



Mass gathering events (MGE), described as groups of more than 1000 persons assembled in a specific place for a defined time,Reference Locoh-Donou, Guofen, Welcher, Berry, O’Connor and Brady1 with limited access to patients and the increased risk of delayed response to medical emergencies,Reference Arbon2 can represent a complex task for local emergency medical services (EMS). Even if this range of events usually involves the participation of mostly healthy people, the rate of illnesses and injuries is higher than in the general population.Reference Arbon, Bottema and Zeitz3 The organization of appropriate on-site medical assistance is a key point to guarantee adequate response to emergencies, and to avoid unnecessary overload to local ambulance services and emergency departments.Reference Milsten, Maguire, Bissell and Seaman4 The risk assessment process related to medical care at an MGE must consider not only the number of attendees, but also a wider range of environmental factors such as location (indoor/outdoor, and seated/unseated), crowd density and behavior, weather conditions, alcohol and drug consumption, and others.Reference Locoh-Donou, Guofen, Welcher, Berry, O’Connor and Brady1,Reference Arbon, Bottema and Zeitz3-Reference Turris, Lund and Hutton5
NARRATIVE
Centrale Operativa 118 Area Omogenea Emilia Est EMS provides assistance every year to a series of MGEs in the area of Bologna, such as street parades, football matches, and concerts with up to over 40000 participants. The management of an international event offered an opportunity to experiment with a different approach in the EMS organization.
The Union of European Football Associations’ (UEFA) Under-21 tournament, which held from June 10 to 27, 2019 required emergency medical assistance during 4 official soccer matches. All matches were held at the municipal stadium Renato Dall’Ara, with a total capacity of 32000 seated spectators. The number of spectators for the 4 matches was 72655, with almost full occupancy of the stadium during the Italian football team matches. Total attendance, including stadium staff and other on-site workers such as police officers and firefighters (minimum of 757, maximum of 882), was 76030.
The on-site medical resources were structured on the Maurer algorithm, as stipulated by the Italian law on MGE organization.Reference Neri6 Medical assistance in the stadium involved 68 operators for each match. The emergency department of Maggiore Hospital, a tertiary emergency trauma centre, is located a distance of 2.3 kilometers away.
Patient Presentation Rates (PPR), calculated over the total attendant number, ranged from 0.11 to 1.35, with a mean value of 0.41; the majority of patients suffered minor illnesses or injuries, and were treated within the venue. Mean Transport To Hospital Rate (TTHR) was 0.08 (min 0.04, max 0.12); one patient was transported to the hospital for a severe traumatic brain injury after a fall from the stands. The detailed data are reported in Table 1.
TABLE 1 Event details
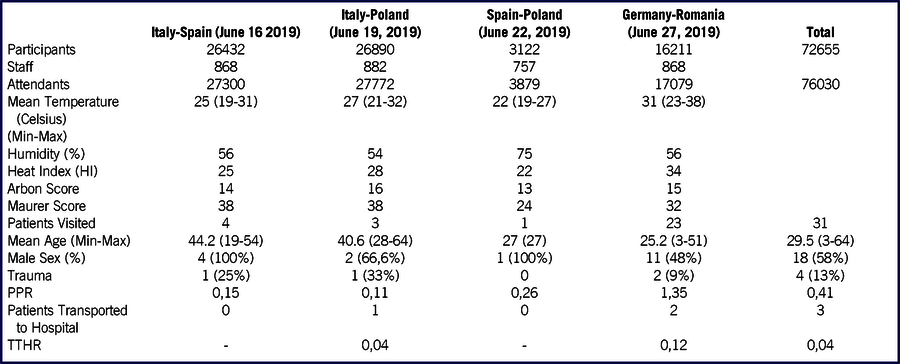
Staff included stewards, players, and team staff, European and Italian soccer federations personnel, referees, volunteers, police officers, firefighters, and medical teams.
PPR and TTHR have been calculated from the total attendant number (participants + staff).
