



Introduction
There are concerns around online learning initiatives directed at non-Western settings to strengthen research capacity. It is argued they impose Western-centric epistemology, provide unidirectional transfer of standardised knowledge, and neglect local paradigms, culture and expertise (de Sousa Santos, Reference de Sousa Santos2015; Adam, Reference Adam2019; Gallagher and Knox, Reference Gallagher and Knox2019; King et al., Reference King, Forsey and Pegrum2019). These approaches are perceived to reinforce colonial legacies of knowledge production, widen social injustices and overlook the value of different histories and epistemologies in forming a diverse global knowledge (Binka, Reference Binka2005; de Sousa Santos, Reference de Sousa Santos2015; Adam, Reference Adam2019; Gallagher and Knox, Reference Gallagher and Knox2019; King et al., Reference King, Forsey and Pegrum2019). In contrast, scholars call for the decolonisation of knowledge as they question the assumption that Western European modes of thinking are universal and superior (Quijano, Reference Quijano2000). Instead, it is argued that decolonising knowledge has the potential to reach ‘social liberation from all power organized as inequality, discrimination, exploitation, and domination’ (Quijano, Reference Quijano2007, p. 178). According to Tuhiwai Smith, decolonisation is concerned with having ‘a more critical understanding of the underlying assumptions, motivations and values that inform research practices’(Smith, Reference Smith2012, p. 24). Hence, decolonisation is a long-term process that involves divesting colonial cultural, linguistic and psychological legacies and fostering local knowledge production and documentation of indigenous struggles.
In this article, we share our experience of offering a collaborative online course aimed at strengthening research capacity among mental health professionals and researchers (MHPR) in the Gaza Strip (GS) in the occupied Palestinian territory (oPt), and seeking to decolonise knowledge. Our course, ‘Research Methods for Mental Health in War and Conflict’, was developed and delivered by researchers from the Institute of Community and Public Health (ICPH) at Birzeit University (BZU) in the oPt and King's College London (KCL), as part of the project Research for Health in Conflict – Middle East and North Africa (R4HC-MENA). Here, we describe, evaluate and critique the methods we employed to integrate local knowledge and expertise to enable multi-directional learning, and present the participants' evaluation.
Mental health in war and conflict: the case of the Gaza Strip
The excessive burden of mental illness among civilian populations in conflict settings (Steel et al., Reference Steel, Chey, Silove, Marnane, Bryant and van Ommeren2009; Luitel et al., Reference Luitel, Jordans, Sapkota, Tol, Kohrt, Thapa, Komproe and Sharma2013; Silove et al., Reference Silove, Liddell, Rees, Chey, Nickerson, Tam, Zwi, Brooks, Sila and Steel2014; Gammouh et al., Reference Gammouh, Al-Smadi, Tawalbeh and Khoury2015; Naja et al., Reference Naja, Aoun, El Khoury, Abdallah and Haddad2016) urgently requires research to inform mental health policies (Charlson et al., Reference Charlson, Flaxman, Ferrari, Vos, Steel and Whiteford2016; Bosqui and Marshoud, Reference Bosqui and Marshoud2018). In the oPt, it was found that the mental health of Palestinians is adversely affected by the violence and human rights abuse faced in the ongoing Palestinian-Israeli conflict since the West Bank (WB) and the GS fell under Israeli military rule in 1967 (Giacaman et al., Reference Giacaman, Khatib, Shabaneh, Ramlawi, Sabri, Sabatinelli, Khawaja and Laurance2009; Cordesman and Moravitz, Reference Cordesman and Moravitz2005; Madianos et al., Reference Madianos, Sarhan and Koukia2011; Dimitry, Reference Dimitry2012; El Masri et al., Reference El Masri, Saymah, Daher and Aisawi2013; WHO Assembly, 2019). Palestinians in the GS have been under siege since the early 1990s which has destroyed the Strip's economy (Smith, Reference Smith2015). Gazans are denied free access to the WB and abroad, including for much-needed medical and other services. In addition to periodic attacks, Israel waged wars on the GS in 2009, 2012, 2014 and 2021, with thousands dead, injured, displaced and maimed (McCarthy, Reference McCarthy2021).
As a consequence of the siege and ongoing attacks, mental health and psychosocial problems have been identified as significant public health challenges. WHO has reported that an estimated one in 10 people in the GS is affected by severe or moderate mental health disorders (WHO Assembly, 2019). A study of adolescents found 68.9% developed post-traumatic stress disorder (PTSD), 40% moderate to severe depression and 94.9% severe anxiety (Elbedour et al., Reference Elbedour, Onwuegbuzie, Ghannam, Whitcome and Hein2007). Similarly, another study highlighted that 41% of children in the GS had PTSD. Of these, 20% suffered from acute levels of PTSD. The study estimated 305 195 children in the GS need urgent psychological, social and medical interventions (Altawil et al., Reference Altawil, Harrold and Samara2008; El-Khodary et al., Reference El-Khodary, Samara and Askew2020).
While mental healthcare needs are high in the GS, the mental health system is weak. Only about 2% of an already underfunded health budget is earmarked for mental health by the Ministry of Health (MoH). The number of healthcare workers in mental health facilities and private practice is just 11.91 per 100 000 population, consisting of 0.25 psychiatrists, 1.6 other medical doctors, 4.8 nurses, 2.2 psychologists, 2.5 social workers, 0.5 occupational therapists and 36.4 other health or mental health workers (Saymah et al., Reference Saymah, Tait and Michail2015). Regarding staff training, it is estimated that 4% of the training for medical doctors was mental health related, in comparison to 7% for nurses, while non-doctor/non-nurse primary health care workers received no mental health training (Saymah et al., Reference Saymah, Tait and Michail2015).
