interested in global disease eradication, sent an American specialist from Yale, Dorothy M. Horstmann, to report on the safety of the vaccine and the validity of the trials in the Soviet Union.Footnote 120 The idea of the visit and the proposal of Horstmann actually came from the United States: John R. Paul, renowned virologist and polio expert at Yale University, recommended his colleague to the Division of Communicable Diseases at the WHOFootnote 121 and to Mikhail Chumakov.Footnote 122 Since 1954, the health agency had established a role for itself in coordinating poliomyelitis research and aiding in the circulation of information in statistics, epidemiology, field trials and laboratory investigation.Footnote 123 It was happy to fulfil the American request for the validation trip.Footnote 124 Its task of scientific evaluation fitted into its self-proclaimed role of bridging the local and global in public health issues.Footnote 125
Between 26 August and 17 October 1959, Horstmann visited Poland, Czechoslovakia and several republics of the Soviet Union to gather information onsite about the vaccine trials. The WHO delegate voiced overall satisfaction in her report on the Soviet Union. She saw no reason to doubt the level of surveillance of polio cases during the trial and judged the Sabin vaccine to be safe. However, Horstmann did admit that it was difficult to say how effective the vaccine was, since many of the subjects had previously received Salk vaccine and little time had elapsed since the trial to draw definite conclusions.
If scepticism about the Russian results was rooted in Western Cold War ideas of the East, Horstmann’s report used a very similar set of tools to dissolve doubts and validate those same results. She drew upon two powerful notions that were connected to communist countries: the centralised, totalitarian state and its submissive citizens.
Horstmann highlighted the role of a centralised and state-operated public health system in successfully organising such a trial: a critical difference between the East and West that was frequently mobilised in Cold War rhetoric on both sides.
The scope and magnitude of the live poliovirus vaccine programmes … are of a type peculiarly fitted to the manner in which the medical profession is organized under the Ministries of Health in these countries. For such mass programmes, it is necessary to have a Medical Service organized almost on a military basis, particularly from the epidemiologic surveillance and Public Health stand point.Footnote 126
In the Soviet case, a state and healthcare system that was centrally controlled from top to bottom could at once be capable of organising a project on a mass scale and, at the same time, of vouching for the rigour and scrutiny that was expected from such a scientific trial. This, implied Horstmann’s report, was the upside of a totalitarian communist regime.
The favourable report was followed by yet another international polio conference, this time specifically on live poliovirus vaccines, in Washington, D.C. One American scientist bluntly confronted the Soviet results, questioning the reliability of their data in the reports of Soviet epidemiological teams.Footnote 127 The Soviet delegate replied shortly: ‘I would like to assure [you] of one thing, that we in the Soviet Union love our children and are as concerned for their well-being as much as people in the United States, or any other part of the world are for their children.’Footnote 128 Thus, polio became the symbol of an equaliser, pointing to the common familial bond, a bond of responsibility between parents and children all over the world. Cold War considerations, however, seemed to be more persistent.
The safety and efficacy of live poliovirus vaccines were fertile grounds for Cold War fears and political considerations. Not only were Sabin’s and Koprowski’s vaccines new, but the whole concept of the live vaccine was novel in disease prevention. The reason for this was the vaccine’s potential to spread the attenuated virus to the non-vaccinated population. Virologists and public-health officials agreed that this was the attractive, and at the same time, dangerous aspect of the new polio vaccines: ‘It is recognized … that the use of a product that spreads beyond those originally vaccinated represents a radical departure from present practices in human preventive medicine.’Footnote 129
New faith had to be created, since the existing faith was in the development of inactivated virus vaccine only. It was also not too easy to bring over to our side the indifferent and the undecided, since my associates and I were alone in this field when the work began and remained so for several years,
Koprowski recalled on the brink of the live vaccine’s success in 1960.Footnote 130 In fact, the problem of creating faith in the attenuated strains remained significant throughout all phases of development, testing, evaluation and implementation of the vaccine. One of the main reasons for concern over the vaccine’s safety was, as Herald Cox pointed out, the difficulty in ‘predict[ing] the behavior of a virus in a human population from what is known about its behavior in the laboratory’.Footnote 131
Following Horstmann’s visit, the WHO took further steps in validating scientific results and establishing trust along the two sides of the Iron Curtain. An expert committee on poliomyelitis, comprised of leading virologists from East and West, compiled a report on the current evaluation of both the Salk and Sabin vaccines.Footnote 132 If the previous report of the committee had given a green light to large field trials and started a wave of vaccine testing all over the globe, the evaluation of those trials was the objective of the next report, published in 1960.
