


The double burden of malnutrition
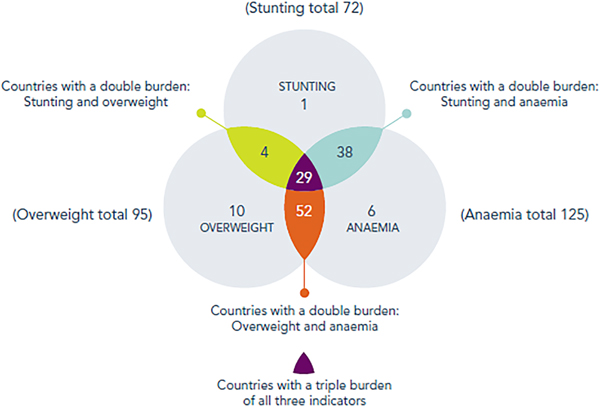
A third of the global population is affected by one or more forms of malnutrition and 88 % of countries face a serious burden of either two or three forms of malnutrition(1) (Fig. 1). These multiple burdens of malnutrition affect both adults and children. Almost two billion adults are overweight or obese, while almost half a billion (462 million) are underweight and over a quarter of a billion (264 million) of women of reproductive age are anaemic(1). With 52 million children aged under 5 years wasted and 155 million stunted, undernutrition is still the dominant form of malnutrition affecting this age group. However, overweight/obesity is also on the rise, affecting about 41 million children aged under 5 years(1). For older children and adolescents (5–19 years), global figures suggest that obesity prevalence (124 million) is catching up with that of underweight (192 million)(2). The nutrition landscape in low- and middle-income countries (LMIC) has therefore become more complex with worldwide obesity rates doubling since 1980(Reference Kelly, Yang and Chen3), while high rates of undernutrition persist(1). This transition to a double burden of malnutrition has been well documented at different scales: from the individual, household, neighbourhood, as well as the national level, therefore representing a pressing public health concern that is increasingly undermining resources allocated to addressing undernutrition.
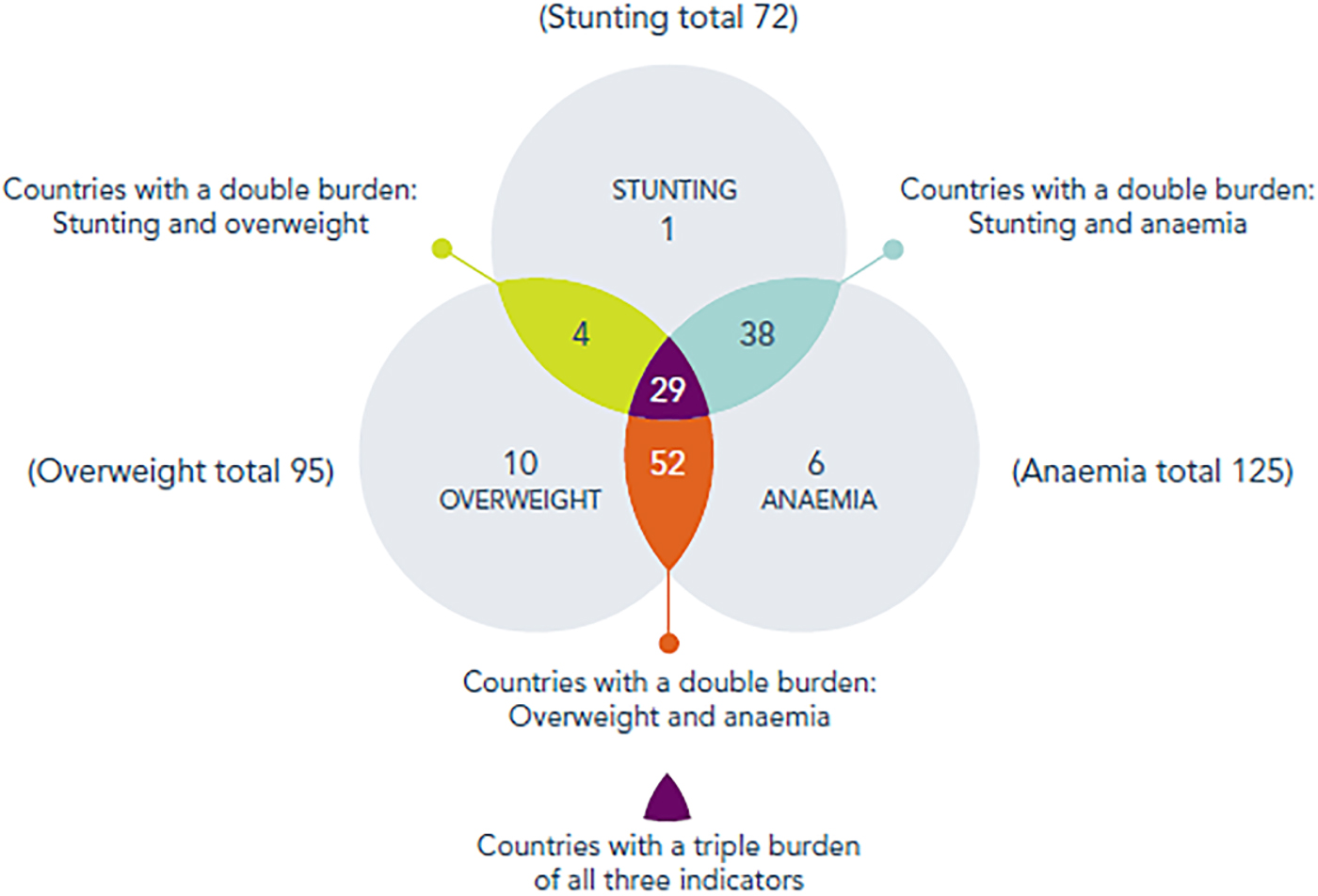
Fig. 1. (Colour online) Number of countries facing burdens of malnutrition.
The need for double-duty actions (interventions and policies)
More recently, there have been calls for double-duty actions that can effectively and simultaneously address multiple goals (i.e. multiple forms of malnutrition)(Reference Hawkes, Demaio and Branca4–Reference Demaio and Branca8). The current lack of integration presents a missed opportunity that hinders optimal utilisation of