



Introduction
Induced abortion is closely associated with maternal morbidity, mortality, and reproductive rights of women and thus continues to draw research interest. In India, 15·6 million abortions took place in 2015, giving an abortion rate of 47 per 1000 women aged 15–49 (Singh et al., Reference Singh, Shekhar, Acharya, Moore, Stillman, Pradhan, Frost, Sahoo, Alagarajan, Hussain, Sundaram, Vlassoff, Kalyanwala and Browne2018). Of those, 73% of abortions were medication abortions done outside of health facilities, and 5% of abortions were done outside of health facilities using methods that were probably unsafe. Unsafe abortion contributes to morbidity and mortality (Banerjee, Reference Banerjee2007; Yokoe et al., Reference Yokoe, Rowe, Choudhury, Rani, Zahir and Nair2019) and is considered a major public health problem in India (Creanga et al., Reference Creanga, Roy and Tsui2008; Duggal & Ramachandran, Reference Duggal and Ramachandran2004; Yokoe et al., Reference Yokoe, Rowe, Choudhury, Rani, Zahir and Nair2019). Many women in India still lack access to safe abortion care, despite legalising abortion through the Medical Termination of Pregnancy Act of 1971 and several amendments acknowledging women’s reproductive choices and rights. Shortage of certified providers and facilities, financial barriers to safe services, providers’ knowledge and attitudes, lack of awareness of abortion laws, and, more importantly, the stigma surrounding abortion affect women’s abortion-seeking behaviour (Hirve, Reference Hirve2004; Pradhan et al., Reference Pradhan, Sekhar, Alagarajan and Sahoo2022; Stillman et al., Reference Stillman, Frost, Singh, Moore and Kalyanwala2014). Lack of privacy and confidentiality and inadequate knowledge about the location of the safe provider further compel women for unsafe abortions in the country (Banerjee et al., Reference Banerjee, Andersen, Baird, Ganatra, Batra and Warvadekar2014; Barua & Apte, Reference Barua and Apte2007; Elul et al., Reference Elul, Barge, Verma, Kumar, Bracken and Sadhwani2004).
Globally, limiting childbearing is the most cited reason given by women for abortion. Interruption of work or education, lack of support from the father, the desire to provide a school for existing children, poverty, unemployment or the inability to support more children, and women’s concern with their partner are among the socioeconomic problems that make up the second most common reason (Bankole, Singh and Haas, Reference Bankole, Singh and Haas1998; Chae et al., Reference Chae, Desai, Crowell and Sedgh2017). In India, abortions are performed for several reasons, including restricted contraception use, financial constraints, already having too many children, religious issues, abortion’s legal status, unwanted pregnancies, pregnancy as a result of rape, and risks to the mother or foetal health. The fundamental underlying causes, however, are lack of knowledge or access to contraceptives (Behera et al., Reference Behera, Bharat and Chandrakant Gawde2015; Grimes et al., Reference Grimes, Benson, Singh, Romero, Ganatra, Okonofua and Shah2006; Warriner & Shah, Reference Warriner and Shah2006). Spacing was the main reason adolescents sought an abortion in Maharashtra (Ganatra & Hirve, Reference Ganatra and Hirve2002). Having women with abortion experiences in their networks enhanced the likelihood of induced abortion in Rajasthan (Elul, Reference Elul2011). Bleeding per vaginum, unwanted pregnancy, and unviable foetus diagnosed by ultrasonography were self-reported reasons for induced abortion in Haryana (Kant et al., Reference Kant, Srivastava, Rai, Misra, Charlette and Pandav2015). In rural Odisha, the most common reason for seeking an abortion was poverty, followed by the husband’s insistence (Pattanaik et al., Reference Pattanaik, Patnaik, Subhadarshini and Sahu2017). Maternal age, religious beliefs, family income, number of parity, and knowledge of legal abortion were associated with abortion in West Bengal (Mollick et al., Reference Mollick, Chakraborty, Ray and Das2022). There are also instances of sex-selective abortions in the country (Ganatra & Hirve, Reference Ganatra and Hirve2002; Jha et al., Reference Jha, Kesler, Kumar, Ram, Ram, Aleksandrowicz, Bassani, Chandra and Banthia2011; Kant et al., Reference Kant, Srivastava, Rai, Misra, Charlette and Pandav2015; Saikia et al., Reference Saikia, Meh, Ram, Bora, Mishra, Chandra and Jha2021; Singh et al., Reference Singh, Shekhar, Acharya, Moore, Stillman, Pradhan, Frost, Sahoo, Alagarajan, Hussain, Sundaram, Vlassoff, Kalyanwala and Browne2018; Zavier et al., Reference Zavier, Jejeebhoy and Kalyanwala2012). A study based on the second round (1998–99) of the National Family Health Survey (NFHS) found that unintended pregnancy, maternal education, and urban residence were positively associated with demand for abortion (Pallikadavath & Stones, Reference Pallikadavath and Stones2006). Another study using the same data revealed a significant north-south difference in the reasons for abortion (Bose & Trent, Reference Bose and Trent2006).
The available evidence on reasons for abortion is mainly based on small-scale studies with inherent limitations that prevent the generalisation of the factors. Additionally, the studies based on the earlier round of NFHS (Bose & Trent, Reference Bose and Trent2006; Pallikadavath & Stones, Reference Pallikadavath and Stones2006) presented a two-decade-old scenario and did not consider many vital predictors such as place of abortion, gestational age, abortion method, and history of contraceptive use. Thus, based on the most recent rounds of NFHS (2019–21), this study assesses if the reasons for abortion differ depending on a woman’s socio-demographic and economic features, as well as to identify the key predictors of mentioned reasons for abortion in India.
