



Rapid demographic change in Africa, partly driven by increasing migration of individuals into cities, has changed people’s food environments and dietary habits(Reference Holdsworth and Landais1). Economic development has increased access to food markets selling energy-dense processed foods at low prices and decreased the price of certain foods such as vegetable oils(Reference Popkin and Gordon-Larsen2). Modification of diet structure towards a higher intake of energy-dense foods (especially from fat and added sugars), a higher consumption of processed foods(Reference Holmes, Dalal and Sewram3), animal source foods, sugar and saturated fats, and a lower intake of complex carbohydrates, dietary fibre, fruit and vegetables has led to a significant change in diet quality over the past 20 years(Reference Imamura, Micha and Khatibzadeh4). The nutrition transition in urban areas of many African countries has resulted in a ‘double burden of disease’ in which there is an increased prevalence of nutrition-related non-communicable diseases (NR-NCD) alongside existing communicable diseases. Although obesity prevalence is higher among African women than men, there has been a rise in both(Reference Kelly, Yang and Chen5,Reference Popkin6) . Children and adolescents are an important group to target in the prevention of overweight and obesity(Reference de Onis, Blössner and Borghi7). In 2010, of the 43 million children estimated to be overweight and obesity, 35 million were from low- and middle-income countries(Reference de Onis, Blössner and Borghi7). The prevalence of overweight and obesity in children in Africa is expected to increase from 8·5 % (2010) to a projected 12·7 % by 2020. By understanding this shift in nutrition and disease, new NR-NCD prevention strategies that account for the factors driving dietary behaviours can be developed across the life course.
A mapping review was previously conducted in 2015(Reference Gissing, Pradeilles and Osei-Kwasi8) to identify drivers of dietary behaviours specifically in adult women within urban settings in African countries and identify priorities for future research. However, the increasing evidence that the overweight and obesity burden is spread more widely across population groups indicates the need for a broader review. Hence, this systematic review mapped the factors influencing dietary behaviours of adolescents and adults of both genders in African urban food environments and identified areas for future research.
Methods
A systematic mapping review(Reference Grant and Booth9) was conducted to map existing literature regarding factors influencing dietary behaviours in urban Africa. Systematic mapping reviews are often conducted as a prelude to further research and are imperative in the identification of research gaps. Prior to conducting the review, the Cochrane Database of Systematic Reviews and MEDLINE were searched to ensure that no similar reviews were underway or had been conducted beyond the original mapping review(Reference Gissing, Pradeilles and Osei-Kwasi8). A review protocol was produced to ensure transparency in the review methodology and then registered with the PROSPERO database of existing and on-going systematic reviews (registration number CRD4201706893).
To determine appropriate inclusion and exclusion criteria for the review, the Sample, Phenomenon of Interest, Design, Evaluation, Research type tool was used(Reference Cooke, Smith and Booth10). Criteria used in the original review were modified to acknowledge the additional population groups (adolescents and adult men)(Reference Gissing, Pradeilles and Osei-Kwasi8); otherwise, the same processes were applied to ensure compatibility.
Inclusion and exclusion criteria
The original review conducted in 2015 investigated women aged 18–70 years living in urban Africa from 1971 to April 2015(Reference Gissing, Pradeilles and Osei-Kwasi8). This current review synthesised recent research in this same group, published since April 2015 to April 2019, and included men (18–70 years) and female/male adolescents (11–17 years), between 1971 and April 2019. All participants were living in urban Africa, those from rural settings were excluded, as were studies with participants <11 years or >70 years. Participants with a clinical diagnosis related to NR-NCD were excluded; excluding studies with specific diseases also ensured that the included studies were of healthy African populations and not specific clinical sub-groups. The phenomenon of interest was defined as factors influencing dietary behaviours. This was purposely broad to enable sensitive mapping of all available literature. Furthermore, studies including African-Americans or African migrants to non-African countries were excluded on the basis of setting. Studies measuring the effect of factors on dietary behaviours were included, but studies that focused on the relationship between diet and diet-related diseases were excluded given the focus on factors influencing dietary behaviour rather than their effect on specific diseases.
To ensure broad coverage of research, all types of study designs were included, that is, randomised controlled trials, cohort studies, case–control studies, ecological/observational studies, reviews and meta-analyses. All publication types were included, provided they were in English or French. Languages were chosen to acknowledge the main publishing languages in Africa.
For adult men and adolescents, any appropriate study from 1971 to 2019 was included. For adult women, studies published since the previous search (April 2015–April 2019) were retrieved. The chosen 1971 start date reflected the earliest appearance of relevant publications concerning health behaviour in the context of the epidemiological transition(Reference Olshansky and Ault11) on the nominated databases and search engines. The primary outcome was dietary behaviour, including macronutrient, food item and food diversity intake, as well as eating habits, preferences, choices and feeding-related mannerisms. Macronutrients were included because of the review’s focus on urban settings where dietary transition is more likely to be associated with dietary change from the nutrition transition, which is associated with increased consumption of fat, vegetable and edible fat and increased added sugar(Reference Popkin6).
