

Introduction
Medical research has improved the health of individuals and communities over the last 50 years [1]. Nevertheless, it takes several years for patients to benefit from advances translated into clinical practice and public health [1–Reference Keramaris3]. To address this gap, the National Institutes of Health (NIH) created the National Center for Advancing Translational Science (NCATS) in 2006. NCATS seeks to expedite the translation of biomedical research into new technologies and treatments by funding novel, innovative educational programming, translational research, and dissemination projects [1]. NCATS has provided funding to 62 academic medical centers through the Clinical and Translational Science Award (CTSA) [1]. The CTSA program provides infrastructure support to academic medical centers to train translational scientists, fund pilot studies and career development awards, build research networks, increase collaborative and team science, and enhance biomedical research [1–4].
In the decade since the first CTSA awards were distributed, NCATS has collaborated with the Institute of Medicine (IOM) to evaluate the program and define focus areas for translational science. This evaluation process indicated that community-engaged research (CEnR) reduces the time needed to translate biomedical research to patients and the public [1]. Furthermore, the evaluators recommended that community-engaged research occur at all phases of biomedical research—including laboratory discoveries, patient-centered outcomes research, and research conducted in and with the public. The IOM report provided room for interpretation about how best to implement this recommendation at each NCATS-funded center. Although the IOM report left room for interpretation, CTSAs share a common understanding of CEnR and its impact on health. CEnR is an inclusive partnership of researchers and community members affiliated by common interest, geography, or situations that encourages mutual respect, recognition of values, strategies, and actions in order to address health issues affecting the community [Reference Ahmed and Palermo5–Reference Jones and Wells7]. It is built on a framework of various study designs used in clinical and translational science [4].
Most CTSAs have programs that provide CEnR education to academics, medical researchers, and communities. In 2010, Ahmed and Palermo [Reference Ahmed and Palermo5] provided detailed recommendations on establishing training programs to increase CEnR. These recommendations emphasized the importance of finding ways to prepare researchers and potential stakeholders to collaborate in the research process and decrease the time to translate findings to patients and communities. This article describes the development of an online curriculum designed as a self-directed resource to increase CEnR in clinical and translational science. The content is easily accessible and contextually relevant to a diverse group of biomedical researchers and stakeholders as they initiate and facilitate CEnR.
Materials and Methods
Program Overview
Our goal was to provide online curriculum in CEnR for faculty, graduate students, residents, fellows, healthcare providers, and community members. The Mayo Clinic Center for Clinical and Translational Science (CCaTS) has created and delivered online course content in CEnR since 2009. In 2011, the Office for Community Engagement in Research (OCER) began providing research consultations to internal and external stakeholders specific to study design, stakeholder identification and engagement, community outreach, and resource referrals. Incremental demand for consultations and assessment of inquiry themes warranted the development of a traditional classroom-based course offered by the Mayo Clinic Graduate School of Biomedical Sciences in the Clinical and Translational Science program, What Every Researcher Should Know About Community-Engaged Research. This initial course generated significant interest, increased awareness, and advanced participants’ knowledge of the principles of CEnR. However, the necessity to attend the course in person and its inaccessibility to those outside the institution undermined the collaborative stakeholder relationships and community-action projects that the course was promoting. In order to remove these obstacles, we created a series of online modules for internal and external self-directed, goal-oriented, project-minded adult learners.
Module Objectives
-
∙ Increase awareness of the fundamental principles of CEnR.
-
∙ Assess readiness to participate in collaborative CEnR partnerships.
-
∙ Identify ways to initiate, facilitate, and sustain community-engaged research partnerships.
CCaTS Education Resources
Education Resources oversees curriculum development for undergraduate, graduate, and professional development programs within Mayo Clinic, and has a long-standing relationship with the Mayo Clinic School of Continuous Professional Development and the Mayo Clinic Graduate School of Biomedical Sciences, both of which are accredited schools within the Mayo Clinic School of Medicine. Mayo Clinic School of Continuous Professional Development has a catalog of over 200 unique education and training opportunities in dozens of disciplines delivered through multiple learning platforms for internal and external learners. Learners can receive continuing medical education (CME) credits from the Accreditation Council for Continuing Medical Education, Accreditation with Commendation, Accreditation Council for Pharmacy Education, American Nurses Credentialing Center, and Maintenance of Certification.
