


During the past decade the demand for organic food (OF) products has grown considerably and various alternatives to the mainstream conventional food products and distribution have been developed and are increasing, especially in developed countries(Reference Lea1). It is difficult to identify reasons for this growth as studies show that OF consumption reflects a complex web of determinants including its availability in food stores, sociodemographic and cultural factors, and personal values and attitudes. Studies, however, also reveal that health considerations are a major factor behind the growth in OF consumption(Reference Torjusen, Sangstad and O'Doherty Jensen2–Reference Magnusson, Arvola and Hursti12). This is noteworthy because a causal association between OF consumption and better health remains to be scientifically established(Reference Velimirov, Huber and Lauridsen13–Reference Woese, Lange and Boess18). Several types of study have been conducted to address the question, but with few or unclear answers for various reasons: the biological and chemical studies in the field are often incomparable, as chemical composition of crops is easily affected by temperature, soil and variety(Reference Lund and O'Doherty Jensen5, Reference Yiridoe, Bonti-Ankomah and Martin7, Reference Schifferstein and Oude Pphuis8, Reference Dangour, Dodhia and Hayter14); few comparable animal studies exist and some may not be relevant for today's farming practice(Reference Velimirov, Huber and Lauridsen13, Reference Magkos, Arvaniti and Zampelas17); and very few intervention studies or prospective observational studies have addressed the potential health benefits of OF products(Reference Dangour, Lock and Hayter16, Reference Grinder-Pedersen, Rasmussen and Bugel19–Reference Rist, Mueller and Barthel21).
In relation to the health effects of OF consumption, the observational study design is complicated by the role of potential confounding factors. Thus, underlying determinants of OF purchase need to be described and included in statistical models in order to minimize potential confounding. The Danish National Birth Cohort (DNBC)(Reference Olsen, Melbye and Olsen22, Reference Olsen, Mikkelsen and Knudsen23) is suitable for addressing this issue as it is one of the largest prospective cohort studies worldwide to have recorded OF preferences during pregnancy along with a multitude of other dietary, health and socio-economic factors. Furthermore, Denmark has a strong system for control and certification of organic farming and manufacturing, a matured organic market and the highest consumption of OF per capita in Europe(Reference Willer and Kilcjer24). Therefore, the DNBC offers unique opportunities to study the impact of OF in pregnancy on maternal and offspring health.
The aim of the present study was to develop a basis for building models that can examine the impact of OF choices on maternal and offspring health among Danish pregnant women. The first step was to identify factors associated with OF consumption. The second step was to employ multivariate methods to identify underlying patterns and to define latent variables that can capture the variability in OF choices among the study population.
Materials and methods
The Danish National Birth Cohort
The DNBC is a cohort with information from 100 000 pregnancies(Reference Olsen, Melbye and Olsen22). Women were recruited between 1996 and 2002 during the first antenatal visit to the general practitioner at around weeks 6–10 of gestation. The data collection in the study included four telephone interviews (two prenatal interviews conducted in gestational weeks 12 and 30, and two postnatal interviews when the child was 6 and 18 months old) and a semi-quantitative FFQ mailed to the women in week 25 of gestation(Reference Olsen, Melbye and Olsen22, Reference Olsen, Mikkelsen and Knudsen23). It was estimated that during the study period approximately 35 % of all deliveries in Denmark were included in the cohort(Reference Olsen, Melbye and Olsen22). Some of the women are registered in the cohort twice or more through subsequent pregnancies during the recruitment period. However, in our study, only the first pregnancy for each participating woman was included to avoid inter-correlation within subjects. Furthermore, multiple pregnancies were excluded from the study. The DNBC complies with the Declaration of Helsinki and was approved by the Danish National Committee on Biomedical Research Ethics.
Definition of organic food preference index
Information on OF consumption was collected through the FFQ(Reference Olsen, Mikkelsen and Knudsen23). About 70 % of the women returned the questionnaire, which was a modified form of a questionnaire used by the Danish Cancer Registry(Reference Overvad, Tjonneland and Haraldsdottir25). Of the 100 000 women in DNBC, 60 773 met the inclusion criteria and had answered the question about OF consumption in the FFQ.