Search strategy
Electronic searches were conducted across six key databases: EMBASE, MEDLINE, CINAHL, PsycINFO, ASSIA and African Index Medicus. The search strategy replicated that used in the previous review with the additional inclusion of search terms representing adult men and adolescents(Reference Gissing, Pradeilles and Osei-Kwasi8). An example of a search strategy used for these databases can be found in Supplemental Table 1 in the online supplementary material. Grey literature was explored through the WHO International Trials Registry Index and Thesis (UK and Ireland) Database.
Reference lists for the seventeen studies included in the initial review were examined, and citation tracking using Google Scholar (through Publish or Perish™) was also conducted. Forward and backward citation tracking sought to ensure that no important studies were missed and that representation of appropriate literature was maximised. Reference lists of newly identified included studies, reflecting the expansion of date range and populations of interest, were also reviewed. The dual approach of subject searching and follow-up citation tracking was considered to provide sufficient coverage of the relevant literature(Reference Cooper, Booth and Britten12).
Study selection
Studies that fulfilled the inclusion and exclusion criteria for title and abstract then underwent full-text screening by two reviewers (A.M./F.G.). Duplicates were removed prior to full-text screening. A second reviewer (H.O.-K./M.H.) assessed 10 % of excluded studies at two stages: the title and abstract stage and the full-text search stage. Any disagreements were resolved by discussion. If no agreement was reached, a third reviewer also assessed the study.
Quality assessment
Quality assessment is not a mandatory requirement for a mapping review(Reference Grant and Booth9). However, by incorporating it into the review methodology, it enhances the credibility of the review’s findings and is particularly useful in documenting uncertainties that persist in relation to previous research(Reference Grant and Booth9). Quality assessment was conducted with a validated tool(Reference Kmet, Lee and Cook13) for qualitative and quantitative studies by two reviewers independently (A.M., M.W. or F.G.).
Data extraction
Data were extracted from included studies by one of two principal reviewers (A.M. or F.G.) supported by a second reviewer (H.O.-K. or M.H.) and was checked by a member of the review team (M.W.). As the aim of this mapping review was to map the factors influencing dietary behaviours of adolescents and adults living in African urban food environments and identify areas for future research, it was decided to include all factors reported by authors and not to restrict the review to reporting factors only where a statistical relationship or association had been demonstrated.
Data synthesis
There are different approaches to updating a review. In this review, the new findings were integrated with those of the original review at the synthesis level(Reference Booth, Sutton and Papaioannou14) in order to present all the evidence for men, women and adolescents for the same timescale. In order to determine which factors influence dietary behaviours in the three population sub-groups, factors influencing dietary behaviours for adults and adolescents of all thirty-eight studies were mapped to the socio-ecological model defined by Story et al. (Reference Story, Kaphingst and Robinson-O’Brien15). Factors were placed within four broad levels: individual, social environment, physical environment and macro-environment and assigned to an appropriate sub-level. For novel factors that emerged, it was decided within the team where to place it in the aforementioned socio-ecological model, similar to the original review(Reference Gissing, Pradeilles and Osei-Kwasi8). Reporting of the review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist(Reference Moher, Liberati and Tetzlaff16).
Results
Search results
The search yielded 2433 title and abstract records after duplicates were removed (Fig. 1); 274 records remained for full-text retrieval, at which stage 247 records were excluded, leaving twenty-seven studies for inclusion for studies of adolescents, men and women (from 2015). Twelve studies from an earlier review of women only aged 18–70 years (1971–2015) were integrated in the review findings, giving a total of thirty-nine studies.

Fig. 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram showing the selection of studies for the present systematic mapping review
Description of included studies
Thirty-nine studies were included in the final data synthesis (Table 1), of which nineteen were conducted in lower middle-income countries(17): Cape Verde, Egypt, Ghana, Kenya, Morocco, Nigeria and Tunisia. Thirteen studies were conducted in upper middle-income countries: Botswana, Mauritius and South Africa, and one study was undertaken in the Seychelles (high-income country). Only six studies were undertaken in low-income countries: Burkina Faso, Benin, Niger and Tanzania (Table 1). Over half of studies were conducted in Ghana and Morocco (six studies each) or South Africa (ten studies).
