



Introduction
China is not only the fastest ageing country in the world, but also the country with the largest number of older people (Hu and Ma, Reference Hu and Ma2018; Chen et al., Reference Chen, Fu and Chang2022). At the end of 2020, the number of people aged 60 years and older reached 264 million and accounted for 18.7 per cent of the total population in China (China National Bureau of Statistics, 2021). Among them, the total number of disabled older adults was over 40.63 million in 2016 and is expected to reach 61.68 million by 2030 and 97.50 million by 2050 (China National Commission on Ageing, 2016). This dramatic increase in the size of the disabled older population will put significant pressure on population health and the health system (Lakomý, Reference Lakomý2020). The leading policy response to these trends in China has been ‘health ageing’ which is a process to optimise opportunities to advance life satisfaction for older individuals, especially disabled older persons (Wu et al., Reference Wu, Newman, Dong and Odden2018), with the goal of simultaneously prolonging life, promoting health and improving the quality of life (World Health Organization, 2015).
Long-term care has been shown to be crucial for older persons to maintain their activities of daily living (Fernández-Ballesteros et al., Reference Fernández-Ballesteros, Dolores Zamarrón and Ruíz2001; Lakomý, Reference Lakomý2020) and to improve their life satisfaction (Wilson, Reference Wilson2012; Falkingham et al., Reference Falkingham, Evandrou, Qin and Vlachantoni2020). Globally, care given to older adults can take many forms. The two most common types are informal care provided by family members or other relatives within families and formal care provided by private institutions and social care systems, with each impacting life satisfaction through different ways (Jacobs et al., Reference Jacobs, Van Tilburg, Groenewegen and Broese Van Groenou2016). Informal care has been shown to reduce negative emotions, such as loneliness and unhappiness, given that it is provided by close family members or friends with whom disabled older persons have close emotional ties (Lakomý, Reference Lakomý2020). Generally, the older adults reach a higher level of life satisfaction if they can stay in their familiar environment which facilitates social interactions: their self-identity and self-esteem can be maintained (Bonsang, Reference Bonsang2009; Kim et al., Reference Kim, Kim, Malonebeach and Han2015). However, for disabled older adults, professional formal care may be more likely to improve their life satisfaction through the enhancement of their physical functions (Verbakel, Reference Verbakel2017). Hence, the findings of older persons may lack generalisability to disabled older adults. Although many scholars found long-term care services impacted older adults’ life satisfaction, few studies explored and compared the effects of the two care forms on life satisfaction among older persons, and even fewer focused on disabled older care recipients (Liu and Zhang, Reference Liu and Zhang2017).
In China, there are three main types of long-term care services for older adults: family-based care, community-based care and institutional care. Informal care provided by family members in the home is the primary source of support for disabled older adults in China (Zhou and Walker, Reference Zhou and Walker2016). Around 85, 10 and 5 per cent of disabled older persons received family-based, institutionally based and community-based care, respectively (Su et al., Reference Su, Peng and Chen2015; Liu and Zhang, Reference Liu and Zhang2018). Influenced by the cultural tradition of filial piety in the Confucian doctrine (Zhan and Montgomery, Reference Zhan and Montgomery2003; Falkingham et al., Reference Falkingham, Evandrou, Qin and Vlachantoni2020), Chinese older people prefer being cared for at home and by their family members, as they believe this offers a higher degree of emotional satisfaction and spiritual comfort (Yan, Reference Yan2018; Zhang and Fu, Reference Zhang and Fu2021). However, changes to the nuclear family and rapid urbanisation have weakened the role of informal care (Chen et al., Reference Chen, Fan and Chu2020). Because informal care alone is insufficient to meet the rising demand for long-term care, the Chinese government has proposed the establishment of an integrated long-term care system where the responsibility for care provision is shared by the family, the private sector and the public sector. The development of this system is challenged by the COVID-19 pandemic. The COVID-19 emergency blocks social interaction, increases the informal care need, while limiting delivery of informal care due to the prevention rules (Cipolletta et al., Reference Cipolletta, Morandini and Tomaino2023). To date, the government has not offered guidance on the relative role to be played by informal and formal care (Feng et al., Reference Feng, Glinskaya, Chen, Gong, Qiu, Xu and Yip2020; Maags, Reference Maags2020).