Abbreviations: PPR, Patient Presentation Rate; TTHR, Transport to Hospital Rate
This field report describes patient presentation, environmental features, organization, and usage of emergency medical resources and personnel during the UEFA matches held in Bologna in June, 2019. Data were collected in an electronic database by the nurse coordinator of each event, and subsequently analyzed in an Excel spreadsheet, version Office Professional Plus 2019 (Microsoft Corporation, Redmond, WA), presenting basic statistical variables (mean values and percentages). Standardized measures were calculated as follows: PPR - patients presenting per 1,000 spectators, and TTHR - patients transported to hospital per 1,000 persons in attendance. Heat Index (HI), representing the ‘perceived temperature’ based upon temperature and humidity, was calculated with an online calculator provided by U.S. National Weather Service (https://www.wpc.ncep.noaa.gov/html/heatindex.shtml).
Institutional EMS in Bologna is historically based upon a collaboration with the local area volunteer ambulance associations. The different resources (physicians, emergency nurses, and volunteer rescuers) deployed for standard emergency medical assistance during football matches were calculated using the Maurer score and the historical experience developed during local football championship matches. The number and type of personnel were adapted according to our EMS organization, using teams of 4 rescuers instead of 3, to ensure safe transport with stretchers from the stands, and using emergency nurses as an intermediate level of care. The Arbon score overestimated in 3 matches, and underestimated in one, the number of participants who effectively requested medical intervention.Reference Arbon7
In addition to medical assistance during the game, it was necessary to guarantee an adequate number of personnel in the streets surrounding the stadium, closed to traffic, where people waited for the opening of the gates between food stands and merchandise shops. Two ambulance spots and two bicycle responder teams, each comprising a nurse and a volunteer rescuer with E-bikes equipped with AED and medical devices, were planned for quick responses over an optimal coverage of a 9.5 square kilometer pedestrian area. During the game, medical resources were deployed into the stadium as follows:
-
10 Basic Life Support (BLS) teams of 4 volunteer rescuers over the stands (equipped with scoop stretchers, AED and emergency backpacks);
-
2 teams of 4 operators at the base of the stands (equipped with wheeled stretchers to transport patients to the medical posts);
-
2 ambulances with 1 emergency nurse and 1 emergency physician, located at the two sides of the stadium (equipped with emergency and resuscitation equipment);
-
1 team (1 emergency nurse and 3 volunteer rescuers) and 1 Advanced Life Support (ALS) team (1 emergency physician, 1 emergency nurse, and 1 rescuer) for intervention within the pitch.
E-bike teams were available in the inner ring of the stadium and ensured rapid intervention by an emergency nurse. This type of organization allowed every patient rescued by volunteers over the stands, to be promptly evaluated by a nurse and if necessary accompanied to the physicians’ stations.
PPR during the UEFA Under -21 championship in Bologna was comparable to previously described international experiences. Analysis of the environmental elements of the 4 matches showed a positive relationship between elevated temperature and HI, as recorded during match 4 (Germany-Romania, 31°C, and 34 HI), with an increased PPR, three times higher than the average of the whole set of matches. Ironically, we can hazard that when free water is not available, patrons prefer to spend their money buying beer rather than bottled water. Absence of free water and increased alcohol consumption due to the hot weather may have contributed to a greater request for medical intervention. Most of the patients were visited and treated in the medical facilities in the stadium.