Methods
Data
The study used data from the fifth round of the NFHS conducted in 2019–21. The NFHS-5 is a nationally representative survey of 636 699 households that provides information for a wide range of monitoring and impact evaluation indicators of health, nutrition, disability, and women’s empowerment. The NFHS-5 sample is a stratified two-stage with an overall response rate of 98%. The primary sampling units, that is, the survey villages in rural areas and census enumeration blocks in urban areas, were selected using probability proportional to size sampling. Trained research investigators gathered the data using computer-assisted personal interviewing. Only those respondents who gave voluntary consent were interviewed. The published survey report provides a more detailed description of the survey design, questionnaire, quality control measures, and survey management information (IIPS/India & ICF, 2022). The present analysis used the data of women aged 15–49 who had terminated their last pregnancy by induced abortion in the five years preceding the survey (n=5835). Specifically, the women mentioned above were asked about abortion and post-abortion complications. The questions included were as follows: Where was the abortion performed? Who performed the abortion? What method was used for the abortion? What was the main reason for the abortion? Did you have any complications from the abortion? Did you seek treatment for the complication? Where did you go for treatment? Why did you not seek treatment?
Outcome variable
The reason a woman had her abortion was taken as the outcome variable. The stated reasons for abortion were grouped into three categories for meaningful interpretation of the data. The first category, ‘Life risk/medical reasons’, includes complications in pregnancy, health did not permit, or foetus’s congenital abnormality. The second category, ‘Sex-selective-abortions,’ includes reasons like a female foetus, male foetus, or husband/mother-in-law did not want. Reasons such as unplanned pregnancy, contraceptive failure, economic reasons and last child too young were grouped under the third category – ‘Unintended pregnancies’. We included ‘mother-in-law/husband did not want’ in the sex-selective abortion group, assuming it is a sex-selective abortion of the foetus compelled by the in-law’s family.
Predictor variables
The individual, household, and community-level predictor variables used in the analysis were based on the information available in the NFHS-5 and literature review. Individual-level characteristics included were women’s age in years (15–24, 25–34, 35–49), gestational age in weeks (≤8, 9–20, >20), method of abortion (medicine, manual vacuum aspiration-MVA, other surgical, other/do not know), place of abortion (public, private, home/other), years of schooling (no schooling, <10 years, ≥10 years), number of surviving children (no child, <3 children, ≥3 children), exposure to mass media (no, yes), correct knowledge of ovulatory cycle (no, yes), and ever used modern spacing contraception (no, yes). The household features like the type of family (nuclear, joint), religion (Hindu, others), caste (scheduled caste/scheduled tribe-SC/ST, other backward classes-OBC, Non-SC/ST/OBC), wealth quintile (poorest, poorer, middle, richer, richest), and community-level characteristics such as place of residence (rural, urban) and geographical regions (North, Central, East, North East, West, South) were also included in the analysis. The women reading newspapers or magazines/watching television/listening to the radio/visiting cinema or theatre were considered exposed to mass media. SC and STs are socio-economically weaker groups and have been found to perform poorly in several health and development indicators. Moreover, the number of women in each group was relatively less, so they were merged for the analysis. Past studies followed a similar approach (Jiwani et al., Reference Jiwani, Raval, Steele and Goldberg2022; Wagner et al., Reference Wagner, Shotwell, Boulton, Carlson and Mathew2021). Non-use of modern contraception and abortion are closely related. Especially women not using any modern spacing method are at a higher risk of unintended pregnancies, which may result in abortion. It is also crucial to understand the relationship between induced abortion and contraceptive use to address the unmet need for contraception and gaps in access to family planning services (Morris & Prata, Reference Morris and Prata2018).
Statistical analysis
Descriptive analysis was used to present the socioeconomic, demographic, and health profiles of women aged 15–49 who had terminated their last pregnancy with an abortion. The individual relationship between the predictors and the outcome variables was determined using bivariate analyses. Since the dependent variable was nominal with more than two categories and multiple independent variables, multinomial logistic regression was used. Adjusted relative risk ratios with 95% confidence intervals were estimated. National-level individual sample weight was used to adjust the non-responses. Stata (v16.0) was used with a 5% significance level for analyses.