A better understanding of the contribution of formal and informal care to life satisfaction is of critical significance to policy decision making, especially in the context of the COVID-19 pandemic, and is therefore the motivation for our work. In spite of the increasing number of disabled older adults and the importance of their life satisfaction, information on how to increase their life satisfaction and advance health-related benefits through long-term care is scant. The purpose of our study is to rectify this informational shortcoming in the research literature. The study highlights the effects of various care types using panel data from the 2011–2018 China Health and Retirement Longitudinal Survey (CHARLS). We explore the different effects depending on the degree of disability, sex and area of residence. We further examine the mechanisms through which the two types of care impact life satisfaction. The findings are of direct relevance for policy makers and practitioners in China concerned with the provision of long-term care to its ageing population.
Data and methods
Data
This study used a nationwide panel dataset from the CHARLS. This survey examined the Chinese population aged 45 years and older based on multistage random probability sampling (Zhao et al., Reference Zhao, Hu, Smith, Strauss and Yang2014). The baseline survey was conducted in 2011 and it was followed up every two years. To date, four waves of this survey (2011, 2013, 2015 and 2018) have been conducted, comprising 17,500 individuals in 150 counties/districts and 450 villages/resident committees in 28 provinces across China. These areas are representative of China and vary substantially in geography, economic development and health indicators. The survey presents a rich array of information about disabled adults, including detailed information on their demographics, socio-economic status and life satisfaction.
The original sample consisted of respondents aged 60 years and above, and only disabled older persons were included in our study. Older adults who had one or more activities of daily living (ADLs; including dressing, bathing, eating, getting in and out of bed, and toileting) or at least one instrumental activity of daily living (IADL; including shopping, preparing meals, doing housework, making phone calls, managing money and taking medicine) limitations were identified as disabled (Pezzin et al., Reference Pezzin, Pollak and Schone2009; Paraponaris et al., Reference Paraponaris, Davin and Verger2012). To take advantage of the sample information, we obtained a final unbalanced panel dataset comprising a total of 8,453 observations after omitting observations with missing values, where 1,475, 2,066, 2,391 and 2,521 samples were derived from 2011, 2013, 2015 and 2018, respectively.
Measures
The dependent variable was life satisfaction, which was taken from answers to the question ‘How satisfied were you with life as a whole?’ The response options were: 1 = not at all satisfied, 2 = not very satisfied, 3 = somewhat satisfied, 4 = very satisfied and 5 = completely satisfied. The self-rated life satisfaction is a valid and reliable measurement of life satisfaction status (Huang et al., Reference Huang, Lian and Li2016).
Care type was included as a dummy independent variable (1 = informal care, 0 = formal care). Respondents from CHARLS reported whether they had received assistance with ADLs or IADLs, and noted the care-givers who provided such assistance and where the care assistance was provided. In our research, care provided by a care recipient's spouse, adult children (including children-in-law) or other relatives in the family was identified as informal care, while care provided by a paid professional helper in a nursing home, hospital or other residential care facility fell into the scope of formal care.
Different care types can impact individual life satisfaction through various channels (Yan et al., Reference Yan, Su, Zhu and He2012; Verbakel, Reference Verbakel2017). We focused on three mediators, i.e. emotions, social activities and physical health in the mechanism analysis. We measured emotions by two questions: ‘How often did you feel happy during the last week?’ and ‘How often did you feel not lonely during the last week?’ All responses were rated on a three-point Likert scale ranging from 0 (rarely or none of the time) to 2 (most or all the time), and the sum score ranges from 0 to 4, with higher scores indicating a greater degree of positive emotions. Social activity was measured by monthly frequency of interacting with friends or visiting community clubs. Responses were rated on a three-point Likert scale ranging from 0 (rarely or none of the time) to 2 (most or all the time), and the sum score ranges from 0 to 4. The physical health status item consists of asking respondents to rate their health status as poor, fair or good.
