


Anthropometric references are useful tools to assess the general health status and growth process in children and adolescents. Subcutaneous fat deposition is used as an energy store and reflects the body’s nutritional status. On the other hand, subcutaneous fat deposition is influenced by gender, chronological age, stage of maturation and nutritional status(Reference Harsha, Voors and Berenson1,Reference Shalitin and Phillip2) . Assessment about total body fat deposition with anthropometric measurements is considered as an easy and reliable method. Local differences in growth and nutritional status of children and adolescents have been shown by several studies(Reference Freedman, Dietz and Srinivasan3,Reference Nooyens, Koppes and Visscher4) . A previous study indicates that there is a relationship between childhood adiposity and adulthood cardiometabolic risk related to body composition. These disorders can be listed as primarily diabetes mellitus and CVD(5).
Marie et al. reported that the prevalence of childhood overweight and obesity has increased both in developed and developing countries, and in the adolescent period, approximately 50 % increase was seen in these figures between 1980 and 2013 in several regions(Reference Marie, Fleming and Robinson6). Although the WHO aims to decrease prevalence of obesity in 2020, Turkey is listed in European countries where childhood and adolescent obesity is still prevalent(7). Turkey Childhood Obesity Surveillance Initiative (COSI-TUR 2013) showed that 8·3 % and 14·2 % of children and adolescents were obese and overweight(8). Only 3 years later, these figures were given as 9·9 % and 14·6 % for obese and overweight, respectively, in COSI-TUR 2016(9).
Although there are several methods such as bioelectrical impedance analysis, dual-energy X-ray absorptiometry, MRI, hydrodensitometry and ultrasound to assess body fat composition and distribution. Almost all of them are expensive, needs time-consuming procedures, may expose children to radiation and not easy to be used in paediatric examination procedures or screening(Reference Noradilah, Ang and Kamaruddin10–Reference Brannsether, Roelants and Bjerknes12). There are several anthropometric measurements including BMI, waist circumference and skinfold thickness to assess obesity and determine body fat composition(Reference Casadei and Kiel13).
Skinfold thickness measurements are non-invasive, simple and less expensive than other laboratory-based methods thus provide a useful and reliable estimate for body fat composition and distribution(Reference Wang, Cheng and Chen14–Reference Bedogni, Iughetti and Ferrari18). Additionally, a significant correlation between increased skinfold thickness and increased levels of cardiometabolic disease risk and metabolic syndrome has been reported(Reference Steinberger, Jacobs and Raatz19–Reference Laurson, Eisenmann and Welk21).
One of the most frequently used skinfold thickness estimation equations is developed by Weststrate and Deurenberg et al. that predict total body fat from triceps and subscapular skinfold thickness’s(Reference Weststrate and Deurenberg22). However, it is also stated that ethnic variations may alter skinfold thickness references significantly(Reference Wells and Fewtrell23).
Since skinfold thickness is a reliable and useful tool to assess body fat composition, it is crucial to rely on standardised measurement techniques for skinfold thickness. The Lambda, Mu, Sigma (LMS) method is accepted as a reliable method to get smoothed percentiles of skinfold thickness as in the case of most anthropometric measures. L, M and S represent the skewness (lambda), median (mu) and CV (sigma) curves, respectively(Reference Cole and Green24). Its interobserver error was reported as <2–3 % for skinfold thickness measurement for experienced healthcare workers(Reference Durnin, De Bruin and Feunekes25).
Skinfold thickness is considered as a useful tool in screening childhood growth together with other anthropometric measurements(Reference Owen26). In Turkey, there are very limited data about skinfold thickness and for most of the geographic regions. A comprehensive study was conducted on 4285 participants in a metropolitan city Kayseri, which is located in Central Anatolia(Reference Çiçek, Özturk and Ünalan27). The current study may provide useful information primarily about Central Anatolia. The present study has provided the data for Western Turkey 10 years after the Central Anatolian study.
The aim of the current study was both to update national skinfold thickness references and provide data about the western part of Turkey. Triceps, biceps, subscapular and suprailiac skinfold data were converted into smoothed references with the LMS method and calculated data was compared with previous national and international data to assess body fat composition and was elaborate a reference for the percentage of body fat, in 6- to 18-year-old children and adolescents in Afyonkarahisar, Turkey.
Methods
Study design
This cross-sectional descriptive study was conducted on 4565 students aged 6 to 18 years between January and May 2017 in Afyonkarahisar/Turkey.