Table 1 Characteristics of the included studies (39 studies and 45 records)
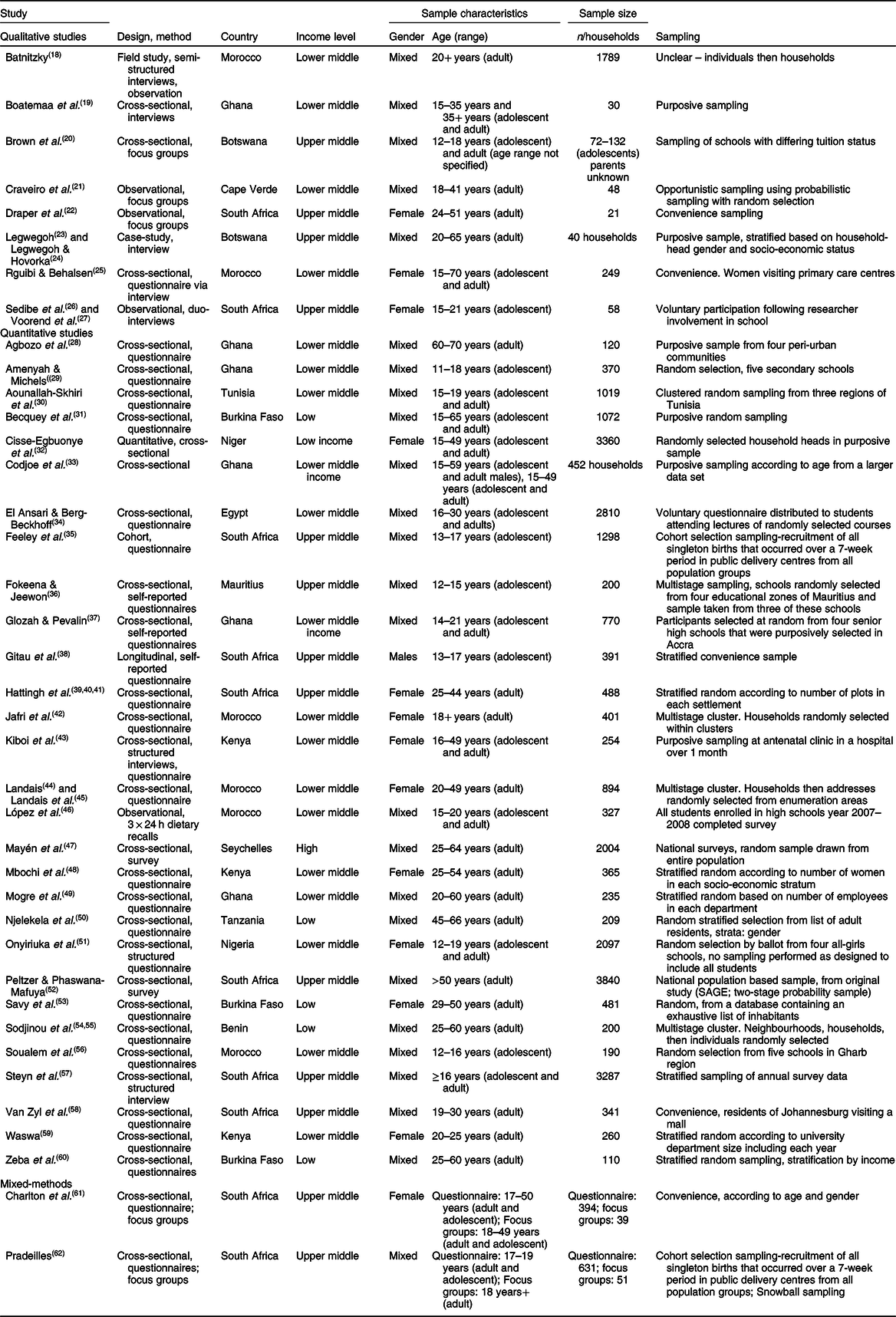
Of the thirty-nine studies, eight were qualitative (ten records)(Reference Batnitzky18–Reference Voorend, Norris and Griffiths27), twenty-nine (thirty-three records) were quantitative(Reference Agbozo, Amardi-Mfoafo and Dwase28–Reference Zeba, Delisle and Renier60) and two used mixed methods(Reference Charlton, Brewitt and Bourne61,Reference Pradeilles62) studies. The qualitative and quantitative data in the latter were extracted separately in order to generate distinct quality assessment scores. Of the thirty-nine studies, thirty-two were cross-sectional studies(Reference Batnitzky18–Reference Brown, Shaibu and Maruapula20,Reference Rguibi and Belahsen25,Reference Agbozo, Amardi-Mfoafo and Dwase28–Reference Glozah and Pevalin37,Reference Hattingh, Walsh and Veldman39–Reference Landais, Bour and Gartner45,Reference Mayén, Bovet and Marti-Soler47–Reference Pradeilles62) , four were observational(Reference Batnitzky18,Reference Craveiro, Alves and Amado21,Reference Sedibe, Feeley and Voorend26,Reference Voorend, Norris and Griffiths27,Reference López, Anzid and Cherkaoui46) , two used a longitudinal design(Reference Gitau, Micklesfield and Pettifor38) and one was a detailed case study(Reference Legwegoh23,Reference Legwegoh and Hovorka24) . The methodology consisted of interviews and focus groups to obtain qualitative data, whereas self-administered or interviewer-led surveys were mostly used for quantitative studies.
Quality assessment
In summary, while most of the quantitative studies scored high on criteria such as appropriate study designs, question/objective sufficiently described and data analysis clearly described, these studies did not report on controlling for confounders or estimation of variance in the main results.