We also included various covariates that have been shown in the literature to be determinants of life satisfaction, including (a) demographic characteristics including age and gender; (b) socio-economic characteristics including marital status, educational attainment and whether enrolled in health insurance or pension insurance; (c) health status and behaviours including number of chronic diseases, smoking status and alcohol consumption; and (d) household variables including residential types, whether having housing tenure, number of children and annual household income. We used the natural logarithm of the household income to account for right skewness. Variable definitions are listed in Table 1.
Table 1. Variable definition

Statistical analyses
We compared life satisfaction for disabled older persons who received informal care with those who received formal care. Research investigating the effects of care types on life satisfaction suffers from problems of selection bias. Also, the estimation of the effects may be biased due to unobserved heterogeneity, such as innate personality or attitude towards life (Kim et al., Reference Kim, Kim, Malonebeach and Han2015). Therefore, we used a fixed effects model along with propensity score matching (PSM) to address the issue of potential selection bias and missing variables simultaneously.
When matching, the propensity score was calculated using a logit regression analysis. We employed the Epanechnikov kernel matching method with a bandwidth of 0.006 to take advantage of the data and minimise the estimation bias (Imbens and Wooldridge, Reference Imbens and Wooldridge2009). Once the problem of selection bias was solved through PSM, we constructed the fixed effects model together with kernel matching to control for unobserved individual heterogeneity. Although the ordered logit model is widely used for categorical ordered dependent variables, it fails to provide estimates of some important statistics of interest, such as the partial effects of covariates (Wooldridge, Reference Wooldridge2002; Niimi, Reference Niimi2016). Thus, we employed linear regressions with fixed effects and allow for the estimation of the partial effects. The model is formalised as:

where LSit is the life satisfaction for individual i at time t, adjusted with the weight derived from the kernel matching method; Caretypesit denotes the care types, including informal and formal care; Xit represents a vector of individual i's observable characteristics at time t; μi represents the unobserved fixed effects; and ɛit is the random error. The coefficient β 1 is our primary interest, i.e. the effects of care types on life satisfaction. We used robust standard estimators to adjust for potential heteroscedasticity and serial correlation (Stock and Watson, Reference Stock and Watson2008). We also constructed the ordered logit model with PSM to verify the robustness of our findings.
We further examined the mechanisms through the use of a mediation model. In particular, we first explored the effects of care types on mediators, and then added the three mediators in the model. Statistical mediating effects were demonstrated by a fall in or loss of significance in coefficients on the care types for life satisfaction when controlling for mediators (Baron and Kenny, Reference Baron and Kenny1986; Fan et al., Reference Fan, Yan, Liu, Cai and Coyte2021). We considered emotions, social activity participation and physical health as possible mediators through which life satisfaction might be affected.
Results
Statistical description
Table 2 presents the descriptive statistics of our research sample. The disabled older persons who received informal care were found to have higher life satisfaction compared with those who received formal care. There were approximately 78.03 per cent who received informal care, and around 26.36 per cent of disabled older persons transferred from one care type to another during the research period. The disabled older persons receiving informal care tended to be older, drink alcohol and have more children. In contrast, the sampled disabled older persons who received formal care were more likely to be healthier, enrol in health or pension insurance, own their home, have a higher educational level and have a higher household income.
