
Contents
COVID-19
SG-APSIC1026: COVID-19 vaccine acceptance and hesitancy among primary healthcare workers in Singapore
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s3
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
C. difficile
Utilizing vancomycin as secondary prophylaxis for the prevention of recurrent Clostridioides difficile infection
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s5
-
- Article
-
- You have access
- Open access
- Export citation
-
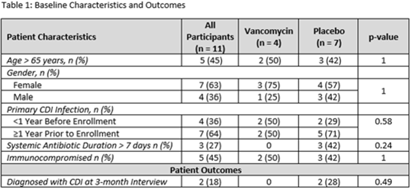
Background: Recurrent Clostridioides difficile infection (CDI) is associated with significant morbidity, mortality, and healthcare-related costs. Although data are minimal, agents including oral vancomycin have been used as secondary prophylaxis to prevent recurrent CDI. Methods: We conducted a randomized, double-blind, placebo-controlled trial to determine the effectiveness of vancomycin at preventing CDI from October 2019 to September 2022. Eligible patients had a history of at least 1 episode of CDI and were receiving systemic antibiotics for another condition. Participants were randomized 1:1 to oral vancomycin 125 mg by mouth twice daily and were interviewed at 1, 2, and 3 months thereafter to assess recurrence. We enrolled 26 patients: 15 completed the 1-month interview, 12 completed the 2-month interview, and 11 completed the full study. Those 15 participants who did not complete the 3-month interview were considered dropouts. The final sample for this study included those 11 participants who completed all interviews. Demographics and outcomes are shown in Table 1. Results: One case of recurrent CDI was reported at the 1-month interview and a second was reported at 3 months; both cases had received the placebo. The study was terminated early due to low enrollment. Conclusions: Although our results did not reach statistical significance and this study was limited in small sample size, our findings suggest that secondary prophylaxis with oral vancomycin may be beneficial in patients who are actively receiving antibiotics, which is consistent with prior retrospective studies. Future studies with larger sample sizes are still needed to examine this important question of whether secondary prophylaxis is useful for preventing recurrent CDI.
Disclosure: None

Original Article
Costs of two vancomycin-resistant enterococci outbreaks in an academic hospital
-
- Published online by Cambridge University Press:
- 13 January 2023, e8
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
COVID-19
SG-APSIC1113: Descriptive study on COVID-19 exposures in Singapore General Hospital
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s3
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
CLABSI
Relative risk of primary bloodstream infection in patients with mechanical circulatory support devices
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s6
-
- Article
-
- You have access
- Open access
- Export citation
-
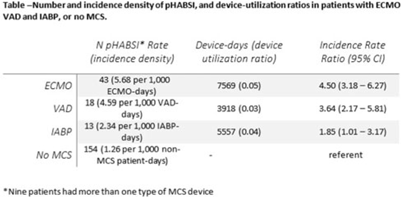
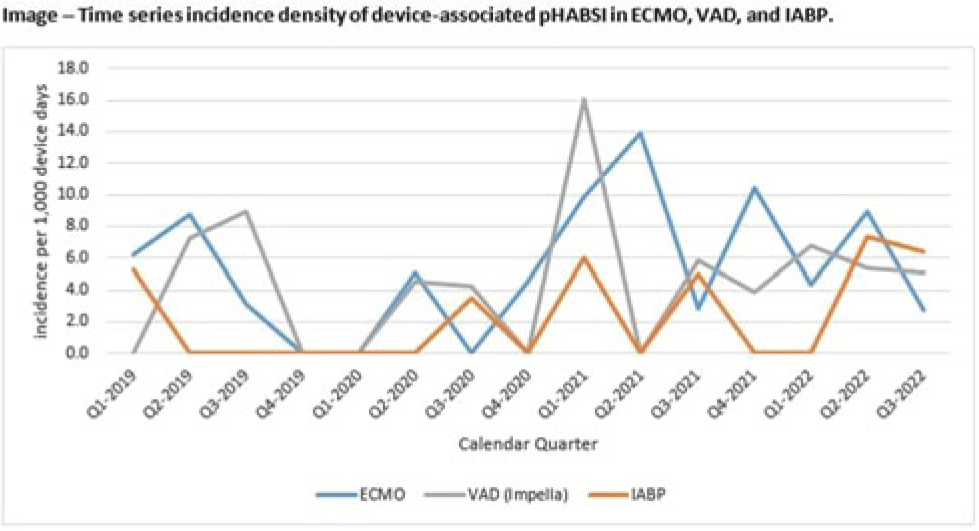
Background: Patients requiring mechanical circulatory support (MCS) during episodes of cardiogenic shock are at risk for hospital-acquired bloodstream infection (HABSI). Clinically MCS devices include extracorporeal membrane oxygenation (ECMO) devices, durable and temporary left ventricular-assist devices (VADs), and intra-aortic balloon pumps (IABPs). However, the MCS exclusion to the NHSN central-line–associated bloodstream infection (CLABSI) surveillance rules in 2018 did not include IABP as a qualifying device. We have described utilization and incidence of primary HABSI (pHABSI) in our patients requiring MCS. Methods: The setting for this study was 9 cardiothoracic and heart failure intensive care units with 131 total beds at the Cleveland Clinic Main Campus. Surveillance for HABSI to include determination of CLABSI was performed prospectively. MCS-associated pHABSI were patients who had ECMO, LVAD, or IABP present for >2 calendar days with device in place on the date of infection or removed the day before. A patient with 2 device types at time of infection was counted as a pHABSI for both groups. Patient, device, and MCS days were extracted from an electronic database. Non-MCS patient days were calculated as the difference between total patient days and total MCS days. The incidence of ECMO-, VAD-, and IABP-associated pHABSI were compared to each other and to non–MCS-associated pHABSI using OpenEpi version 3.01 software. Results: Surveillance results are shown in Table 1. During the observation period, there were 221 pHABSIs and 139,013 patient days. Moreover, 67 pHABSIs were associated with an MCS device over 17,044 total MCS days: 43 ECMO days, 18 VAD days, and 13 IABP days. Also, 9 patients had >1 type of eligible device and 7 (39%) of the IABP-associated pHABSIs were CLABSIs.