The FFQ covered the pregnant woman's diet during the preceding 4 weeks and included one question about OF consumption: ‘How often do you eat organic foods?’. The question was divided into six categories: ‘milk products’, ‘cereals’, ‘egg’, ‘vegetables’, ‘fruit’ and ‘meat’. The answer categories were ‘never’, ‘sometimes’, ‘regularly’ or ‘always’. Based on the question we calculated an OF preference index. Each answer category was given a score (never = 1, sometimes = 2, regularly = 3, always = 4) and summarized across categories to form an organic index (OX). Missing values were characterized as ‘never eating organic’. Due to the fact that vegetarians and vegans in general have no consumption of meat and vegans have no consumption of meat, egg and milk products, the meat category was excluded for both groups and the egg and milk categories were excluded for vegans. Based on the constructed index the women were divided into four groups: ‘non-users’ (OX = 6), ‘low users’ (6<OX ≤ 12), ‘moderate users’ (12<OX ≥ 18) and ‘frequent users’ (OX > 18).
Assessment of dietary patterns
In the FFQ the women were asked about frequencies for approximately 360 different food and beverage items. To estimate food intake standard portion sizes and standard recipes were applied for all items in the questionnaire. Standard portion sizes were multiplied with the daily frequencies to estimate the intake of each food item in grams. For more complex items standard recipes were made and the intakes of foods present in different items were aggregated. The estimated amounts of all items were coupled with the Danish food composition tables(26) and corrected for loss of fat, water, vitamins and minerals. The 360 different items were divided into thirty-five main food groups and sixty-five more specific food groups representing the entire diet of the women. All nutrients were energy adjusted by the residual method, as described by Willett et al.(Reference Willett, Howe and Kushi27). Only women with an energy intake >4500 kJ/d and <20 000 kJ/d were included in the analyses for dietary intakes to avoid unrealistic estimates. The FFQ used in the DNBC has been validated in a group of younger non-pregnant women(Reference Friis, Kruger Kjaer and Stripp28) and in the DNBC for the intake of fruit, vegetables and pregnancy-relevant nutrients (folate, protein, retinol and n-3 fatty acids) by a 7 d weighed food diary and biomarkers(Reference Mikkelsen, Osler and Olsen29, Reference Mikkelsen, Olsen and Rasmussen30).
Assessment of sociodemographic and lifestyle factors
Sociodemographic and lifestyle variables were gathered from the consent form, the FFQ and the telephone interviews and included: age (<20, 20–24, 25–29, 30–34, 35–39, ≥40 years); parity (0, 1, 2, 3+); occupational status (high-level proficiencies, medium-level proficiencies, skilled, student, unskilled, unemployed); cohabitation status (single, couple/married); urbanization (capital city, capital suburbs, 100 000+, 10 000–99 999, <10 000 citizens); smoking during pregnancy (non-smoker, occasional smoker, <15 cigarettes/d, ≥15 cigarettes/d); alcohol intake in pregnancy (not at all, yes); energy intake (in quintiles); physical activity (none, light, moderate, high level); intake of dietary supplements in the pregnancy (no, yes); maternal pre-pregnant BMI (<18·5, 18·5–24·9, 25·0–29·9, 30·0–34·9, ≥35·0 kg/m2); living area in Denmark (West or East part of the country); and vegetarianism (yes, no). Most of these variables have been described and used in earlier studies based on the DNBC(Reference Halldorsson, Thorsdottir and Meltzer31–Reference Strom, Mortensen and Halldorsson40).
Statistical analysis
Univariate and multivariate logistic regression was used to estimate the association between OF consumption and sociodemographic characteristics and linear regression was used to analyse differences in dietary intake between non-users and frequent OF users. In these analyses the focus was on the differences between non-users and frequent users in order to obtain the biggest contrast between OF consumers. All analyses were performed with the SAS statistical software package version 9·1.