Table 2. Descriptive statistics
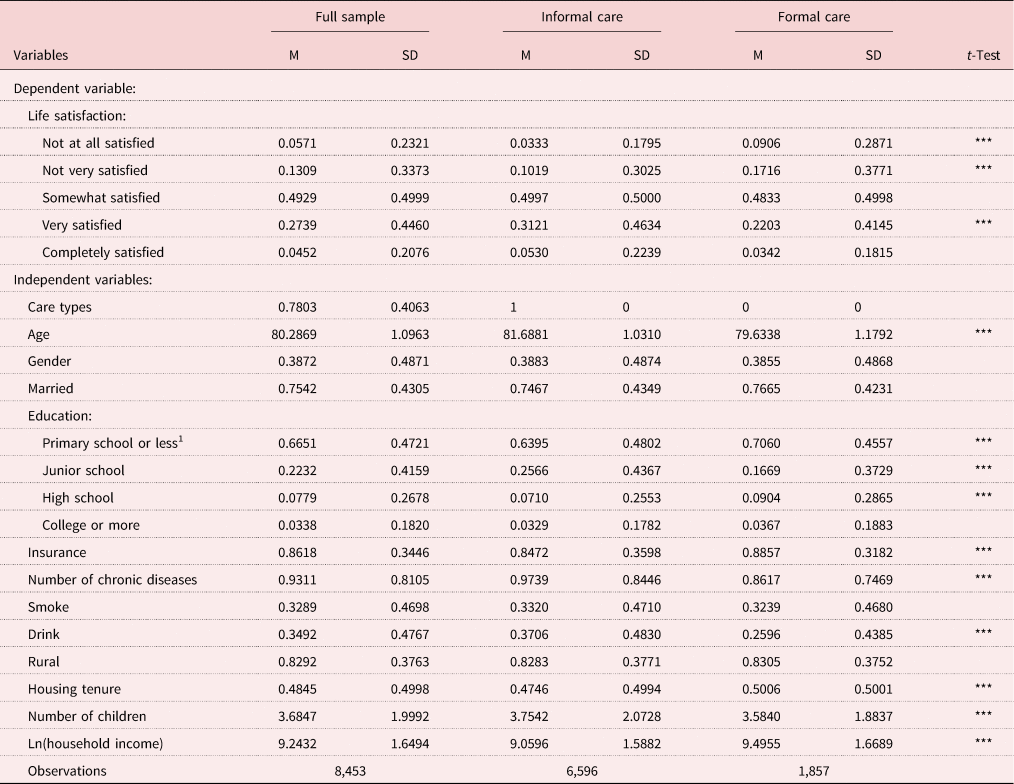
Notes: 1. Refers to the base group. M: mean value. SD: standard deviation.
Significance level: *** p < 0.01.
Full analysis
Table 3 reports the marginal effects of various care types on life satisfaction. We compared the results derived from a fixed effects model (FE) and a fixed effects model with PSM (PSM-FE) to highlight the importance of using PSM-FE to control for potential selection bias. The FE (columns 1 and 2) estimates suggest that informal care had a positive effect on life satisfaction for disabled older persons (β = 0.41, p < 0.01). When accounting for the selection bias using PSM-FE, the positive effect of informal care on life satisfaction was significantly larger at 0.63 (columns 3 and 4). These results suggest that the effects may be underestimated in the absence of controls for selection bias. The common support hypothesis of performing PSM was satisfied, as 8,441 samples were included, and only 12 samples were excluded in the matched sample. The covariate balance test showed that all the covariates were balanced after matching, indicating that the PSM method achieved the randomisation requirement.
Table 3. Effects of care types on life satisfaction
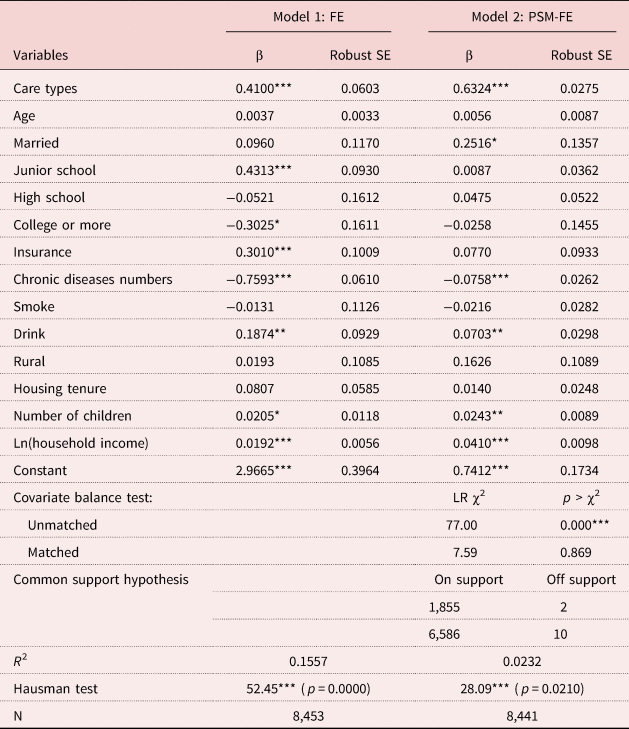
Notes: FE: fixed effects model. PSM-FE: fixed effects model with propensity score matching. SE: standard error.