Similarly, in all qualitative studies, authors failed to report on procedures to establish credibility or show reflexivity. The individual aspects of the quality assessment conducted for all thirty-nine included studies (see online supplementary material, Supplemental Tables 2 and 3).
Factors influencing diet or dietary behaviour in urban Africa
In total, seventy-seven factors influencing dietary behaviours were identified, with two-thirds at the individual level (45/77). Factors in the social (11/77), physical (12/77) and macro (9/77) environments were investigated less. Slightly more studies investigating social-level factors studied adolescent populations (Table 2). The configuration of dietary factors in adult men paralleled that of adult women, probably because relevant included studies examined a mixed adult population. In all population groups, the individual and household factors level of the socio-ecological model was the most studied.
Table 2 Factors in urban African food environments influencing dietary behaviours in the included studies (n 39)

MM, mixed methods; QN, quantitative study; QL, qualitative study.
* Association not assessed/reported.
† Significant association.
‡ Association assessed but NS.
Dietary factors in adult women, adult men and adolescents
Individual level
Almost two-thirds of factors identified were on the individual level (45/77), of which twelve related to cognitions, fifteen to lifestyle/behaviours, nine were biological factors and nine were demographic factors (Fig. 2). Factors specific to adolescents included self-esteem, body satisfaction, dieting, spoken language, school attendance, gender, body composition, pubertal development, BMI and fat mass.
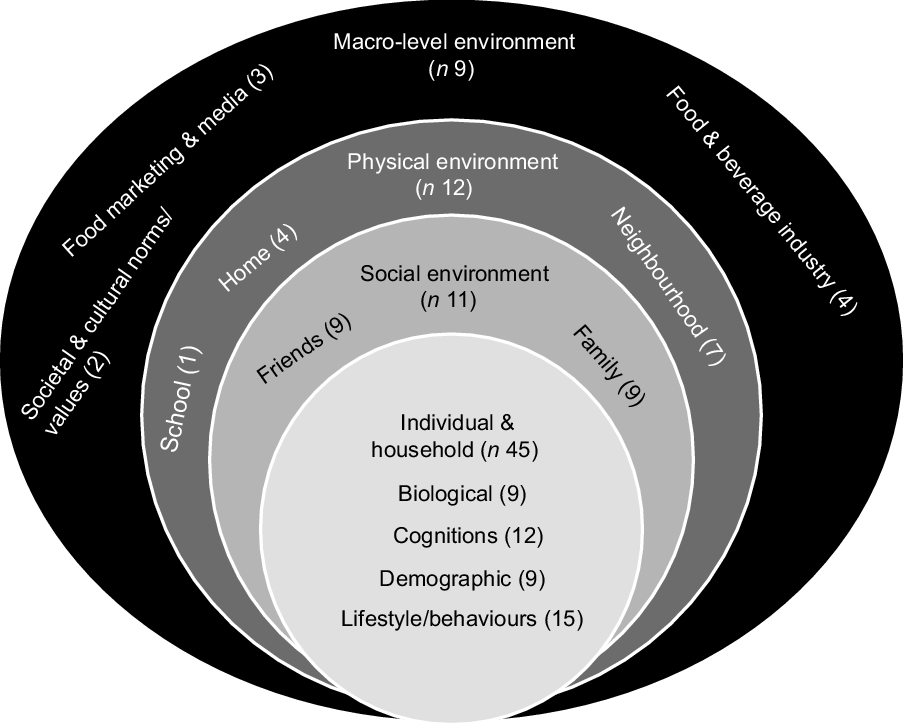
Fig. 2 A summary of factors (n 77) emerging from the included studies at different environmental levels
Cognitions
Taste and hunger were cognition-related factors only found within adult studies(Reference Sedibe, Feeley and Voorend26,Reference Voorend, Norris and Griffiths27,Reference Cisse-Egbuonye, Ishdorj and McKyer32,Reference Van Zyl, Steyn and Marais58,Reference Charlton, Brewitt and Bourne61) . For instance, one quantitative study(Reference Van Zyl, Steyn and Marais58) in Johannesburg found that 52·5 % of participants believed taste influenced fast-food intake. Higher perceived stress levels were found to significantly decrease the amount of fruit and vegetable consumption in a mixed adult population in Egypt, with a more pronouned effect in men(Reference El Ansari and Berg-Beckhoff34). Food knowledge and subjective health status was more commonly reported in the studies of adults(Reference Agbozo, Amardi-Mfoafo and Dwase28,Reference López, Anzid and Cherkaoui46,Reference Waswa59) . Preferences, mood and perception of diet quality and quantity were reported in both qualitative and quantitative studies of both adolescents and adults(Reference Boatemaa, Badasu and De-Graft Aikins19,Reference Sedibe, Feeley and Voorend26,Reference Voorend, Norris and Griffiths27,Reference Becquey, Savy and Danel31,Reference Waswa59) .