Principal components analysis (PCA) was used for exploration of the associations between the sixty-five food groups. PCA is conducted to uncover the systematic correlation structure between variables while excluding the non-systematic variation. PCA is a widely used method for compression of large data sets, often with a large number of variables, into a few underlying latent variables (principal components), describing the systematic variation. The number of variables in the present work is manageable from a univariate point of view, and PCA is hence not applied as a ‘second to none’ alternative compared with the univariate analysis. PCA in combination with visualization reveals the inter-variable correlation structure and hence adds a dimension on top of what can be explored from univariate analysis(Reference Wold, Esbensen and Geladi41). PCA models were implemented in MATLAB version 7·9·0·529 (R2009b) using PLS toolbox version 5·2·2 (Eigenvector Research Inc.) and in-house algorithms for plotting of results. The Spearman rank correlation test was used to find the correlation between principal components and OF consumption.
Results
The responses to the OF question are shown in Table 1. The frequencies of organic consumption through the six food categories differed substantially. The consumption of organic eggs and milk was common among the women, whereas intakes of organic cereals, vegetables, fruit and meat were low. According to the constructed OF preference index, 12 % of the study population were classified as non-users, 44 % were low users, 37 % moderate users and 7 % were frequent users.
Table 1 Distribution of answers in the six food categories: pregnant women (n 60 773), Danish National Birth Cohort (DNBC), 1996–2002
Table 2 shows associations between OF preferences and sociodemographic and lifestyle characteristics as odds ratios and 95 % confidence intervals for being a frequent user as opposed to a non-user. The crude OR are based on univariate analyses, whereas the adjusted OR are based on a multivariate analysis showing the associations with OF preferences for each explaining variable independently of all the other variables in the table. The women's age had a strong and independent association with OF preferences and so did vegetarianism. Social group, smoking, BMI, physical activity, living area and urbanization were all associated with OF preferences in the crude analysis; however, adjusting for other factors attenuated their associations with OF preferences, although living area and urbanization still had strong associations. Regarding cohabitation status, adjustment tended to strengthen the association with OF preferences. For alcohol intake, use of dietary supplements, physical activity and occupational status the association with OF preferences was eliminated upon adjustment for the other covariates.
Table 2 Association between organic food preferences and different sociodemographic factors (odds ratios for being a frequent user as opposed to a non-user): pregnant women (n 60 773), Danish National Birth Cohort (DNBC), 1996–2002

Ref, referent category.
*Mutually adjusted.
†P value for trend for exposures with more than two categories.
Table 3 shows the mean daily intakes of food items for non-users and the adjusted increments in intake for frequent users compared with non-users. Intakes differed significantly across OF preference for almost all foods and food groups. The most marked differences in intake were observed for vegetables, legumes, fruit and berries, nuts, lamb, seafood, plant oils and tea; all with higher intakes for frequent OF consumers. Adjustment for covariates attenuated the observed differences and reversed the association between OF preferences and the intake of alcohol and desserts (candy, ice cream and cakes). Compared with non-users, frequent users seemed to substitute certain items with others, e.g. margarines with oils, white bread with dark bread, pork with poultry, lamb with fish, coffee with tea and soft drinks with water and juice.
Table 3 Associations between the intake of different food items and organic consumption: pregnant women (n 60 773), Danish National Birth Cohort (DNBC), 1996–2002

*Change compared with non-users.
†Multivariate linear regression. Covariates: cohabitation status, age, smoking habits, parity, pre-pregnant BMI, occupational status, physical activity, energy intake, urbanization and living area.
Table 4 shows daily intakes of specified nutrients according to OF preferences. Nearly all comparisons between frequent users and non-users were statistically significant. The most marked differences were observed for n-3 fatty acids, fibre, iodine, β-carotene, folate and vitamins D, K and C – which were higher among frequent users – and SFA, MUFA, n-6 fatty acids, trans fatty acids, cholesterol and retinol – which were lower among frequent users. Adjustment attenuated the differences; however, significantly higher intakes of certain nutrients were still observed.