As well as gaps in mental health training, there is a lack of systematic mental health research, and a need to strengthen the local mental health research capacity (Marie et al., Reference Marie, Hannigan and Jones2016; AlKhaldi et al., Reference AlKhaldi, Alkaiyat, Abed, Pfeiffer, Halaseh, Salah, Idries, Abueida, Idries, Jeries, Meghari, Shaar, Tanner and Haj-Yahia2018). This is partly because MHPR face systemic barriers to learning about, and training in, research methods, mainly because restrictions on civilian movement make it difficult for external educators to visit, and for Gazans to travel for training (Marie et al., Reference Marie, Hannigan and Jones2016; Giacaman et al., Reference Giacaman, Hammoudeh, Kienzler, Massazza and Tamimi2018). This is also emblematic of other war-affected contexts where local researchers struggle to build research capacity due to insecurity, restricted and unsafe movement, language barriers, lack of finance and limited face-to-face training (Zaheer et al., Reference Zaheer, Jabeen and Qadri2015; Bosqui and Marshoud, Reference Bosqui and Marshoud2018; Hameed et al., Reference Hameed, Al Taiar, O'leary and Kaynge2018). Consequently, there are few authors from low- and middle-income countries (LMICs) and war and conflict settings, writing about local mental health issues in international journals. Policy making is mainly based on evidence generated by high-income country (HIC) scholars and interventionists using Western research tools and interpretative frameworks (McKee et al., Reference McKee, Stuckler and Basu2012; Bowsher et al., Reference Bowsher, Papamichail, El Achi, Ekzayez, Roberts, Sullivan and Patel2019; Sukarieh and Tannock, Reference Sukarieh and Tannock2019).
Online learning in contexts of war and conflict
To our knowledge, there is no specific mental health research training in GS as capacity building focuses mainly on mental health service delivery. Nevertheless, in the oPt, online learning forms an essential part of higher education. Palestinian universities developed joint online programmes with international co-operation, such as OpenMed and METHOD (Mikki and Jondi, Reference Mikki, Jondi and Demiray2010). However, online learning in the oPt faces a lack of the following: an online learning culture; infrastructure and availability of necessary technology in households due to high cost, and regular electricity cuts; needs assessment and evaluation surveys among potential learners; sustainable funding; proper accreditation and recognition; educators and the political support and interest in the pedagogic value of online learning and staff development (Mikki and Jondi, Reference Mikki, Jondi and Demiray2010; Khader and Abu-aisheh, Reference Khader and Abu-aisheh2012; Al-Sayyed and Abdalhaq, Reference Al-Sayyed and Abdalhaq2016).
Overall, evidence shows that online learning effectively builds learners' capacity, overcomes insufficient research capacity and reduces the brain drain (International Telecommunication Union, 2006; Zander et al., Reference Zander, Schloeder, Jacobs and Murphrey2006; Dodani et al., Reference Dodani, Songer, Ahmed and Laporte2012; Zaheer et al., Reference Zaheer, Jabeen and Qadri2015). Online learning initiatives provide active, flexible learning with an emphasis on applying knowledge and interaction by combining a mix of pedagogical components focusing on simulation, communication, leadership and mentoring (Mason, Reference Mason2003; Aczel et al., Reference Aczel, Peake and Hardy2008). Online learning courses have also been criticised for their Western-centric focus and unquestioned colonial legacy (Bockstael, Reference Bockstael2017), and for their delivery via corporatised, Western, digital platforms which ‘embed coloniality through digital neo-colonialism’ (Adam, Reference Adam2019, p. 366; Gallagher and Knox, Reference Gallagher and Knox2019). This is further perpetuated by restricting learning opportunities to fee-paying learners; designing and delivering courses solely by Western-based educators and institutions; using unidirectional, standardised, Western educational approaches to diverse international learners; using only Western languages; and lacking content which reflects local needs and culture (Adam, Reference Adam2019). Such approaches assume superiority of Western knowledge systems and overlook the value of incorporating local knowledge, epistemologies and experiences.
While designing and evaluating our online course, we were not only mindful of these challenges, but also aware we were not able to fully overcome them. This was despite the fact we aimed to promote a culture of critical thinking amongst participants, encouraged social interaction and dialogue, stimulated deeper awareness of the social, economic, cultural and political circumstances that shape people's lives and their role in creating social change. We further recognised the fundamental relationship between knowledge and power (Foucault, Reference Foucault2008) and the importance and impact of power imbalance in the educational process (Freire, Reference Freire1984). While our aim was to advance a heterogeneous, global knowledge system reflecting local contexts (Bockstael, Reference Bockstael2017; Vaditya, Reference Vaditya2018; Adam, Reference Adam2019; Gallagher and Knox, Reference Gallagher and Knox2019), we acknowledge that we based our course content on Western epistemic knowledge systems, trying to render them culturally sensitive, while at the same time incorporating diverse paradigms and local knowledge in a reflective manner(de Sousa Santos, Reference de Sousa Santos2015; Adam, Reference Adam2019; King et al., Reference King, Forsey and Pegrum2019). We are therefore cautious that simply adapting Western epistemologies to local realities might inadvertently contribute to perpetuating epistemic oppression whereby local knowledge is, once again, pushed to the margins rather than occupying a central place in knowledge generation and exchange.
Methods
Context
Our online course forms part of the R4HC-MENA project, an initiative funded over 4 years by UK Research and Innovation (UKRI), to strengthen research and policy capacity across four countries affected by conflict: oPt, Lebanon, Jordan and Turkey. As part of this project, our Mental Health and Conflict workstream aims to support interdisciplinary mental health research capacity, by providing training in mental health research methods and creating a sustainable community network for local researchers. Simultaneously, our aim is for UK researchers to gain an increased knowledge and understanding of the epistemology, methods and practices used by researchers in the Middle East and North Africa (MENA) region, integrating this into their worldview, future training and research.