The cumulative incidences of pHABSI associated with ECMO, VAD, and IABP were 5.68, 4.59, and 2.34 per 1,000 MCS days, respectively. The incidence of IABP pHABSI was not significantly different from VAD pHABSI (P = .06), but it was different from ECMO pHABSI (P < .01). The pHABSI rate for non-MCS days was 1.26 per 1,000 patient days. Conclusions: In our patients requiring MCS, the risk of pHABSI associated with IABP was significantly greater than in patients without MCS and was similar to patients with VAD. MCS of all types should be considered a risk for HABSI in patients with cardiogenic shock beyond the presence of a central line. Protocols to further prevent HABSI morbidity in IABP patients are needed.
Disclosure: None


Original Article
Measuring clinical outcomes of highly multiplex molecular diagnostics for respiratory infections: A systematic review and conceptual framework
-
- Published online by Cambridge University Press:
- 09 January 2023, e9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
COVID-19
SG-APSIC1158: COVID-19 vaccine booster hesitancy among healthcare workers: A retrospective observational study in Singapore
-
- Published online by Cambridge University Press:
- 16 March 2023, pp. s3-s4
-
- Article
-
- You have access
- Open access
- Export citation
Commentary
Antimicrobial Stewardship and Healthcare Epidemiology year in review, 2022: Celebrating successes while focusing on the future
-
- Published online by Cambridge University Press:
- 11 January 2023, e10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Poster Presentation - Top Poster Award
COVID-19
Healthcare personnel at non–acute-care facilities are at risk of COVID-19 from workplace and community exposures
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s6
-
- Article
-
- You have access
- Open access
- Export citation
COVID-19
SG-APSIC1054: Sputnik-V postvaccination immunologic responses in nasal mucosa: A prospective cohort study in Kazakhstan
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s4
-
- Article
-
- You have access
- Open access
- Export citation
Original Article
Increasing cefazolin use for surgical prophylaxis in penicillin-allergy–labeled patients
-
- Published online by Cambridge University Press:
- 11 January 2023, e11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
COVID-19
SG-APSIC1119: N95 mask concordance amongst female Muslim healthcare workers undergoing mask fitting with and without tudung
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s4
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
COVID-19
Low infectivity among asymptomatic patients with a positive SARS-CoV-2 admission test at a tertiary-care center, 2020–2022
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s7
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Many hospitals have implemented admission SARS-CoV-2 testing to evaluate for the need for transmission-based precautions. However, a positive test in an asymptomatic patient may represent (1) active infection, signifying infectiousness; (2) false positivity; or (3) past infection with prolonged viral shedding. We used a strand-specific SARS-CoV-2 reverse real-time polymerase chain reaction (rRT-PCR) assay to assess infectivity among asymptomatic patients with a positive SARS-CoV-2 PCR admission test. Methods: We used a 2-step rRT-PCR specific to the minus strand of the SARS-CoV-2 envelope gene. We reviewed records of patients with a positive SARS-CoV-2 PCR who were also tested for the strand-specific SARS-CoV-2 PCR within 2 days of admission at Stanford Health Care during July 2020–April 2022. We restricted our analysis to each patient’s first test. We calculated the percentage of detectable minus strand-specific tests among asymptomatic patients over time and gathered descriptive statistics for age, sex, and immunocompromised state. Results: In total, 848 admitted patients had strand-specific SARS-CoV-2 assays performed. Of 532 patients with a strand-specific assay done within 2 days of admission, 242 (45%) were asymptomatic. Among asymptomatic patients, the mean age was 56 years (range, 19–99), 133 (55%) were male, 50 (21%) had immunocompromising conditions, and 30 (12%) were admitted for a surgical procedure. In total, 21 (9%; range, 4%–25% per quarter) had detectable minus strand-specific assays (Fig. 1). Conclusions: Most asymptomatic patients tested for SARS-CoV-2 on admission were not infectious. Hospitals using SARS-CoV-2 PCR admission testing may need to re-evaluate the continued use of this practice.
