



Introduction
According to the World Health Organization (WHO), palliative care is a medical specialty given to improve the quality of life of patients who face physical, psychological, social, or spiritual difficulties of life-threatening diseases, and their families. Approximately 40 million people need palliative care annually. More than half of these people live in low- and middle-income countries. Worldwide, only 14% of people who need palliative care can benefit from these services (WHO 2022). Due to the lack of trained palliative specialists, national and international programs, policies, and resources, access to palliative care is inadequate. The need for palliative care is increasing as a global need due to the increased burden of the aging of the population, the presence of some noninfectious diseases, and the recent increase in some infectious diseases. Early delivery of palliative care reduces unnecessary hospitalizations and the burden on healthcare services. Palliative care is a basic need and human right that should be ensured for all people, regardless of income, age, sex, race, religion, and disease (Çamcı and Oğuz Reference Çamcı and Oğuz2018; Reference Çamcı and Oğuz2023; WHO 2022). In palliative care centers, the aim is to improve the quality of life of terminal patients, relieve their pain, provide psychological support to patients and their relatives, and enable patients to spend their time with less pain (Enginyurt Reference Enginyurt2019).
Patients have the right to have adequate and accurate information about their illnesses. The right to have this information has been declared at the global level in the Universal Declaration of Bioethics and Human Rights and approved by UNESCO on 19 October 2005, based on the Universal Declaration of Human Rights dated 10 December 1948 (UNESCO 2005). In Turkey, according to the regulation of patient rights, doctors have the authority to hide the diagnosis “in cases where there is a possibility of worsening in the disease that would negatively affect the moral structure of the patient and the course and outcomes of the disease” (Patient Rights Regulation 2016). Relatives of palliative care patients may hide some information about their patients or misrepresent their disease to make patients feel psychologically, spiritually, and physically better. In particular, terminal patients are prevented from accessing real information (de la Piedra‐Torres et al. Reference de la Piedra‐torres, López‐Martínez and Ramírez‐Maestre2022; Martín-Fortea et al. Reference Martín-Fortea, de Fernando-gros and Longas-Gaspar2020). Some patient relatives hide only the diagnosis from their patients, whereas others hide both the diagnosis and the prognosis (Alfaya-Góngora et al. Reference Alfaya-Góngora, Sánchez-Ojeda and Má2021). However, it has been reported that information concealment has adverse psychological effects on patients such as increased pain, decreased autonomy, depressive symptoms, lack of control, fear, suffering, lack of communication, isolation, and feelings of loneliness and deception (Lemus-Riscanevo et al. Reference Lemus-Riscanevo, Carreño-Moreno and Arias-Rojas2019; Tuca et al. Reference Tuca, Viladot and Barrera2021). This study was planned to establish the validity and reliability of the Turkish version of the Information Concealment Scale for Caregivers of palliative care patients.
Method
Research objective
This methodological study aimed to establish the validity and reliability of the Turkish version of the Information Concealment Scale for Caregivers of palliative care patients.
Research place and time
The study was carried out between January and June 2023 with patient relatives who give care to patients hospitalized in the palliative care units of a state hospital and a training and research hospital in Istanbul, Turkey.
Research population and sample
It has been stated that the sample size should be at least 5–10 times the number of scale items to perform factor analysis in validity and reliability analyses (Esin Reference Esin, Erdoğan, Nahcivan and Esin2021; Karakoç and Dönmez Reference Karakoç and Dönmez2014). Since the Information Concealment Scale for Caregivers consists of 15 items, the aim was to reach at least 150 people. During the study dates, 155 caregivers who met the inclusion criteria were reached. The inclusion criteria of the study were being aged over 18, having no problem that would prevent answering questions (such as vision, hearing, language, etc.), and signing the informed consent form.
Data collection method and tools
A general information form and the Turkish version of the Information Concealment Scale for Caregivers were used for data collection. Data were collected face-to-face in the patient’s or waiting rooms. Data collection took 10–15 minutes for each caregiver.