resources (fiscal, human and time) to tackle multiple forms of malnutrition simultaneously. Global attention has moved from focusing on hunger alone in the millennium development goals, to a broader focus on nutrition and environmental sustainability in the sustainable development goals (SDG), particularly SDG 2 ‘end hunger, achieve food security and improved nutrition and promote sustainable agriculture’, SDG 3 ‘ensure healthy lives and promote wellbeing for all at all ages’, SDG 11 ‘make cities and human settlements inclusive, safe, resilient and sustainable’ and SDG 13 ‘take urgent action to combat climate change and its impact’, thus providing opportunities to link nutrition and environmental sustainability for sustainable development.
The WHO has recently proposed five potential double-duty actions (Table 1): (i) initiatives to promote and protect exclusive breast-feeding (EBF) in the first 6 months, and beyond; (ii) promotion of appropriate early and complementary feeding in infants; (iii) regulations on marketing; (iv) maternal nutrition and antenatal care programmes; and (v) school food policies and programmes(7). Their proposed mechanisms for their impact on the different forms of malnutrition are described in Table 1. However, the proposed double-duty actions that are likely to have the greatest reach in preventing the double burden of malnutrition remains unknown. This requires identification of shared drivers influencing all forms of malnutrition and prioritising double-duty actions that address the maximum number of drivers with positive impact on both malnutrition and environmental sustainability. Therefore, the aim of the present paper was to identify shared drivers for multiple forms of malnutrition, to assess which double-duty actions are likely to have the greatest reach in preventing and addressing the double burden of malnutrition, in the context of the SDG agenda.
Table 1. Potential candidates for achieving double duty
NCD, non-communicable disease.
Source: WHO(7).
