This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
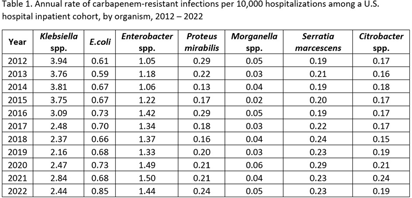
Background: Carbapenem-resistant Enterobacterales (CRE) infections are an urgent public health threat. An estimated 12,700 CRE (including E. coli, Klebsiella spp., and Enterobacter spp.) infections occurred in the United States in 2020. While the estimated incidence of CRE infections has been relatively stable between 2012 and 2020, organism-specific trends, including those for organisms not typically included in CRE surveillance definitions, have not been described. We estimated the annual rate of carbapenem-resistant Enterobacterales infections, disaggregated by organism, from 2012 to 2022. Methods: Data on inpatient hospitalizations from a dynamic cohort of short-term acute care hospitals reporting microbiology data between 2012 and 2022 were obtained from the PINC AI Database and the BD Insights Research Database. We included patients with clinical isolates of E. coli, Enterobacter spp., Klebsiella spp., Citrobacter spp., Serratia marcescens, Proteus mirabilis, and Morganella spp. and sufficient susceptibility results to identify carbapenem resistance. We limited our analysis to incident isolates, defined as a patient’s first isolate of a given organism and carbapenem resistance phenotype in a 14-day period. We calculated the annual rate of carbapenem-resistant infections per 10,000 hospitalizations for each organism. Results: There were 3,018,792 incident isolates from 55.8 million hospitalizations included in the analysis. Overall, 31,226 incident carbapenem-resistant isolates were identified. The rate of carbapenem-resistant infections varied by organism and over time (Table 1). The rate of carbapenem-resistant Klebsiella spp. infections appeared to decline from 3.94 in 2012 to 2.44 infections per 10,000 hospitalizations in 2022. The rate of carbapenem-resistant Enterobacter spp. infections appeared to increase from 1.05 in 2012 to 1.44 infections per 10,000 hospitalizations in 2022. The rate of carbapenem-resistant E. coli infections also appeared to increase, from 0.61 in 2012 to 0.85 infections per 10,000 hospitalizations in 2022. Rates of carbapenem-resistant Proteus mirabilis, Morganella spp., Citrobacter spp., or Serratia marcescens infections were similar