Place
Afyonkarahisar is a city located on the border of Central and Western regions of Anatolia at an altitude of 1034 m and has 725 568 inhabitants. In the current study, Afyonkarahisar was chosen because its demographic and geographic structure which are similar to Turkey(28), and the research team was located in this province and/or in the immediate vicinity.
Participants
In the 2016–2017 academic year, the total number of children between the ages of 6 and 18 was 137 350. The stratification of the final sample size was done according to the socio-economic level of parents and their proportion in the general population. The seven primary, thirteen secondary and fifteen high schools were randomly selected, and the study sample size was reached at these thirty-five schools. Lack of family consent, students’ refusal, in attendance to school for several reasons were caused od data loss so that study was conducted with 4565 students consisting of 2133 (46·6 %) boys and 2432 (53·1 %) girls. This final sample size was corresponded to 3·3 % of the students in this age group in Afyonkarahisar/Turkey.
Students’ health status was questioned by their parents, educators and health records if available. Those who have any metabolic or chromosomal disorder, using drugs that may alter their growth and development, older than 18 or less than 6 years of age were excluded from the study.
Data collection
The data of the students were collected through a questionnaire filled in by the parents of the students. The questionnaire consisted of questions including socio-demographic characteristics, health status, previous diseases and medications used, etc.
Anthropometric measurements were performed by a trained team consisting of twelve healthcare staff but skilled three personnel measured only the skinfold thicknesses of the students. Others were assigned to make the length and weight measurements. The study team was trained in the pre-study period, about how to make anthropometric measurements. The 5 d long training programme was composed of theoretical information and practice of anthropometric measurements. In the post-training period, a pilot study was carried out in a school, allowing each team member to perform at least fifty practices. Data obtained from the pilot study were not included in the study.
Two expert observers checked measurement techniques and corrected them during the whole study.
Anthropometric measures
Measurements were done in the morning hours, between 7:00 and 10:00 a.m. Attention was paid to privacy during taking anthropometric measurements of children, and measurements were made in a private room with two personnel. Children were informed before taking the measurements.
Skinfold thickness was measured using Holtain skinfold caliper (Holtain Ltd., United Kingdom) with dial graduation of 0·2 mm. The study team was taught the calibration method and the application standardisation of the measuring instruments and calibration materials to be used during the application was provided.
The four sites of measurement were marked carefully before measurement. Triceps skinfold was measured over the midpoint of the triceps muscle between the olecranon-process and the acromion, as the biceps skinfold was measured at the same point, but in the anterior line of the arm. The subscapular skinfold was measured just below the scapula at an angle of 45° to the lateral side of the body and finally the suprailiac was measured with the natural angle of the iliac crest at the anterior axillary line(Reference Marfell-Jones, Stewart and Carter29,Reference Harrison, Bushkirk, Carter, Lohman, Roche and Martorell30) .
All measurements of the adipose folds were taken on the right side of the body and were made twice by the same person, and but second scores were made after the first set of all measurements was completed to avoid memory bias. The third measurement was taken when there was 1 mm difference between the two measurements and averages were calculated later. Intra- and inter-rater technical errors of measurement were within published reference ranges for all of the measurements(Reference Harrison, Bushkirk, Carter, Lohman, Roche and Martorell30).
Skinfold thicknesses and body fat percentages were grouped by age and gender.
Data analysis
Descriptive statistics, numbers and percentages for the categorical data, arithmetic mean and sD (S) values were calculated for the anthropometric measurements. In all analyses, α = 0·05 was chosen as the level of error. SPSS 20.0 software for the windows program was used. The age was calculated for the date of measurement. The smoothed 3rd, 5th, 10th, 25th, 50th, 75th, 90th, 95th and 97th percentiles curves for each gender and age were produced. This is a cross-sectional profile.
We used the LMS method described by Cole and excluded the extreme values in data analysis(Reference Cole and Green24,Reference Öztürk, Budak and Çiçek31) . Body fat percentage was calculated with the Westrate and Deurenberg equation(Reference Weststrate and Deurenberg22).
Results
Some socio-demographic characteristics of children were presented in Table 1. According to this, the education level of the mothers of the children was lower than the fathers, and most of them were housewives. Monthly income of 31·4 % of fathers is below the minimum wage.
