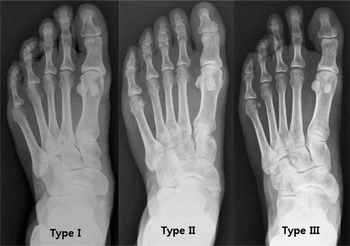
The accessory navicular bone (AN) is an extra bone located medial to the tuberosity of the tarsal navicular bone (Offenbecker & Case, Reference Offenbecker and Case2012). It is an anatomic variant that develops as a result of an incompletely fused secondary ossification center of the navicular tuberosity. The AN is classified into three types according to its shape and connection to the navicular bone (Figure 1). Type I is a small sesamoid bone embedded in the posterior tibial tendon, type II is a heart-shaped or triangular ossicle that is connected to the navicular by synchondrosis, and type III is an enlarged medial horn of the navicular after fusion of the extra bone (Vaughan & Singh, Reference Vaughan and Singh2014).
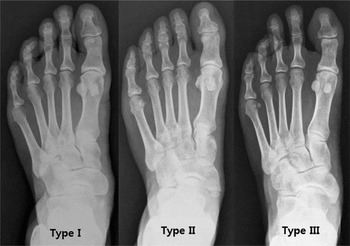
FIGURE 1 The foot radiographs of three different types of accessory navicular bone.
An AN is the most common ossicle in the foot (Coskun et al., Reference Coskun, Yuksel, Cevener, Arican, Ozdemir, Bircan and Sindel2009), with an overall incidence of 4–21% in the general population (Coskun et al., Reference Coskun, Yuksel, Cevener, Arican, Ozdemir, Bircan and Sindel2009; Miller et al., Reference Miller, Staron, Feldman, Parisien, Glucksman and Gandolfo1995). An AN may be symptomatic, causing pain in the medial foot and other resultant problems, including rare cases of fracture (Mikami & Azuma, Reference Mikami and Azuma1978). The accessory ossicle in the navicular may cause the posterior tibial tendon to insert either directly into the AN or become displaced inward and upward (Kiter et al., Reference Kiter, Erdag, Karatosun and Gunal1999; Vaughan & Singh, Reference Vaughan and Singh2014), which may lead to tendon insufficiency followed by decreased dynamic Stability and possibly progressive flattening of the longitudinal arch of the foot (Chen et al., Reference Chen, Hsu and Liang1997; Keles Coskun et al., Reference Keles Coskun, Arican, Utuk, Ozcanli and Sindel2009; Offenbecker & Case, Reference Offenbecker and Case2012; Vaughan & Singh, Reference Vaughan and Singh2014). The presence of an AN is also associated with medial foot pain, which occurs at its interface with the navicular tuberosity (Offenbecker & Case, Reference Offenbecker and Case2012), also called painful navicular syndrome (Bernaerts et al., Reference Bernaerts, Vanhoenacker, Van De Perre, De Schepper and Parizel2004), and it may lead to degenerative changes and restricted range of motion due to overuse or trauma (Huang et al., Reference Huang, Zhang, Ma, Wang, Zhang and Chen2014). The symptomatic AN can be managed with treatment ranging from conservative methods, such as activity modification, comfortable shoes with orthosis, and physical therapy to eventual surgical intervention in refractory cases (Seehausen et al., Reference Seehausen, Harris, Kay and Pace2016; Vaughan & Singh, Reference Vaughan and Singh2014). This aspect of an AN in relation to posterior tibial tendon pathology, flat foot, and a possible cause of medial foot pain has generated growing interest among clinicians.
The increasing clinical role of an AN in foot pathology has resulted in increased attention to its inheritance, with respect to whether it is passed down from generation to generation. Nevertheless, only a few studies have documented the inheritance of an AN by examining the pedigree of the families (Dobbs & Walton, Reference Dobbs and Walton2004; Kiter et al., Reference Kiter, Erduran and Gunal2000), and evaluation of genetic influence on an AN in a large sample has not yet been done.
This study aimed to estimate the heritability of an AN using data from a large-size study of twins and family that provide various types of family relationships.
Materials and Methods
Subjects
The study included a total of 996 Korean adults composed of twins of the same gender and their first-degree relatives from the participants enrolled in the Healthy Twin Study from May 2008 to April 2010. They consisted of 135 MZ twin pairs, 25 DZ pairs, and 676 singleton family members of the twins. From them, 280 father–offspring pairs, 477 mother–offspring pairs, and 266 pooled DZ and sibling pairs were identified in addition to the twin pairs.
The Healthy Twin Study was a cohort study initiated in 2005 in order to investigate genetic and environmental aspects of complex diseases. Details of the study design and protocols have been previously published (Gombojav et al., Reference Gombojav, Song, Lee, Yang, Kho, Hwang and Sung2013). Study participants were recruited through a nationwide advertisement and a mail-out to some members of the Korean twin-family register whose contact information was available. All participants of the healthy twin study underwent full medical examinations and completed detailed questionnaires asking about lifestyle and epidemiologic characteristics, after providing written informed consent. The operation or any intervention of the feet were identified and excluded. The persons who participated in the Healthy Twin Study between May 2008 and April 2010, additionally underwent physical examinations and radiographic measurements of feet in order to assess the presence of an AN and its type.