Identifying and categorising the shared drivers of the double burden of malnutrition
Existing conceptual frameworks relating to undernutrition(9–Reference Herforth and Harris11) and obesity(12), and the non-communicable disease (NCD) global monitoring framework(13) were reviewed (Supplementary Materials 1–5). These conceptual frameworks are internationally recognised and have been used extensively in the field of nutrition. Based on the different conceptual frameworks, drivers of undernutrition and obesity identified in the frameworks were listed separately. Drivers that influence both forms of malnutrition: (i) in the same direction; (ii) through either direct or indirect pathways; and (iii) immediately or later in life were considered as shared. For example, EBF prevents undernutrition (e.g. wasting, stunting and micronutrient deficiency) in early infancy(Reference Rollins, Bhandari and Hajeebhoy14), but also prevents obesity and nutrition-related NCD in later life(Reference Victora, Bahl and Barros15, 16). Conversely, consumption of energy-dense, nutrient-poor diets in the context of urban LMIC could lead to excessive weight gain while simultaneously contributing to micronutrient deficiencies. Finally, in the context of LMIC, food safety constitutes a shared driver for both forms of malnutrition. For example, consumption of unsafe foods and water contributes to the high diarrhoeal burden in LMIC. Actions taken to avoid such contamination could lead to a preference for soft drinks over water, for highly processed foods over freshly prepared ones, particularly in urban areas where the availability of these products is high. Such shifts in dietary choices can predispose individuals and communities to a dietary pattern associated with increased risk of overweight/obesity and NCD.
Drivers mentioned in only one of the frameworks but where evidence suggested they impact on other forms of malnutrition were included. Additional factors that were absent from the frameworks and for which evidence exist were added (e.g. high-sugar, nutrient-poor foods, ultra-processed foods(Reference Kant17–Reference Silva, Giatti and de Figueiredo23), food environment(Reference Herforth and Ahmed24, Reference Cobb, Appel and Franco25), supermarket growth(Reference Demmler, Ecker and Qaim26), street vendors, food eaten away from home(Reference Cunha, Bezerra and Pereira27, Reference Popkin and Reardon28), literacy(Reference Madjdian, Azupogo and Osendarp29), urban residency(Reference Hawkes, Harris and Gillespie30), microbiome(Reference Hartstra, Bouter and Bäckhed31, Reference Million, Diallo and Raoult32)). The final list of shared drivers was reviewed by the authors and drivers for which consensus was reached that they are shared were maintained, and in some cases, the terminologies were harmonised.
Using the validated DONE framework of determinants of nutrition and eating(Reference Stok, Hoffmann and Volkert33), the identified shared drivers were categorised using a socio-ecological approach into four main levels: individual, interpersonal, environmental and policy(Reference Stok, Hoffmann and Volkert33). A socio-ecological approach is useful for developing future interventions and policies as it accounts for the environments in which people live(Reference Story, Kaphingst and Robinson-O'Brien34). The DONE framework was chosen for categorising the shared drivers because of its rigorous external validation involving a multi-Delphi process by international experts. The DONE framework categorises determinants (drivers) into four main levels (individual, interpersonal, environment and policy), twelve stem categories (biological, demographic, psychological, situational, social, cultural, product, micro, meso/macro, industry, services/infrastructure, government) and fifty-one leaf categories (e.g. socioeconomic status, cultural behaviours, eating environment). Some adaptations were made to the model to include dietary intake as a relevant stem category.
Assessing the contribution of the shared drivers to environmental sustainability
Existing conceptual frameworks relating to environmental sustainability were reviewed(Reference Holdsworth and Bricas35) (Supplementary Materials 6–7) to select which shared drivers from our pre-defined list proposed in the adapted DONE framework would be sensitive to influencing environmental sustainability. Several other sources of evidence were used to develop the list of environmentally sensitive drivers: food variety, dietary diversity, food availability and access, purchasing power, supermarket growth(Reference Jones, Hoey and Blesh36); convenience, food away from home, grazing(Reference Jackson and Viehoff37); street vendors(Reference Ekanem38); medicine use(Reference Thomas and Depledge39) and TV watching(Reference Michaelowa and Dransfeld40). When assessing the potential relationship between the shared drivers and environmental sustainability, both direct and indirect pathways (e.g. acting through malnutrition) were considered.
Mapping of recommended interventions and their link with shared drivers
The five double-duty actions proposed by the WHO (Table 1) were linked with the list of identified shared drivers of malnutrition. For each policy action, drivers were extensively reviewed and those that could be addressed by the suggested policies were highlighted. This was based on extensive discussion among the co-authors and review of existing available literature. A list of addressed and unaddressed drivers was then compiled for each policy. Shared drivers that were likely candidates for having an impact on environmental sustainability were also linked to the five double-duty actions, to assess the extent to which the proposed set of double-duty actions could address both malnutrition and environmental sustainability simultaneously.