A small number of factors emerged on the relationship between body satisfaction and dietary behaviours. An association was identified between decreased self-esteem and body satisfaction with disordered eating in South African adolescents, as measured by the Eating Attitudes Tests 26(Reference Gitau, Micklesfield and Pettifor38). No significant association was found between body image perception and food intake in a quantitative study of female adults(Reference Waswa59).
Lifestyle/behaviours
A third of individual-level factors identified for adults were categorised under the lifestyle/behaviours sub-level. Time limitation was found to be an important factor in five studies encompassing qualitative and quantitative data conducted in Botswana, Cape Verde, Ghana and South Africa(Reference Brown, Shaibu and Maruapula20,Reference Craveiro, Alves and Amado21,Reference Legwegoh23,Reference Legwegoh and Hovorka24,Reference Mogre, Atibilla and Kandoh49,Reference Van Zyl, Steyn and Marais58) . In the qualitative study conducted in Cape Verde(Reference Craveiro, Alves and Amado21), reduced time availability was associated with the intake of unhealthy street foods. Other important lifestyle-related factors identified in a quantitative study related to lack of fruit and vegetable intake(Reference Peltzer and Phaswana-Mafuya52) were tobacco use, alcohol use, physical inactivity and low quality of life. Spoken language was found to be significantly associated with dietary quality in one quantitative study conducted in Morocco, as adolescents who only spoke Arabic had a poorer quality of diet than those who spoke both Arabic and French(Reference Soualem, Ahami and Aboussaleh56).
Biological
Evidence from quantitative studies was found for the role of biological factors, which were associated with dietary behaviours in adults, that is, morbidity(Reference Kiboi, Kimiywe and Chege43), age(Reference Becquey, Savy and Danel31,Reference Hattingh, Walsh and Veldman39–Reference Jafri, Jabari and Dahhak42,Reference Landais44,Reference Landais, Bour and Gartner45,Reference Onyiriuka, Umoru and Ibeawuchi51,Reference Savy, Martin-Prével and Danel53,Reference Soualem, Ahami and Aboussaleh56) and having multiple children (parity)(Reference Landais44,Reference Landais, Bour and Gartner45,Reference Sodjinou, Agueh and Fayomi54) . For instance, increased morbidity was significantly associated with minimum dietary diversity among pregnant women in Kenya(Reference Kiboi, Kimiywe and Chege43).
More diverse biological factors were investigated for adolescents than for adults. However, only age(Reference Onyiriuka, Umoru and Ibeawuchi51), BMI and fat mass(Reference Feeley, Musenge and Pettifor35) were significantly associated with dietary behaviours. For instance, increasing age was significantly associated with skipping meals among schoolgirls in Nigeria(Reference Onyiriuka, Umoru and Ibeawuchi51) and fat mass was negatively associated with poor eating behaviour(Reference Feeley, Musenge and Pettifor35).
Demographic
More demographic factors were identified in adult women than in mixed adult studies. In one quantitative study of adults conducted in Burkina Faso, males of higher SES, as measured by income and education were significantly aggregated in the ‘urban’ diet cluster, while there were proportionally more lower income, non-educated and female subjects in the ‘traditional’ diet cluster(Reference Sodjinou, Agueh and Fayomi54). Other factors that were investigated were household composition and family profession, but their relationship with dietary behaviours was NS. Adolescents with high SES adhered to more aspects of dietary guidelines than those of low SES in one quantitative study in Mauritius(Reference Fokeena and Jeewon36).
Qualitative and quantitative studies have found that the importance of household SES was apparent across a range of SES indicators including household income or wealth(Reference Legwegoh23,Reference Legwegoh and Hovorka24,Reference Codjoe, Okutu and Abu33,Reference Kiboi, Kimiywe and Chege43,Reference Njelekela, Liu and Mpembeni50,Reference Sodjinou, Agueh and Fayomi54,Reference Steyn, Labadarios and Nel57) , employment(Reference Cisse-Egbuonye, Ishdorj and McKyer32,Reference Kiboi, Kimiywe and Chege43,Reference Landais, Bour and Gartner45,Reference Soualem, Ahami and Aboussaleh56,Reference Steyn, Labadarios and Nel57) , land ownership(Reference Kiboi, Kimiywe and Chege43) and financial insecurity(Reference Draper, Davidowitz and Goedecke22). Educational level of individuals or parents was also found to play a role in dietary behaviours in several quantitative studies(Reference Aounallah-Skhiri, Trasissac and El-Ati30,Reference Codjoe, Okutu and Abu33,Reference Glozah and Pevalin37,Reference Kiboi, Kimiywe and Chege43–Reference López, Anzid and Cherkaoui46,Reference Peltzer and Phaswana-Mafuya52,Reference Sodjinou, Agueh and Fayomi54,Reference Soualem, Ahami and Aboussaleh56) . Higher parental education level was associated with better dietary intake in four quantitative studies among adolescents(Reference Aounallah-Skhiri, Trasissac and El-Ati30,Reference Codjoe, Okutu and Abu33,Reference Glozah and Pevalin37,Reference López, Anzid and Cherkaoui46) , resulting in a higher modern dietary diversity score for adolescents in Tunisia,(Reference Aounallah-Skhiri, Trasissac and El-Ati30) higher household dietary diversity score in Ghana(Reference Codjoe, Okutu and Abu33) and better healthy eating behaviours in Ghana(Reference Glozah and Pevalin37) and Morocco(Reference López, Anzid and Cherkaoui46) than those whose parents had average or low educational attainment.