General information form
The general information form was prepared by reviewing the literature (de la Piedra‐Torres et al. Reference de la Piedra‐torres, López‐Martínez and Ramírez‐Maestre2022; Tuca et al. Reference Tuca, Viladot and Barrera2021) and consists of 7 questions regarding demographic information (economic status, age, sex, etc.).
Information Concealment Scale for Caregivers
The scale was developed by de la Piedra‐Torres et al. (Reference de la Piedra‐torres, López‐Martínez and Ramírez‐Maestre2022) and consists of 15 items that are ranked on a 4-point Likert-type scale as 0 = Never, 1 = Sometimes, 2 = Often/Usually, and 3 = Always. Items 2 and 3 are reverse scored (the equivalent of 0 is 3 or vice versa). The scale has 3 subscales: concealment about the disease, misrepresentation of the condition, and control of information. A high score on the scale indicates that the level of information concealment is high. The Cronbach’s α of the scale is 0.90 (de la Piedra‐Torres et al. Reference de la Piedra‐torres, López‐Martínez and Ramírez‐Maestre2022).
Ethical consideration
Verbal and written consent was obtained from the participants. To conduct validity and reliability analyses, permission was received via e-mail from the corresponding author (Antonio J. de la Piedra-Torres), who developed the Information Concealment Scale for Caregivers. Ethical approval was taken from the non-invasive clinical research ethics committee of Marmara University Faculty of Health Sciences (29.12.2022/131).
Data evaluation
The SPSS (Statistical Package for Social Sciences) package program and the trial version of the AMOS 24 program were used in the analysis of the research data. Descriptive statistical methods (number, percentage, mean, standard deviation) were used to evaluate the data. Content validity and construct validity were performed in the validity analysis. The Information Concealment Scale for Caregivers was translated from English to Turkish by 2 linguists. Two faculty members compared translations and a draft inventory was obtained. Eight experts evaluated the Draft Inventory. The scale items were revised based on the feedback of the experts. A pilot study was conducted with 10 caregivers. Later, 2 different linguists back translated the Draft Inventory from Turkish to English. The final version of the scale was used in the study. Exploratory factor analysis and confirmatory factor analysis were performed for construct validity. In the exploratory factor analysis, the Kaiser–Meyer-Olkin (KMO) and Bartlett sphericity tests were performed to check the fitness of the sample size for factor analysis. Direct oblimin rotation was used since the correlation between the factors was >0.30 (Çapık et al. Reference Çapık, Gözüm and Aksayan2018; Esin Reference Esin, Erdoğan, Nahcivan and Esin2021). The fit index (CMIN/df, RMSEA, RMR, and GFI) of the model was evaluated with confirmatory factor analysis (Levine Reference Levine, Berger, Roloff, Wilson, Dillard, Caughlin and Solomon2015). Cronbach’s α, item-total correlation, intraclass correlation coefficient (ICC), and Pearson correlation analysis were used for reliability analyses. A value of ≥0.30 was considered a criterion for item-total correlation. A value of >0.7 was considered appropriate for Cronbach’s α and ICC values (Souza et al. Reference Souza, Alexandre and Guirardello2017).
Results
Of the participants, 54.2% were female; 69% were married; 33.5% were primary school-secondary school graduates; 41.3% were high school graduates; 25.2% had a bachelor’s degree; 67.1% were employed; 65.8% had an income equal to their expenses; 12.9% had a chronic disease. The mean age of the individuals was 37.96 ± 12.25 years (Table 1).