The study was approved by the Institutional Review Board at the Samsung Medical Center (IRB file No.: SMC2005-08-113)
Radiographic Assessment
Foot X-rays with an antero-posterior and lateral weight-bearing view were taken from all study participants. Two physicians well-acquainted with the types of ANs determined the presence and the type of an AN based on the interpretation of foot X-rays according to Coughlin's classification (Coughlin, Reference Coughlin2006). Inter-rater reliability between these two physicians was quantified using Cohen's kappa coefficient and it showed high reliability for any type of the AN, ranging from 0.74 to 0.95 (Table S1). The round- or oval-shaped small accessory ossicle without connection to the navicular bone was determined as Type I. Type II was defined when a triangular or heart-shaped bone was present with its base connected to the talar process by an acute angle or when it was situated inferiorly to the navicular bone. Last, when the AN was united to the navicular by a bony ridge, forming cornuate navicular bone, it was classified as Type III (Coughlin, Reference Coughlin2006; Huang et al., Reference Huang, Zhang, Ma, Wang, Zhang and Chen2014).
Zygosity and Family Relationship Ascertainment
Sixteen short tandem repeat marker kits (PerkinElmer's AmpFlSTR®, Norwalk, CT) were used to determine the zygosity of twins and to ascertain the family relationship of the other participants. A zygosity questionnaire developed by the research team, which showed a predictive value of more than 98% for MZ twins (Song et al., Reference Song, Lee, Lee, Lee, Lee, Hong and Sung2010), was also used as a supplementary mean for determining zygosity.
Statistical Analysis
Correlations within each various intrafamilial pair for the presence and classification of an AN were calculated using Cohen's kappa coefficient. The agreement for the presence and classification of an AN between the left foot and the right foot was evaluated using the chi-square test. A p value less than .05 was considered statistically significant. Descriptive statistics, calculation of the kappa coefficients, and a chi-square test were performed using statistical software (SAS software 9.4; SAS Inc., Cary, NC).
Heritability was calculated as the proportion of the total phenotypic variance explained by additive genetic effects in a statistical genetic analysis software package (Sequential Oligogenic Linkage Analysis Routines, Eclipse version 7.6.4; Allison et al., Reference Allison, Neale, Zannolli, Schork, Amos and Blangero1999; Almasy & Blangero, Reference Almasy and Blangero1998). Total phenotypic variation in an AN after adjusting for linear and non-linear effects of age, sex, and interactions between age and sex was partitioned into additive genetic (бa2), shared environmental component within a family (бc2), and individual specific unique environmental component (бe2), according to the variance decomposition model. The key assumption of this model was that the effects of environmental factors are common to the members of a family and that the three factors (бa2, бc2, and бe2) have independent and additive effects on the trait variance, with the total residual variance being the sum of the additive and individual specific variance components (бp2 = бa2 + бc2 + бe2). Thus, heritability (h 2) in the narrow sense, which represents the proportion of residual variance attributed to additive genetic factors, is the ratio of the additive component and the total variance (бa2/бp2). This assumes that all genetic variance is additive; in other words, there are no gene interactions.
Results
The demographic characteristics of the participants and the prevalence of an AN are presented in Table 1. The mean age of the participants was 43.99 years and the mean body mass index was 23.87. The prevalence of an AN in either foot was 40.96%.
TABLE 1 Characteristics of the Study Participants

Data were presented as number (percentage) for categorical variables or mean ± standard deviation for continuous variables.
a The presence of any type of an accessory navicular bone in the right foot or the left foot.
Table 2 shows the prevalence of an AN among participants in both feet and in both sexes. Type II was the most common type in both feet. There was no significant difference in the AN prevalence between right foot and left foot (p > .05) and between both sexes (p > .05).
TABLE 2 Prevalence (per 100 Persons) of Accessory Navicular Bone By Subtypes

Data were presented as number (percentage).
*Agreement of accessary navicular bone on the right foot and left foot was evaluated by Cohen's kappa coefficient.
Table 3 shows the laterality of an AN and the difference in the distribution of an AN subtypes between the right and left feet in bilateral cases. An AN tended to be present bilaterally (69.36%) rather than in only one foot (30.64%), and the majority (85.16%) of bilateral ANs showed concordance between both sides. Among the bilaterally concordant cases, type II AN was more common than the other types. Among the bilaterally discordant cases, the type I–type II combination was the most common, followed by the II–III combination.
TABLE 3 Laterality of Accessory Navicular Bone and Side to Side Expression (Difference in the Distribution of Subtypes Between Right Foot and Left Foot) in Bilateral Cases

a Percentage among total number of participants (996 in all, 604 in women, and 392 in men).
b Percentage among total number of bilateral accessory navicular bone (283 in all, 178 in women, and 105 in men).