Consistent with the capacity strengthening literature emphasising the importance of collaboration between academic institutions of HICs and LMICs (Curry et al., Reference Curry, Taylor, Chen and Bradley2012; Thornicroft et al., Reference Thornicroft, Cooper, Bortel, Kakuma and Lund2012; Ng et al., Reference Ng, Magidson, Hock, Joska, Fekadu, Hanlon and Henderson2016; Beran et al., Reference Beran, Byass, Gbakima, Kahn, Sankoh, Tollman, Witham and Davies2017), our course was the result of a longstanding partnership between researchers from KCL and BZU. Course materials were developed collectively and equally by teams of academics, research assistants, students and online technicians from both institutions. Except the technicians, all contributors are authors of this article. WH, HH and RG are Palestinians living in the WB. NT is Palestinian British, HK is German, MR is Belgian, all reside in the UK. Connected through almost a decade of collegiality and friendship, this collaboration rests on trust, respect, two-way knowledge exchange and learning.
We set out to reflectively engage with pedagogical approaches, literatures and research, through which we shared an understanding that Western paradigms dominate and influence our work in differential ways. Confronting educational power is challenging, as the Western power-knowledge nexus (Foucault, Reference Foucault1977) is firmly seated in university settings internationally. We came to understand that international collaboration, no matter how equitable it intends to be, is not enough to decolonise pedagogies in ways envisioned by thinkers like Paolo Freire, who fought for a liberated education where those involved can influence political powers by developing their own perceptual and analytical tools (Freire, Reference Freire2013). Nevertheless, we believe it is crucial to work towards a future which challenges current power dynamics by fostering locally-driven knowledge production and use. This could be achieved through longstanding international partnerships, based on equity and solidarity between academics with different experience and knowledge (Bleiklie and Powell, Reference Bleiklie and Powell2005). Our online course has been inspired by this vision.
Development
The course itself took shape when our team from KCL and BZU designed and delivered a face-to-face course, ‘Research Methods for Mental Health in War and Conflict’, at BZU in 2018. Although the course was open to MHPR from WB and the GS, none of the Gazans accepted onto the course were granted permission by Israel to travel to the WB. To overcome this, and to meet the need for mental health research, we decided to deliver the course to Gazans online.
It took about a year to develop and deliver the online course. First, our team reviewed online capacity strengthening literature and publicly available syllabi, identifying a lack of online courses providing qualitative methods training for mental health in conflict settings. These reviews, in addition to the findings of our previously conducted Training Needs Assessment among local Palestinian researchers (Giacaman et al., Reference Giacaman, Hammoudeh, Kienzler, Massazza and Tamimi2018), and participants' feedback following the face-to-face course, provided a robust background to the online course design.
Next, we explored transforming our face-to-face course into an online course with King's Online Service. Although we opted to use the KCL service provider who has expertise and established service provision, our teams from both KCL and BZU collaborated at every development stage through in-person meetings, zoom meetings and online training. An instructional designer trained us in curriculum development, course architecture, good practice for online learning, plus technical and design process. Our priority was to ensure the highest quality, local contextualisation of content, and the relevance to potential participants, while taking into account logistical challenges like lack of electricity and internet broadband in GS. We would have employed a Palestinian online course developer, but, to our knowledge, the local expertise in technology-enhanced learning was limited in the early stages of our course development. Fortunately, such expertise has developed since COVID 19 (UNESCO, 2020).
A major consideration was maintaining equal partnership between KCL and BZU. To ensure KCL would not be the sole owner of the course, we opted against hosting it on the KCL internal KEATS platform, and partnered with the external, UK-based online platform, Future Learn (FL), instead. While FL has extensive experience in delivering online courses across the world, including the MENA region, we are reflexive of the problems inherent in using a corporatised, UK-based platform for further education. Firstly, FL is considered a global platform not only because it is accessible everywhere in the world (Future Learn, 2021a), but also because it is in English, which reinforces the notion that ‘to be global is to be Western’ (Adam, Reference Adam2019, p. 366). Further, systemic inequalities are embedded in platforms such as FL, as they contribute to the privatisation of education and limit the production of courses to ‘top institutions’, which are mostly Western (Future Learn, 2021b). We are conscious that our choice of platform limits our agenda of decolonising education, rendering it ‘partial’ colonial (Bhabha, Reference Bhabha1994; Adam, Reference Adam2019). However, given the systemic barriers resulting from the ongoing military occupation of Palestine, including its tech and education sectors, locally developed online learning platforms are not readily available. Consequently, we resorted to FL, while maintaining close contact and discussions among the team.
Recruitment and evaluation
For course promotion, we used BZU's strong institutional network in GS, advertised through local mental health and psychosocial support organisations, and posted on social media platforms. We received 50 applications from professionals and researchers with Diploma, Bachelor, Master's or Ph.D. degrees. The team created an application ranking sheet, using a scoring system evaluating the overall quality of each application, assessing if the applicant worked or studied in the mental health field, resided in Gaza, or could have accessed similar training through institutional affiliations. English competency was also assessed and justified as the course was delivered in English and it was important to communicate with English-speaking instructors. We are aware that many courses in the medical and health professions are taught in English in the GS, and that the majority of mental health professionals are competent in English. However, it disadvantaged potential candidates with less exposure to Western-style education. Thus, we are mindful that our approach reinforced unequal power dynamics whereby Western approaches to knowledge production and dissemination were privileged. Aware of this weakness, we are currently translating the entire course into Arabic.
The course was delivered in February 2020 with 17 participants (11 women, six men) (Table 1). Among them, 14 participants met the requirements to receive an achievement certificate. Twelve participants (eight men, four women) completed the pre-course questionnaire, and 15 (11 men, four women) completed the post-course questionnaire while four (two men, two women) participated in semi-structured interviews. The pre-course questionnaire asked participants to self-assess their qualitative research skills, state their training needs and highlight their expectations (see Appendix 1 for survey). The results showed participants wanted to learn and strengthen their qualitative analysis skills, specifying thematic and content analysis; ‘choose appropriate methods’, and achieve ‘minimal bias’; conduct research projects independently; and improve research skills, ‘especially during emergency and conflicts’.