Table 1. Sociodemographic characteristics of participants (N:155)
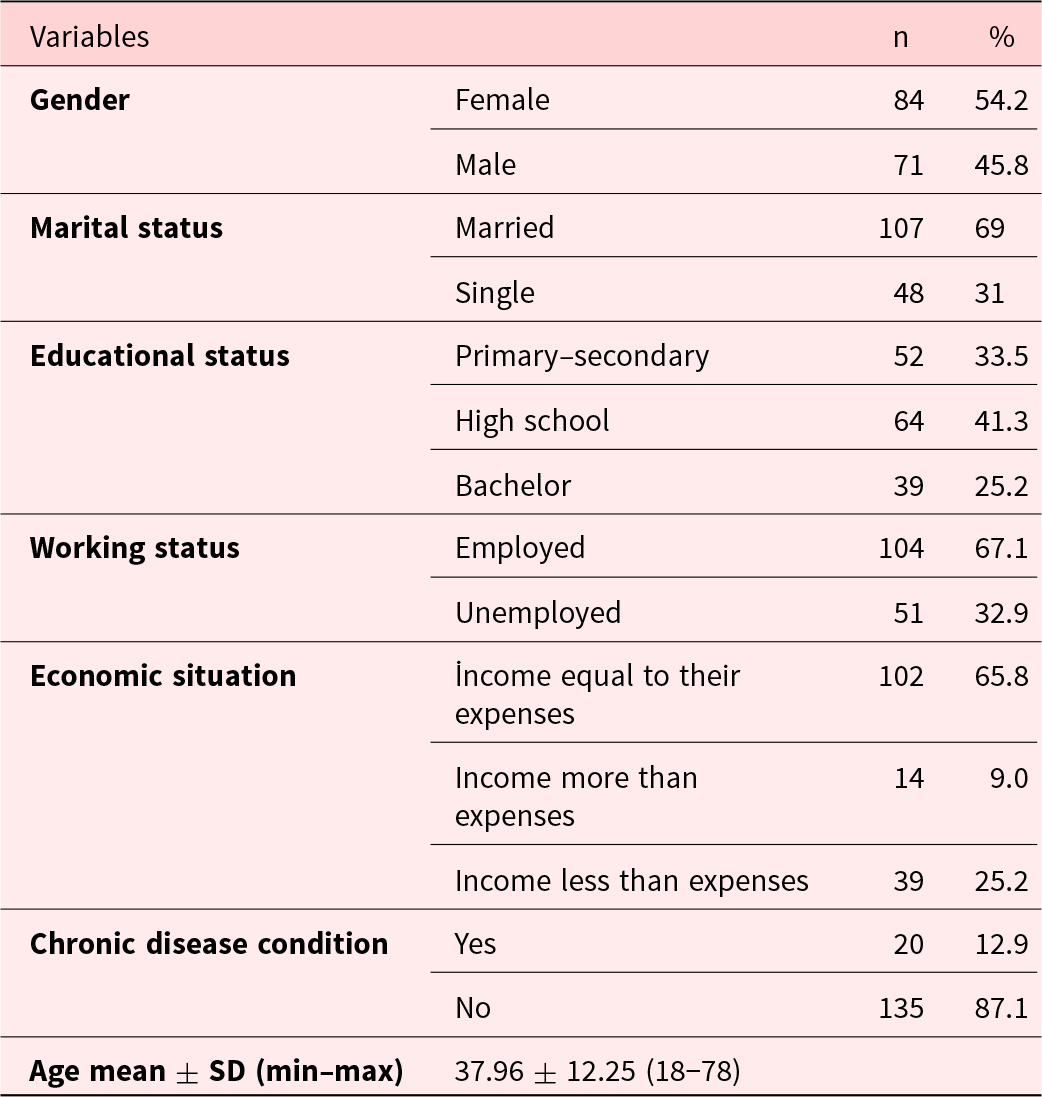
Sd: standard deviation.
Validity
Exploratory factor analysis
The KMO measure value of sampling adequacy was 0.772. The results of Bartlett’s test of sphericity were Approx. Chi-square = 1087.761, df = 105, and p = .001. According to the exploratory factor analysis, the scale consists of 3 subscales. The factor loads of the first factor were between 0.51 and 0.80; the eigenvalue was 4.52; and the explained variance was 30.15%. The factor loads of the second factor were between 0.82 and 0.91; the eigenvalue was 2.75; and the explained variance was 18.34%. The factor loads of the third factor were between 0.51 and 0.90; the eigenvalue was 1.58; and the explained variance was 10.57%. The total variance of the scale was 59.07%. The first factor of the scale was expressed as “misrepresentation of the disease”; the second factor as “concealment of information”; and the third factor as “misrepresentation of the real situation” (Table 2).