Significance levels: * p < 0.10, ** p < 0.05, *** p < 0.01.
Robustness checks
We conducted two series of sensitivity analyses. We first used the nearest matching method with matching ratios 1:1 and 1:4, and then the radius matching method to check the robustness. As shown in Table 4 (Panel A), informal care had significant positive effects on life satisfaction, which is consistent with findings in our core analysis. We also estimated the effects of care types on life satisfaction using an ordered logit estimator. As shown in Table 4 (Panel B), disabled older persons receiving informal care were more likely to report they were satisfied with life compared to those receiving formal care. All of these analyses verified the robustness of our research findings.
Table 4. Robust checks of care types on life satisfaction
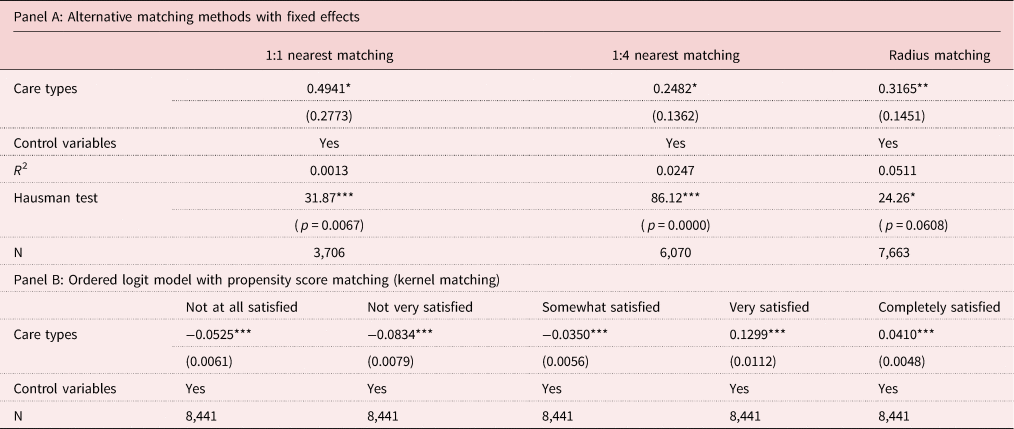
Notes: Robust standard errors are reported in parentheses. The other control variables are the same as shown in Table 3. The results are marginal effects of care types in Panel B.
Significance levels: * p < 0.10, ** p < 0.05, *** p < 0.01.
Subsample analysis
We further explored the extent to which the effects of care types on life satisfaction varied across subgroups through adding interaction terms to the FE-PSM. We first examined whether the effects differed by degree of disability. Participants who had at least one IADL limitation or one to two ADL limitations were identified as mildly disabled, whereas individuals who had at least three ADL limitations were considered moderately or severely disabled. As shown in Table 5 (Panel A), the addition of the disability degree interaction led to a significant 0.75 increase in life satisfaction. The results indicated that compared with individuals with moderate or severe disability, informal care had larger positive effects on life satisfaction for older adults with mild disability.
Table 5. Heterogeneity analysis of care types on life satisfaction

Notes: Robust standard error are reported in parentheses. The other control variables are the same as shown in Table 3. We were unable to obtain the coefficient for sex in the fixed effects model with propensity score matching as it is time-invariant.
Significance levels: * p < 0.10, ** p < 0.05, *** p < 0.01.
We also included two interaction terms (care types × gender; care types × region) to conduct heterogeneity analysis by sex and region. As shown in Table 5 (Panel B), the positive effects of informal care on life satisfaction were found to be larger for males compared to their female counterparts (β = 0.95, p < 0.01). As shown in Table 5 (Panel C), compared with those living in urban regions, the positive effects of informal care on life satisfaction for disabled older persons living in rural areas were found to be significant (β = 0.70, p < 0.01).