Results
Characteristics of women seeking an abortion
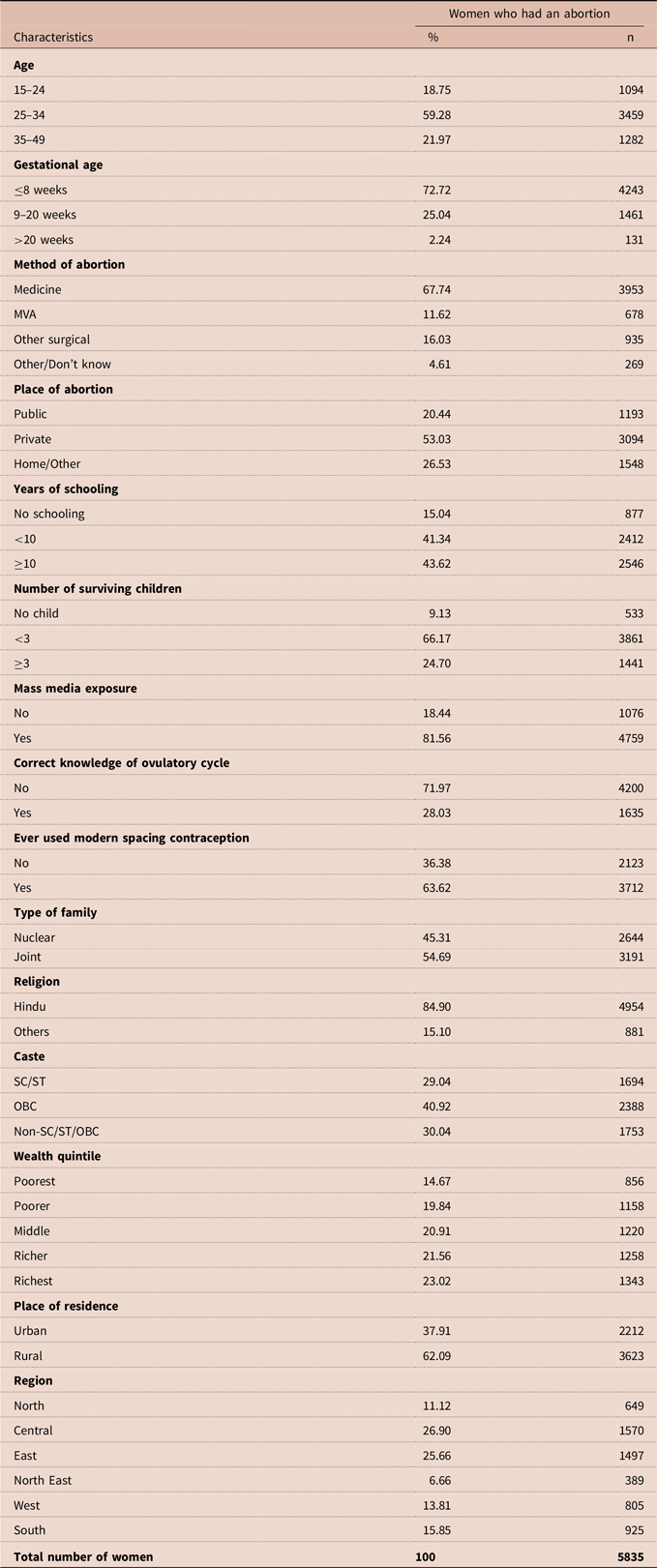
Eleven per cent of all surveyed women reported that their last pregnancy ended in a non-live birth, that is, miscarriage (7%), abortion (3%), or stillbirth (1%), in the five years preceding the survey (Figure 1). Table 1 presents the characteristics of the surveyed women who had terminated their last pregnancy with an abortion. Of the women, 59% were 25–34 years old, 22% were 35–49 years old, and the remaining 19% were 15–24 years old. While obtaining an abortion, 73% of women had a gestational age of fewer than eight weeks, 25% had a gestational age of 9–20 weeks, and 2% had a gestational age of more than 20 weeks. Sixty-eight per cent of women took medicine, 16% used another surgical method, 12% had MVA, and only 5% used other methods/do not know the method used for abortion. More than half (53%) of the women had their abortion in the private health sector, 27% at home/others, and the remaining 20% in the public sector. Forty-four per cent of the women did schooling for ten or more years, 41% did schooling for less than ten years, and 15% did no schooling. Two-thirds (66%) of the women had less than three surviving children, 25 % had three or more surviving children, and 9% had no child. Eighty-two per cent of women had exposure to mass media. Only 28% of women had correct knowledge of the ovulatory cycle, and 64% had ever used any modern spacing contraceptive method. More than half (55%) of the women lived in a joint family. The majority of women (85%) belonged to the Hindu religion. Forty-one per cent of the women belonged to OBC, 30% to Non-SC/ST/OBC, and 29% to SC/ST category. Twenty-three per cent of women belonged to the richest, 21% to the richer, 21% to the middle, 20% to the poorer and 15% to the poorest wealth quintile households. About three-fifths (62%) of these women resided in rural areas. Of the women, 27% belong to the central region, 26% to the eastern region, 16% to the southern region, 14% to the western region, 11% to the northern region, and 6% to the north-eastern region.
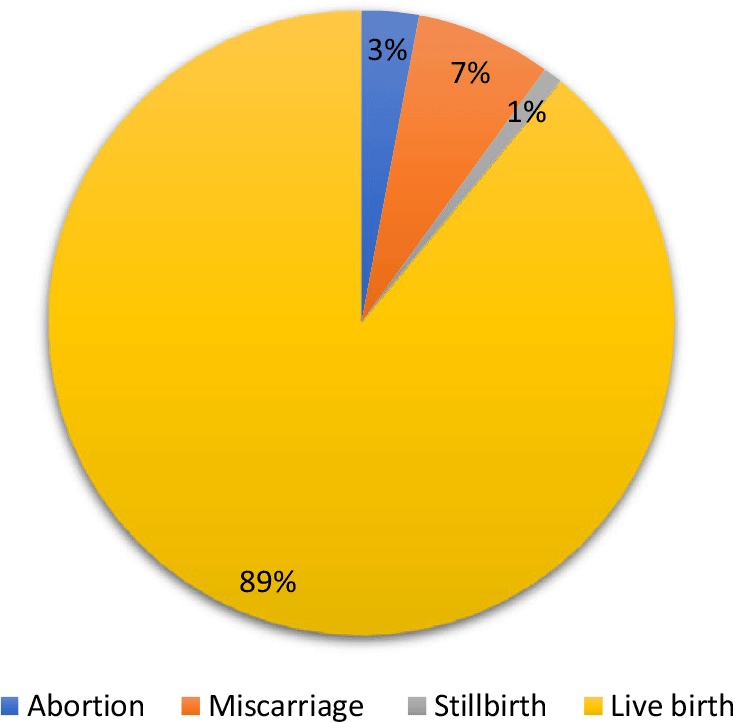
Figure 1. Per cent distribution of outcome of all pregnancies during the past five years preceding the survey, India, 2019–21.