Table 4 Associations between nutrients from the diet (energy-adjusted) and organic consumption: pregnant women (n 60 773), Danish National Birth Cohort (DNBC), 1996–2002
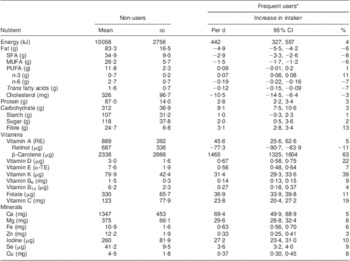
RE, retinol equivalents; α-TE, α-tocopherol equivalents.
*Change compared with non-users.
†Multivariate linear regression. Covariates: cohabitation status, age, smoking habits, parity, pre-pregnant BMI, occupational status, physical activity, urbanization and living area.
Figure 1 shows results from the PCA. Inter-correlation of food groups is shown as a scatter plot of the first two principal components for the food groups. The food groups are coloured according to common food classes. When two variables are positioned close to each other they are correlated with respect to the variance explained by the two components.

Fig. 1 Results from the principal components analysis: inter-correlation of food groups shown as a scatter plot of the first two principal components (PC1 and PC2) for the food groups. Food groups are coloured according to common food classes. Dietary data from pregnant women (n 60 773), Danish National Birth Cohort (DNBC), 1996–2002
From the PCA (Fig. 1) two distinct eating patterns, describing 14·2 % of the total variation in data, can be derived. PC1 is associated with a dietary pattern comprising more vegetables, cabbage, roots, legumes, fish, etc., as these food groups obtain high positive values in PC1. We named this component the ‘prudent dietary pattern’. PC2 is characterized by a high intake of pork, mixed/processed meat, white bread, margarine, French fries, etc., as these food groups obtain high positive values in PC2. This component we named the ‘Western dietary pattern’. The prudent dietary pattern was found to be positively correlated with frequent OF consumption (r = 0·26, P < 0·00001), whereas the Western dietary pattern was negatively correlated with OF consumption (r = −0·28, P < 0·00001). Nevertheless, these two components were not correlated but orthogonal, implying that the Western dietary pattern is not the opposite of the prudent dietary pattern.
Discussion
In the present study we found that OF use was an eating habit related to higher social class and healthier lifestyle and diet – all characteristics that predispose OF users to lower risks of chronic diseases that may affect fetal health during pregnancy. Thus, the study illustrates the major confounder problem that faces researchers who are seeking to tease out the relationship between OF consumption and health outcomes.
Very few studies have compared the diet of non-users and frequent OF users and in general they are of poor quality. However, there seems to be an overall tendency towards higher intakes of fruit and vegetables and a lower intake of meat among OF users(Reference Denver, Christensen and Krarup42–Reference Brombacher and Hamm44), consistent with our findings. It has been argued that the healthier diet observed among frequent OF users can be explained by differences in food supply and prices(Reference O'Doherty Jensen, Larsen and Mølgaard45). Frequent users have a higher propensity to purchase OF products from speciality shops, but also from direct sales channels such as farm gates, box schemes, street stalls in urban areas, etc. that may affect OF product availability and consumption(Reference Wier, O'Doherty Jensen and Andersen46). In the beginning of 2000 the availability of organic foods in supermarkets and discount stores was lower than today(47), especially for organic meat, which can explain the lower OF intake for that product category.
A higher number of vegetarians among frequent OF users might in turn explain the lower intake of meat among frequent OF users in our study. However, stratification by vegetarianism showed a significantly lower adjusted intake of total meat (data not shown) among non-vegetarian OF users compared with non-vegetarian non-users. This finding is supported by a recent survey among 515 Danish consumers which showed that the highest quartile in relation to organic preferences consumed 50 % less meat than non-users(48).