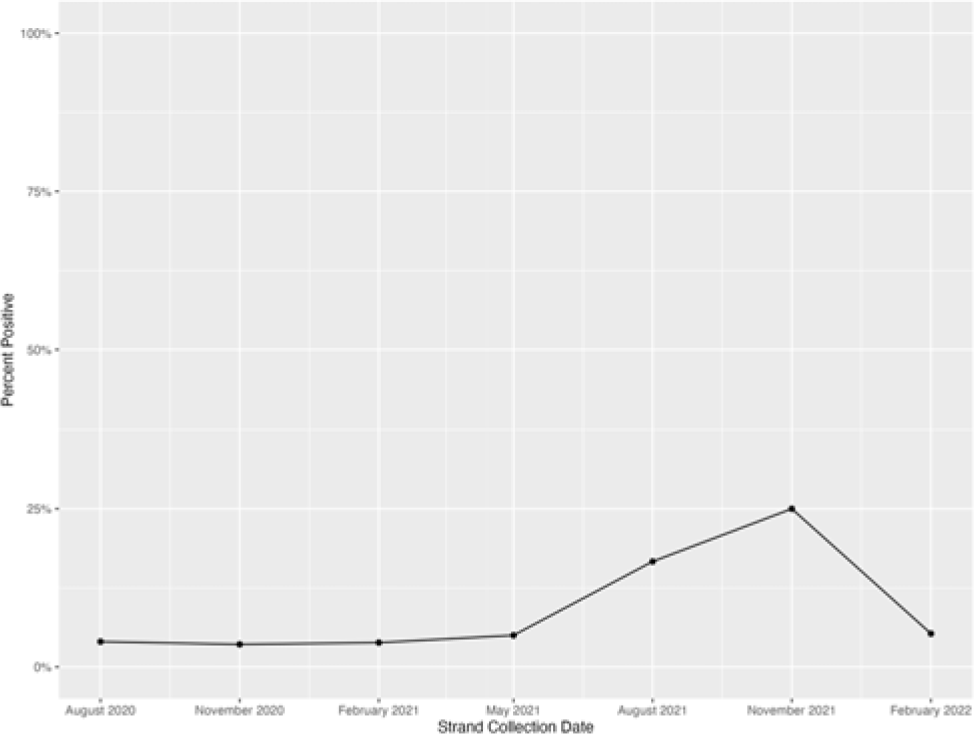
Fig. 1. Minus strand-specific SARS-CoV-2 assay percentage positivity per quarter among asymptomatic patients tested within 2 days of admission. The peak positivity in November 2021–January 2022 quarter coincided with the SARS-CoV-2 omicron variant surge in our county.
Disclosure: None

Concise Communication
Trends in pediatric community-onset Staphylococcus aureus antibiotic susceptibilities over a five-year period in a multihospital health system
-
- Published online by Cambridge University Press:
- 17 January 2023, e12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
COVID-19
SG-APSIC1049: Immunogenicity of Gam-COVID-Vac and Sinopharm BBIBP-CorV vaccines in seropositive and seronegative adults
-
- Published online by Cambridge University Press:
- 16 March 2023, pp. s4-s5
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
COVID-19
Hospital-onset COVID-19: Associations with population- and hospital-level measures to guide infection prevention efforts
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s7
-
- Article
-
- You have access
- Open access
- Export citation
-
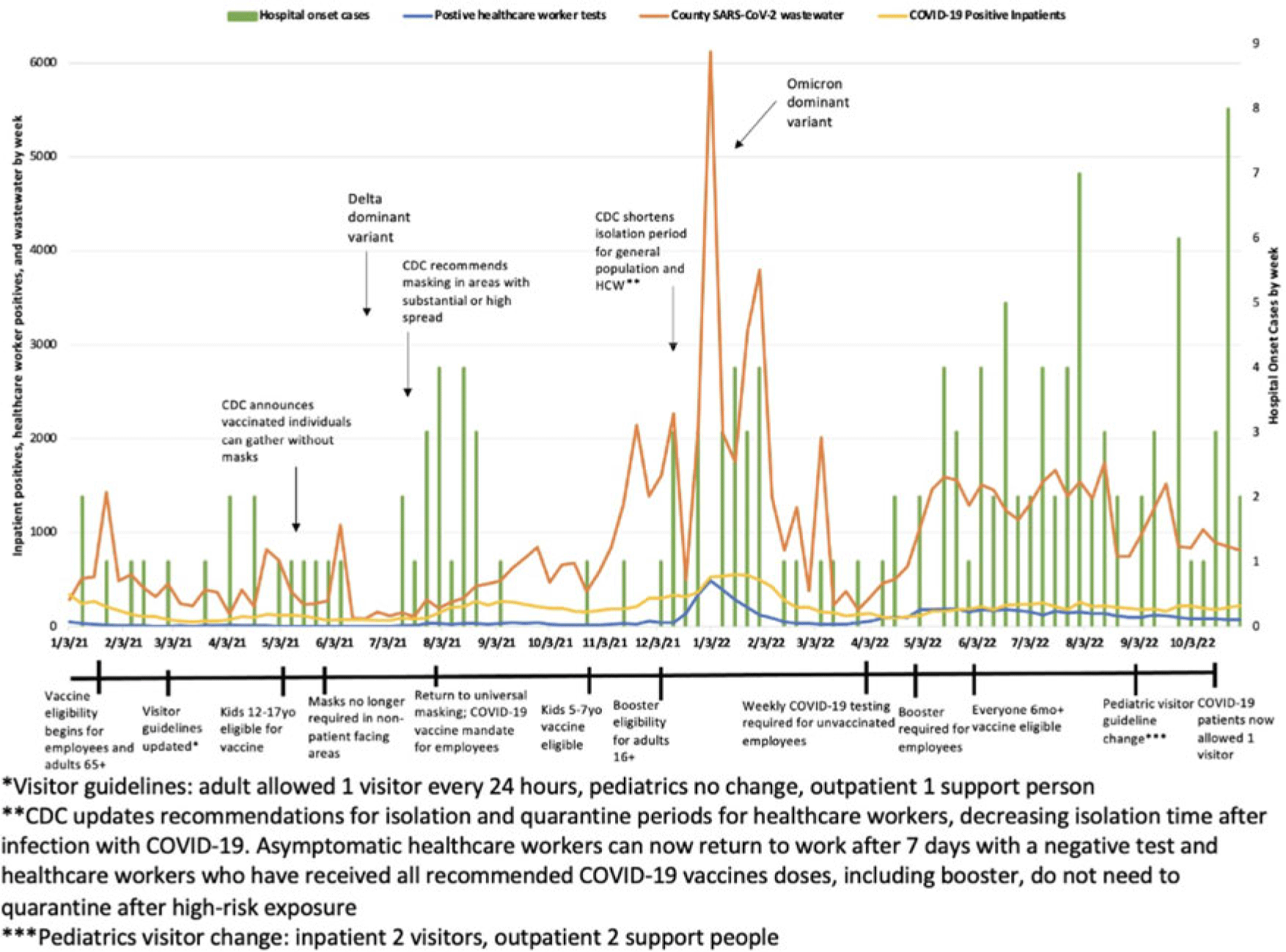
Objective: To characterize hospital-onset COVID-19 cases and to investigate the associations between these rates and population and hospital-level rates including trends in healthcare worker infections (HCW), community cases, and COVID-19 wastewater data. Design: Retrospective cohort study from January 1, 2021, to November 23, 2022. Setting: This study was conducted at a 589-bed urban Midwestern tertiary-care hospital system. Participants and interventions: The infection prevention team reviewed the electronic medical records (EMR) of patients who were admitted for >48 hours and subsequently tested positive for SARS-CoV-2 to determine whether COVID-19 was likely to be hospital-onset illness. Each case was further categorized as definite, probable, or possible