Table 1 Some socio-demographic characteristics of children*

* n is the people who answered this question.
† In 2017 when the research was carried out, Net Minimum Wage was 1·404 Turkish Liras, and 1 Dollar was equal to 3·7412 Turkish Liras (Central Bank of Turkey).
Smoothed age- and sex-specific percentiles and L, M, S values for triceps and biceps skinfold thickness (mm) were presented in Tables 2 and 3.
Table 2 Smoothed age- and sex-specific percentiles and L, M, S values for triceps skinfold thickness (mm)

Table 3 Smoothed age- and sex-specific percentiles and L, M, S values for biceps skinfold thickness (mm)
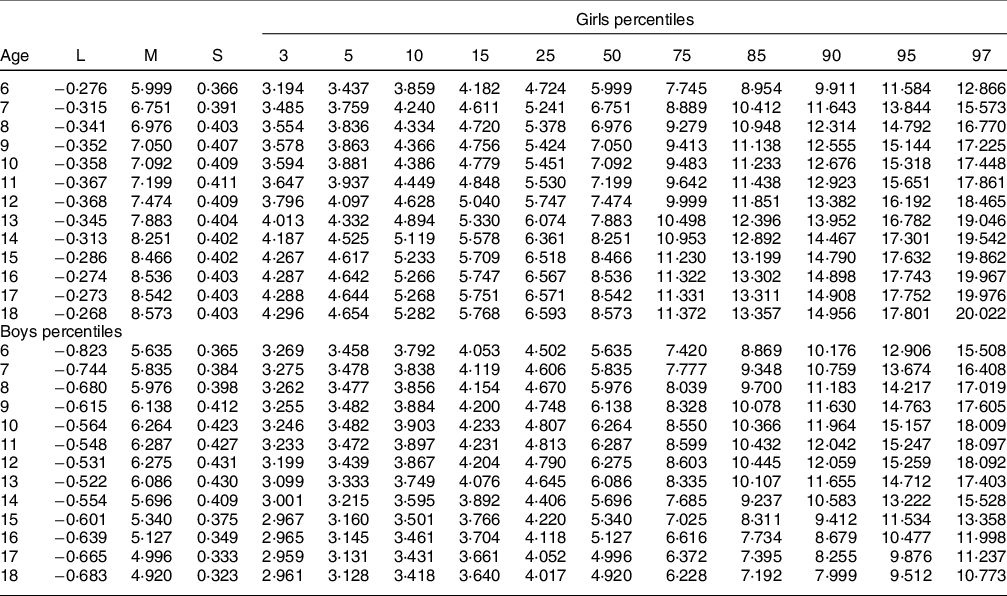
There was a steady increase in triceps and biceps skinfold thickness of girls, from 6 to 18 years of age, in all percentiles. In boys, increase in triceps and biceps skinfold thickness peaked at 12 years old then decreased gradually. In particular, this decrease in the 97th percentile of boys’ biceps was quite evident. The triceps skinfold thickness percentiles in the preadolescent period increased significantly. However, triceps and biceps skinfold thickness values of the 18-year-old boys were lower than 6-year-old boys.
In all age groups, girls’ triceps and biceps skinfold thickness were higher than boys. The 50th percentile triceps skinfold thickness of boys ranged from 8·8 mm to 12·2 mm through 6–18 years and biceps skinfold thickness ranged from 4·9 mm to 6·3 mm. Triceps skinfold thickness ranged from 10·5 mm to 17·4 mm, and biceps skinfold thickness ranged from 6 mm to 8·6 mm in girls (Tables 2 and 3).
Increases in subscapular and suprailiac skinfold thicknesses with increasing age were observed in both girls and boys. In boys, decreases in subscapular skinfold were observed in the 97th percentile over 13 years, 95th percentile over 15 years and 90th percentile over 17 years. The subscapular skinfold thickness of 6-year-old boys for 97th percentiles at 16 years was lower than those of 6-year-old boys. There was no such similar difference in girls’ percentiles. The subscapular and suprailiac skinfold thicknesses of the girls were higher than boys, other than the 97th percentile. We found that girls’ suprailiac skinfold thickness decreased over 14 years of age for 97th and over 16 years for 95th percentile. The subscapular skinfold thickness through 6 to 18 years of age ranged from 17·2 mm to 16·5 mm and 18·9 to 26·8 mm in boys and girls, respectively. The corresponding suprailiac skinfold thicknesses ranged from 22·3 mm to 28·1 and 19·6 mm to 27·4 mm for boys and girls, respectively (Tables 4 and 5). In 18-year-old obese children, the subscapular skinfold was between 16·5 mm and 26·8 mm, respectively, for boys and girls. The subscapular skinfolds were much higher in girls indicating a higher level of subcutaneous adiposity than boys.