The committee’s report on the whole was favourable, and the majority supported the introduction of live vaccines into national prevention programmes. However, since concerns over safety still persisted in the application of a vaccine that had not been used for a long time, the WHO claimed future roles in continuing to coordinate investigation:
The Committee pointed out that the spread of live-virus vaccine used in large-scale trials within a given country, even though less extensive than had been anticipated, has already caused concern in neighbouring states which were not using the vaccine … It appears, therefore, that there is need for international cooperation in these vaccination programmes between neighbouring states and for coordination in the timing of mass programmes along national borders. The Committee considered that such coordination might best be effected through the WHO.Footnote 133
Thus, it was national concerns that warranted international cooperation. As pathogens did not heed barbed wire, watchtowers and strictly enforced border patrols, the fear of the entry of attenuated viruses provided grounds for coordinated preventive measures across national boundaries.
The history of polio vaccination in Hungary shows that the mutual and rhetorically depoliticised goal of saving children from disability and death opened spaces in domestic and foreign policies on both sides of the Iron Curtain that legitimised actions contradicting contemporary political attitudes and processes. While political agendas and Cold War divisions pervade the story of polio vaccine development, polio prevention on the whole overrode Cold War politics to unite and coordinate efforts. Polio was not seen in the West as a Red virus, nor was it perceived in the East as an imperialist cancer on society or a disease to be ‘contained’. Instead, it brought about the perception of a noble enterprise in an age when millions of children on both sides of the Iron Curtain were threatened by the crippling disease.
At the same time, the accomplishment came to serve as proof of the East’s superiority in caring for its citizens in terms of healthcare and economic systems. Eastern Europeans used the success of the Sabin vaccine to emphasise their cultural, economic and moral superiority over the West, especially the United States, embroiled in its market economy and racial segregation. The prospect of polio elimination, which became associated early on with live poliovirus vaccines, gained particular Cold War political meanings and stakes. The Sabin vaccine was (and still is) at its most potent when applied using this method. Free mass vaccination was a cherished symbol of universal healthcare in which Eastern European countries took pride, but, in some parts of the Western world, it was perceived as the devil itself. As David Oshinsky points out, health officials in the United States connected this system of prevention with socialised medicine, ‘one of the great bugaboos of the Cold War era’.Footnote 134 In this reading, American resistance to widespread use of the Sabin vaccine when it first appeared can partly be traced back to healthcare ideology.
Leading Hungarian virologist Tibor Bakács remembers being puzzled as to why the United States had not switched to the Sabin vaccine, when socialist countries had already done so in 1959. He posed this question to Sabin himself when the professor was visiting the State Hygienic Institute in 1960. According to Bakács’ memoir,
He gave a short, but thought-provoking answer: ‘Sir! In the West vaccine production is mainly in private hands. These have, since 1954, since Salk has discovered his vaccine, been producing that with great capacity. They hoped to gain a huge profit from the production and distribution of this first, partially effective vaccine. Although my vaccine is more efficient, they do not produce it until there are significant Salk-vaccine supplies waiting to be sold. Until these are depleted, they will not start the mass production of the Sabin drops.’ Only socialist countries chose to abandon their existing Salk-vaccine supplies. This is the reason why there were still big epidemics in the rich, Western countries in the 1960s.Footnote 135

While Sabin’s reply was most probably born out of frustration from a decade-long conflict with Jonas Salk and American funding bodies, and Bakács might have interpreted Sabin’s words in a way that conformed to his own sentiments, the success of the Sabin vaccination in Hungary became a recurring example of the superiority of socialism. This narrative was reinforced by the government through newspapers as well.Footnote 136 Seven years after the vaccination began, Vilmos Kapos, director of the Budapest Public Health and Epidemiology Station, still felt it necessary to make a remark on the international significance of the Sabin vaccine in an internal party meeting in 1966:
The social implications of the fight against epidemic diseases are demonstrated by the fact that while in socialist countries the occurrence of polio could be reduced to the minimum with the use of the free and effective Sabin vaccine, the results of capitalist countries, due to economic problems, do not come even close to this.Footnote 137
The Hungarian success in polio vaccination was thus celebrated as the triumph of an entire system of political ideology, welfare and economic structure. It became the ultimate proof of the superiority of communist values and its system.