in 2022 compared to 2012. Conclusions: Disaggregating data by organism revealed heterogeneous trends, with apparent increases in rates of carbapenem-resistant Enterobacter spp. and E. coli infections and apparent decreases in rates of carbapenem-resistant Klebsiella spp. infections. Organism-specific CRE analyses may provide additional insight into CRE epidemiology.
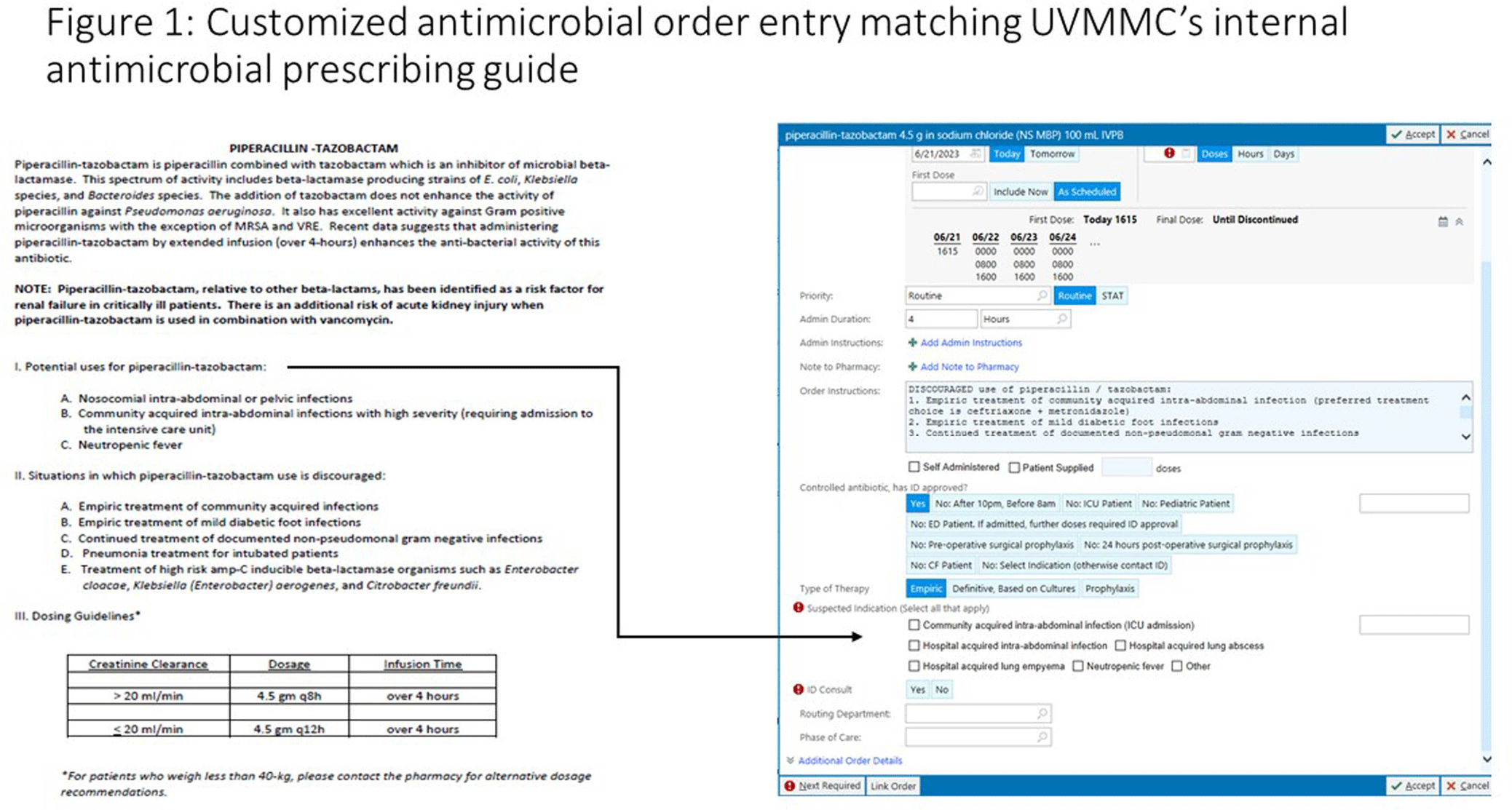
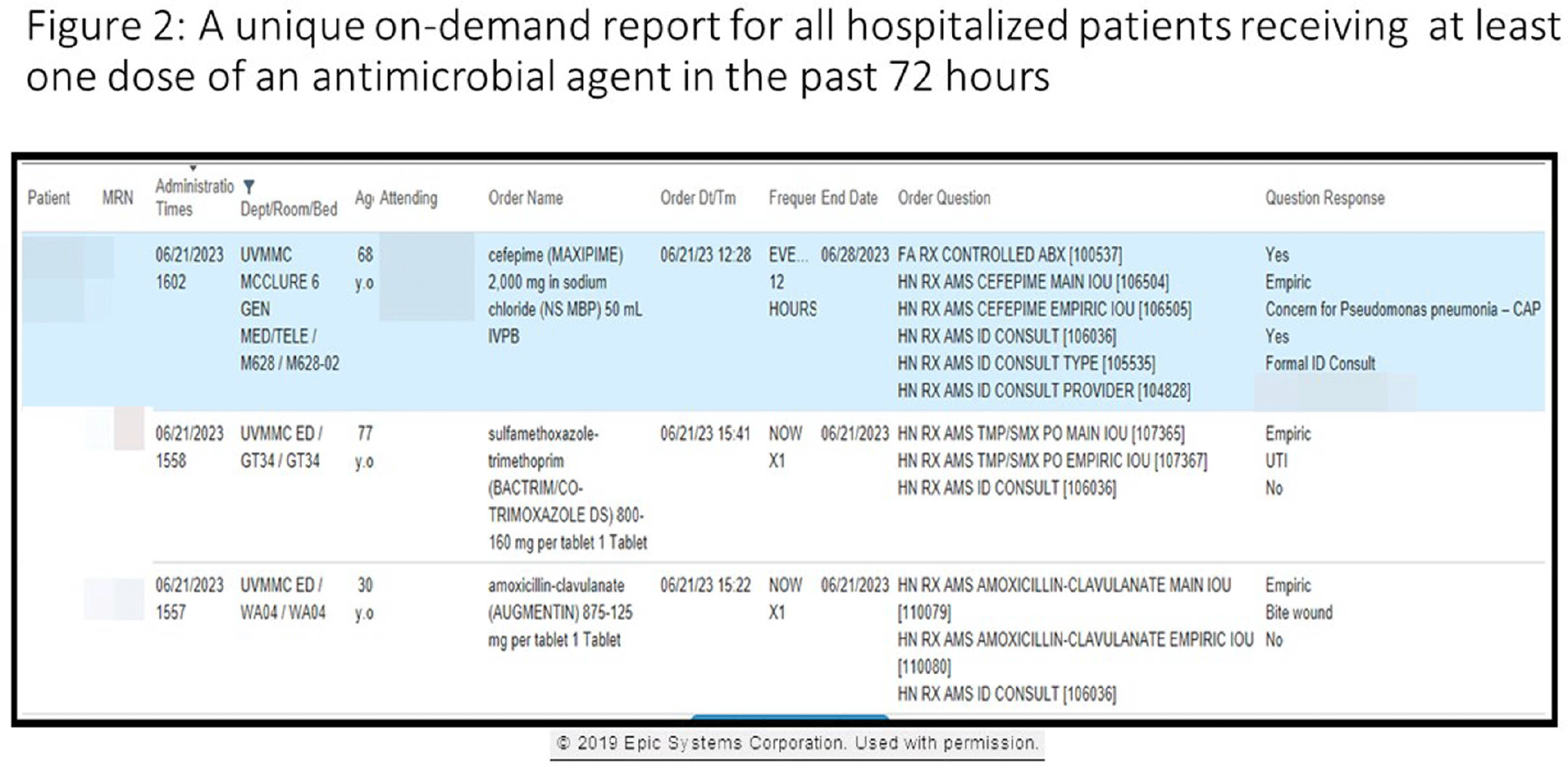
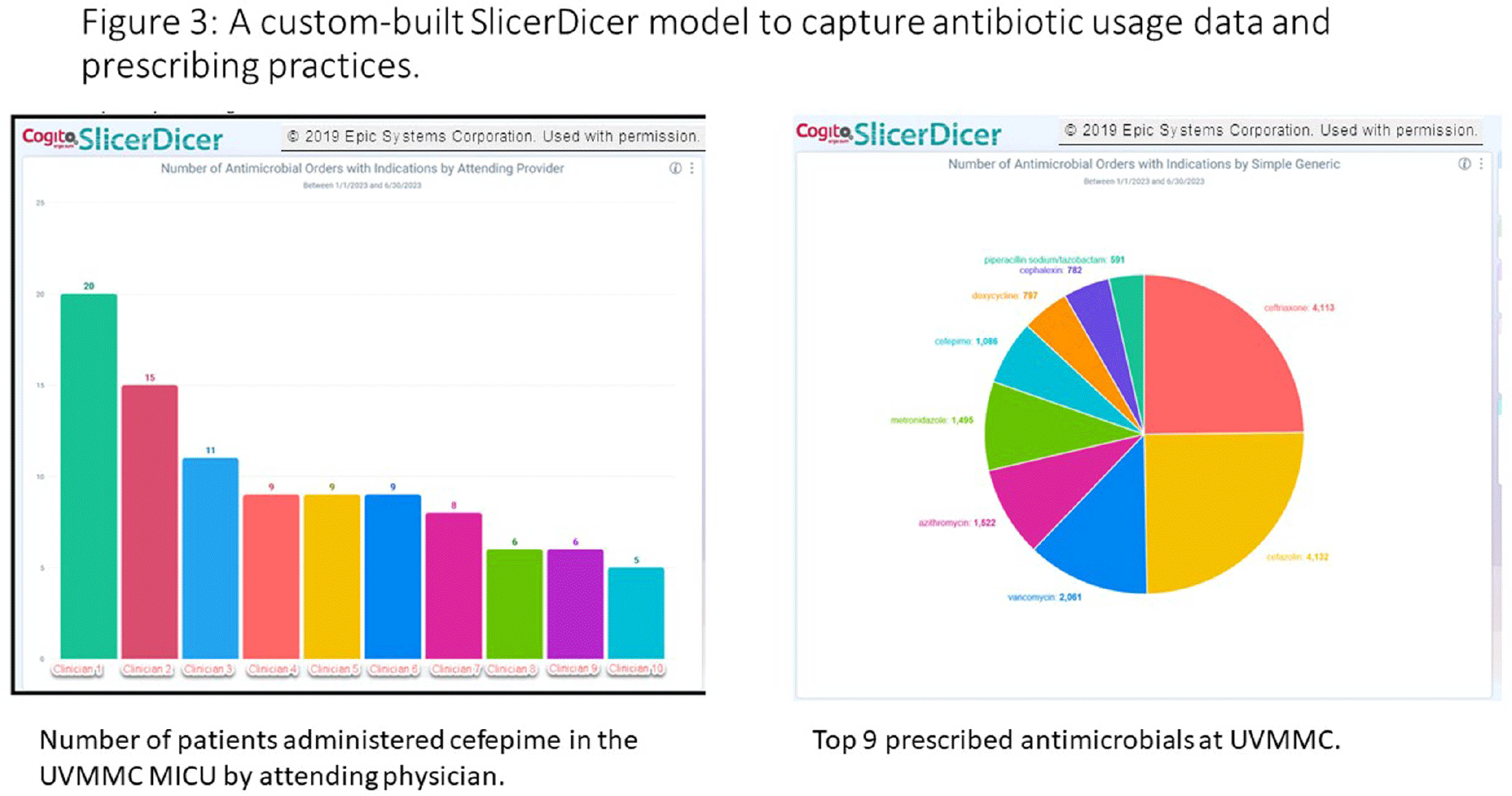
Background: Antimicrobial stewardship programs rely heavily on the electronic medical record (EMR) to carry out daily activities, make interventions, optimize patient care, and collect data. In 2019 the University of Vermont Medical Center transitioned from using a third party platform to the Epic (Verona, WI, www.epic.com) Bugsy module for antimicrobial stewardship. Method: We have spent the past 4 years optimizing the Epic foundation to match our institutional antimicrobial prescribing guidelines, susceptibility patterns, and build reports to extract actionable data. Result: During the build process, we readily identified three areas needed for customization: (1) Empiric, definitive, and prophylactic indications of use for all antimicrobials based on our hospital’s internally published books “Guide to Antimicrobial Therapy for Adults” and “Guide to Antimicrobial Therapy for Pediatrics” (figure 1); (2) An on-demand report to capture all patients with new administrations of antimicrobials in the preceding 72 hours, that includes ordering clinician, stop date of therapy, and indication (figure 2); and (3) A unique, custom-built slicer-dicer report to capture high-level data on how each antimicrobial is being prescribed by indication, dose, route of administration, ordering clinician, attending physician, and department (figure 3). Conclusion: We have built a system where we can readily identify patients that are receiving antimicrobials both within and outside of institutional guidelines and know the ordering clinician to contact to provide in-the-moment feedback. We can also collect retrospective data to know which antimicrobial agents were prescribed for all infectious syndromes. These three institutional customizations have provided invaluable information to improve patient care.