Several efforts have been made to describe OF consumers through descriptive, socio-economic and behavioural factors. However, comparisons between studies are complicated by different market conditions between countries and different study methods. In general, reviews across countries show little consistency and no clear differences or patterns between organic and conventional food users(Reference Yiridoe, Bonti-Ankomah and Martin7, Reference Bonti-Ankomah and Yiridoe49). Nevertheless, higher OF consumption tends to be related to vegetarianism(Reference Schifferstein and Oude Pphuis8, Reference Holt43, Reference Brombacher and Hamm44, Reference Torjusen, Brantsaeter and Haugen50, Reference Onyango51), educational level(Reference Torjusen, Sangstad and O'Doherty Jensen2, Reference O'Doherty Jensen, Larsen and Mølgaard45, Reference Wier, O'Doherty Jensen and Andersen46) and urbanization(Reference Torjusen, Sangstad and O'Doherty Jensen2, Reference O'Doherty Jensen, Larsen and Mølgaard45, Reference Wier, O'Doherty Jensen and Andersen46) which is supported by our findings.
In previous studies frequent OF users have been described as ‘intellectuals’ from urban areas(Reference Torjusen, Sangstad and O'Doherty Jensen2) and the most common reason not to purchase OF products was lack of knowledge or awareness(Reference Yiridoe, Bonti-Ankomah and Martin7). It has been hypothesized that higher educational level provides the consumer more information and experiences to believe that personal behaviour, including OF purchasing behaviour, and personal decisions affect other people(Reference O'Doherty Jensen, Larsen and Mølgaard45). We found occupational status to be strongly associated with OF preferences, which supports these previous studies. In relation to the higher OF use in or near the capital city our findings support the description of ‘intellectuals’ and the tendency to higher purchase in urban areas.
In general, income does not seem to explain differences in OF purchasing behaviour(Reference Yiridoe, Bonti-Ankomah and Martin7, Reference Bonti-Ankomah and Yiridoe49) and income is a weak determinant in highly industrialized countries such as Denmark(Reference O'Doherty Jensen, Larsen and Mølgaard45). Other findings suggest that OF users in some cases may have lower food expenditures than conventional households, despite the fact that OF products are more expensive, and this can be due to differences in dietary habits of the households(Reference Brombacher and Hamm44). Thus, higher price for OF products appears irrelevant in relation to other incentives underlying OF preferences.
There seems to be good agreement concerning incentives for OF use among countries(Reference Yiridoe, Bonti-Ankomah and Martin7, Reference O'Doherty Jensen, Larsen and Mølgaard45). Several studies have found that health considerations are one of the most important incentives for organic preferences followed by concern for the environment(Reference Torjusen, Sangstad and O'Doherty Jensen2, Reference Yiridoe, Bonti-Ankomah and Martin7, Reference Magnusson, Arvola and Hursti12, Reference Bonti-Ankomah and Yiridoe49) and concern about pesticide residues(Reference Byrne, Bacon and Toensmeyer10). In fact, it has been argued that frequent OF users consider the concern for health and environment to be one and the same thing(Reference O'Doherty Jensen, Larsen and Mølgaard45). Since health apparently is a serious concern for OF users, it can be assumed that they follow recommendations about health and exercise to a higher extent than non-users. This is also reflected in our results, even after adjustment for occupational status.
The strength of our study is the large sample size as we have been able to include more than 60 000 pregnant women. It can be argued that self-reported dietary intake may be prone to bias, such as over- or underestimation, but an FFQ is a valid method for classifying individuals according to high or low intake, which was the main interest with respect to OF consumption. The FFQ has been validated against a 7 d weighed food record and the validation showed that the FFQ was useful in separating high and low intake(Reference Mikkelsen, Osler and Olsen29). The dietary calculations were based on assumptions of average portions, sizes and standard recipes for complex dishes, which may have introduced bias in the estimates. In the present study we do not focus on the accuracy of specific nutrient estimates, but instead on the differences between estimates. Thus, we find the dietary intake between non-users and frequent users to be valid.