Identification of unaddressed shared drivers and suggestions for additional de novo policy actions
The list of unaddressed drivers was reviewed to propose modifications of current actions or suggestions of new double-duty actions (i.e. de novo actions) that could address them. Proven and recommended interventions for overweight/obesity and nutrition-related NCD(41, Reference Swinburn, Vandevijvere and Kraak42) and undernutrition(Reference Bhutta, Das and Rizvi43, Reference Ruel, Alderman and Maternal44) were considered and chosen actions were grouped into broader policy actions, in line with the SDG.
Review of existing frameworks and identification of shared drivers of the double burden of malnutrition and environmental sustainability
Drivers have been conceptualised differently for the two forms of malnutrition (undernutrition and obesity), using different terminologies and categorisation, which may have previously hindered the development of an integrated conceptual framework guiding efforts to prioritise interventions that address both forms of malnutrition simultaneously. Those specialising in undernutrition have mainly adopted a socio-ecological approach to represent drivers, while those specialising in obesity have used both socio-ecological and systems approaches. A significant proportion of the drivers of obesity and undernutrition are shared (eighty-three of the 207), with forty-four (53·0 %), twelve (14·5 %), twenty-three (27·7 %) and four (4·8 %) of these drivers at the individual, interpersonal, environment and policy levels, respectively (Fig. 2).
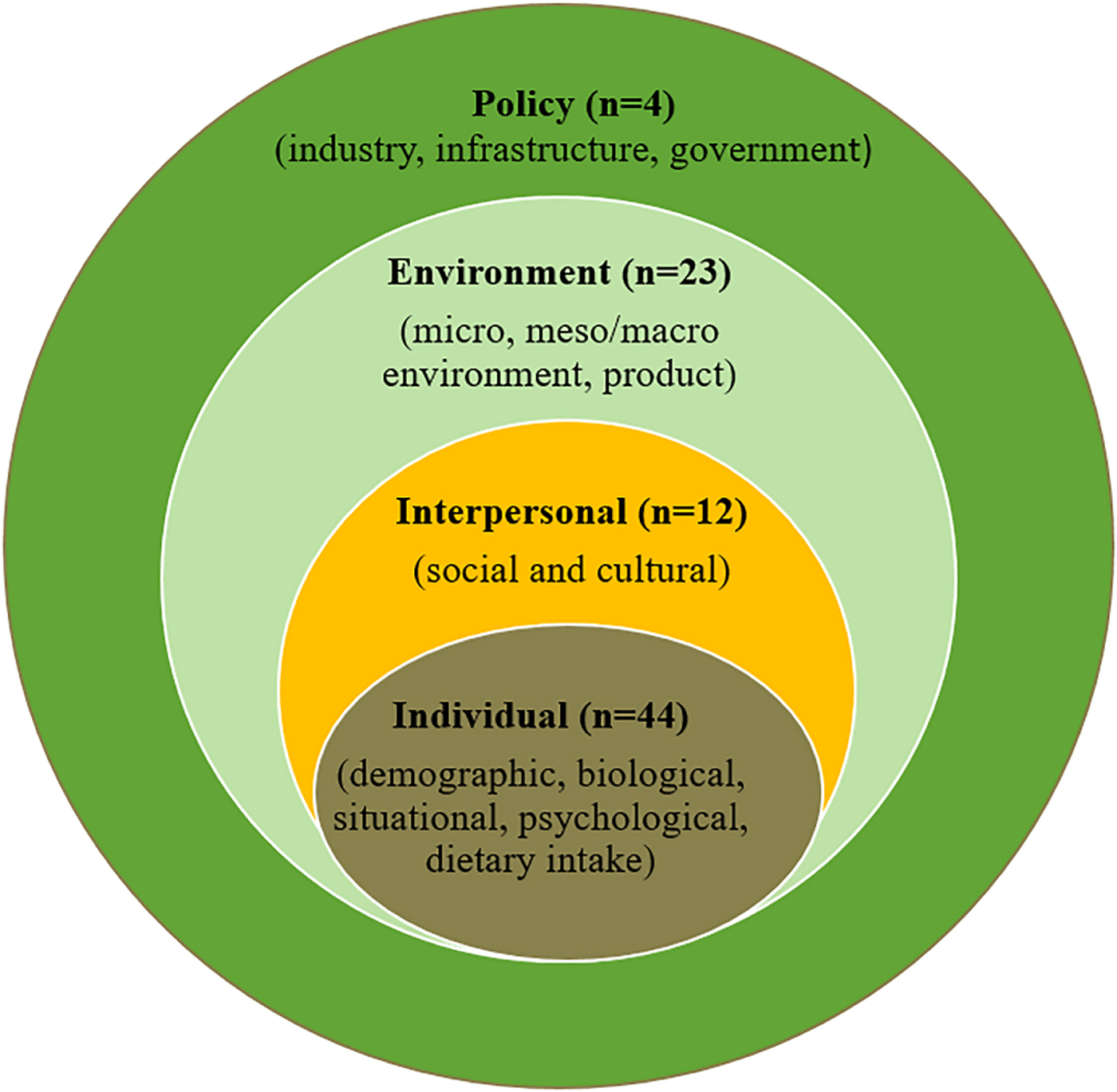
Fig. 2. (Colour online) Summary of the shared drivers of the double burden of malnutrition across socio-ecological levels.