Table 1. Demographics of course participants

a Managerial position includes General Directorate, Medical Officer, National Professional Officer, Head of Health Centre, General Manager, Director Assistant.
b Health professional includes Medical Doctor, Nurse, Registered Nurse, Psychologist, Social Worker.
At the end of the course, participants evaluated it by addressing the same topics in the baseline questionnaire for comparative purposes. Participants also rated their agreement/disagreement with statements that captured their course experience and wrote about what they liked or disliked about the course, the challenging components, topics that they would have liked to learn about but weren't taught, and suggestions for future improvements (see Appendix 2 for survey). Quantitative survey results were analysed using SurveyMonkey, an online application with inbuilt software that automatically analyses data.
The semi-structured interviews were conducted with course participants to further understand their perceptions on the pedagogical methods and materials, integrated local knowledge and experiences. Interviewees were also invited to suggest further online course improvements. The topic guide was created by team members from both universities. While a recruitment email was sent to all participants, only four agreed to participate. Unfortunately, the sample was small (four) and involved participants who were all highly satisfied with the course, which created a positive bias. We attempted to mitigate this bias by clearly identifying their reflections in the results section. The interviews were carried out by NT using English or Arabic language, whichever the interviewees preferred. Anonymity and confidentiality were discussed. Three interviews were conducted in Arabic and one in English. They were conducted via Zoom, audio-recorded, lasted approximately 30 min and were transcribed by a professional transcriber (see Appendix 3 for topic guide). The qualitative feedback and interview transcripts were coded inductively and mostly descriptively (Saldana, Reference Saldaňa2012), and analysed using thematic analysis as outlined by Braun and Clarke (Reference Braun and Clarke2006). The analysis was performed by the first author in consultation with both teams at BZU and KCL.
Ethical approval for conducting the surveys and semi-structured interviews was first obtained from the ICPH Ethics Review Committee. The positive outcome was then officially accepted by the Research Ethics Board at KCL MRA-19/20-18045.
Implementation
The course ran over 4 weeks. First, we introduced the course and educators, learning objectives, and certification. To progress from one week to the next, participants had to pass an end of week test. We offered flexible timing, so participants could start and progress at any time. To receive the certificate, they had to complete at least 90% of the course, and score 70% in the tests overall. Certificates were issued jointly by KCL and BZU.
The first week introduced concepts and theories of war, societal violence and health, social suffering, and the qualitative paradigm. The second week addressed qualitative research design. The third week focused on qualitative data collection. The fourth week addressed qualitative data analysis and presenting research findings. Sessions were co-designed and taught by academics from both universities. Delivery methods included articles, discussions, exercises, quizzes, videos and end of week tests. Participants received personalised feedback from the teaching team for most exercises (Table 2). We employed the following methods to integrate local expertise and knowledge:
• Case studies
Table 2. The delivery method for each week's topics
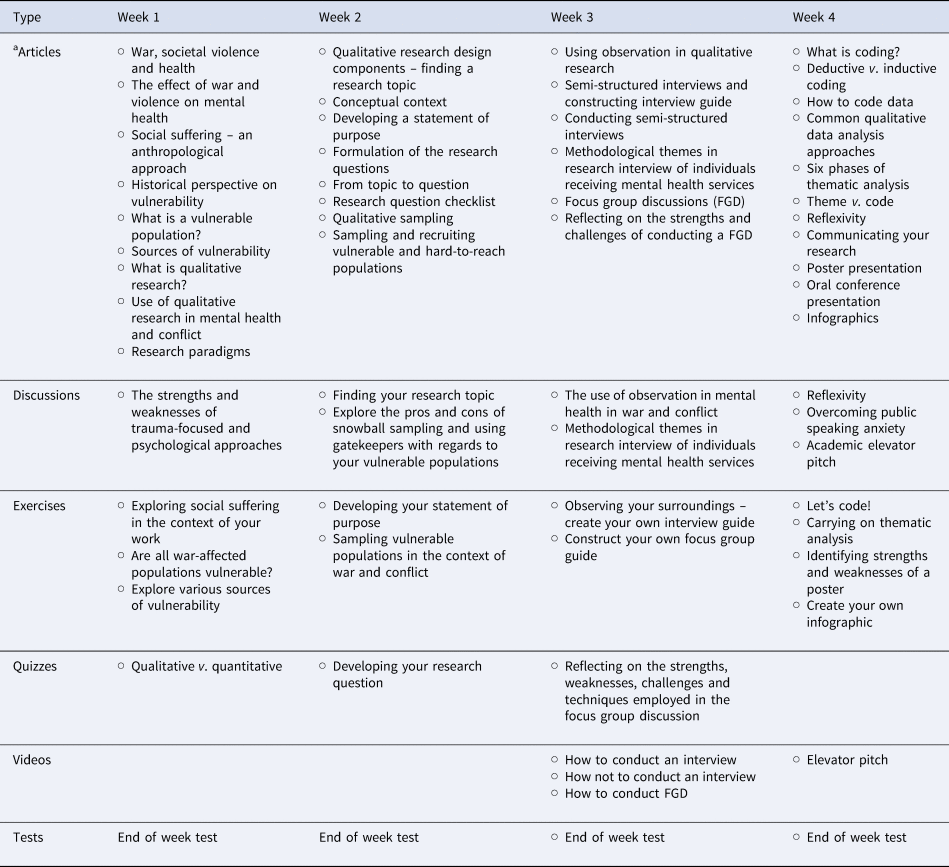
a Articles refer to text materials written by the educators of the online course.