Until today, very few aetiological studies about organic consumption have been published. The major explanation underlying this may be found in the impact of surrounding multiple factors, unbalance in data, low compliance, and lack of knowledge about dietary components and the impact of pesticides on human health. Our findings add one more parameter because OF consumers in general seem to have a healthier lifestyle and diet. In relation to the previous findings of OF users being more conscious regarding health, observational studies aiming at examining the impact of OF use on human health are complicated.
It is relevant to consider whether OF consumption is part of a specific organic lifestyle including healthy diet, physical activity and health and environmental awareness. If this is the case it may be of no significance to estimate the relationship between OF use and health outcomes in observational studies, because the risk of chronic diseases already is lowered by the diet and exercise. However, it is still important to investigate whether OF products can contribute to lower risk of diseases. Therefore careful epidemiological modelling that can control for confounding factors is needed.
In theory, a randomized controlled trial would be the optimal study design for investigating health effects of human OF consumption. However, in many cases such a trial would require a long intervention period and strict control of foods consumed and would be affected by long study period, high costs and low compliance. Measurements of biomarkers in blood, e.g. pesticide residues and fatty acids composition, would be desirable; however, in a study including 60 000 women this would be financially unfeasible. Moreover, possible health effects can be related to other factors that are undetectable in blood.
The DNBC gives us an opportunity to examine associations in observational studies; however, the statistical models used to analyse these associations must be designed to manage residual confounding and several covariates. Our approach is to devise a stratification strategy for selecting exchangeable groups of women for low and high OF consumption based on relevant confounders and our basis for this will be PCA. This will restrict the study population and hence reduce the statistical power, but in return produce conservative estimates with reduced bias for effects under the assumption of perfect exchangeability.
Conclusions
Frequent OF users in the DNBC had a healthier lifestyle and consumed a more prudent diet with higher intakes of fruit and vegetables, fibre, vitamins, minerals, n-3 fatty acids and less saturated fat. Furthermore, they had a higher occupational status and were living in urban areas, which together indicate an impact of a social gradient on OF purchasing behaviour. Our findings point to a major challenge in examining the impact of OF consumption on health in observational studies due to potentially irremediable confounding by generally healthier food choices among frequent users. Thus, in future studies it is crucial to manage this particular confounder problem. Our detailed analyses constitute a strong basis for such later advancement of strategies for analyses that can allow for unbalance in data, when we compare maternal organic and non-organic food consumers and their offspring in relation to health outcomes.
Acknowledgements
Sources of funding: The research was funded by the Danish Fund for Organic Agriculture and the European Union Integrated Research Project EARNEST (FOOD-CT-2005-007036). The Centre for Fetal Programming is financed by the Danish Council for Strategic Research (grant no. 09-067124) and the DNBC has been financed by the March of Dimes Birth Defects Foundation, the Danish Heart Association, the Danish Medical Research Council, Sygekassernes Helsefond, the Danish National Research Foundation, the Danish Pharmaceutical Association, the Ministry of Health, the National Board of Health and Statens Serum Institut. Conflicts of interest: None of the authors had a personal or financial conflict of interest. Authors’ contributions: S.B.P. and S.F.O.: study conception and design; S.B.P. and M.A.R.: analysis and interpretation of data; S.B.P. and M.A.R.: drafting of the manuscript, statistical analysis, full access to all of the data, responsibility for the integrity of the data and the accuracy of the data analysis; S.B.P., M.S., T.I.H. and S.F.O.: critical revision of the manuscript; S.B.P. and S.F.O.: acquisition of data and responsibility for the entire contents of the manuscript. Acknowledgements: The authors gratefully acknowledge Hanne Torjusen, Helle Margrete Meltzer, Anne Lise Brantsæter and Margaretha Haugen from the Division of Environmental Medicine, Norwegian Institute of Public Health for inspiring cooperation, and the managerial team of the DNBC for their contributions.