Dietary behaviours were associated with ethnicity in South African adults(Reference Gitau, Micklesfield and Pettifor38,Reference Peltzer and Phaswana-Mafuya52) and adolescents in South Africa(Reference Gitau, Micklesfield and Pettifor38) and Nigeria(Reference Onyiriuka, Umoru and Ibeawuchi51).
Social environment
Eleven factors emerged that related to the social environment, eleven studies (both qualitative and quantitative) explored family influences(Reference Batnitzky18–Reference Brown, Shaibu and Maruapula20,Reference Rguibi and Belahsen25,Reference Becquey, Savy and Danel31,Reference Jafri, Jabari and Dahhak42,Reference Landais44,Reference Landais, Bour and Gartner45,Reference Onyiriuka, Umoru and Ibeawuchi51,Reference Savy, Martin-Prével and Danel53,Reference Waswa59,Reference Charlton, Brewitt and Bourne61) and four studies investigated friendship(Reference Boatemaa, Badasu and De-Graft Aikins19,Reference Sedibe, Feeley and Voorend26,Reference Voorend, Norris and Griffiths27,Reference Peltzer and Phaswana-Mafuya52,Reference Waswa59) (Fig. 2).
Family
The social environment was particularly investigated in adolescent studies; nine factors related to the family including marital status, with evidence coming from both qualitative and quantitative studies(Reference Rguibi and Belahsen25,Reference Becquey, Savy and Danel31,Reference Jafri, Jabari and Dahhak42,Reference Landais44,Reference Savy, Martin-Prével and Danel53) , what the rest of the family eats(Reference Boatemaa, Badasu and De-Graft Aikins19,Reference Charlton, Brewitt and Bourne61) and support in the household(Reference Boatemaa, Badasu and De-Graft Aikins19,Reference Becquey, Savy and Danel31,Reference Savy, Martin-Prével and Danel53) .
Friends
Two qualitative studies examined the role of friendship on dietary habits and reported that friendship was associated with dietary habits in South African adolescents(Reference Sedibe, Feeley and Voorend26,Reference Voorend, Norris and Griffiths27) , stating that ‘participants often ate the same food as their friends’ and that shared food consumption between friends was common. In another qualitative study in Ghana, some participants mentioned friends as influencing food choice; foods recommended among peers were usually processed foods such as savoury snacks, soda and instant noodles(Reference Boatemaa, Badasu and De-Graft Aikins19). A quantitative study conducted among South African adults(Reference Peltzer and Phaswana-Mafuya52) did not find a significant association between social cohesion and fruit and vegetable consumption.
Physical environment
Fourteen studies (qualitative and quantitative) investigated the role of the physical environment on dietary behaviours, of which nine included adolescents(Reference Boatemaa, Badasu and De-Graft Aikins19,Reference Sedibe, Feeley and Voorend26,Reference Voorend, Norris and Griffiths27,Reference Becquey, Savy and Danel31,Reference Codjoe, Okutu and Abu33,Reference Feeley, Musenge and Pettifor35,Reference Kiboi, Kimiywe and Chege43,Reference Onyiriuka, Umoru and Ibeawuchi51,Reference Steyn, Labadarios and Nel57,Reference Pradeilles62) . Twelve factors emerged in the physical food environment that influenced dietary behaviours. Seven of these were in the neighbourhood, four in the home environment and one in the school environment (Fig. 2).
Convenience and availability of food were the most investigated factors in the physical environment. For instance, convenience was identified as a factor influencing fast-food intake with one quantitative study in South Africa noting that 58·1 % of participants believed it influenced their food choices(Reference Van Zyl, Steyn and Marais58). Significant associations were found between housing conditions and where food is bought with dietary behaviours in South Africa(Reference Steyn, Labadarios and Nel57). Two studies found an association between eating outside the home and dietary behaviours(Reference Codjoe, Okutu and Abu33,Reference Landais44,Reference Landais, Bour and Gartner45) . Eating outside the home was associated with higher household dietary diversity in a quantitative study in Ghana, while food eaten at home was associated with lower household dietary diversity scores(Reference Codjoe, Okutu and Abu33).
The influence of school on dietary habits was investigated by only one qualitative study(Reference Sedibe, Feeley and Voorend26), which found that availability of food within schools, as well as sharing food within school, influenced dietary habits in South Africa.
Macro-environment
Nine factors emerged as influencing dietary behaviours that were on the macro-environment level. Three of these factors related to the food marketing and media environment, two related to societal and cultural values and four related to the role of the food and beverage industry.