Table 4 Smoothed age- and sex-specific percentiles and L, M, S values for subscapular skinfold thickness (mm)
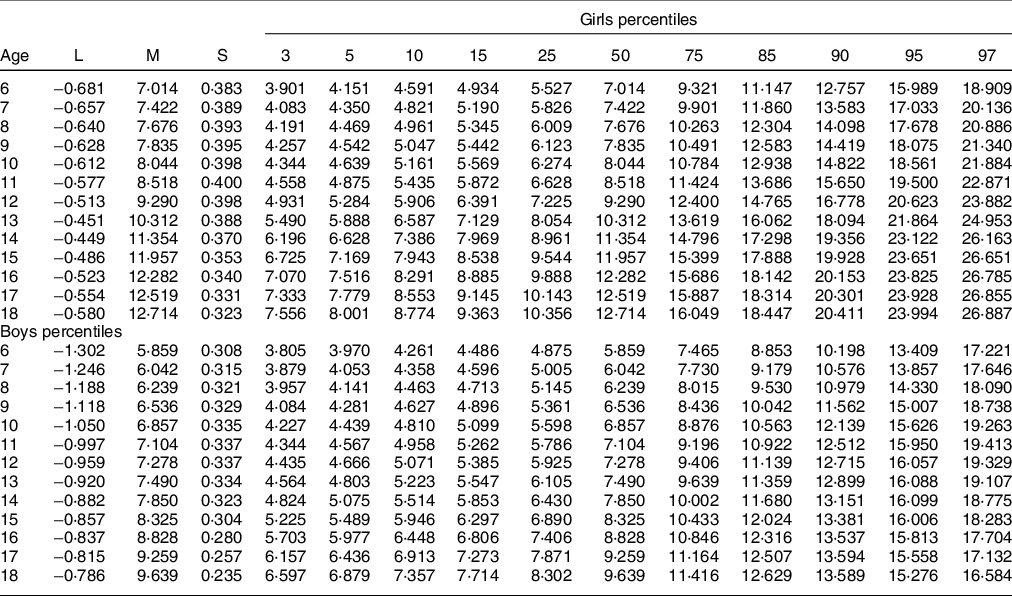
Table 5 Smoothed age and sex-specific percentiles and L, M, S values for suprailiac skinfold thickness (mm)
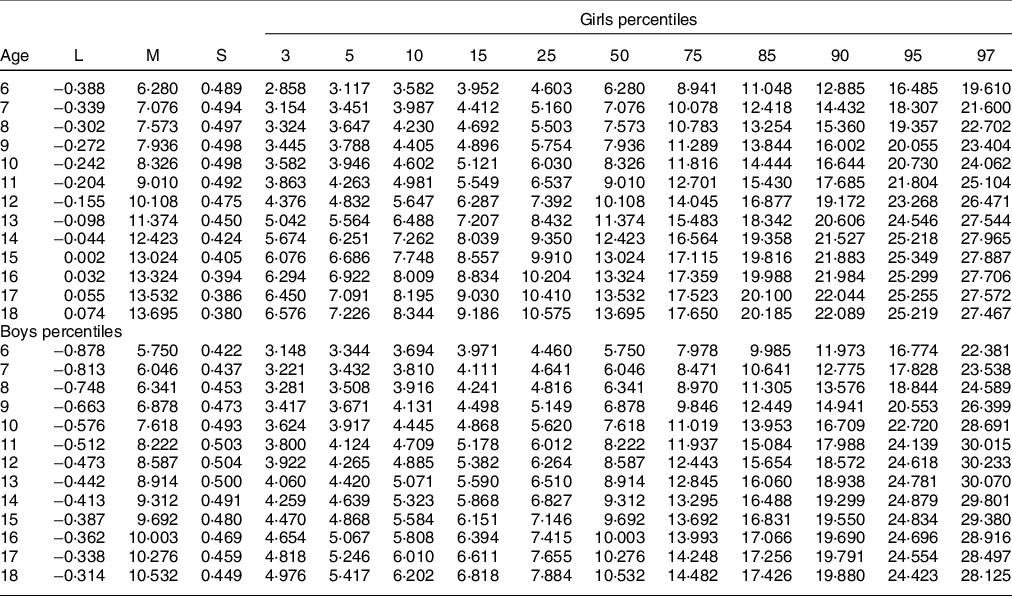
Table 6 shows the variation in subcutaneous fat with increasing age in both genders. The sum of four skinfold thicknesses in girls increased with age, and it was prevalent during the adolescent period. However, in adolescent boys, skinfolds thickness decreased particularly in the 75th percentile and over. The sum of four skinfold thicknesses of the girls was higher than the boys (P < 0·001). This difference became more evident after the age of 12. The sum of four skinfold thicknesses of boys through 6 to 18 years of age ranged from 27·1 mm to 34·4 mm in the 50th percentile. The corresponding change through 6 to 18 years of age girls for the four-site skinfold thicknesses ranged from 30·4 mm to 53·2 mm (Table 6).