based on viral sequencing, caregiver tracing analysis, symptoms, and cycle threshold values. Patients were excluded if there was a known exposure prior to admission. Clinical data including vaccination status were collected from the EMR. HCW case data were collected via our institution’s employee health services. Community cases and wastewater data were collected via the Wisconsin Department of Health Services database. Additionally, we evaluated the timing of changes in infection prevention guidance such as visitor restrictions. Results: In total, 156 patients met criteria for hospital-onset COVID-19. Overall, 6% of cases were categorized as definite, 24% were probable, and 70% were possible hospital-onset illness. Most patients were tested prior to a procedure (31%), for new symptoms (30%), and for discharge planning (30%). Also, 53% were symptomatic and 41% received treatment for their COVID-19. Overall, 38% of patients were immunocompromised and 27% were unvaccinated. Overall, 12% of patients died within 1 month of their positive SARS-CoV-2 test, and 11% required ICU admission during their hospital stay. Hospital-onset COVID-19 increased in fall of 2022. Specifically, October 2022 had 16 cases, whereas fall of 2021 (September–November) only had 3 cases total. Finally, similar peaks were observed in total cases by week between healthcare workers, county cases, and COVID-19 wastewater levels. These peaks correspond with the SARS-CoV-2 delta and omicron variant surges, respectively. Conclusions: Hospital-onset cases followed similar trends as population and hospital-level data throughout the study period. However, hospital-onset rate did not correlate as strongly in the second half of 2022 when cases were disproportionately high. Given that hospital-onset cases can result in significant morbidity, continued enhanced infection prevention efforts and low threshold for testing are warranted in the inpatient environment.