Food prices were associated with fast-food intake in one South African quantitative study of young adults(Reference Van Zyl, Steyn and Marais58). Media and advertising were found to be associated with dietary intake of adults in both qualitative and quantitative studies in Botswana(Reference Legwegoh23,Reference Legwegoh and Hovorka24) and South Africa(Reference Van Zyl, Steyn and Marais58). About 49 % of participants in one study in South Africa stated that they believed media messages influenced their decision to purchase fast food(Reference Van Zyl, Steyn and Marais58). In a quantitative study conducted in South Africa, ideal body size was related to dietary behaviours(Reference Gitau, Micklesfield and Pettifor38). A quantitative study conducted in Ghana(Reference Amenyah and Michels29) identified that larger ideal body size was associated with a changed Eating Attitudes Tests 26 score. Lack of religious involvement was associated with dietary behaviour in one quantitative study of adults in South Africa(Reference Peltzer and Phaswana-Mafuya52), and one quantitative study of adults and adolescents in Ghana but was not associated with meal skipping or food choices in adults(Reference Mogre, Atibilla and Kandoh49).
Discussion
This systematic mapping review mapped the factors influencing dietary behaviours of adolescents and adults in African urban food environments and identified areas for future research. Thirty-nine studies (forty-five records) were included in the final data synthesis. In total, seventy-seven factors influencing dietary behaviours were identified, with two-thirds at the individual level (45/77). Factors in the social (11/77), physical (12/77) and macro (9/77) environments were investigated less. The inclusion of two additional population groups (adult men and adolescents), in comparison to the original review, expands the generalisability of findings to the general population in urban Africa. Studies included in this review were from fifteen African countries, encompassing a range of low-, middle- and high-income African countries, reflecting the heterogeneity of urban African contexts. However, over half (22/39) were conducted in Ghana, Morocco or South Africa. This updates and extends a previous review, which was restricted to women(Reference Gissing, Pradeilles and Osei-Kwasi8). The current review updated and extended the demographic scope to include men and adolescents, as well as women.
Findings synthesised from included studies indicate that the most investigated factors for adults and adolescents were the individual and household environment of the socio-ecological model as described by Story et al. (Reference Story, Kaphingst and Robinson-O’Brien15). This finding is consistent with our previous review(Reference Gissing, Pradeilles and Osei-Kwasi8). Dietary behaviour was significantly associated with a range of individual and household environmental factors: household income, educational level, employment, land ownership, socio-economic status (SES), ethnicity and financial insecurity. Low self-esteem, high levels of stress and lack of time were associated with unhealthy dietary behaviours. The focus on individual-level factors might be attributable to the fact that promoting healthy eating and preventing obesity have predominantly focused on changing behaviour through interventions such as nutrition education, although such interventions alone have met with little success(Reference Delormier, Frohlich and Potvin63).
Studies involving adolescents investigated factors in their social environments and were less focused on the role of the physical food environment on dietary behaviours, than for adults. This bias is unsurprising given that adolescence is defined as a transient formative period where many life patterns are learnt(Reference Rees, Christine and Adams64), particularly through the social environment. Shared food consumption between adolescent friends was common. Evidence from the wider literature outlines the social transmission of eating behaviours, whereby a strong relationship exists between the social environment and amount or types of food eaten(Reference Robinson, Thomas and Aveyard65). This implies individuals tend to eat according to the usual social group they find themselves, either in terms of quantity or types of food eaten(Reference Powell, Wilcox and Clonan66). Thus, understanding the role of the social environment among adults and adolescents as a modifiable factor influencing dietary behaviours offers an opportunity for developing nutrition interventions that harness social relationships.
Convenience and availability of food were the most investigated factors in the physical environment. Significant associations were found between housing conditions and dietary intake, and where food was purchased and dietary intake. In contrast to the socio-ecological model(Reference Story, Kaphingst and Robinson-O’Brien15), our map lacks evidence for the role of several factors in the physical environment such as workplaces, schools (one study), supermarkets and convenience stores.
In contrast to studies conducted in high-income countries, factors influencing dietary behaviours in the macro-environment were rarely investigated in our review for adults or adolescents. Only food/drink advertising and religion (adolescents only) and food prices were associated with unhealthy dietary behaviours, but many macro-level factors are known to influence diet, such as the political context, economic systems, health care systems and behavioural regulations(Reference Sleddens, Kroeze and Kohl67) that were not studied. One possible explanation may be that because Story’s model was generated following research within high-income counties, some of the sub-levels may be less relevant to the African context. Factors that have been shown to influence dietary behaviours in high-income countries and were investigated in studies included in this review include food prices, social networks (friendship), time constraints and convenience. However, in high-income countries these factors are often reported in low-income groups(Reference Osei-Kwasi, Nicolaou and Powell68). Another important finding from this review is the consistent association between SES and dietary behaviours as expected. SES is a global concern, and several studies have shown that lower SES restricts food choices, thus compelling the consumption of unhealthy foods(Reference Powell, Zhao and Wang69–Reference Vogel, Ntani and Inskip71).