Included were case studies reflecting the mental health situation in Palestine and that of other conflict settings such as Afghanistan, Turkey, Serbia and Bosnia.
• Video production
Teaching videos about conducting semi-structured interviews, focus group discussions and an academic elevator pitch were created with support from KCL and BZU online teams. Topics and conversations focused on themes relevant to the Palestinian context.
• Dialogic, open discussions
Open discussion threads were offered for topics, encouraging participants to share their professional and research experiences, with the option to communicate in Arabic and English. We monitored and engaged with discussions daily. Input by participants included providing feedback on the course content, sharing examples and experiences, asking questions and engaging in peer discussions. Here is one example where a learner reflects on ethical considerations in research:
Maintaining privacy and anonymity is quite important for victims of torture. Such [a] vulnerable group [is] sensitive and fragile, especially if the case is a woman or a child. As a researcher, I will ensure building a trust relationship with the case before requesting them to sign a consent form for observation purposes.
• Multi-directional learning
We regarded our learners as experts, and encouraged them to link their learning to their personal experience. Reflective exercises helped us learn from participants, e.g. participants discussed characteristics of a vulnerable population in oPt and obstacles of recruitment, and described and presented research topics linked to the local context, such as, ‘Psychological disorders during the war among displaced families living in shelters’, and ‘Mental health and coping mechanisms among the medical team of emergency departments in GS hospitals during 2014 war’.
• Critique of Western adopted theories
We encouraged participants to address the relevance and applicability of Western adopted theories to the local context, stimulating reflections and locally-derived concepts. The following exchange between a participant and educator is exemplary:
Learner: When we want to study suicide, we commonly use the interpersonal theory (…) The theory explains the suicidal behaviour based on three components: the perceived burdensome, the acquired capacity to suicide, and the thwarted belonging.
Educator: This is one of the most popular theories in suicidology and has been used widely in the literature. However, some scholars questioned if the theory explains all suicides everywhere; rejecting the idea of the ‘universal truths’ that can be applied to all suicides; and highlighting that suicide is a complex, multi-factorial phenomenon and a highly contextual phenomenon. I wonder if you think such a critique is warranted when researching suicide in Palestine?
Learner: I totally agree with you. There are several limitations to Joiner's theory that can be observed from the suicidal cases in Gaza. Here, the psychological component within the focus of Joiner's theory, is highly dependent on the economic and social factors, in addition to the impulsive behaviour.
Results: course evaluation and feedback
Pre-course survey compared to post-course evaluation
Our pre-course survey showed a gap between various research tasks participants considered important, and their self-assessed ability to perform these well. The biggest gap was coding and analysing qualitative data, followed by using data for planning projects, communicating research findings and accurate data record keeping (Table 3).
Table 3. Participants’ pre-course training needs identification

The post-course survey showed a small, or no, gap between most research tasks participants considered very or moderately important, and their self-assessed ability to perform them well, or very well. The results indicated no gap in developing an appropriate research objective, designing research projects, identifying ethical concerns and communicating research findings.
Later, we compared the pre- and post-course surveys. The findings showed a tangible improvement in the participants' reported qualitative research skills. The number of participants who indicated their ability to perform all the research activities very well after the course was consistently higher than those who indicated a shortfall before the course. For example, before the course, only two participants noted they could develop an appropriate research objective very well, six well and two moderately well, while after the course, six noted very well and eight well (Chart 1).

Chart 1. A Comparison Between Pre- and Post- Course Questionnaires. How well participants thought they could carry out a particular activity before and after the training.
Course delivery evaluation
All participants were highly satisfied with the course. Of the 14 who completed the evaluation, 10 strongly agreed, and four agreed that the course improved their qualitative research skills. The majority strongly agreed or agreed that the course was delivered well, that topics were covered comprehensively, that examples were relevant and informative, that discussions were stimulating, that exercises improved learning, and that the interaction with course participants expanded their knowledge (Chart 2).

Chart 2. Course Delivery Evaluation.
Qualitative course evaluation feedback and semi-structured interviews
Themes that were identified based on our thematic analysis included (1) the course was locally contextualised and met students' needs; (2) the course fostered dialogic and multi-directional learning and (3) suggestions for improvements. Notably, participants did not explicitly talk about, or criticise, the imposition of Western-centric epistemology, unidirectional knowledge transfer, neglect of local paradigms and notions of expertise. This may have been because the open-ended survey questions did not include probes into these topics and the semi-structured interviews were conducted with highly satisfied participants, who felt the course had catered to their expectations and needs.
Theme 1: the course was locally contextualised and met students' needs
Participants praised the accessibility of the course for Gazans who rarely get the opportunity to attend international training. One interviewee said, ‘There is no way to go out to travel, to communicate with people like you, so you are coming to us through these courses, so I do appreciate it’. Others praised the local relevance of the course. For example, one interviewee said:
This course was exactly what we needed for researchers in Gaza, we have so many conditions like wars, conflicts, mental health issues, but we need to know how to correctly do research, [and] how to collect data regarding these issues specifically. It's not like a general issue, it's like unique issues in Gaza, so I guess this course exactly touches on what we need.
Some participants commented that studies from other conflict regions had enriched their knowledge and widened their perspectives. One interviewee said, ‘With Palestinians, with refugees in Syria and other countries, we have some things in common, but when other examples like in Africa or in other countries, it added to my knowledge’.
Overall, participants found the course coherent, comprehensive and ‘full of valuable details’. Participants especially praised the diverse training methods. One interviewee said, ‘This course was one of the most amazing online training I had’, and described applying what she had learned during the course to improve her Master's research project: ‘I changed some of the techniques I was applying when I was collecting data based on the information provided in this course’. Other participants emphasised the course taught transferrable skills applicable to their jobs, which involve monitoring, evaluation and need assessment. One said: ‘It provides me with new knowledge and skills regarding the qualitative research theories, coding, analysis and findings presentation’.