This ideological role of polio prevention was not unique to Hungary. Czechoslovakian scientists and public health officials chose to emphasise their own contribution to vaccine development and the role of the communist state in the project. Vilém Škovránek, Chief Hygienist, declared the achievement of the Czechoslovakian polio prevention strategy to be an evidence of good government: ‘The success of the mass vaccination was a proof of the highly developed organising abilities of the Czechoslovak Ministry of Health and the profound understanding of our people for health problems. The vaccination campaign was accomplished without any particular troubles and the attendance of the population was very high.’Footnote 138
Sabin vaccination thus became a particularly Eastern European project. It was through collaboration with Soviet, Czechoslovak and Hungarian virologists and public health officials that the vaccine became a powerful tool for polio prevention. As Viktor Zhdanov put it in his concluding remarks to the favourable evaluation of the Soviet field trials with the Sabin vaccine, ‘a feature worthy of comment is the fruitful international cooperation on the problem of the live poliovirus vaccine … on the basis of a wide exchange of scientific information, personal meetings, the exchange of the results of research work and mutual support’.Footnote 139 As an acknowledgement of his work and collaboration with scientists in Hungary, Sabin was offered honorary membership in the Hungarian Academy of Sciences in 1965.Footnote 140
Since the late 1950s, Sabin has been seen as a great friend to the people and politics of Eastern Europe and, subsequently, his Americanness has diminished. The Sabin vaccine has been incorporated into Eastern European identity to the extent that today a number of Hungarians who grew up during the communist era believe that Sabin was in fact Russian.Footnote 141 Sabin himself was very cognisant of his vaccine being the product of international collaboration and the result of a global project, and emphasised the importance of working with colleagues across borders in interviews and talks upon his visit to Hungary in 1960.Footnote 142 He also used the story of his vaccine to champion reconciliation and urge the end of the Cold War in the 1980s with his article, ‘Role of my cooperation with Soviet scientists in the elimination of polio: Possible lessons for relations between the U.S.A. and the U.S.S.R.’.Footnote 143
The Eastern European-ness and the particular Cold War politics that the success of polio vaccination represented contributed to the erasure of this history on the Western side of the Iron Curtain, with a strong influence on current historiography and popular historical narratives. In Western narratives during the Cold War and in current historical analyses, Sabin’s work is addressed mostly through his lifelong conflict and competition with Salk and his vaccine is considered to be undoubtedly American.Footnote 144 The intricate and thorough ways in which the development of the Sabin vaccine was an international project have mostly been written out of its history. Moreover, the Eastern European-ness of the Sabin vaccine disappeared altogether. In the official narrative represented by the Global Polio Eradication Initiative, for instance, it is in 1961 that ‘Dr Albert Sabin develops a ‘live’ oral vaccine against polio (OPV), which rapidly becomes the vaccine of choice for most national immunization programmes in the world’.Footnote 145 By that time, polio epidemics had all but disappeared from several Eastern European countries through official national vaccination campaigns.
Despite the erasure of the Eastern European history of live polio vaccine development, this socialist history should be taken into account when considering twentieth-century epidemics, international and global public health and eradication programmes. Countries like Hungary, Czechoslovakia and the Soviet Union were not only sites of scientific and technological innovation; just as in the West, virological work was embedded in a particular political ideology of what health was, who was responsible for it and how access to it should be distributed. Similarly to the ways in which particular American ideas played a substantive part in the development of and trials with the Salk vaccine, the Sabin vaccine itself is inseparable from the political, social and cultural context in which it was developed and tested in Eastern Europe. As we have seen in previous chapters, political decisions and scientific assessments regarding disease prevention shaped the development and introduction of the Sabin vaccine, and were based on experiences on a very local level. These socialist political and social structures, in turn, had a tremendous effect on the global polio eradication programme of the later twentieth and twenty-first centuries.


 Open access
Open access