Table 6 Smoothed age- and sex-specific percentiles and L, M, S values for sum of four skinfold (mm)

Body fat percentiles of girls fluctuated. A decrease from 7 to 12 years of age then increases until the age of 15 years followed by a gradual decrease. However, the body fat percentiles of boys were more consistent, and they gradually decreased with the increasing age. We found that the fat percentiles of the girls were lower than the fat percentiles of the boys until the age of 12, it then increased so that exceeds the boys. The 50th percentile of body fat percentages ranged from 17·9 mm to 19·7 mm and from14·8 mm to 18·5 mm for girls and boys, respectively (Table 7).
Table 7 Smoothed age- and sex-specific percentiles and L, M, S values for body fat percentage

The mean values of triceps, biceps, subscapular and suprailiac skinfold thicknesses of girls were higher than boys in all ages except 6 years; the gender difference was significant (P < 0·001) (Table 8). Similarly, the sum of four skinfold thickness percentiles was also higher in girls except 6 years of age (P < 0·001). However, body fat percentages of girls estimated by Westrate and Deurenberg equation were lower than boys, but it increased in contrast to the decline observed after 12 years of age boys but higher than that of boys (P < 0·001) (Table 9).
Table 8 The mean values and sexual dimorphism of the subcutaneous skinfolds
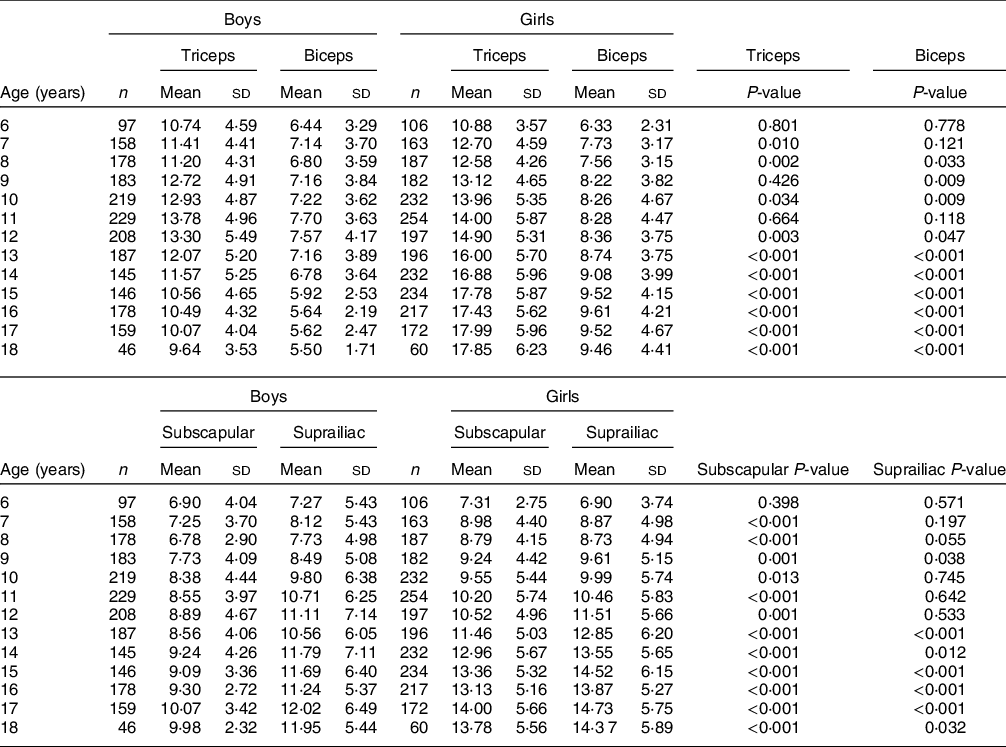
Age: Indicates the period after the completed age to the last date of the actual age (e.g. 7 00–7 99 years, etc.).