Disclosure: None

COVID-19
SG-APSIC1176: Laboratory-acquired COVID-19 during the SARS-CoV-2 ο (omicron) pandemic wave at a tertiary-care hospital in Korea
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s5
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
Decolonization Strategies
Effectiveness of a Staphylococcus aureus mupirocin decolonization protocol in a neonatal intensive care unit
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s8
-
- Article
-
- You have access
- Open access
- Export citation
-
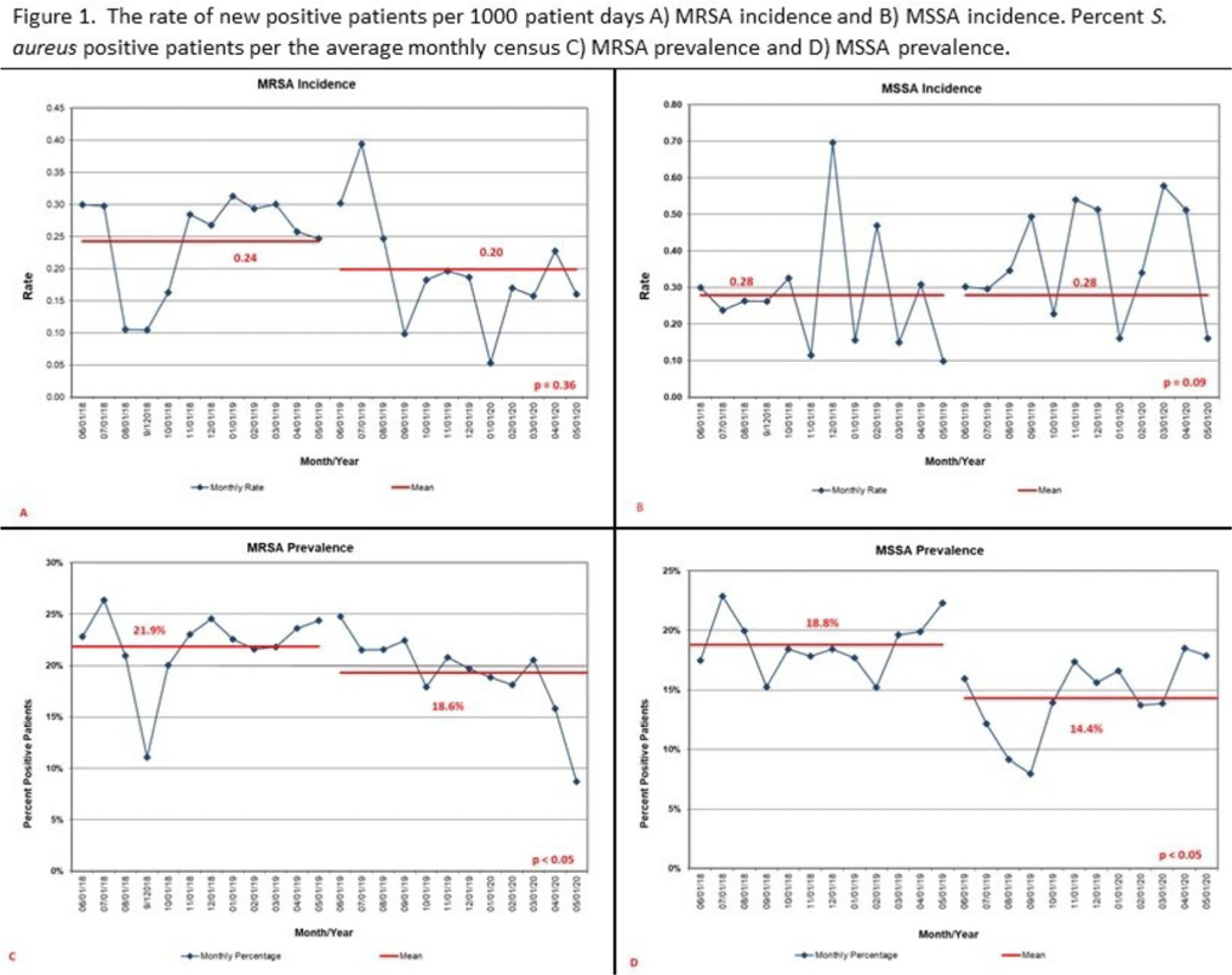
Background: Staphylococcus aureus infections are a significant cause of morbidity in neonatal intensive care units (NICUs), and they are typically preceded by nasal colonization. Mupirocin decolonization protocols as an infection prevention tool can halt S. aureus outbreaks and prevent infections. We examined the effect of a mupirocin treatment protocol on S. aureus incidence, prevalence, decolonization, and infections in a level IV NICU. Methods: We conducted a retrospective before-and-after observational study from June 1, 2018, to May 31, 2020. Beginning June 1, 2019, patients identified with either methicillin-sensitive or -resistant S. aureus (MSSA or MRSA) received mupirocin ointment to bilateral nares 3 times daily for 5 days. Patients with central lines or surgical incisions were treated every 30 days. All NICU patients were screened weekly unless positive for MRSA. We defined MSSA decolonization as 3 consecutive negative screens following mupirocin treatment. We calculated monthly S. aureus incidence as any new positive per 1,000 patient days and monthly prevalence as a percentage of the average daily number of patients