Table 1. Profile of the women aged 15–49 who terminated their last pregnancy with an abortion in the five years prior to the survey, India, 2019–21 (n=5835)
Socioeconomic and demographic differentials in reasons for abortion
Of the women undergoing an induced abortion, about half (49%) cited unplanned pregnancy as the reason (Figure 2). Eleven per cent of these women aborted their pregnancy due to health concerns, while another 10% revealed having a young child as the reason. Eight per cent of the pregnancies were aborted due to pregnancy complications. Contraceptive failure was the reason for abortion for four per cent of the women, while an equal number also cited their husband/in-law’s reluctance.
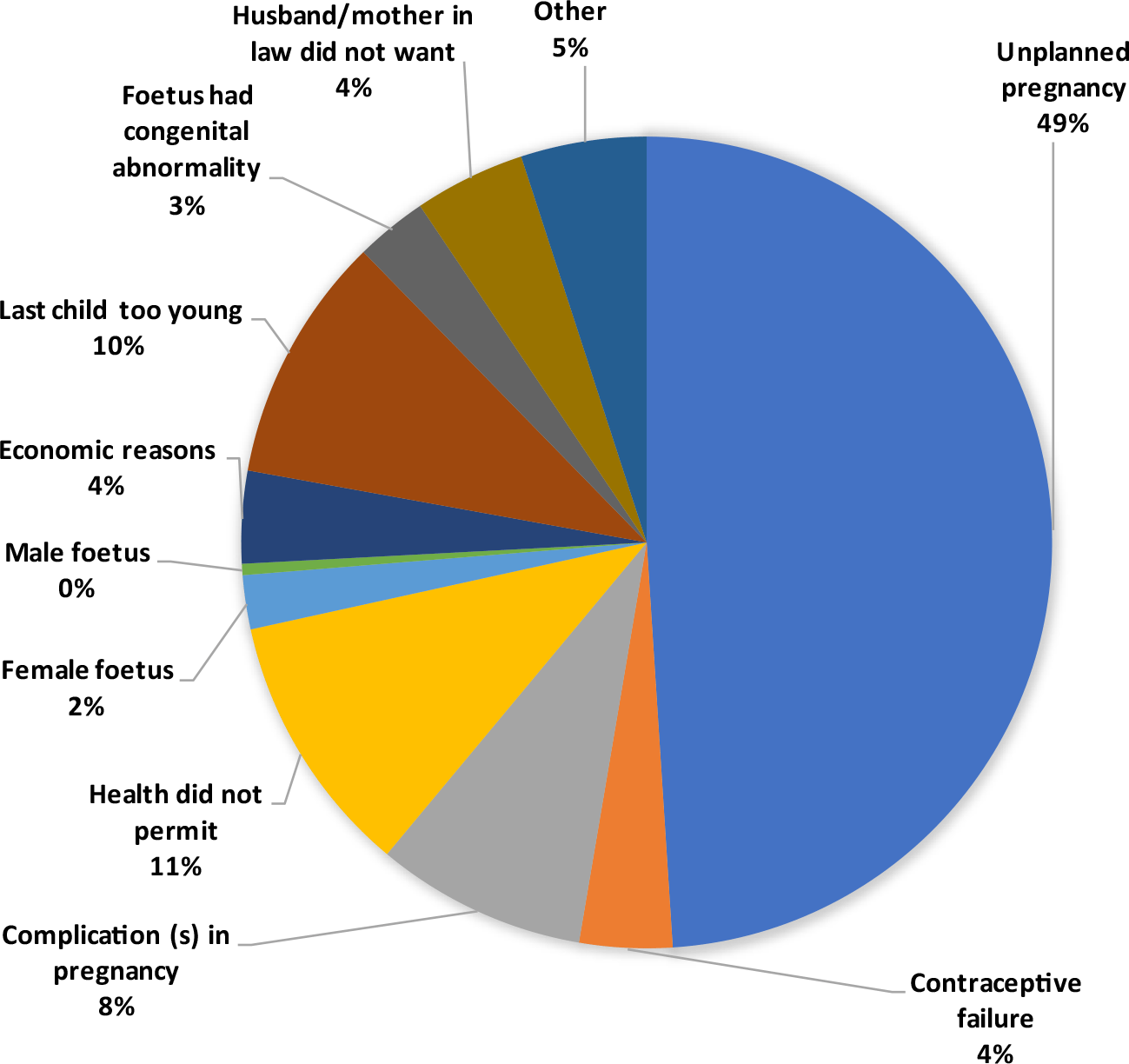
Figure 2. Reasons for abortion among women aged 15–49 years, India, 2019–21.