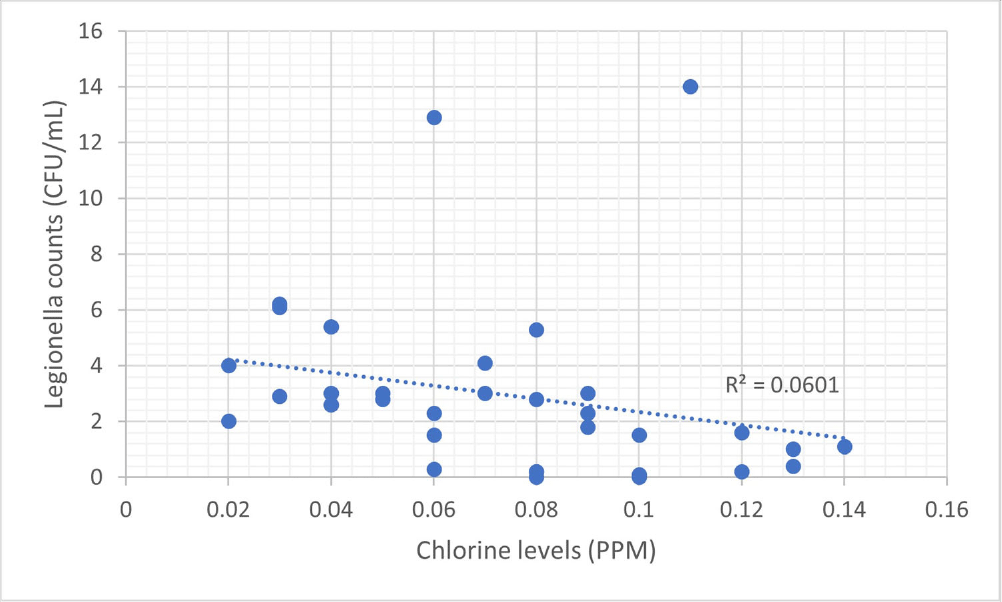
Background: Legionella, first identified in the 1970s, is increasingly recognized as an opportunistic pathogen in healthcare facilities.1 The National University Hospital (NUH) is a large quaternary level academic hospital with 1,200 beds located in equatorial Singapore. Its first building, completed in 1985, still serves patients today. In 2022, the infection prevention team (IPT) was informed of two cases of nosocomial legionella, which sparked the start of an extensive investigation consisting of water quality testing of multiple sources, case finding, and formation of a water management committee. Methods: 250mL water samples were collected and cultured by an external vendor using direct membrane filtration followed by plating on selective agar according to ISO 11731 standards. Bacterial colonies were then identified, quantified and speciated. At the same time, NUH’s facility management measured chlorine levels using a portable colorimeter. Results: In total, we cultured 34 samples taken from sinks, shower heads, potable water dispensers. 91.2% of samples were positive for legionella. Of the 91.2%, 35.3% of sites grew Legionella pneumophila serogroup 1 while 79.4% of sites grew Legionella pneumophila serogroup 2-15. We attributed our high rates of legionella positivity to an aging plumbing system and Singapore’s high humidity and temperatures. In addition, the maximal temperature of our hot water is only 48-50 °C. Although chlorine levels were generally low, they were still within the local recommendation of less than 2ppm (Singapore does not have guidance on minimum chlorine levels). We found no statistically significant correlation between the number of legionella colony forming units (CFUs) and chlorine levels (ranging between 0.02 to 0.14ppm). This supports the United States Environmental Protection Agency’s recommendation, as well as the findings from in vitro and in vivo studies, for a minimal chlorine of 0.2 PPM at the taps for acute care hospitals.2,3However, these levels may be inadequate in the presence of acanthamoeba or a high biofilm load within water systems.4,5 Conclusion: Hospital water management programs should require a minimal level of chlorine at hospital taps and at levels above those recommended by public water systems, in order to control legionella growth. In addition, the formation of a hospital water management committee is essential to improve hospital water quality and put mitigation measures in place. References 1. Phin, N. et al. Epidemiology and clinical management of Legionnaires’ disease. Lancet Infect. Dis. 14, 1011–1021 (2014). 2. Marchesi, I. et al. Monochloramine and chlorine dioxide for controlling Legionella pneumophila contamination: biocide levels and disinfection by-product formation in hospital water networks. J. Water Health11, 738–747 (2013). 3. Cervero-Aragó, S., Rodríguez-Martínez, S., Puertas-Bennasar, A. & Araujo, R. M. Effect of Common Drinking Water Disinfectants, Chlorine and Heat, on Free Legionella and AmoebaeAssociated Legionella. PloS One 10, e0134726 (2015). 4. Kessler, M. A., Osman, F., Marx, J., Pop-Vicas, A. & Safdar, N. Hospital-acquired Legionella pneumonia outbreak at an academic medical center: Lessons learned. Am. J. Infect. Control 49, 1014–1020 (2021).