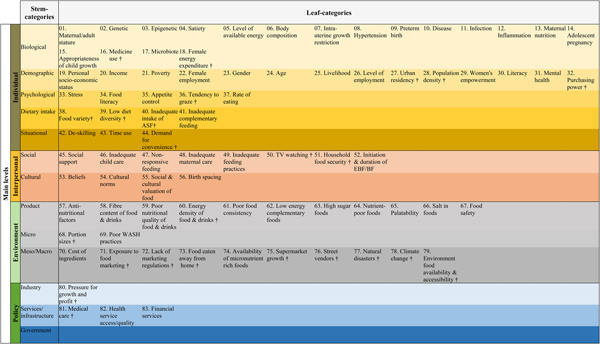
Most of the shared drivers at the individual level can be classified as biological (e.g. intra-uterine growth restriction, hypertension, preterm birth, diseases, maternal nutrition and appropriateness of child growth). Drivers at the interpersonal level were mostly classified as social (e.g. inadequate child and maternal care, initiation/duration of (exclusive) breast-feeding, inadequate feeding). Most of the shared drivers at the environment level address product-related factors (e.g. energy density of food and drinks, low nutrient-density foods/drinks, high-sugar foods) or meso-/macro-level factors (e.g. environment food availability and accessibility, climate change, lack of marketing regulations); whereas, policy-level drivers mainly relate to services and infrastructure (e.g. medical care, health service access and quality, financial services) and industry (e.g. pressure for growth and profit). A detailed list of the drivers at each level of the socio-ecological model is provided in Fig. 3.
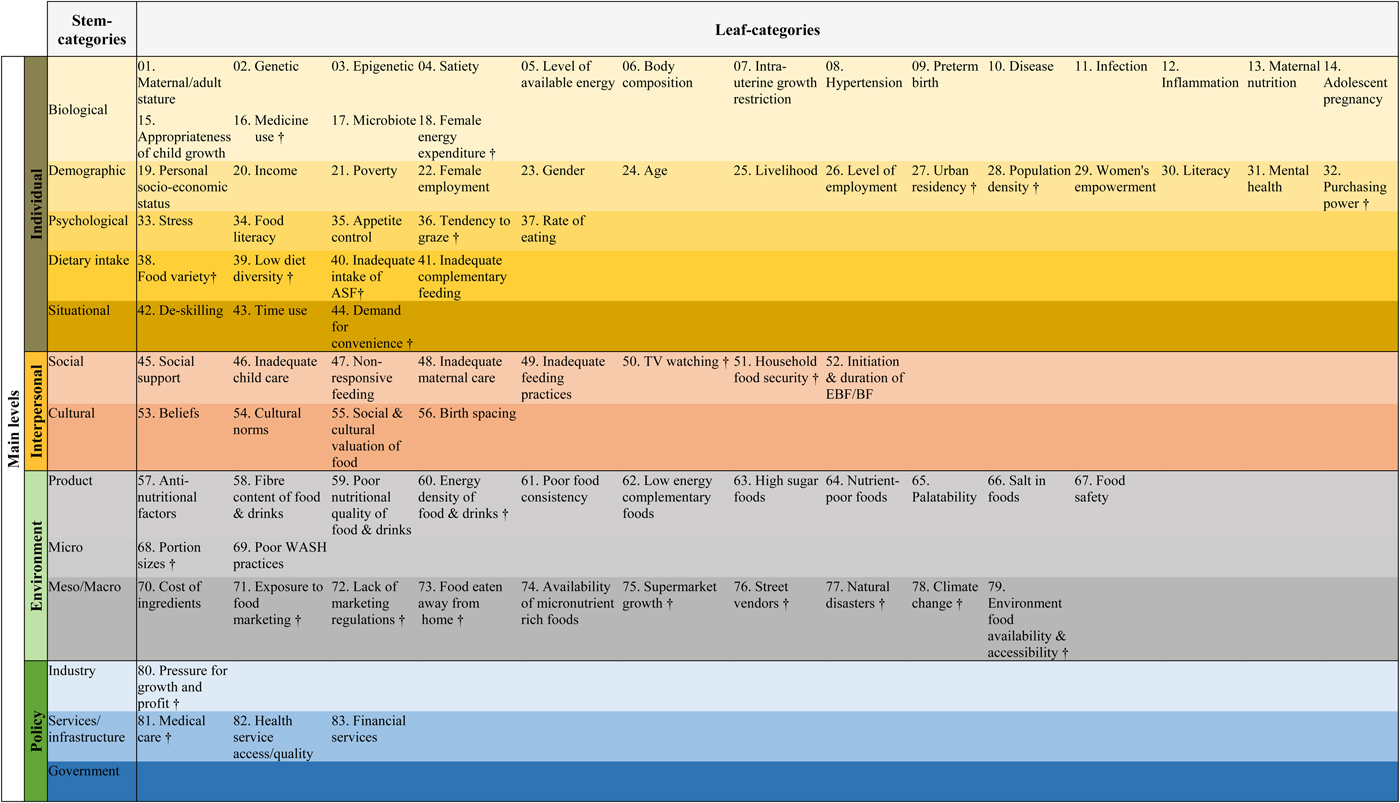
Fig. 3. (Colour online) Shared drivers of the double burden of malnutrition. Source: Adapted from Stock et al. (2017). The DONE framework: Creation, evaluation, and updating of an interdisciplinary, dynamic framework 2.0 of determinants of nutrition and eating. PLoS One.12(2):e0171077. ASF, animal source foods; EBF, exclusive breastfeeding; BF, breastfeeding; WASH, water, sanitation and hygiene; †, environmental sensitive drivers.
Drivers can have effects on both forms of malnutrition through direct (e.g. inappropriate complementary feeding) or indirect (e.g. maternal time use) pathways. Maternal time use influences caring and feeding practices, which in turn could lead to one or more forms of malnutrition. Unlike in the afore-mentioned examples, the effects of some drivers, such as intra-uterine growth restriction or preterm birth, may not necessarily be immediate. For instance, intra-uterine growth restriction