Regarding technological aspects, accessibility and flexibility of the course delivery, participants liked our video content and, in particular, the FGD video produced at BZU that touched on the challenges people face in GS. It was also positively noted that the course format provided ‘the possibility of studying at any time’ and that the material was downloadable to access during electricity cuts. Only a few anticipated more advanced training, but confirmed the course consolidated their existing skills. For the majority, however, the course filled a gap in their qualitative capabilities.
Theme 2: the course fostered dialogic and multi-directional learning
Participants praised the interactive element with other participants and educators which they considered ‘very effective’. They appreciated the opportunities to participate and did not feel they were ‘at the receiving end’. During a semi-structured interview, one participant said, ‘Encouragement for discussions among participants inspired me to participate and interact’. Another interviewee praised the opportunity to initiate debates. Another participant said,
I can't say it is one direction, you used many of the technology or many of the skills, or the methodology, I guess two ways, because you were interactive, you are not just giving us the course online and not answering and submitting only. Through that course, we had discussions and what I appreciate that every comment we gave I found someone is answering my comment and discussing it with me.
Participants also liked the mix of local and non-local educators as it enriched their knowledge of other cultures and experiences.
From a critical perspective, a few participants were disappointed by the lack of engagement by some fellow participants. While acknowledging this could be due to work-life commitments, they proposed incorporating live components, or stringent enrolment criteria, with mandatory participation. They considered that exchanging experiences was a vital part of learning.
Theme 3: suggestions for improvements
While some participants found the course ‘easy’, others found several new topics challenging, such as how to define a relevant sample, coding and extracting themes. One participant described some of the content as ‘heavy meal of information [that] need[s] time to digest’. Other participants suggested the course run for longer, with more practical examples. One interviewee preferred to do more research tasks and critical analysis rather than quizzes, and suggested ending the course with a research project to present at a follow-up course. A few also wanted advanced training in topics such as participatory approaches and mixed methods. Several participants proposed conducting research supervised by course instructors, highlighting that research collaboration with Western institutions facilitates global visibility of local researchers. Participants suggested incorporating more interactive elements such as ‘online discussion’, ‘open meeting with trainers’ and ‘webinar sessions’. Finally, although the majority did not consider the English language a personal obstacle, with a few highlighting the vitality of English competency to reach the global audience, it was noted that ‘some highly qualified professionals might find the English language an obstacle’, and suggested providing course materials in the Arabic language.
Discussion
Our online course aimed to strengthen the qualitative research capacities of MHPR in the GS to empower them to conduct high quality and locally relevant mental health research. To our knowledge, it is the first training delivered in the GS combining the fields of mental health, qualitative research methods and conflict, while addressing the ‘digital neo-colonialism critique’ (Binka, Reference Binka2005; de Sousa Santos, Reference de Sousa Santos2015; Adam, Reference Adam2019; Gallagher and Knox, Reference Gallagher and Knox2019; King et al., Reference King, Forsey and Pegrum2019).
Our pedagogical practice was shaped by the awareness of inherent inequalities in global health research related to unequal access to resources, scientific information, high-quality training and opportunities for knowledge dissemination (Minn, Reference Minn2015; Murphy et al., Reference Murphy, Hatfield, Afsana and Neufeld2015). It was also informed by critical pedagogy which exposes the domination and propagation of Western knowledge generally (Freire, Reference Freire1984; Thiong'o, Reference Thiong'o and Mkandawire2005; Fanon, Reference Fanon2008), as well as in the digital realm of online training courses more specifically (Adam, Reference Adam2019). In order to destabilise hegemonic practices to knowledge generation and dissemination, we tried to create spaces for a plurality of knowledges, experiences and histories to co-exist (Adam, Reference Adam2019).
To achieve this, we employed a combination of methods for course development, content and delivery which enabled multi-directional learning, and integration of local paradigms and expertise (de Sousa Santos, Reference de Sousa Santos2015; Adam, Reference Adam2019; Gallagher and Knox, Reference Gallagher and Knox2019; King et al., Reference King, Forsey and Pegrum2019). Firstly, the course was the result of a longstanding collaboration between researchers from KCL and BZU, and the course materials were developed equally by a team of academics, research assistants, students and online technicians from both institutions. It has been shown that creating equal partnerships between academic institutions in HICs and LMICs is the optimum approach to ensure sustainable academic relationships, and to strengthen research capacities of new generations of local health professionals (Lansang and Dennis, Reference Lansang and Dennis2007; Gezmu et al., Reference Gezmu, DeGruttola, Dixon, Essex, Halloran, Hogan, Grobler, Kim, McDermott, McKaig and Neaton2011; Fricchione et al., Reference Fricchione, Borba, Alem, Shibre, Carney and Henderson2012; Thornicroft et al., Reference Thornicroft, Cooper, Bortel, Kakuma and Lund2012; Semrau et al., Reference Semrau, Alem, Abdulmalik, Docrat, Evans-Lacko, Gureje, Kigozi, Lempp, Lund, Petersen, Shidhaye, Thornicroft and Hanlon2018).
Secondly, our course content addressed a locally identified need for qualitative research training among MHPR (Giacaman et al., Reference Giacaman, Hammoudeh, Kienzler, Massazza and Tamimi2018). We incorporated relevant local and regional case studies, and accounted for the logistical challenges relating to electricity and Internet broadband.