Table 2. Distribution of factor loadings of scale subdimensions according to exploratory factor analysis
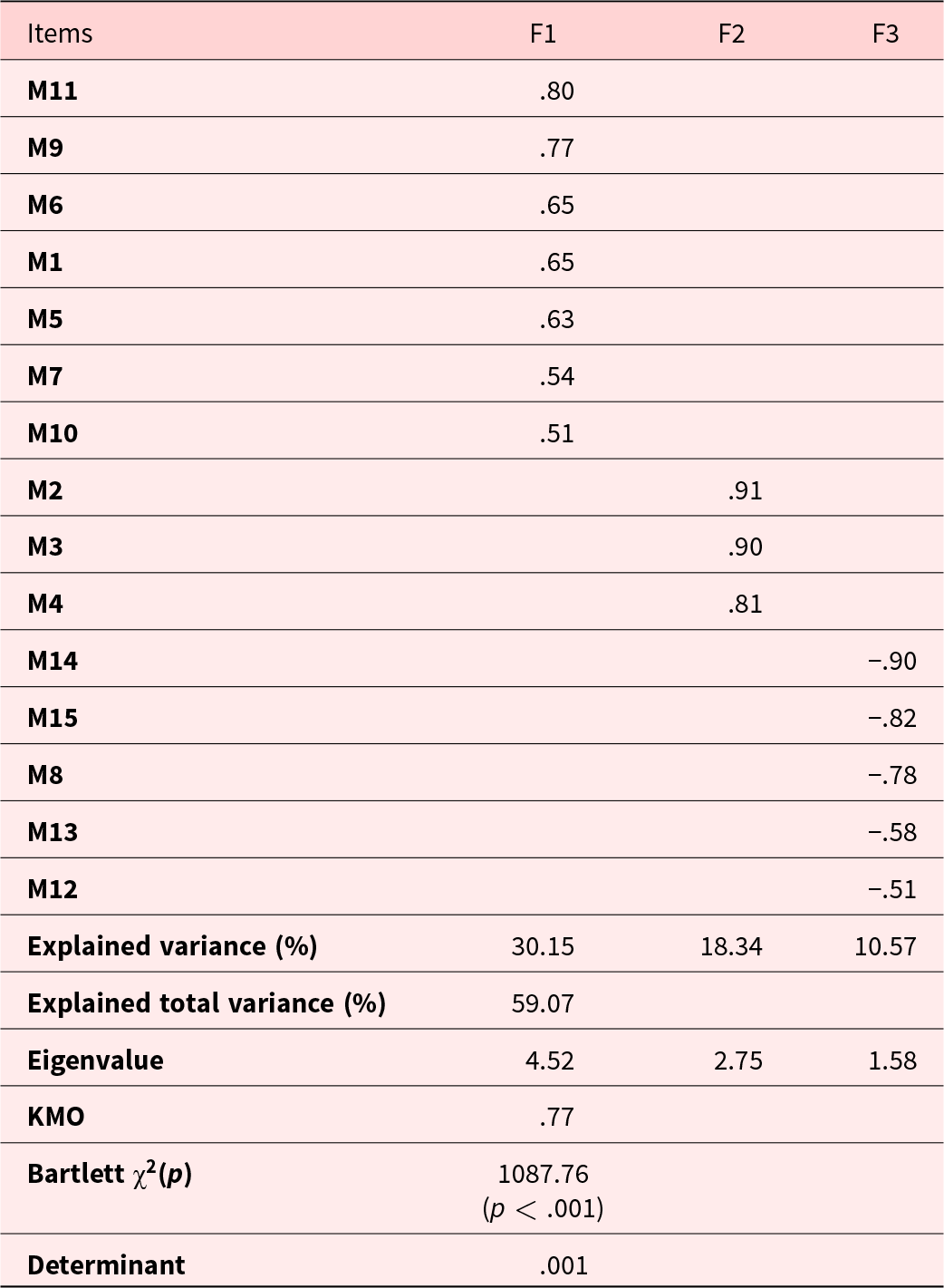
KMO: Kaiser–Meyer–Olkin.