would impact on growth in the first few years of life (likely to influence stunting levels)(Reference Christian, Lee and Donahue Angel45), but could also impact on overweight/obesity and nutrition-related NCD in later life(Reference Oken and Gillman46, Reference Crume, Scherzinger and Stamm47). A deeper understanding of the different ways that the shared drivers operate would provide a unique opportunity for interventions to address malnutrition across the spectrum more sustainably.
The review of existing environmental sustainability frameworks identified twenty-four of the eighty-three shared drivers (28·9 %) that could be potential candidates for having an impact on environmental sustainability (n 10 at the individual level (e.g. demand for convenience, excess intake of animal source foods); n 2 at the interpersonal level (food watching and food security); n 10 at the environment level (e.g. portion sizes, energy density of foods and drinks, natural disasters, climate change) and n 2 at the policy level (pressure for growth and profit and medical care); Fig. 3).
Review of WHO double-duty actions with identified shared drivers of the double burden of malnutrition
The double-duty actions proposed by the WHO addressed a significant number of the drivers, but not all (Table 2). ‘Regulations on marketing’ addressed the highest proportion of shared drivers (65·1 %) followed by ‘promotion of appropriate early and complementary feeding in infants’ (53·0 %), ‘maternal nutrition and antenatal care programmes’ (43·4 %), ‘school food programmes and policies (41·0 %) and ‘initiatives to promote and protect EBF in the first 6 months, and beyond’ (28·9 %). The actions addressed mostly individual- and interpersonal-level drivers. Little emphasis was given to women's empowerment as it was only partly addressed by the policy on ‘maternal nutrition and antenatal care programmes’. Policy-level drivers were seldom targeted by the proposed actions, which focused mainly on the individual level.