OCER
OCER provides the oversight and determined content needed to make community engagement in research the norm for translational science. OCER is located within CCaTS and is the operational arm of the CCaTS’s community-engaged research structure. OCER provides consultations in person, by telephone, and email to internal and external faculty, graduate students, residents, fellows, healthcare providers, and community members at Mayo Clinic.
Curriculum Design
The curriculum-design team, which included OCER and Education Resources personnel as well as internal and external subject matter experts (SME), created a competency/curriculum matrix (Table 1) to prioritize and develop the modules. Inquiries addressed during OCER consultations and discussions with SMEs provided content materials. They chose the initial 4 topics after a review of the CEnR scientific literature, which also delineated best practices, principles, and models to be included in this foundational curriculum.
Table 1 Module learning objectives

CEnR, community-engaged research.
We have built a searchable library of online modules with links to additional resources at http://ocerblog.mayo.edu/online-courses/. This web-based educational portal facilitates the active dissemination of education, assessment of participant usage, online discussion forums, networking capabilities, and project development and tracking.
Theoretical Framework
We referenced Malcolm Knowles Adult Learning Theory and James Prochaska Trans-Theoretical Model to develop the modules [Reference Knowles, Holton and Swanson8, Reference Prochaska, Redding and Evers9]. We based the curriculum-design process on assumptions that adult learners are self-directed, goal oriented, reliant on relevance, and able to draw on past experiences and previous knowledge. We organized content to foster retention and enable the application of new knowledge and skills. The online modules may be completed independently of each other and are available on demand. Alternatively, learners can progress sequentially through the module guides. The revised constructs of Trans-theoretical Model Stages of Change identify 4 levels of readiness to apply CEnR. These levels are as follows:
-
1. contemplation—the learner desires to gain knowledge of community engagement in research;
-
2. determination—the learner is ready to engage in the research process (there is a project they would like to complete);
-
3. action—the learner acquires stakeholders and implements a research plan; and
-
4. maintenance—the learner has stakeholders, has started or completed a project, and aspires to maintain collaborations and disseminate findings to stakeholders and other communities.
Module Development and Content
Fig. 1 shows the timeline for the creation of the first 4 modules with their release dates. The curriculum-design team worked directly with the SMEs to design content. The SME—with additional support from the curriculum-design team—developed the modules within ~7 hours.

Fig. 1 Curriculum timeline 2014.
The Education Specialist and Curriculum Designer organized content, designed instructional materials, and uploaded modules onto the delivery platforms using PowerPoint and Articulate Storyline software programs. They organized and grouped content to increase retention and application of knowledge. The team used videos, animations, and interactive applications to engage learners in multiple approaches to foster knowledge uptake. Modules are available on the Mayo Clinic learning-management systems for internal and external audiences. The total design time to publish the modules took ~40 hours per module.
Each module contains an interactive presentation and additional reading materials to meet Accreditation Council for Continuing Medical Education accreditation standards for continuing education. Table 1 lists the completed modules with their learning objectives.
The current modules guide learners through the contemplation and determination stages of CEnR. Future modules will facilitate progression through the action and maintenance stages. Each self-paced module is designed to be completed in 25 minutes or less [Reference Smart and Cappel10]. The modules offer additional supplemental content and resources within the platform for learners seeking a deeper immersion. Each module is worth one AMA PRA Category 1 CME credit.
Currently Available Modules
-
1. Community-Engaged Research: An Overview—features asynchronous course content highlighting the principles of CEnR in the context of clinical and translational science. Didactic examples include a comparison of traditional research with community-engaged and community-placed research. Community-engaged stakeholder testimonials provide context to the course material and highlight the importance of engaging stakeholders in the research process. Case studies expand on the role of the community advocate by decreasing the translational science gap.
-
2. Foundations of Community Engagement in Research—summarizes stakeholder theory [Reference Freeman11] and demonstrates the application of theoretical principles through real-life scenarios in diverse environments. A community-engaged clinical and translational scientist describes his experience with a juxtaposition of social problems, health, and collaboration.