Confirmatory factor analysis
The model fit of the 3-factor scale obtained in the exploratory factor analysis was checked by confirmatory factor analysis. The first-level confirmatory factor analysis of the Information Concealment Scale for Caregivers, which consists of 3 subscales and 15 items, is shown in Fig. 1. In confirmatory factor analysis, the factor loads of the items were between 0.35 and 0.94. As a result of the modifications made in confirmatory factor analysis, the goodness-of-fit values were calculated as follows: CMIN/df(χ2/SD) = 175.16/815 = 2.16; RMR = 0.070; RMSEA = 0.079; GFI = 0.88; CFI = 0.91; NFI = 0.90. These values showed that the 3-factor model is acceptable (Fig. 1).
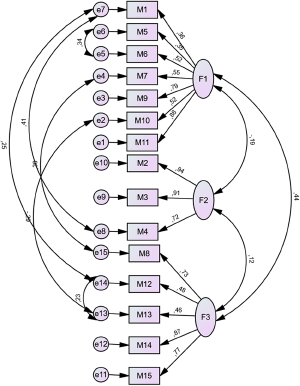
Figure 1. Confirmatory factor analysis path diagram.
Reliability
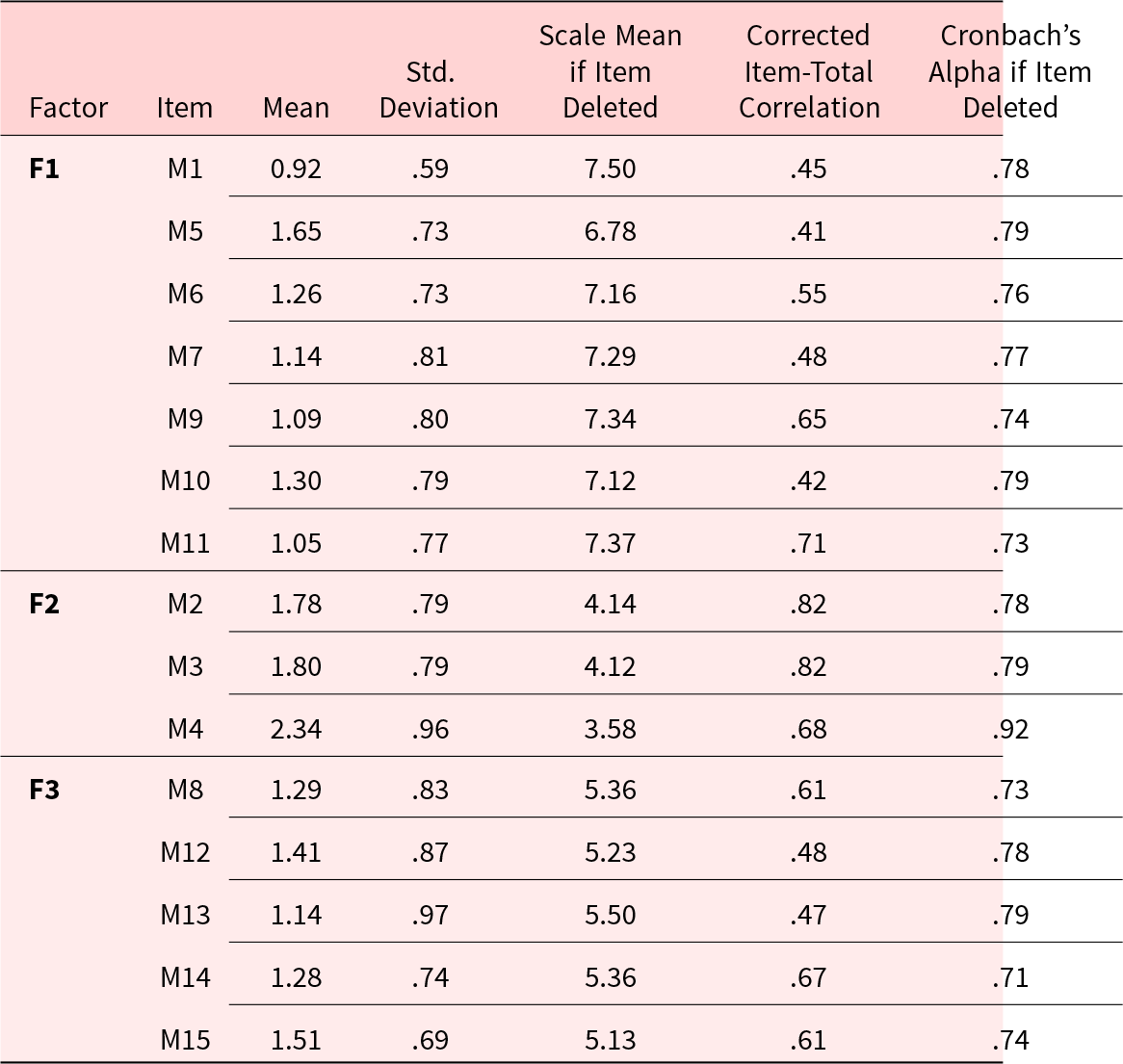
The mean scores on scale items were between 0.92 and 2.34. The item-total correlation of the misrepresentation of the disease (F1) subscale was between 0.41 and 0.71. When an item was removed, the Cronbach’s α value was found to be between 0.73 and 0.79. The item-total correlation of the concealment of information (F2) subscale was between 0.68 and 0.82. When