Table 2 presents the percentages of women whose last pregnancy ended in an abortion in the five years preceding the survey by selected reason for abortion and background characteristics. Seventy-one per cent of the women who terminated their last pregnancy with abortion cited unintended pregnancies, 22% to avoid life risk and 7% for sex-selective reasons. The 7% sex-selective reason comprised 4% abortions due to husband/in-law’s reluctance, 2% due to female foetus, and 1% due to male foetus. Sixty-seven per cent of those aged 15–24 years went for induced abortion due to unintended pregnancy, while the corresponding figure was 73% among women aged 35–49. With the increasing age of women, sex-selective abortions went up (6% among 15–24 years vs 8% among 35–49 years) and while the percentage of abortions for life risk reasons decreased (27% among 15–24 years vs 19% among 35–49 years). Of the women who terminated their pregnancy at less than nine weeks of gestational age, 15% did it to avoid life risk, 6% had a sex-selective abortion, and the rest was unintended pregnancy. The corresponding figures for abortions after 20 weeks of gestation were 65%, 8%, and 27%, respectively. Of women who had their abortion by other surgical methods, 35% cited life risk as a reason. Most (86%) abortions conducted at home/non-institution were for unintended pregnancies. Sex-selective abortions were higher among women with no schooling (10%) than those with 10 or more years of schooling (6%). Again, a higher percentage of the women with no schooling (74%) underwent abortions for unintended pregnancy than their counterparts with ten or more years of schooling (66%).
Table 2. Percentage of women aged 15–49 whose last pregnancy terminated in an abortion by reason for abortion and background characteristics, India, 2019–21 (n=5835)
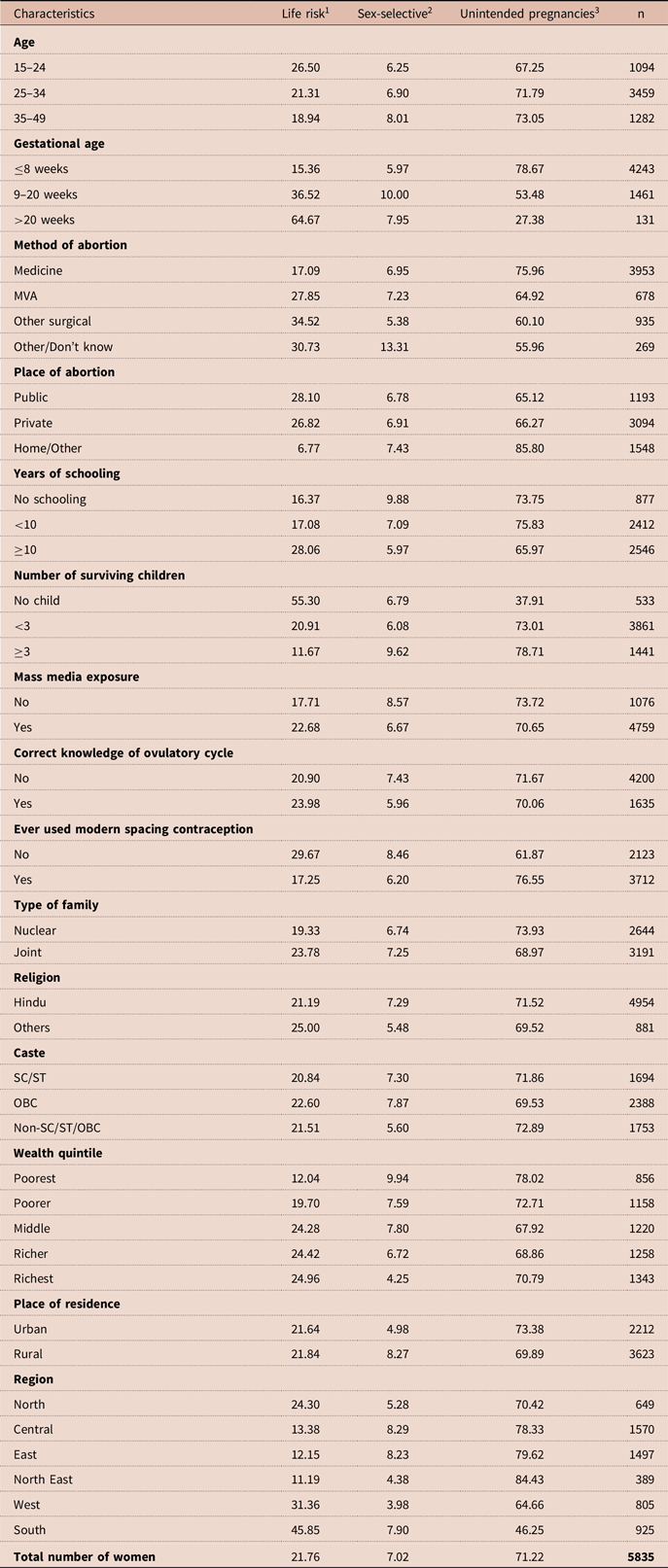
1 Complications in the pregnancy/health did not permit/foetus had congenital abnormality.
2 Female foetus/male foetus/husband or in-law did not want.
3 Unplanned pregnancy/contraceptive failure/economic reason/last child too young/other.
Sex-selective abortions were lower among women with less than three surviving children (7%) than those with at least three surviving children (10%). Unintended pregnancy as a reason for abortion was higher among women with three and more children (79%) than those with no child (38%). Twenty-three per cent of women exposed to mass media aborted their last pregnancy due to life risk, compared with 18% of those without mass media exposure. Of the women who never used any modern spacing contraceptive method, 38% had their abortion for life risk (30%) and sex-selective (8%) reasons. The corresponding figures were 17% and 6% for those who used any modern spacing contraception. Sex-selective abortion was reported by 7% of Hindus and 5% non-Hindu women. Additionally, 6% of the women from the Non-SC/ST/OBC category had a sex-selective abortion, which was 8% among their counterparts from OBC and 7% among those from SC/ST category.