Table 9 The mean values and sexual dimorphism of the sum of four folds and body fat percentage estimated by Westrate and Deurenberg

Age: Indicates the period after the completed age to the last date of the actual age (e.g. 7 00–7 99 years, etc.).
WD % Fat: Westrate and Deurenberg equation derived % fat.
Discussion
It has been shown that physiologically normal amounts of fat mass vary according to age and gender. Age also affects the distribution of body fat, both genders have equal amounts of central and peripheral subcutaneous adipose tissue in the newborn and infancy period. Although central to peripheral subcutaneous fat distribution remains throughout life in both genders, the lowest central to peripheral tissue body fat mass level was determined in approximately 5 years of age(Reference Rolland-Cachera, Bellisle and Deheeger32,Reference Wickramasinghe, Lamabadusuriay and Cleghorn33) .
It has been reported that the ratio of subcutaneous adipose tissue to fat mass is almost similar in both boys and girls aged 9–15 years. In girls, a decrease is observed in subcutaneous adipose tissue to fat mass ratio during adolescence period and thereafter it remains stable. In boys, an increase is seen until 20 years of age and then a gradual decrease occurs. During adolescence, because boys gain more central subcutaneous adipose tissue than peripheral subcutaneous adipose tissue, adult males have less subcutaneous adipose tissue and more visceral adipose tissue with the increasing age, whereas females gain fat in both areas(Reference Rolland-Cachera, Bellisle and Deheeger32).
Skinfold thickness measurement is frequently used to estimate the body fat percentage(Reference Petkeviciene, Klumbiene and Kriaucioniene20,Reference Haas, Liepold and Schwandt34,Reference Rodrı´Guez, Moreno and Blay35) . Triceps (regional) and subscapular (central) skinfold thicknesses show almost all of the changes in body composition(Reference Brannsether, Roelants and Bjerknes12).
The peripheral subcutaneous adipose tissue distribution calculated from triceps and biceps skinfold thicknesses have shown that peripheral distribution in 6 years of age is the lowest but then it increases with the age(Reference Wickramasinghe, Lamabadusuriay and Cleghorn33). In the present study, triceps and biceps skinfold thicknesses of girls were higher than boys in all age groups. Triceps and biceps skinfold thickness, increased in all percentiles for girls from 6 to 18 years of age, whereas in boys, these two skinfold thicknesses increased gradually from the age of 6 to 12 years then decreased to the levels of 6 years of age. These findings were consistent with the results of the study conducted in Germany by Rönnecke et al. who reported a peak at the beginning of adolescence with a subsequent decrease for biceps and triceps skinfold thicknesses in boys, while a rise among girls percentile values across the age range(Reference Rönnecke, Mandy and Busslera11). The increasing trend in girls and the pubertal peak in boys were also observed in the USA(Reference Addo and Himes36), German(Reference Wickramasinghe, Lamabadusuriay and Cleghorn33,Reference Kromeyer-Hauschild, Glässer and Zellner37) , Polish(Reference Jaworski, Zbigniew and Pludowski38) and Norwegian children(Reference Brannsether, Roelants and Bjerknes12). Our results also similar to the data reported by Velez et al. from Colombia(Reference Vélez, Cifuentes and Bautista39) and by Nagy et al. (Reference Nagy, Kovacs and Moreno40) from different European countries where girls had higher percentiles triceps skinfold thickness than boys.