an item was removed, the Cronbach’s α value was found to be between 0.78 and 0.92. The item-total correlation of the misrepresentation of the real situation (F3) subscale was between 0.48 and 0.67. When an item was removed, the Cronbach’s α value was found to be between 0.73 and 0.79 (Table 3).
Table 3. Analysis results of the items of the information concealment scale for caregivers
For the subscales of the Information Concealment Scale for Caregivers, the Cronbach’s α value was 0.79 for misrepresentation of the disease, 0.87 for concealment of information, and 0.78 for misrepresentation of the real situation. The Cronbach’s α value of the total scale was 0. 81. Test–retest reliability was calculated by ICC with the data from 30 caregivers at 2-week intervals. ICC values were between 0.90 and 0.95 at a confidence interval of 95% (Table 4).
Table 4. Mean scores, Cronbach’s α values, and ICCs of the subdimensions of the Information Concealment Scale for Caregivers
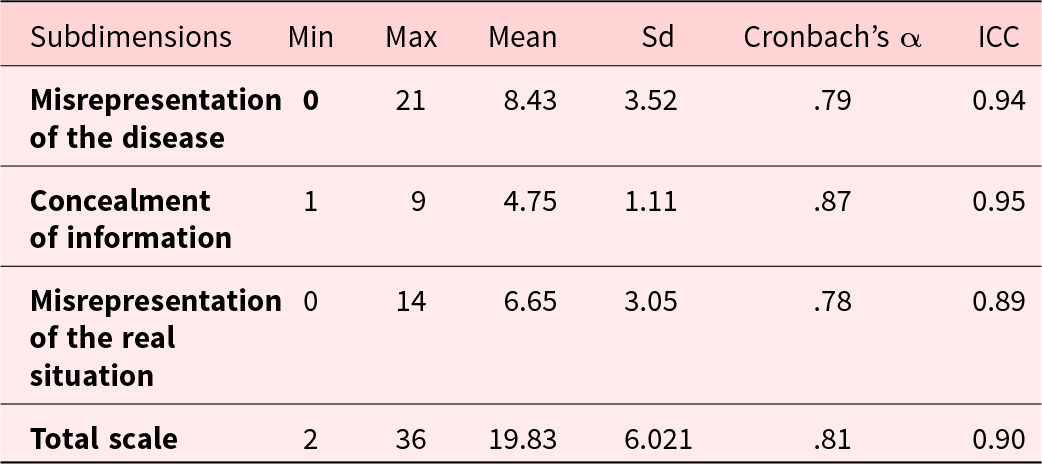
Sd: standard deviation ICC: intraclass correlation coefficient.
There was a positive correlation between the subscales of the Information Concealment Scale for Caregivers (Table 5).