with S. aureus per the average monthly census. Total number of infections were compared. Statistical significance was determined using a 2 sample proportions test and P < .05. Decolonization was calculated as percentage of occurrences among treated patients. Results: Overall, 190 patients received mupirocin; 142 patients received 1 course and 48 received 2 or more courses. There was no difference in incidence of MSSA (P = .09), but prevalence decreased from 18.8% to 14.4% (P < .05) (Fig. 1). Of 66 patients with MSSA, 35% were decolonized. An additional mupirocin treatment for 16 of these patients had a 50% decolonization rate. For MRSA, incidence decreased from 0.24 to 0.20 (P = .36) and prevalence decreased from 21.9% to 18.6% (P < .05) (Fig. 1). There was no statistical difference in the number of total S. aureus infections (P = .91) or when stratified by MSSA (P = .72) or MRSA (P = .82). In the postmupirocin population, there were 5 MRSA and 7 MSSA infections. Of the MSSA-infected patients, 6 remained colonized at the time of infection. Conclusions: Implementing a single mupirocin treatment course for S. aureus decolonization in NICU was only effective in one-third of patients and had no effect on infection occurrence. Changes in incidence and prevalence could be confounded by other infection prevention practices. Further study is needed to determine whether continued screening and additional mupirocin treatment could improve effectiveness of S. aureus decolonization programs.
Disclosure: None

Original Article
Developing a quality measure to assess use of antibiotic medications for respiratory conditions
-
- Published online by Cambridge University Press:
- 17 January 2023, e13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Poster Presentation - Top Poster Award
Diagnostic/Microbiology
Implementation of diagnostic stewardship in two surgical ICUs: Time for a blood-culture change
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s9-s10
-
- Article
-
- You have access
- Open access
- Export citation
-
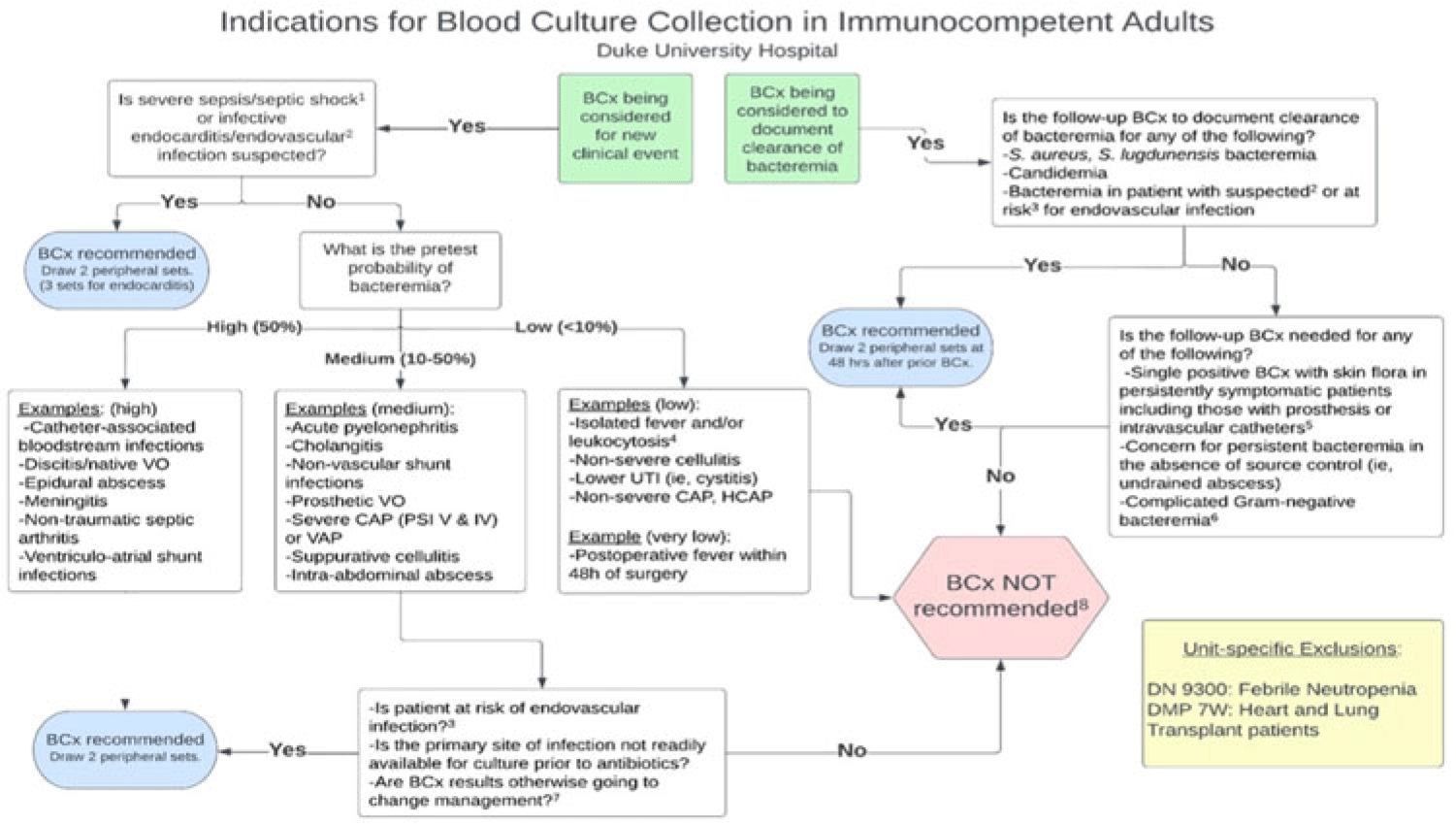
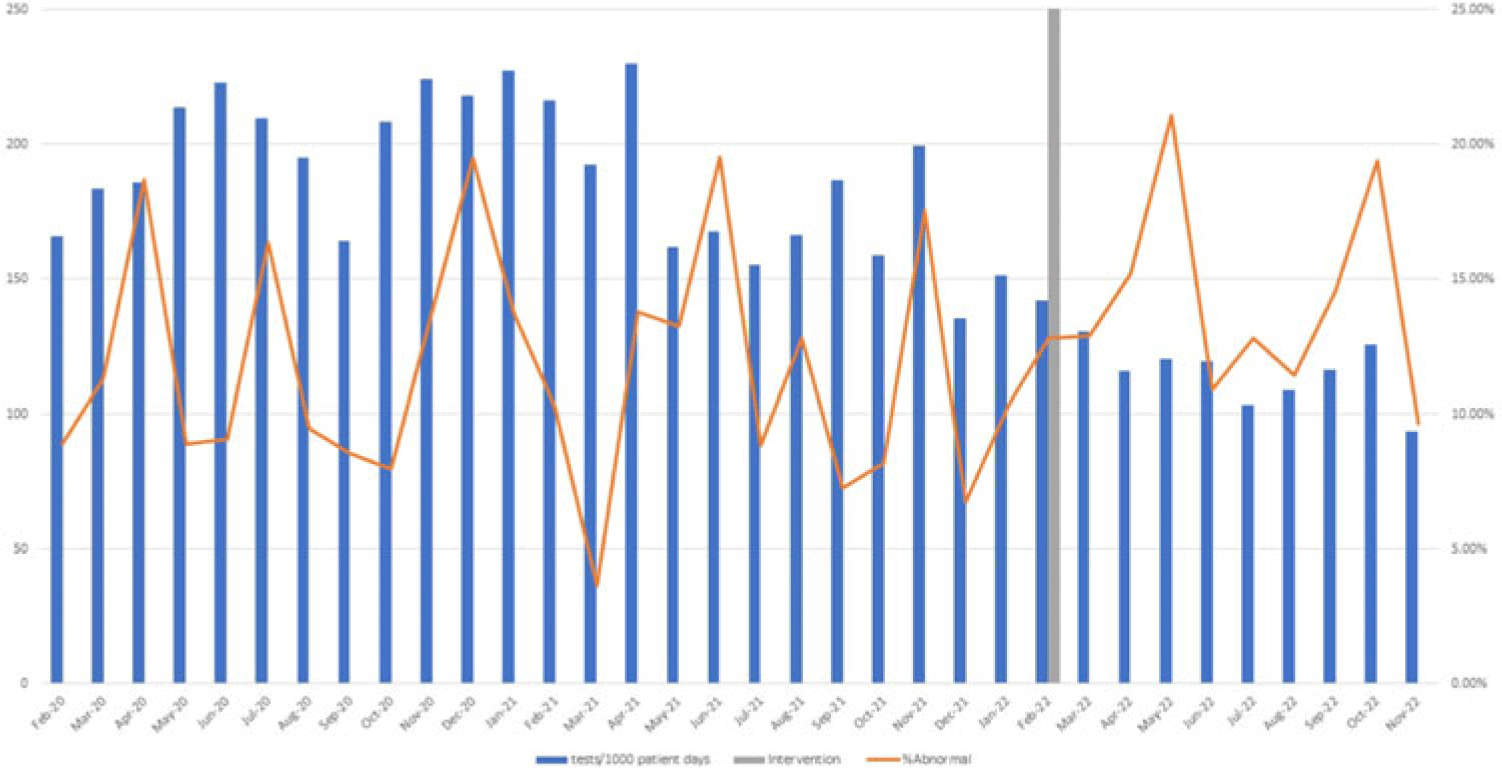
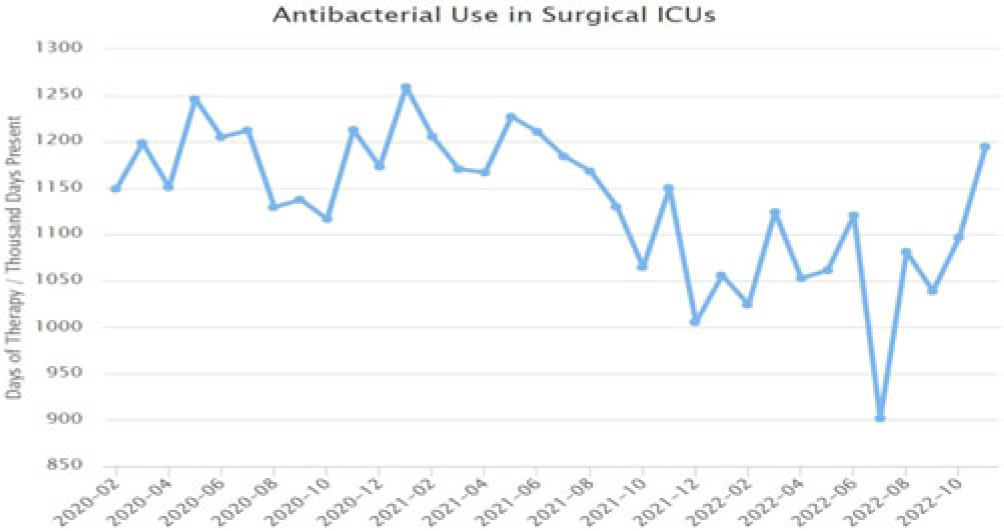
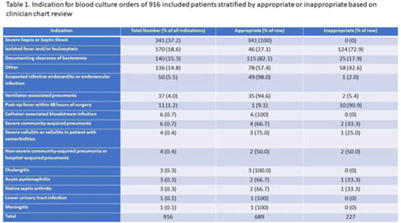
Background: Blood cultures are commonly ordered for patients with low risk of bacteremia. Liberal blood-culture ordering increases the risk of false-positive results, which can lead to increased length of stay, excess antibiotics, and unnecessary diagnostic procedures. We implemented a blood-culture indication algorithm with data feedback and assessed the impact on ordering volume and percent positivity. Methods: We performed a prospective cohort study from February 2022 to November 2022 using historical controls from February 2020 to January 2022. We introduced the blood-culture algorithm (Fig. 1) in 2 adult surgical intensive care units (ICUs). Clinicians reviewed charts of eligible patients with blood cultures weekly to determine whether the blood-culture algorithm was followed. They provided feedback to the unit medical directors weekly. We defined a blood-culture event as ≥1 blood culture within 24 hours. We excluded patients aged <18 years, absolute neutrophil count <500, and heart and lung transplant recipients at the time of blood-culture review. Results: In total, 7,315 blood-culture events in the preintervention group and 2,506 blood-culture events in the postintervention