Table 4 shows the intrapair agreement and heritability of AN. The intrapair agreement within MZ twin pairs was more than two times higher than that in other intrafamilial pairs, such as father–offspring pair, mother–offspring pair, and pooled DZ twin and sibling pairs. After adjusting for age and sex, the heritability estimate for the presence of any type of an AN in any foot was 0.88 (95% CI [0.82, 0.94]). Specifically, type II AN showed the highest heritability of 0.82 (95% CI [0.71, 0.93]).
TABLE 4 Intrafamilial AgreementFootnote * and Heritability of an Accessory Navicular Bone

MZ = monozygotic twins, DZ = dizygotic twins, SB = sibling, SE = standard error.
* Assessed by Cohen's kappa coefficient. † Adjusted for age and and sex. §Any type of an accessory navicular bone in the right foot or the left foot.
Discussion
In the present study of Korean healthy twins and their first-degree family members, we found that an AN in the foot is a highly heritable trait. To date, there have been a few studies on the inheritance of an AN (Dobbs & Walton, Reference Dobbs and Walton2004; Kiter et al., Reference Kiter, Erduran and Gunal2000; Offenbecker & Case, Reference Offenbecker and Case2012).
Kiter et al. (Reference Kiter, Erduran and Gunal2000) studied three generations of three pedigrees and found that an AN is transmitted in an autosomal dominant pattern with incomplete penetrance. Dobbs and Walton (Reference Dobbs and Walton2004) also verified the same result through studying two pedigrees of Scandinavian family. However, these studies stopped at unearthing the inheritance pattern because the number of participants was fewer than 80. To the best of our knowledge, this is the first study to examine twins and their families to determine precise heritability of AN, with a large, sufficient number of participants of almost 1,000. Heritability estimation in a study involving both twins and their families may have a strength that overestimation of heritability can be avoided through the comparisons of phenotypic correlations between various familial relationships compared to the twin-only study or family-only study (Tenesa & Haley, Reference Tenesa and Haley2013).
In our study, among the different types of ANs, type II AN was the most common and the most highly heritable type among the different types. This is a clinically noteworthy finding as type II AN is also the most symptomatic type.
The laterality of an AN has been a lingering controversy. Some researchers have claimed the bilateral presence of an AN (Mygind, Reference Mygind1953; Shands & Wentz, Reference Shands and Wentz1953), while another researcher claimed there is laterality in an AN (Coskun et al., Reference Coskun, Yuksel, Cevener, Arican, Ozdemir, Bircan and Sindel2009). In our study, there was a significant bilateral tendency of an AN and significant concordance in the type expression in both feet, with bilateral type II AN being the most common. These findings are strong evidence to support the bilateral tendency of AN.
Human height is a widely known inherited trait with an authorized prediction method for height of the next generation, the mid-parental height. Given that the reported heritability of height in humans is 0.8 (Silventoinen, Reference Silventoinen2003; Visscher et al., Reference Visscher, Hill and Wray2008) from a study by Silventoinen in 2003, and that the heritability of hallux valgus is 0.51 (Lee et al., Reference Lee, Lee, Kang, Jung, Song, Lee and Sung2014), the heritability estimate of 0.88 implies a very strong genetic contribution to the presence of an AN in the foot. As the clinical role of an AN in foot pathology is considerable due to its association with posterior tibial tendon insufficiency, malalignment of the medial foot arch and probably pes planus, high heritability of an AN needs to be further emphasized. Being well acquainted with high heritability and bilateral tendency of an AN would aid clinically in dealing with foot pain in patients with a family history of an AN. The physicians should be aware of the possibility of an AN in order to avoid missing or misdiagnosing a symptomatic AN as simple arthritis or any other disease pathology.
The present study has a limitation to be considered. First, the presence and the type of an AN were ascertained using foot X-rays with only the antero-posterior and lateral weight-bearing views. An additional lateral oblique view of foot X-ray is often helpful in determining the subtypes of type II and III ANs, and occasionally for differentiation of type II AN from type III AN in difficult cases. Therefore, we think an extra oblique view would have improved the precision of radiographic assessment, especially regarding the type differentiation. However, the effect of the limited X-ray view seems to have had a modest impact on the findings of our study, given that the presence of an AN can still be determined simply by an antero-posterior view (Vaughan & Singh, Reference Vaughan and Singh2014). Moreover, the high interrater reliability (kappa coefficients ranged between 0.74 and 0.95) between the two measurers of an AN in our study also supports that significant measurement bias is less likely to be involved. Second, we estimated narrow sense heritability of AN. Given that the narrow sense heritability assumes all genetic variance as additive and does not consider dominance variance or epistasis, the heritability estimation of an AN in our study might have been a bit inflated.
In conclusion, we found that genetic influence plays a major role in the development of an AN in the foot, using the data of Korean healthy twins and their first degree family members. This finding may serve an evidence supporting that prediction of an AN in a person is possible by reviewing a family history of AN. Further studies are needed to elucidate genes that are involved in determination of an AN development.
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Science, ICT and future Planning(2014R1A2A2A01002705).
Disclosure of Interests
None.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/thg.2017.21