Table 5. Correlation of subscales of the Information Concealment Scale for Caregivers
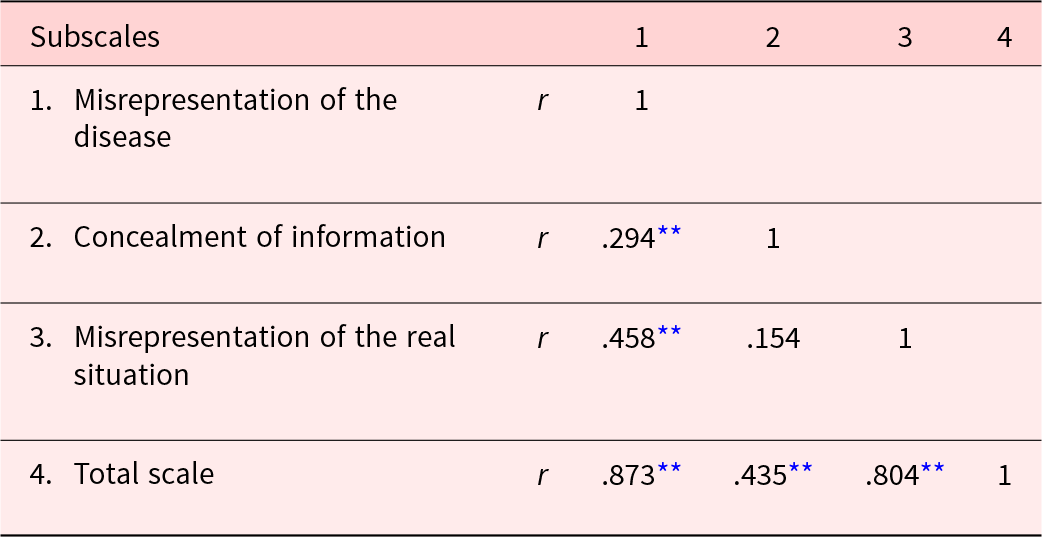
r = Pearson correlation.
** p < 0.01.
Discussion
In this study, which was conducted to establish the validity and reliability of the Information Concealment Scale for Caregivers, it was determined that the scale is a valid and reliable tool. For factor analysis, KMO should be >0.60 and Bartlett’s test of sphericity should be significant (Çokluk et al. Reference Çokluk, Şekercioğlu and Büyüköztürk2016; Esin Reference Esin, Erdoğan, Nahcivan and Esin2021; Field Reference Field2017). In this study, the KMO coefficient was 0.772 and the result of Bartlett’s test of sphericity was statistically significant (χ2 = 1087.761, p = .001) (Table 2). According to the results of the Bartlett test and KMO values, the data set used in the validity and reliability studies of the Turkish version of the Information Concealment Scale for Caregivers was appropriate and had a sufficient size for factor analysis. Exploratory factor analysis was first performed for construct analysis. According to the exploratory factor analysis, it was determined that the scale consisted of 3 subscales. Factor loads of the items were found to be between 0.51 and 0.91. The eigenvalue of the first factor was 4.52 and the explained variance was 30.15%. The eigenvalue of the second factor was 2.75 and the explained variance was 18.34%. The eigenvalue of the third factor was 1.58 and the explained variance was 10.57%. The total variance of the scale was determined as 59.07%. In exploratory factor analysis, subscales of a scale are determined. The factor load value is a coefficient that explains the relationships of items with factors. The factor load values of the items in the factor to which the items belong are expected to be high. If there is a cluster of highly correlated items in a factor, those items measure that factor. Factor load values must be 0.32 and above (Çokluk et al. Reference Çokluk, Şekercioğlu and Büyüköztürk2016; Yong and Pearce Reference Yong and Pearce2013). In some sources, this value is at least 0.30 (Çokluk et al. Reference Çokluk, Şekercioğlu and Büyüköztürk2016; Howard Reference Howard2016). Eigenvalues are used to calculate the variance explained by the factors and to decide the number of factors. In factor analysis, factors with eigenvalues of 1 or above are accepted. The total variance must be 40% or over (Howard Reference Howard2016; Watkins Reference Watkins2018). If a scale is newly developed, first exploratory factor analysis should be performed. In studies in which a scale is adapted from another language, only confirmatory factor analysis may be sufficient (Esin Reference Esin, Erdoğan, Nahcivan and Esin2021). However, since the confirmatory factor structure of the original scale was not confirmed, exploratory factor analysis was performed first in this study. According to the results of EFA, it was found that the Information Concealment Scale for Caregivers, consisting of 3 subscales and 15 items, was similar to the original inventory (de la Piedra‐Torres et al. Reference de la Piedra‐torres, López‐Martínez and Ramírez‐Maestre2022). However, the places of the items in the factors were changed. The first factor of the scale was expressed as “misrepresentation of the disease”; the second factor as “concealment of information”; the third factor as “misrepresentation of the real situation.” Since the scale has not been adapted to other languages and cultures, no comparison could not be made.