As the wealth quintile increased from poorest to richest, the percentage of women terminating their pregnancy due to life risk increased from 12% to 25%, and sex-selective abortions decreased from 10% to 4%. Five per cent of the women from urban areas and 8% of their counterparts from the rural area reported sex-selective abortion. Abortion for unintended pregnancies was more common in the north-eastern (84%) and eastern (80%) regions than in the southern region (46%). Sex-selective abortions were reported by 4% of women each from the western region and the north-eastern region, while it was 8% among women from the central, eastern, and southern regions of the country. At the state level, Tripura had the highest percentage of abortions due to unintended pregnancies, while Lakshadweep and Mizoram had the lowest (0%) (Figure 3). The percentage reporting sex-selective abortion varied across major states ranging from 0% in Meghalaya, Sikkim, Chandigarh, Kerala, Mizoram, and Lakshadweep to 16% in Dadra & Nagar Haveli.
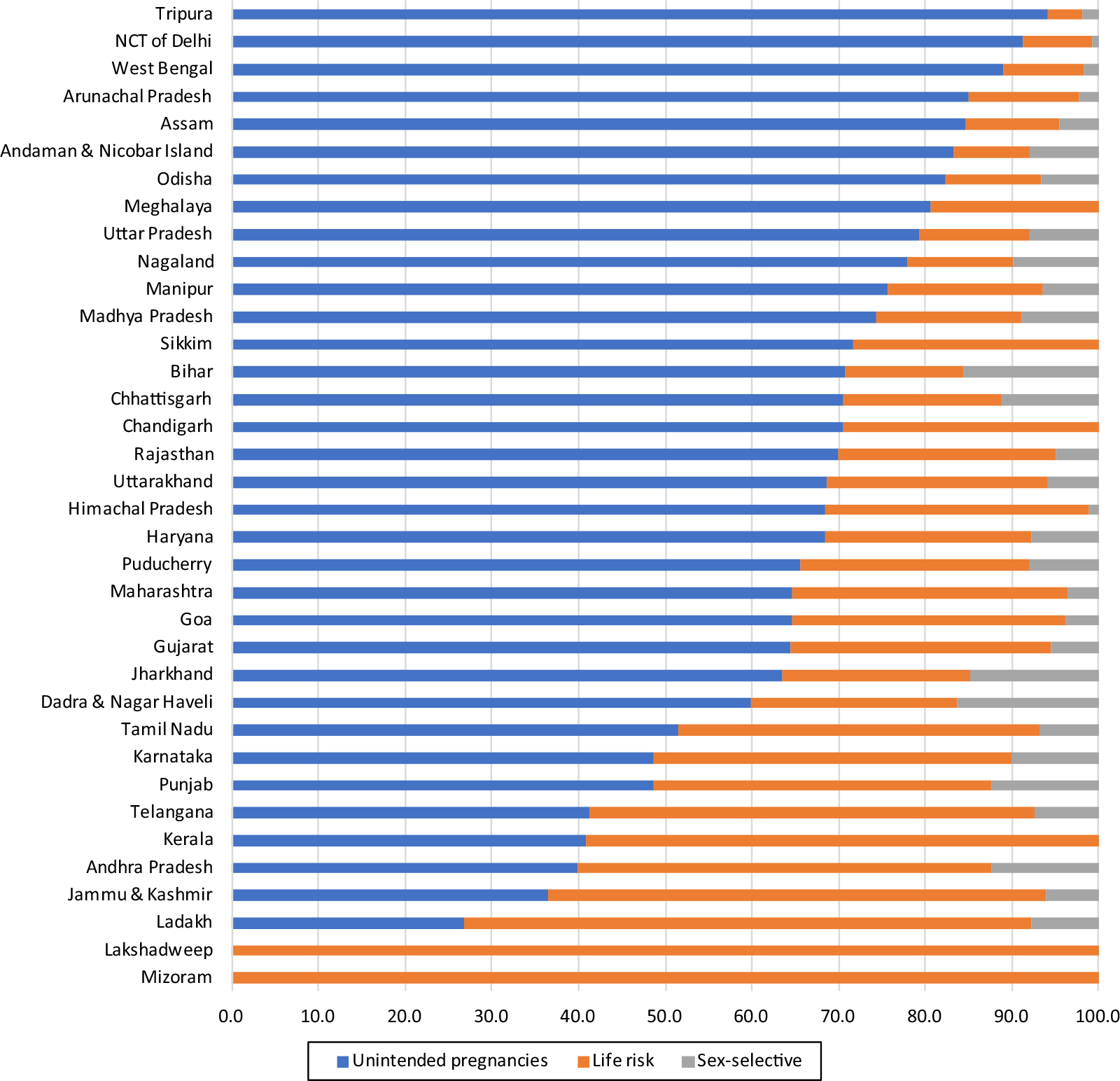
Figure 3. Reasons for abortion by states, India, 2019–21.