group met eligibility criteria. The average monthly blood-culture rate decreased from 190 blood cultures per 1,000 patient days to 142 blood cultures per 1,000 patient days (P < .01) after the algorithm was implemented. (Fig. 2) The average monthly blood-culture positivity increased from 11.7% to 14.2% (P = .13). Average monthly days of antibiotic therapy (DOT) was lower in the postintervention period than in the preintervention period (2,200 vs 1,940; P < .01). (Fig. 3) The ICU length of stay did not change before the intervention compared to after the intervention: 10 days (IQR, 5–18) versus 10 days (IQR, 5–17; P = .63). The in-hospital mortality rate was lower during the postintervention period, but the difference was not statistically significant: 9.24% versus 8.34% (P = .17). The all-cause 30-day mortality was significantly lower during the intervention period: 11.9% versus 9.7% (P < .01). The unplanned 30-day readmission percentage was significantly lower during the intervention period (10.6% vs 7.6%; P < .01). Over the 9-month intervention, we reviewed 916 blood-culture events in 452 unique patients. Overall, 74.6% of blood cultures followed the algorithm. The most common reasons overall for ordering blood cultures were severe sepsis or septic shock (37%), isolated fever and/or leukocytosis (19%), and documenting clearance of bacteremia (15%) (Table 1). The most common indications for inappropriate blood cultures were isolated fever and/or leukocytosis (53%). Conclusions: We introduced a blood-culture algorithm with data feedback in 2 surgical ICUs and observed decreases in blood-culture volume without a negative impact on ICU LOS or mortality rate.
Disclosure: None