Of the thirty-nine studies identified, none specifically investigated adult men, as they were only included in mixed adult population studies. Adult men and women studies identified during this review showed similar types of factors associated with dietary behaviour across the different environments, suggesting that similar interventions could be targeted at both men and women. However, demographic factors were identified more in adult women than in mixed adult studies. This implies that the household is an important setting in which to reach women. The findings for women from this review went beyond that of the previous review. Three more factors (stress, self-esteem and body satisfaction) were identified in the updated review. Furthermore, the expanded review identified evidence of more physical-level dietary factors including housing, living area, convenience and where food is bought.
As the most common study methodology of included studies was cross-sectional, it is not possible to conclude on causality of the factors in different components of the food environment on dietary behaviours. Limitations regarding the use of the socio-ecological model(Reference Osei-Kwasi, Nicolaou and Powell68) became evident during the review, as there is overlap between the different environmental levels for factors such as SES, spoken language and religious group. For instance, SES crosses multiple levels of the model, particularly in adolescents, as SES is often measured via physical or household/family-related factors. Another example is religious groups, which do not fit within the current sub-categories defined by Story’s ecological model(Reference Story, Kaphingst and Robinson-O’Brien15). Although religion may broadly be classified as a factor in the macro-environment, religious groups may best fit in the social environment. While the socio-ecological model depicts reality as artificially separating individual and social experiences(Reference Osei-Kwasi, Nicolaou and Powell68), it is still a useful tool to communicate with policy makers and practitioners, unlike systems-based approaches, which are better at representing reality but rely on data on causality and mechanisms that are often lacking in cross-sectional and quantitative studies(Reference Holdsworth, Nicolaou and Langoien72) and are harder to communicate to a non-expert audience.
This review revealed considerable heterogeneity in the design of quantitative studies and the outcome measures used for assessing dietary behaviours. Future quantitative studies should ensure that outcome measures are clearly defined and report the direction of association between the factors examined and whether dietary behaviours are healthy or unhealthy. Quantitative studies should enhance the control of confounding variables to prevent them from introducing bias into the findings, and longitudinal quantitative studies are needed to be able to measure how factors influencing dietary behaviours are changing with the transformation of food environments. Qualitative studies are useful for understanding the complex relationships between determinants of dietary behaviours. Qualitative studies need to have a rigorous design and improve the reporting of reflexivity by considering the impact of the role of researcher characteristics on the data collected to improve their quality.
This review highlights the need for robust mixed methods studies to gain a better understanding of the drivers of dietary behaviours in urban food environments in Africa.
This is the first systematic mapping review that focuses on environmental factors of dietary behaviour for all population groups in an urban African context. The nutrition transition has been associated with changes in dietary patterns globally with concomitant increases in obesity and NR-NCD, now among the leading causes of death(73). In African countries, NR-NCD risk is increasing at a faster rate and at a lower economic threshold than seen in high-income countries(Reference Popkin74), hence the need for this review that identifies context specific factors that influence dietary behaviours. The recent focus on good health and well-being as part of the Sustainable Development Goals (SDG3)(75) also reflects this review’s aim to identify the underlying determinants of dietary behaviour in the urban African context to identify avenues for interventions.
Conclusion
The relatively small number of appropriate studies identified, following an extensive literature search, indicates a significant gap in research into understanding of the factors influencing diets in food environments in urban Africa. Due to the increasing presence of multiple burdens of malnutrition in urban Africa, secondary to the nutrition transition(Reference Popkin6), more studies should be directed at investigating how food environments are changing and driving this complex nutritional landscape. In particular, future research could emphasise the investigation of adult men and adolescents. The evidence from this review will contribute towards developing a socio-ecological framework of factors influencing dietary behaviours adapted to urban African food environments.
Acknowledgements
Acknowledgements: Emmanuel Cohen was supported by the South African DST/NRF Centre of Excellence in Human development. Financial support: This research was funded by a Global Challenges Research Fund Foundation Award led by the MRC, and supported by AHRC, BBSRC, ESRC and NERC, with the aim of improving the health and prosperity of low- and middle-income countries. The TACLED (Transitions in African Cities Leveraging Evidence for Diet-related non-communicable diseases) project code is MR/P025153/1. The funders had no role in the design, analysis or writing of this article. Conflict of interest: There are no conflicts of interest. Authorship: All authors designed the review. A.M. conducted the searches and screening. H.O.-K. checked 10 % of excluded records at title/abstract and full-text screening stages. A.M., F.G. and H.O.-K. extracted data and conducted analyses and quality assessment. M.W. checked data extraction and quality assessment. H.O.-K. drafted the manuscript. All authors reviewed draft versions of the manuscript and provided suggestions and critical feedback. All authors have made a significant contribution to this manuscript and approved the final manuscript. Ethics of human subject participation: Not applicable.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980019005305







 Open access
Open access