Mechanism analysis
In this section, we performed mediation analysis to examine the mechanisms through which care types affect life satisfaction. As shown in Table 6 (Panel A, Models 1–3), informal care significantly reduced loneness and unhappiness, increased participation in social activity and promoted physical health status for disabled older persons. In Model 4 (Table 6, Panel B), where positive emotions were constructed as the mediator, the effects of informal care on life satisfaction significantly reduced by 32.07 per cent. As shown in Model 5, social activity decreased the effects of informal care on life satisfaction by 3.95 per cent. In Model 6, where physical health was constructed as a mediator, the effects of informal care on life satisfaction significantly reduced by 6.97 per cent.
Table 6. Mediation effects of care types on life satisfaction
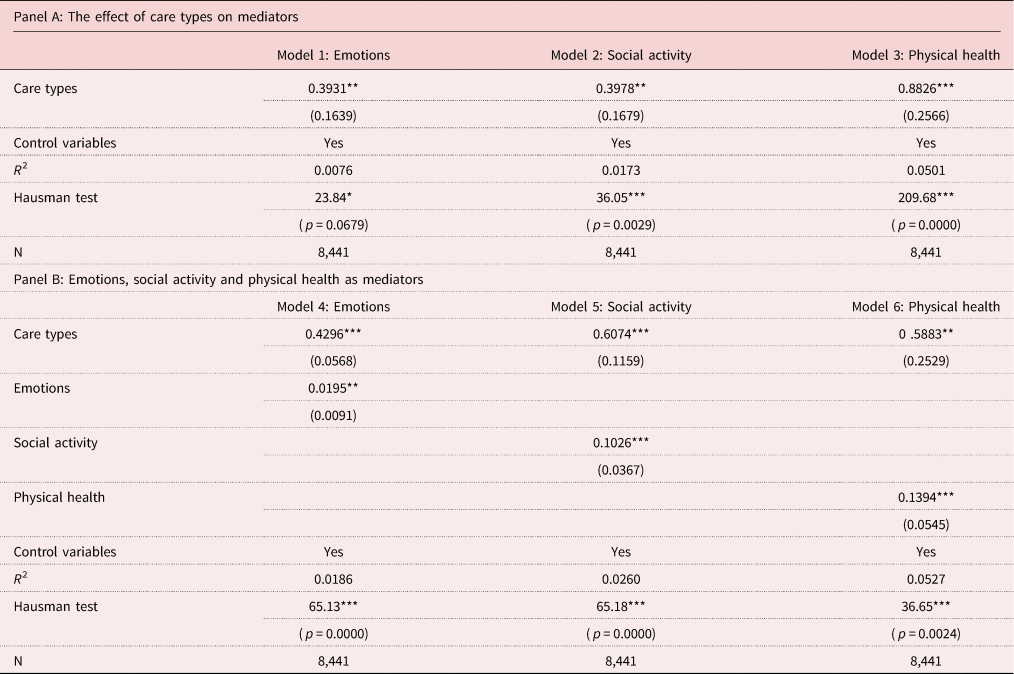
Notes: Robust standard error are reported in parentheses. The other control variables are the same as shown in Table 3.
Significance levels: * p < 0.10, ** p < 0.05, *** p < 0.01.
Discussion
Our study investigated how care type affects life satisfaction for disabled older adults in China. We found clear evidence that compared with formal care, informal care was associated with greater life satisfaction for disabled older persons. These findings are consistent with a number of previous studies. For instance, Horsfall et al. (Reference Horsfall, Leonard, Rosenberg and Noonan2017) used data from the China Health and Nutrition Survey and found that providing end-of-life care at home was associated with higher life satisfaction. Likewise, informal care has been demonstrated to improve life satisfaction for disabled older persons (Liu and Zhang, Reference Liu and Zhang2017).