-
3. Overcoming Barriers in Community Engagement in Research—highlights a number of barriers to CEnR, provides strategies to build trust and respect among community stakeholders and biomedical researchers, and, through an expert testimonial, discusses how to maintain a long-standing research partnership. The module emphasizes sensitivity to the diversity of stakeholders while designing research plans; it reinforces the importance of community engagement during data collection and dissemination of study findings.
-
4. Measuring Your Readiness & Preparing to Engage—focuses on stakeholders’ readiness to engage in a collaborative research process. Video testimonials showcase both a clinical and a translational scientist—one has a national focus and the other has a more local context aimed at addressing community health concerns. The module includes several interactive educational tools that facilitate the application of concepts related to readiness to engage.
Results
Evaluation
To date, 43 unique learners have completed 75 modules (81% internal; 19% external). The learners include 6 faculty members (including residents and fellows), 17 research and administrative staff, 2 students, 8 others, and 10 community members.
We incorporated a multifaceted evaluation into the curriculum design and delivery process. Frequent formative evaluation takes place throughout the design of the curriculum following the Successive Approximation Model [Reference Allen and Sites12]. Our systematic approach to deliver the curriculum included several assessment checkpoints for soliciting feedback from the SME and the curriculum-design team. The SME and design team managed these checkpoints by videoconferences, teleconferences, and in person. In addition, we used web analytics tools to measure page views, user demographics, navigation through module, and duration of time the module was “open;” pages viewed were also tracked upon exiting the module. We collected outcome evaluation data through CME credit requests, postcourse surveys, and qualitative interviews. This robust amount of data was transformed into information for the group to discuss and inform decision making for improvement purposes. This interactive evaluation practice provides context and content for future revisions of existing modules [Reference King and Stevahn13].
Despite as-yet limited evaluation data, an initial analysis suggests that the modules are well received; the majority of respondents reported that they are of fair-to-excellent quality, meet educational needs, and increase their intent to learn more about CEnR (Table 2).
Table 2 Learners’ evaluation of modules
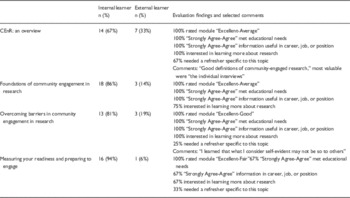
CEnR, community-engaged research.
Discussion
The creation and delivery of online education modules ensure that all stakeholders in CEnR can advance their awareness, knowledge, and skills in this growing area of research. These resources are critical to the success of investigators, clinicians, and community members initiating and facilitating community-academic relationships [Reference Ahmed and Palermo5]. Our ongoing analysis confirms the feasibility, ease of use, and satisfaction of this type of web-based, online educational modules for a diverse internal and external audience.
Future Directions
Our curriculum plan includes the creation of additional modules with content specific to outreach, recruitment, dissemination, and implementation of CEnR. We plan to link the modules to social media platforms as well as our collection of digital stories (testimonials) from faculty and community partners to enhance learning opportunities [Reference Lal, Donnelly and Shin14].
Colleagues at other minority-serving academic medical centers have asked to utilize the modules in their health disparities and community-engaged research training programs. One community advisory board has already successfully used the modules for training their members on the principles of CEnR; the first module served as a mechanism to spark dialog about research. We will continuously evaluate this curriculum to provide the most appropriate training for diverse learners interested in increasing CEnR in clinical and translational science.
Declaration of Interest
The authors report no conflicts of interest.
Acknowledgments
The authors thank the following groups from Mayo Clinic: the CCaTS Education Resources Continuous Professional Development Program; eLearning Design and Development Center; the Office of Applied Scholarship and Education Science; the Mayo Clinic Online Learning, Center for Social Media; Public Affairs; and Marlené Boyd for assistance with manuscript submission.
Financial Support
This publication was made possible by CTSA grant number UL1 TR000135 (Dr Sundeep Khosla, Principal Investigator) from the NCATS a component of NIH. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH.




 Open access
Open access