Previous studies have shown that there is a steady increase in subscapular skinfold thickness in both genders through 9 to 14 years of age in some geographic areas.(Reference Kromeyer-Hauschild, Glässer and Zellner37,Reference Palczewska and Niedzwiedzka41) In the present study, regarding the subcutaneous body fat distribution, the 97th percentile subscapular skinfold thickness in boys over 16 years of age was lower than those of 6 years old. However, we could not find a similar difference in girls. When compared with boys, higher subscapular and suprailiac skinfold in girls were also determined by previous studies(Reference Brannsether, Roelants and Bjerknes12,Reference Haas, Liepold and Schwandt34,Reference Addo and Himes36,Reference Jaworski, Zbigniew and Pludowski38) . The increase in the distribution of central adipose tissue measured by subscapular and suprailiac skinfold thickness in Sri Lankan children was reported to be prominent in girls(Reference Wickramasinghe, Lamabadusuriay and Cleghorn33). In our study, much higher subscapular skinfold thickness values were obtained in girls that indicate girls have a higher level of subcutaneous adiposity than boys.
We made cross-cultural comparisons of the 50th percentile triceps and subscapular skinfold thickness percentiles with Colombia(Reference Ramírez-Vélez, López-Cifuentes and Correa-Bautista15), Spain(Reference Moreno, Mesana and Gonzalez-Gross42), Germany(Reference Rönnecke, Mandy and Busslera11,Reference Haas, Liepold and Schwandt43) , Norway(Reference Brannseether, Roelants and Bjerknes44) and the USA(Reference Addo and Himes36). This comparison showed that both boys and girls in Afyonkarahisar had higher values for triceps and subscapular skinfolds in all of the age groups than the children in Norway(Reference Brannseether, Roelants and Bjerknes44), Germany(Reference Haas, Liepold and Schwandt43) and USA(Reference Addo and Himes36) and higher values for triceps and subscapular skinfolds in girls of all of the age groups than German girls(Reference Rönnecke, Mandy and Busslera11) but has lower 50th percentile triceps and subscapular skinfold thickness percentiles than the Colombian(Reference Ramírez-Vélez, López-Cifuentes and Correa-Bautista15) and Spanish(Reference Moreno, Mesana and Gonzalez-Gross42) children and adolescents. These results indicate that there may be differences between different ethnic groups concerning both triceps and subscapular skinfolds.
Our findings indicate that the sum of the four skinfold thicknesses of the girls was higher in boys over 7 years of age. This difference became more apparent over 12 years of age. This finding in our study was similar to a study conducted in Germany(Reference Rönnecke, Mandy and Busslera11).
We found that the triceps and subscapular skinfold thickness of girls were higher than boys in all age groups boys. This was similar to the results of the study performed by Kromeyer-Hauschild et al. on a population of 2132 boys and girls in the city of Jena, Germany(Reference Kromeyer-Hauschild, Glässer and Zellner37). In another study conducted by Marrodán et al. in five countries (Argentina, Cuba, Mexico, Spain and Venezuela), four-site skinfolds of girls were detected as greater than boys(Reference Marrodan, Espinosa and Herraez45). The study by Addo and Himes(Reference Addo and Himes36) and Aristizabal et al. (Reference Aristizabal, Barona and Hoyos46) reported similar results with our findings in those girls had higher triceps and subscapular skinfold thickness than boys through 6–18 years old.
Our results were also similar to the limited number of previous studies in Turkey. In the study of Öztürk et al. conducted on 5553 students aged 6 to 17 years in Kayseri (Turkey), it was reported that the mid-upper arm circumference, triceps skinfold thickness and arm fat area and fat percentage in each age group were significantly higher in girls than in boys(Reference Öztürk, Budak and Çiçek31). In another study conducted in Kayseri by Çiçek et al., the overweight category of boys was found as 9–11·9 years of age(Reference Çiçek, Özturk and Ünalan27). Similar to our results, the peripheral skinfolds of girls increased with the advancing age. They found an increase in peripheral skinfolds of boys up to 10 years and thereafter they detected a gradual decrease. However, in our study, increases in peripheral skinfolds were detected in boys through 6 to 12 years and then it decreased gradually.
In the current study, triceps values (except 97th percentile) in all percentiles of 17-year-old girls and subscapular percentile values of 85th and above for all ages were found higher than the values determined in the study conducted in 2008 in Kayseri(Reference Çiçek, Özturk and Ünalan27). On the other hand, 50th percentile of triceps and subscapular skinfold thickness of boys through 6 to 16 years were higher than the values determined in Kayseri.
The results of the present study may show that the rate of adiposity in children increases in Turkey since 2008, or these differences between our study and previous studies may be due to heterogeneity in the timing of data collection, ethnic distribution and statistical methodology.