Table 2. Summary table of the double-duty actions and their likely impact on the double burden of malnutrition and environmental sustainability
Source of images: WHO(7).
EBF, exclusive breastfeeding; NCD, non-communicable diseases; BF, breast-feeding; SES, socio-economic status; WASH, water, sanitation and hygiene; ASF, animal source foods; WRA, women of reproductive age; ANC, antenatal care; †environmental-sensitive drivers.
About 10 % of the shared drivers: short maternal/adult stature, epigenetic, level of available energy, body composition, disease, infection, inflammation and inadequate feeding practices were addressed by all five policies. However, a quarter of the shared drivers (n 12 at the individual level, n 4 at the interpersonal level, n 3 at the environment level and n 2 at the policy level) remained unaddressed. Among the unaddressed drivers, some were non-modifiable (e.g. genetic, age, sex and natural disasters), while others were only modifiable to a lesser extent (e.g. adolescent pregnancy, medicine use, livelihood, urban residency, population density, literacy, mental health, stress, time use, social support, TV watching, beliefs, cultural norms, cost of ingredients, supermarket growth, health service/access quality, financial services).
Environmental sustainability of the double-duty actions
Eight of these drivers were targeted by at least three of the double-duty actions (tendency to graze, food variety, low dietary diversity, inadequate/excess of animal source foods, energy density of foods and drinks, portion sizes, climate change and female energy expenditure). Four of these drivers were targeted by two of the double-duty actions (food security, exposure to food marketing, pressure for growth and profit; and environment food availability and accessibility). Twelve of these drivers were targeted by either one double-duty action (lack of marketing regulations, purchasing power, demand for convenience, food eaten away from home, street vendors and medical care) or none (medicine use, urban residency, population density, TV watching, supermarket growth and natural disasters). In their existing forms, the highest number of environmental sustainability sensitive drivers were targeted by ‘regulations on marketing’ (15/24 environmentally sensitive drivers) and ‘school food programmes and policies’ (11/24), which suggests that these actions need to be prioritised (Table 2).
Suggestions for modifications of existing WHO double-duty actions
Some of the unaddressed modifiable shared drivers could be addressed by introducing slight modifications to the existing WHO double-duty actions. For example, to effectively implement the policy on ‘EBF in the first 6 months, and beyond’, it is critical to ensure paid maternity leave for at least 6 months to allow women to have time to provide appropriate care for their offspring and themselves (Table 2). The ‘regulations on marketing’ policy needs to be expanded to include adolescent girls and women of reproductive age and move away from the sole focus on infants and younger children. In addition to marketing regulation of breastmilk substitutes, other foods such as energy-dense and nutrient-poor foods need to be defined and targeted. Marketing regulations along with food pricing policies (e.g. taxes and subsidies) could be leveraged to make healthier diets (both in terms of safety and nutrition) affordable and accessible. Our synthesis suggests that the policy on ‘maternal nutrition and antenatal care programmes’ could be expanded to target women of reproductive age both in pre- and post-pregnancy periods and widen the focus from nutrition to overall health. Women's empowerment, reproductive health, mental health, water, sanitation and hygiene practices as well as the prevention of substance abuse should be core actions. The impact of the ‘school food programmes and policies’ could be maximised by acknowledging the importance of a safe and nutritious food environment within and around schools.
Suggestions for de novo policy actions
Two additional double-duty actions are proposed in an attempt to address the remaining unaddressed drivers that were deemed modifiable (i.e. adolescent pregnancy, livelihood, urban residency, population density, literacy, mental health, stress, time use, social support and health service/access quality). Other drivers were either unmodifiable (i.e. genetic, sex, age and natural disasters) or less easy to modify (i.e. TV watching, medicine use, beliefs, cultural norms, cost of ingredients, supermarket growth and financial services) and were therefore not prioritised when identifying possible de novo actions.