Thirdly, our delivery fostered interaction, engagement, active and multi-way learning (Mason, Reference Mason2003; International Telecommunication Union, 2006; Zander et al., Reference Zander, Schloeder, Jacobs and Murphrey2006; Aczel et al., Reference Aczel, Peake and Hardy2008; Dodani et al., Reference Dodani, Songer, Ahmed and Laporte2012; Zaheer et al., Reference Zaheer, Jabeen and Qadri2015) by encouraging participants to share their expertise and local experiences, and by critically reflecting on the applicability of Western concepts and paradigms to their local realities. We also promoted dialogic and open discussions among participants and educators, with the option to communicate in Arabic and English. While such pluralistic and multi-directional learning has been shown to improve cultural competencies, research design and methods (Murphy et al., Reference Murphy, Hatfield, Afsana and Neufeld2015), we were conscious that our training material itself was not as diverse. Even if mostly authored by scholars from the MENA region, it was heavily informed by Western approaches to knowledge generation and interpretation and, thus, not free from neo-colonial agendas which emphasise Western modes of knowing and suppress, or marginalise, indigenous ways of organising and conceptualising reality (Thiong'o, Reference Thiong'o and Mkandawire2005; Minn, Reference Minn2015; Adam, Reference Adam2019). Our course is one step towards decolonial approaches that should involve more systemic and broader level change across the board.
Despite these limitations, the overall course feedback showed the course was well-received, leading to reported improvement in qualitative research skills. Participants felt their experiences, voices and local knowledge were incorporated and valued. Overall, the main strength of our course was its local relevance and contextualisation. However, course participants also highlighted course limitations and suggested improvements. They strongly highlighted that they would have liked to explore their different viewpoints and expertise in greater depth with each other and the course organisers via video conferencing platforms. We agree such an exchange could have led to more effective multi-way learning, critical reflections and ongoing suggestions for course improvement.
Other specific practical issues warrant reflection when developing similar training. Firstly, due to the large number of needs identified, only those of the highest demand, and essential to research, could be addressed in our course. Although few participants asked for specific topics to be taught and for others to be expanded, several found the content dense. To meet both requirements, further advanced courses could be designed building on this course and incorporating lessons learned. For future online courses, we recommend providing less dense content and offering follow-up opportunities combined with synchronously delivered drop-in sessions.
Secondly, we became aware of the huge costs and administrative challenges (Leary and Berge, Reference Leary and Berge2006) because the material had to be developed specifically for the course, not simply converting traditional learning material to online material; so, we recommend designing material specific to the targeted audience, which combines a plurality of local and international epistemologies and case studies. Although our team reviewed course material, we recommend an independent reviewer from the respective conflict region to read the material critically.
Thirdly, since we believe evidence-based capacity strengthening is needed for mental health system strengthening (Hanlon et al., Reference Hanlon, Semrau, Alem, Abayneh, Abdulmalik, Docrat, Evans-Lacko, Gureje, Jordans, Lempp, Mugisha, Petersen, Shidhaye and Thornicroft2018), we attempted to capture the immediate outcome of our course by conducting pre- and post-course assessments and interviews with participants. However, due to budget, resource and timeframe restrictions, it is difficult to measure changes in capacity, and its impact, in the longer term (Vallejo and Wehn, Reference Vallejo and Wehn2016). Although our interviews showed a short-term positive impact, we stress the need for multi-path approaches to capture capacity changes and to evaluate their sustainability and impact over the medium, or long term (Vallejo and Wehn, Reference Vallejo and Wehn2016; Bowsher et al., Reference Bowsher, Papamichail, El Achi, Ekzayez, Roberts, Sullivan and Patel2019). Positive long-term impact would be course participants leading on publications, grants and academic production, based on locally identified needs, and carried out through locally developed research designs, methods and modes of interpretation (McKee et al., Reference McKee, Stuckler and Basu2012; Bowsher et al., Reference Bowsher, Papamichail, El Achi, Ekzayez, Roberts, Sullivan and Patel2019; Sukarieh and Tannock, Reference Sukarieh and Tannock2019).
Fourthly, to develop and implement courses like ours, it is important to ensure sustainability through funding, collaboration, research output and policy impact (Aczel et al., Reference Aczel, Peake and Hardy2008; Siriwardhana et al., Reference Siriwardhana, Sumathipala, Siribaddana, Samaraweera, Abeysinghe, Prince and Hotopf2011; Vallejo and Wehn, Reference Vallejo and Wehn2016; Franzen et al., Reference Franzen, Chandler and Lang2017). As our funding is time limited, we will have to make the course fully open access and sign some of our rights over to the FL platform for it to continue. The course will therefore become more commercial (while participants will be able to access learning material for free, they will have to pay for the course certificates), and, consequently, inequalities arise that are not in line with our pedagogical stance.
Overall, the development and implementation of this course was as much a learning experience for us as course developers, as it was for our participants. We became aware of the practical difficulties our learners face on the ground when conducting research, the limited and short-term learning opportunities, and the lack of continuous professional development to meet their needs. We were impressed by the resilience our participants showed, and their determination to produce high-quality local research, committed to exposing the living experiences and suffering of Gazans through contextually relevant frameworks that require critical engagement with theory and method. Although we do not claim to have overcome epistemic oppression, and are a long way from decolonising knowledge production and dissemination, we were pleased that the multi-directional nature of learning on our course allowed participants and instructors to swap roles at any point, and pushed against the assumed confines and directionality of some capacity strengthening models, whilst overcoming geopolitical borders imposed by military occupation and siege.
This course exemplifies early attempts to address the domination of Western knowledge in the developing world, including the oPt. Much needs to be done, given that educational and health systems are still largely dominated by Western epistemology, approaches and knowledge production. While this is the legacy of colonialism and post colonialism, it indicates the need to address the problem not only from a one-off training course, but also by systematically examining educational and health systems, working towards equalising power relationships, and relating epistemologies and knowledge to their relevance and appropriateness to the local context.
To this end, this project represents the beginning of what should be an ongoing project, seeking to make systems approaches more relevant and appropriate to context. Working in a settler colonial context, we are deeply aware that the hegemony of the Israeli state over the Palestinian society transcends to the academic arena, makes decolonising knowledge production a constant struggle for local and non-local researchers. Hence the importance of our course and similar efforts to strengthen research capacity with the vision of resisting the repression of indigenous knowledge and experience while building equitable international research partnerships. It is also essential to enhance the capacity and seek to employ local expertise at different levels, such as educators and technology-enhanced trainers and providers.