Schwandt et al. calculated the body fat percentage of children aged 3 to 18 years in Nuremberg(Reference Schwandt, Eckardstein and Haas47). Their findings showed a higher median body fat percentage in girls than in boys, and the body fat percentage peak that occurred in 11-year-old boys was similar to our findings. The means of triceps, biceps, subscapular and suprailiac skinfold thickness as well as the mean of the sum of four skinfold thickness were higher in girls of our study group when compared with boys except the age of 6 years was similar to the findings of Çiçek et al. (Reference Çiçek, Özturk and Ünalan27) Increase in body fat percentage is the evidence of obesity risk for children and adolescents(Reference Çiçek, Özturk and Ünalan27). In the current study, we calculated body fat percentages with the Westrate–Deurenberg equation and when compared with boys, girls had lower body fat percentage before the adolescence period and body fat percentage tended to increase and exceeded that of boys after 12 years of age. Çiçek et al. also reported similar trends both in girls and boys and a peripheral (subcutaneous) rather than central (visceral) fat deposition in children and adolescents(Reference Çiçek, Özturk and Ünalan27).
According to the Ministry of Health, obesity and overweight have become a dramatic problem in the last decade in Turkey. Compared to 2010, the overweight (64·9 %) and obesity (70·7 %) ratio of adults increased in Turkey Nutrition and Health Survey-2017. In 2017, the ratio of obesity was higher among women than in men (42·6 %, 26·3 % respectively)(48,49) . The current study has also shown that the basis of obesity begins in childhood and adolescence and girls at higher risk of obesity in Turkey.
There are some limitations of the current study. Collection of data from a single province may be regarded as a limitation, but this particular province represents certain characteristics of a specific region (West of Central and East of Aegean region of Anatolia the Turkish mainland). Additionally, the puberty stages of children affecting body composition could not be determined due to the large sample size. Another limitation, the nutritional profile and physical activity of children/adolescent could not be evaluated due to the large sample size and the need for long time and specialized methods and trained personnel.
Conclusions
The results of the current study have provided gender- and age-specific reference values for skinfold thickness in children and adolescents of Afyonkarahisar, Turkey. The smoothed LMS curves of girls were high in girls when compared with boys for triceps and subscapular skinfold thickness independent of age that indicates higher adiposity in girls than in boys. Our findings may be used both to compare adiposity with different locations and construct a cause relationship for several independent variables to explain high adiposity in children and adolescents. These additional findings may contribute to developing preventive measures.
Acknowledgements
Acknowledgements: The authors thank everybody in the team especially Gamze Soykan, Kübra Gedik and Gamze Taşdemir for taking skinfold thickness measurements and all students and parents for their participation. The authors are grateful to the Afyonkarahisar Directorate of National Education and their teachers for their cooperation. Financial support: The current study was supported by Afyon Kocatepe University Scientific Research Projects Commission Presidency (Project no: 15.HIZ.DES.114). The funding agencies had no role in the design, analysis or writing of this article.The equipment used in the project and study teams finances (travelling, meal, etc) were covered by the funder. Conflict of interest: There are no conflicts of interest. Authorship: Creating the hypothesis and idea of the manuscript: N.Ş. and M.S. Designing the method that will achieve results: M.S., N.Ş., A.Ö. Organising the conduct of the research: N.Ş., İ.D., N.D. Collecting, organising and reporting data: N.Ş., M.S., İ.D., N.D. Evaluating and concluding the findings: M.S., N.Ş., A.Ö., İ.D., M.M.M. Scanning resources required for the study: M.S., N.Ş., N.D. Writing the whole or important parts of the manuscript: M.S., N.Ş., M.M.M. Making a critical review: N.Ş., M.M.M. Ethics of human subject participation: Ethics committee approval was obtained from the Eskişehir Osmangazi University Ethics Committee (80558721/G-176). All procedures involving research study participants were approved by the Eskişehir Osmangazi University, Clinical Research Ethics Committee. The current study was carried out following the latest version of the Helsinki Declaration. Necessary written permission was obtained from the Afyonkarahisar Directorate of National Education for the study to be conducted in schools (Number: 86649407-605-E-11729885). School administrators and teachers were informed about the research. All students and also their parents were informed about research and practice, and the ‘Enlightened Written Consent Form’ was received from students themselves aged 18 and from the parents of students under 18 years old. Attention was paid to privacy during taking anthropometric measurements of children, and measurements were made in a private room with two researchers.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980021003323