We discovered that the effects of care types on life satisfaction varied according to older person's degree of disability, sex and living region. In particular, larger positive effects of informal care on life satisfaction were found among older persons with mild disability. This may be attributed to older adults with severe disability tending to require higher-intensity care provided by formal health organisations or professionals (Pezzin et al., Reference Pezzin, Pollak and Schone2009; Liu and Zhang, Reference Liu and Zhang2018). The positive impacts of informal care appeared to be greater among men than their women counterparts. This may lie in that the family social capital is particularly important for improving the life satisfaction of older men compared to older women in China. Older men benefit more psychologically from close family relationships and sufficient family support than their women counterparts (Bai et al., Reference Bai, Guo and Fu2018; Lu et al., Reference Lu, Jiang, Lou, Zeng and Liu2018; Chen et al., Reference Chen, Fu and Chang2022). We also found that informal care could only increase life satisfaction for disabled older adults living in rural areas compared to those living in urban areas. Two explanations may account for this disparity. First, deeply influenced by filial piety in Confucianism, the disabled older persons living in rural China believe to ‘raise children for old age’ and therefore family care is preferred by them (Cohen et al., Reference Cohen, McIlmail and Greaney2020; Falkingham et al., Reference Falkingham, Evandrou, Qin and Vlachantoni2020). Second, the substitutes for informal care, such as care services provided by health-care institutions, are still extremely scarce or of low quality in rural China (Chen et al., Reference Chen, Fan and Chu2020). Furthermore, we revealed that informal care was expected to reduce loneliness and unhappiness, increase social activity participation and promote physical health, which in turn promotes life satisfaction for disabled older persons.
This study extends the literature on the relationship between care types and life satisfaction in a number of ways. First, this study examined the effects of long-term care on life satisfaction for various care types, and focused on disabled older adults in China. Research in this area offers valuable implications in terms of identifying key determinants of life satisfaction to guide future policy design. Second, previous studies have proposed competing conceptualisations of the link between informal and formal care. However, our study indicates that informal care increased life satisfaction for older adults with mild disability, while formal care has larger positive effects for those with severe disability. These findings offer a perspective of complementary relationship between the two care types in a comprehensive welfare context. Third, the study further examined the mechanisms behind the effects, which provides a more comprehensive picture of the effects of care types on life satisfaction.
Our finding has implications for promoting ‘health ageing’ in China. Making full use of the various social support resources of disabled older persons can be a useful approach when designing the integrated long-term care system in China. Meanwhile, family-based care is suggested to be further promoted in China considering its foundational role in providing emotional and spiritual supports for older adults with disability. Moreover, higher-intensity care provided by formal health-care professionals or institutions is also recommended by our study as a supplement to informal care when advanced care services are needed by older individuals with severe disability.
However, some limitations of our study warranted recognition. In our study, limited by data accessibility, we classified informal and formal care by care-givers who assisted disabled older persons to perform ADLs or IADLs. Particularly, we were unable to examine how specific informal care forms (e.g. economic support, life care and spiritual comfort) would affect life satisfaction. In addition, the association between care intensity or duration and life satisfaction remains unclear and is suggested to be examined by future study. Finally, it would be of interest to examine the impact of community-based care on life satisfaction as the Chinese government is to expand the capacity of community-based care. This is also left as one of the key agendas for future research when more information becomes available.
Conclusions
This study demonstrates that compared with formal care, informal care has the potential to improve life satisfaction for disabled older persons. Also, the positive effects of informal care on life satisfaction were found to be more significant among disabled older individuals with mild disability, males and rural residents than their counterparts. Informal care was found to enhance life satisfaction through reduced loneliness and unhappiness, increased participation in social activities and improved physical health. Our study emphasises the complementary role of formal and informal care in enhancing health for disabled older persons in China.
Author contributions
All authors contributed to the conceptualisation, data analysis and writing.
Financial support
This work was supported by the National Social Science Fund of China (grant number 19CSH073); the National Natural Science Fund of China (grant number 72171133); the Natural Science Fund of Shandong Province (grant number ZR2021QG017); and the Social Science Fund of Shandong Province (grant number 18BJJJ08).
Conflict of interest
The authors declare no conflicts of interest.