Socioeconomic and demographic predictors of the reason for abortion
Table 3 presents the relative risks for the specific reason for abortion for the sampled women by their background characteristics. Women with 9–20 weeks of pregnancy were 61% (RR: 0.39; CI: 0.33–0.46) less likely, and those with more than 20 weeks were 84% (RR: 0.16; CI: 0.10–0.26) less likely than those with less than eight weeks of gestation to abort their pregnancy due to unintended pregnancies rather than due to life risk. Moreover, abortions in more than 20 gestational weeks were 53% (RR: 0.47; CI: 0.22–0.98) less likely than those with less than eight weeks of gestation due to sex-selective reasons rather than due to life risk. The use of the MVA method was 34% (RR: 0.66; CI: 0.53–0.83) less likely, and other surgical methods were 39% (RR: 0.61; CI: 0.50–0.74) less likely than medicines taken among women who had their abortion due to unintended pregnancies rather than due to life risk. Similarly, the MVA method was 44% (RR: 0.56; CI: 0.37–0.84) less likely, and other surgical methods were 53% (RR: 0.47; CI: 0.32–0.68) less likely than medicines taken among women who had their abortion due to sex-selective reasons rather than due to life risk. Women were more likely to abort their pregnancy at home/other than in the public health sector if unintended pregnancies (RR: 2.79; CI: 2.15–3.61) and sex-selective abortions (RR: 2.43; CI: 1.67–3.55) rather than life risk. Women with less than three children (RR: 2.88; CI: 2.26–3.67) and three or more children (RR: 4.16; CI: 3.06–5.64) were more likely to abort their pregnancy than those with no child due to unintended pregnancies rather than life risk. Again, women with less than three children (RR: 1.70; CI: 0.70–1.46) and those with three or more children (RR: 2.71; CI: 1.65–4.45) were highly likely to abort their children than those women with no child due to sex-selective reasons rather than life risk. Women with correct knowledge of the ovulatory cycle were 26% less likely (RR: 0.74; CI: 0.56–0.97) to abort their pregnancy than those without knowledge due to sex-selective reasons rather than life risk.
Table 3. Adjusted relative risk ratio for stating a non-medical reason rather than a medical reason for abortion for women aged 15–49 by background characteristics, India, 2019–21

Note: * p < 0.05; ** p < 0.01; *** p < 0.001.
Compared with the Hindu women, non-Hindus were 31% (RR: 0.69; CI: 0.57–0.54) and 25% (RR: 0.65; CI: 0.46–0.91) less likely to abort their child due to unintended pregnancies and sex-selective reasons rather than life risk. Women in the richer and richest wealth quintiles were 40% (RR: 0.60, CI: 0.37–0.97) and 45% (RR: 0.55, CI: 0.31–0.97) less likely to abort their pregnancy than their counterparts from the poorest wealth quintile due to sex-selective reasons rather than life risk. Women in rural areas were 18% less likely (RR: 0.82; CI: 0.68–0.98) than those in urban areas to abort due to unintended pregnancies rather than life risk. Compared with women from the north, women from the central region were 73% (RR: 1.73; CI: 1.35–2.23), the eastern region was 87% (RR: 1.87; CI: 1.43–2.46), and those from the north-eastern were more than three times more likely (RR: 3.47; CI: 2.63–4.59) to abort their pregnancy due to unintended pregnancies rather than life risk. However, women from the southern region were 39% less likely (RR: 0.61; CI: 0.47–0.80) to abort their pregnancy due to unintended pregnancies rather than life risk. Similarly, women from the central (RR: 2.35; CI: 1.52–3.66), the eastern (RR: 2.68; CI: 1.70–4.22), and the north-eastern region (RR: 2.22; CI: 1.34–3.69) were highly likely to abort their pregnancy than the northern region due to sex-selective reasons rather than life risk.
Discussion
The study found unintended pregnancy as the major contributor to induced abortion in India, although some women undergo the procedure due to medical reasons and the undesired gender of the unborn child. The reasons for abortion vary considerably by socioeconomic, demographic, and health profile of the women. Unintended pregnancies that end in abortion are strongly correlated with gestational age, method of abortion, place of abortion, number of surviving children, religion, place of residence, and region. Again, there is a strong association between the sex-selective reason for abortion and the gestational age, method of abortion, place of abortion, number of surviving children, correct knowledge of the ovulatory cycle, religion, wealth quintile, and region. The study found that unintended pregnancies and sex-selective abortion were more likely among women with a gestational age of fewer than eight weeks, and the results conform to earlier studies (Agarwal & Salhan, Reference Agarwal and Salhan2008; Pattanaik et al., Reference Pattanaik, Patnaik, Subhadarshini and Sahu2017), which found that the majority of abortions were within 12 weeks of gestation.