DISCUSSION
One of the main objectives during medical assistance in MGE is to provide evaluation and treat illnesses and trauma with adequate resources on site, without affecting the local ambulance service and emergency department. To fulfil this task, a preventive evaluation of the number and type of healthcare personnel necessary for every MGE is mandatory. Even if the local experience developed during similar events can be useful to predict medical usage, accurate planning should consider a wider range of factors in addition to the simple number of tickets sold, usually considered as the main variable by the public authorities.Reference Turris, Lund and Hutton5,Reference Lund, Turris and Bowles9,Reference Hartman, Williamson and Sojka10 Studies and theories identify MGE as a complex interaction of different factors such as the type of event (e.g., concert, parade, football match), location (indoor/outdoor and seated/unseated) and the participants’ ages. Other elements like unavailability of free water, alcohol and/or drug consumption, weather (temperature and humidity), and crowd behavior are reported to be determinants which increase the risk of emergencies.Reference Locoh-Donou, Guofen, Welcher, Berry, O’Connor and Brady1,Reference Turris, Lund and Hutton5,Reference Locoh-Donou, Yan and Berry11 Football events, and particularly derby matches, are reported to have higher PPR when compared to other types of MGE.Reference Locoh-Donou, Guofen, Welcher, Berry, O’Connor and Brady1,Reference Locoh-Donou, Yan and Berry11 Absence of free water accounts for a 71% increase in PPR; alcohol consumption may cause falls and illnesses, and is associated with a 12% increase in PPR.Reference Arbon, Bottema and Zeitz3,Reference Locoh-Donou, Yan and Berry11
A series of studies describe a positive correlation between high temperature and the number of participants requiring medical assistance; furthermore, high temperature may lead to increased alcohol consumption, particularly when free water is not available. HI has been identified as an important variable in predictive models of MGE.Reference Arbon, Bottema and Zeitz3,Reference Baird, O’Connor, Williamson, Sojka, Alibertis and Brady12-Reference Marino, Albergoni and Andreassi14 PPR described in previous researches varies from 0.14 to 90/1000 with the majority of the reported MGE within 0.5 and 2.6/1000, with an average of 0.798/1000.Reference Locoh-Donou, Guofen, Welcher, Berry, O’Connor and Brady1,Reference Arbon7,Reference Baird, O’Connor, Williamson, Sojka, Alibertis and Brady12 Even if the number of illnesses and trauma in MGE are reported higher than in the general population, they usually are of minor relevance and do not require hospitalization.Reference Arbon, Bottema and Zeitz3,Reference Milsten, Maguire, Bissell and Seaman4 Adequate planning of emergency medical care should consider different levels of resources, from Basic to Advanced Life Support teams. Emergency healthcare professionals can provide effective care on site and even if physicians are required in less than half of the patients, they can reduce the number of patients requiring hospitalization.Reference Lund, Turris and Bowles9,Reference Grange, Baumann and Vaezazizi15
LIMITATIONS
High level evidence studies on MGE are difficult to realize and this report only aims to describe our experience in managing this series of events while reporting standardized measures such as PPR and TTHR.Reference Ranse and Hutton8 The limitations mainly stem from our small sample size from a limited series of events, (only four football matches) where the number of patients assisted in medical emergencies or transported to the hospital was relatively low, even if in accordance with literature findings.
CONCLUSIONS
PPR and TTHR reported in this set of football events are within the range of previously published results. Climatic factors (such as heat and humidity), as well as absence of free water and increased alcohol consumption, appear to be related to an increased request for medical assistance. The different resources involved in medical assistance during UEFA Under -21 championship matches in Bologna, ranging from volunteer rescuers to emergency nurses and physicians, were efficiently allocated to shorten the time to access patients and provide effective care. A more comprehensive approach, not only limited to the number of participants and the historical experience developed during similar MGE, can be useful to establish an adequate level of risk assessment to plan the necessary number of healthcare professionals and volunteer rescuers. Operator training, preliminary briefing, perfect knowledge of the location particularly entrance and exit pathways within the stadium, and effective communication between the nurse coordinators and other rescue teams are key elements for good organization.
Author Contributions
All authors contributed to the study conception and design. FC and GG reviewed and authorized the project. Material preparation, data collection, and analysis were performed by AF, TB, and GI. The first draft of the manuscript was written by GI and AF, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors express sincere thanks to all personnel, technicians, nurses and emergency physicians of Centrale Operativa 118 Area Omogenea Emilia Est EMS, and all volunteer rescuers who participated in medical assistance during the UEFA 2019 Under- 21 championship. We would also like to thank UEFA staff for their excellent cooperation.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Ethics Approval
This retrospective study performed on a database of anonymized patients was approved by local Ethics Committee (CE AVEC number 256/2020/OSS/AUSLBO) on March 25, 2020.
Consent to Participate
Due to the retrospective design of this study, informed consent of participants was impossible to obtain for organizational purposes, due to the circumstances surrounding the MGE. A substitute declaration of informed consent has been submitted and approved by the Institutional Ethical Committee.
Availability of Data and Material
Data set is available on request.


 Open access
Open access