Conclusions
In this article, we shared our experience of providing an online qualitative research method course, designed and delivered equally by KCL and BZU, for MHPR in GS. We described methods employed to address digital neo-colonialism, and presented findings of the pre-course need assessment, post-evaluation and semi-structured interviews. To achieve sustainable and locally responsive online research capacity in conflict settings, a plurality of voices, histories and epistemologies must be valued and integrated. Our future outlook is to improve the online course. We will reduce the density of the content, include live, interactive sessions, and provide the course content in Arabic and English. While doing so, we aim to foster multi-directional learning to ensure that non-Western knowledge, epistemologies and languages gain a prominent presence in the Western academic world. We believe a real social transformation would see local researchers and educators confidently engage with, and use, local methods and paradigms in the international realm as they design projects, collect data and develop theories for mental health in war and conflict.
Acknowledgements
The authors would like to thank the course participants for sharing their insights, experience and valuable feedback on the course.
Financial support
Funding was received from the UK Research and Innovation GCRF Research For Health in Conflict (R4hC-MENA), developing capabilities, partnerships and research in the Middle East and Near East (MENA) ES/P010962/1. The funding body has no role in the design of the study and collection, analysis and interpretation of data, and in writing the manuscript.
Conflict of interest
None.
Ethical standards
Ethical approval was obtained from the ICPH Ethics Review Committee and the Research Ethics Board of KCL (Ethical review reference number: MRA-19/20-18045).
Appendix 1
The pre-course questionnaire

Appendix 2
The post-course questionnaire

What did you particularly like about the course?
What did you dislike about the course?
Were there any components of the course that you found challenging to understand?
Were there any topics that you wished to be covered and were not included in the course? If yes, please list them
How do you think the course could be improved?
What kind of follow-up training would you like to receive?
Appendix 3
Interview guide:
Name:
Gender:
Date of birth
Professional affiliations:
Job title:
1) Please read the following statement to discuss in link with our course. “Research capacity in conflict environments is characterized by unidirectional knowledge transfer, imposition of Western knowledge, and neglect of local expertise”.
2) Do you think your learning experience would have been different if the course had been designed and delivered either (a) only by Palestinian researchers and teachers or (b) only British researchers and teachers?
3) How sensitive is the training course to the needs and skills of the participants? Please think about the positive and negative aspects.
4) To what extent does the course value and integrate the participants' knowledge and experience? Please think about the positive and negative aspects.
5) What are your thoughts on the case studies that were used in the course? Do you feel that they reflect the local and regional context in which you live and work? If so, how? If not, why not?
6) How successful was the course in stimulating ideas about local concepts and experiences? Please think about the positive and negative aspects.
7) What do you think about the fact that the course content and exercises are written in English? Do you think that your participation would have been different if the course was in Arabic? If so, why?
8) Were you able to use any part of the course material, conceptual, methodological or other, in your work/research/studies? Usage does not necessarily mean only systematic or practical, but can also mean how to visualize problems in different ways compared to before taking the course?
9) In your opinion, how can the course be improved to be more responsive to local needs and aspirations?
10) Is there anything else you would like to add?
1) يرجى قراءة المقطع التالي والتفكير فيه فيما يتعلق بدورتنا: في الأبحاث قيل أن "التعلم عبر الإنترنت المستخدم لتعزيز ". القدرة البحثية في بيئات الصراع يتميز بنقل المعرفة أحادي الاتجاه ، وفرض المعرفة الغربية ، وإهمال الخبرة المحلية مناقشة
2) هل تعتقد أن تجربة التعلم الخاصة بك كانت ستختلف لو تم تصميم الدورة وتقديمها إما (أ) فقط من قبل الباحثين والمدرسين الفلسطينيين أو (ب ) من قبل الباحثين والمعلمين البريطانيين فقط؟
3) ما مدى مراعاة الدورة التدريبية لاحتياجات المشاركين ومهاراتهم؟ يرجى التفكير في الجوانب الإيجابية والسلبية.
4) إلى أي مدى تقدر الدورة وتدمج معارف وخبرات المشاركين؟ يرجى التفكير في الجوانب الإيجابية والسلبية.
التي تم استخدامها في الدورة؟ هل تشعر أنها تعكس “case studies” 5) ما هي أفكارك حول دراسات الحالة السياق المحلي والإقليمي الذي تعيش فيه وتعمل فيه؟ إذا كان الأمر كذلك ، فكيف؟ إذا لم يكن كذلك ، فلماذا لا؟
6) ما مدى نجاح الدورة في تحفيز الأفكار حول المفاهيم والتجارب المحلية؟ يرجى التفكير في الجوانب الإيجابية .والسلبية
7) ما رأيك في حقيقة أن محتوى الدورة والتمارين مكتوبة باللغة الإنجليزية؟ هل تعتقد أنك مشاركتك كانت ستختلف لو كانت الدورة باللغة العربية؟ إذا كان الأمر كذلك، لماذا؟
8) هل تمكنت من استخدام أي جزء من مادة الدورة التدريبية ، المفاهيمية أو المنهجية أو غيرها ، في عملك / أبحاثك / دراساتك؟ لا يعني الاستخدام بالضرورة منهجيًا أو عمليًا فحسب ، بل يمكن أن يعني أيضًا كيفية تصور المشكلات بطرق مختلفة مقارنةً بما قبل أخذ الدورة؟
9) في رأيك ، كيف يمكن تحسين الدورة لتكون أكثر استجابة للاحتياجات و التطلعات المحلية ؟
10) هل هناك أي شيء آخر تود إضافته؟






 Open access
Open access