In this study, medicine was strongly associated with abortions for unintended pregnancies, and most abortions are conducted at home. A past study had similar observations (Singh et al., Reference Singh, Shekhar, Acharya, Moore, Stillman, Pradhan, Frost, Sahoo, Alagarajan, Hussain, Sundaram, Vlassoff, Kalyanwala and Browne2018). The most likely explanation is that women who had abortions at home chose to do so because they did not want to tell their families about them and were afraid to visit a hospital. As a result, they acquired abortion drugs from neighbourhood pharmacies (Gaur et al., Reference Gaur, Shukla and Acharya2021). A study in Nepal suggests that the lack of knowledge and barriers to access and use of safe abortion services fuel the demand for MA through pharmacies (Rogers et al., Reference Rogers, Sapkota, Tako and Dantas2019). In Bangladesh, patients purchase Mifepristone/Misoprostol from pharmacists because they are logistically easier to access (Crouthamel et al., Reference Crouthamel, Pearson, Tilford, Hurst, Paul, Aqtar and Averbach2021). A recent systematic review suggests that expanding access to medical abortion through pharmacies is a potential strategy to promote safe abortion care (Rodriguez et al., Reference Rodriguez, Edelman, Hersh, Gartoulla and Henderson2021). The study found that women who had abortions because of unwanted pregnancies had at least one surviving child. This finding is similar to those of studies by Kumar et al. (Reference Kumar, Jyoti, Aruna, Poddar, Dhariwal and Shailendra2012) and Pallikadavath and Stones (Reference Pallikadavath and Stones2006), which found that the most common reason for abortion among women who had previously had two living children was an unintended pregnancy. As documented in earlier studies (Begum et al., Reference Begum, Dwivedi, Pandey and Mittal2010; Sarder et al., Reference Sarder, Islam, Talukder and Ahammed2021), this study also found that women who practised Hinduism had a higher rate of abortions because of unintended pregnancies. Unintended pregnancies led to more abortions among urban women; the stress of city living and improved access to safer methods of abortion is believed to be the reasons (Lamina, Reference Lamina2015). The study revealed inter-region variation in reasons for abortion, which conforms to an earlier study by Bose and Trent (Reference Bose and Trent2006). The Central, Eastern, and North-Eastern regions had much higher rates of abortion due to unintended pregnancies, whereas the Southern region had significantly lower rates than the Northern region. These regional disparities may result from cultural factors and variances in the quality and accessibility of family planning services (Dixit et al., Reference Dixit, Ram and Dwivedi2012).
The study found that medicine was strongly linked to sex-selective abortions, which were more frequently performed at home. Again, women aborting for sex-selective reasons is associated with an increasing number of surviving children. This finding is consistent with a past study that revealed that most sex-selective abortions occurred when only one or two children were alive (Ganatra et al., Reference Ganatra, Hirve and Rao2001). Sex-selective abortion was more prevalent among women who did not know the ovulatory cycle correctly. The most likely explanation is that highly educated women have a low preference for sons than those with low/no education (Bhalotra & Cochrane, Reference Bhalotra and Cochrane2010; Clark, Reference Clark2000; Pande & Astone, Reference Pande and Astone2007; Sinha & Yoong, Reference Sinha and Yoong2009), and the latter will initially have inaccurate knowledge about the ovulatory cycle. Our research revealed that sex-selective abortions were more prevalent among Hindu women, but other studies had varying findings (Bhat & Zavier, Reference Bhat and Zavier2003; Nanda et al., Reference Nanda, Abhishek, Ravi, Aarushi, Nizamuddin, Dhanashri, Shobhana and Sanjay2014; Robitaille & Chatterjee, Reference Robitaille and Chatterjee2018). This study found that women from the lowest wealth quintile were more likely to have an abortion due to sex-selective reasons, which is similar to earlier studies that found women from higher income groups with low son preference (Bhalotra & Cochrane, Reference Bhalotra and Cochrane2010; Bhat & Zavier, Reference Bhat and Zavier2003; Nanda et al., Reference Nanda, Abhishek, Ravi, Aarushi, Nizamuddin, Dhanashri, Shobhana and Sanjay2014). The country’s Central, Eastern, and North-Eastern regions had much higher rates of sex-selective abortion, consistent with a past study (Abbamonte, Reference Abbamonte2019). The desire for a male child persists despite India’s ongoing efforts to improve women’s status in society and develop programmes to increase the worth of the girl child because of a combination of detrimental societal practices and conventions which cause gender bias and imbalances, which in turn cause infanticide, female feticide, and the neglect of young girls (Chakravarty et al., Reference Chakravarty, Dabla, Sagar, Neogi, Markan, Segan, Agnani, Kapahi and Neogi2022). A study from Nepal reveals that sex-selective abortion is an increasing problem, and the high value placed on sons is a major contributing factor (Lamichhane et al., Reference Lamichhane, Harken, Puri, Darney, Blum, Harper and Henderson2011).
The strength of this study is the thorough description of the pattern and determinants of the reasons for abortion in India using data from a recent nationally representative household survey with a robust sampling design. The findings are current and pertinent for policy and programme interventions focusing on providing comprehensive abortion care. Understanding why women have abortions increases our understanding of how women’s socioeconomic status and demographic characteristics relate to those reasons. However, the cross-sectional design of the survey limits the causal association between the predictors and outcome variables included in the analysis. Reasons for abortion in the five years preceding the survey are self-reported, thus prone to recall bias. Moreover, social desirability response bias cannot be ruled out as abortion continues to be a sensitive issue. ‘Mother-in-law/husband did not want’ as a reason for abortion has been clubbed under sex-selective abortion with the assumption that they are sex-selective abortion, although there may be exceptions. The NFHS 5 survey’s second phase covering almost half of the country occurred during the COVID-19 pandemic when women were perceived to have restricted access to various reproductive healthcare services. This may also have influenced the study’s findings.
Women had abortions mainly due to unintended pregnancies, and there was socioeconomic, demographic, and geographic variation in the reasons for abortion in India. Sex-selective abortions continue to exist, especially among women of higher parity, poorest households and from the central, eastern, and north-eastern regions. The key to reducing unintended pregnancies and abortions is raising the understanding of contraception and empowering women in reproductive decisions. Reducing unintended pregnancies will contribute to lower induced abortion and thus improve women’s health. Reduced induced abortions will further help achieve the sustainable development goals, which include reducing maternal mortality, ensuring reproductive rights, and achieving universal access to sexual and reproductive health information, education, and services.
Acknowledgements
None.
Funding
This research received no specific grant from any funding agency, commercial entity, or not-for-profit organisation.
Competing interest
The authors have no conflicts of interest to declare.
Ethical approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.