The first de novo action we propose could focus on improving urban settlements for improved access to safe water, sanitation and hygiene and appropriate living conditions. This has the potential to address drivers such as poor urban residency and high population density. The second action could develop or strengthen social support systems (e.g. social protection schemes) which would, in turn, help to address drivers such as education/literacy, adolescent pregnancy, poor mental health, time use, livelihood, access to health services and stress (Table 2). Some of the previously proposed amendments to the actions on ‘EBF in the first 6 months, and beyond’ and ‘maternal nutrition and antenatal care programmes’ would also further tackle drivers such as mental health, adolescent pregnancy, time use and stress. The existing and de novo double-duty actions could catalyse the achievement of several SDG including those that are not directly related to nutrition, for example, SDG 2 ‘end hunger, achieve food security and improved nutrition and promote sustainable agriculture’, SDG 3 ‘ensure healthy lives and promote wellbeing for all at all ages’, SDG 11 ‘make cities and human settlement inclusive, safe, resilient and sustainable’ and SDG 13 ‘take urgent action to combat climate change and its impact’.
Conclusions
The nutrition landscape in LMIC is becoming more complex, with multiple forms of malnutrition (the double burden) co-existing; obesity prevalence has escalated, while all forms of undernutrition persist throughout the life course. However, most interventions and policies address only one form of malnutrition, so there is a need for double-duty actions to address this growing double burden of malnutrition more effectively, since policy-makers have limited resources. Identifying shared drivers of the double burden of malnutrition is a first step towards effective interventions that simultaneously address the double burden of malnutrition (double-duty actions). The present paper identified the shared drivers for multiple forms of malnutrition, to assess which double-duty actions are likely to have the greatest reach in preventing the double burden of malnutrition, in the context of sustainable development. A significant proportion of the drivers of obesity and undernutrition are shared (approximately 40·0 %), but the use of different terminologies and concepts to describe them may have previously hindered the development of an integrated conceptual framework guiding efforts to prioritise interventions that address both forms of malnutrition simultaneously. Using a common language is thus critical to clearly understand actions proposed across areas of activity to ensure sustainable and effective implementation of double-duty actions. Linking the five double-duty actions proposed by the WHO to the shared drivers that we have identified showed that actions with the most benefit for nutrition and environmental sustainability are: regulations on marketing, promotion of appropriate early and complementary feeding in infants and maternal nutrition and antenatal care programmes. These actions therefore need to be prioritised.
Substantially more drivers could be addressed with minor modifications of the WHO double-duty actions and the addition of the two proposed de novo double-duty actions: (i) improving settlements for improved access to safe water, sanitation and hygiene and appropriate living conditions; and (ii) developing and strengthening social support systems. Effective implementation of the double-duty actions requires recognition that they are interconnected and that they do not necessarily operate at the same levels (i.e. individual, household, community, societal).
Future research
Prioritisation of the suggested double-duty actions is critical within each country and region, using epidemiological evidence. Data on effectiveness (effect size, cost-benefit analyses) and consideration of trade-offs and tensions between action are needed. Further research on the impact of these actions on environmental sustainability is also required, including empirical data from different LMIC to ensure that evidence is culturally appropriate to the context(Reference Jones, Hoey and Blesh36).
A paradigm shift in the way research is conducted and financed is needed to catalyse progress in addressing both forms of malnutrition simultaneously. Research should encourage the use of indicators that capture and assess both forms of malnutrition within the same study and evaluate the effectiveness of actions on both forms of malnutrition. To this end, the proposed shared drivers could help integrate the two artificially separated nutrition specialities of undernutrition and obesity.
A single evidence-based and validated conceptual framework integrating shared drivers of both forms of malnutrition is needed to guide programmes, actions and policies. This evaluation is one step to developing such a framework so that integrated efforts can be developed to leverage the increased attention given to nutrition. The validation process should use rigorous methods, such as the best fit framework approach(Reference Booth and Carroll48) and consult with an interdisciplinary panel of experts. Failure to tackle both forms of malnutrition will compromise the achievement of the SDG given that nutrition is both an input and output of many of the SDG.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0029665118002616
Financial Support
R. P. received a research stimulation prize from the School of Health and Related Research, University of Sheffield for travel to Addis Ababa University, and for K. B. to travel to the University of Sheffield, to work on the present paper.
Conflict of Interest
None.
Authorship
The authors had joint responsibility for all aspects of preparation of this paper.






 Open access
Open access