Goodness-of-fit indices indicate how well a model explains data. The model’s fit indices in the confirmatory factor analysis of the Turkish version of the Information Concealment Scale for Caregivers were as follows: CMIN/Df(X2/SD) = 175.16/815 = 2.16; RMR = 0.070; RMSEA = 0.079; GFI = 0.88; CFI = 0.91; NFI = 0.90 (Fig. 1). A χ2/df value of <3 indicates good fit and 3 < χ2/df < 5 indicates acceptable fit. Since χ2 value is influenced by the sample size, degrees of freedom ratio give more reliable results. An RMR of <0.05 is considered good and an RMR of <0.08 is considered an acceptable value. It tests the residual covariances between the covariance matrix of the population and the covariance matrix of the sample. RMSEA < 0.05 is considered good and RMSEA < 0.08 is considered an acceptable value. Considering the degree of freedom, it tests how well the model fits with the sample covariance. GFI > 0.95 is considered good and GFI > 0.90 is considered acceptable value. It tests the model fit regardless of sample size. CFI > 0.95 is considered good and CFI > 0.90 is considered an acceptable value. It compares the tested model with the base model, considering the degree of freedom and sample size. NFI > 0.95 is considered good and NFI > 0.90 is considered an acceptable value (Hox Reference Hox2021; Steenkamp and Maydeu-Olivares Reference Steenkamp and Maydeu-Olivares2023). The fit indices of the Turkish version of the Information Concealment Scale for Caregivers were determined to be acceptable. The fit indices of the original scale, χ2/gl = 1648.3/105, p < .001, RMSEA = 0.06, SRMR = 0.06, and CFI = 0.98, were reported to be good for the model (de la Piedra‐Torres et al. Reference de la Piedra‐torres, López‐Martínez and Ramírez‐Maestre2022). The fit indices determined in this study are consistent with those in the original study. The results of the study show that the Turkish version of the scale is consistent with the original model.
Cronbach’s α value gives information about the consistency of scale items with each other (Kalaycı Reference Kalaycı2018). A Cronbach’s α value of >.70 is acceptable, >.80 is good, and >.90 is excellent (George and Mallery Reference George and Mallery2020). The Cronbach’s α value was found to be 0.79 for misrepresentation of the disease, 0.87 for concealment of information, and 0.78 for misrepresentation of the real situation. The Cronbach’s α value of the total scale was 0.81 (Table 4). These results showed that the Turkish version of the Information Concealment Scale for Caregivers is a reliable tool. The Cronbach’s α value of the original scale is between 0.82 and 0.86 (de la Piedra‐Torres et al. Reference de la Piedra‐torres, López‐Martínez and Ramírez‐Maestre2022). The reliability results obtained in this study are similar to those in the original study.
Strengths and limitations
In this study, the English scale was translated into Turkish and used. The author who developed the scale applied the Spanish version of the scale to the caregivers. Therefore, the English version of the scale may not be standardized. This study was conducted with the relatives of palliative care patients and the sample size was small. It is recommended that the scale be studied with a larger sample and with different caregiver groups.
Conclusion
In this study, it was shown that the Turkish version of the Information Concealment Scale for Caregivers is a valid and reliable tool with 3 subscales and 15 items. The scale is easy to use and can be easily used for caregivers in Turkey. Using this tool, the information concealment status of caregivers is measured. Hereby, the effect of information concealment on the patient can be examined. It is recommended that the validity of the scale be evaluated in other caregivers. Further research is needed to examine the Information Concealment Scale for Caregivers in different languages and cultures.






