

In the year 1931, I was married to Nassif D., a shoe maker from Jaffa, and had from him six children, four girls and two boys. During 1944–1945, my husband became ill and then lost his mind; Your Excellency may allow me to state that apart from our being in a complete state of distress, my husband beats me and the children practically every night and has on many occasions tried to burn the hut in which we live. I have in vain approached the Public Health Department and the Police Authorities in Jaffa to send him to a Lunatic Asylum but they have failed to do so. I therefore have been advised to refer the matter to Your Excellency and respectfully trust that Your Excellency will order the department concerned to act as soon as possible before it is too late, as I am sure that one of these days, my children and myself will be the victims of a lunatic man.Footnote 1
In December 1945, Zmurud D. wrote in desperation to the High Commissioner of Palestine, the highest-ranking official in the British mandate government that had, by then, governed Palestine for over two decades. Experiencing violence at the hands of a husband who had ‘lost his mind’, she had already sought help from the department of health as well as the police in Jaffa, but to no avail; petitioning the High Commissioner directly was her last resort. Zmurud’s gambit yielded results, though not in a form she had anticipated. Rather than admit her husband, the department of health arranged for him to be offered a course of electro-convulsive therapy at the government mental hospital near Jaffa as an outpatient. While this meant the overcrowded hospital could treat him without filling one of their precious beds, these ‘inoculations’ – as Zmurud erroneously called them a few months later – made her husband ‘very furious’. Every time he returned home from the hospital, he beat her and the children, and poured kerosene over their mattresses in his attempts to burn down the house. Faced with this unbearable situation, Zmurud wrote once again to the High Commissioner to demand that her husband be sent to a mental institution before it was too late.Footnote 2 This time, she was assured that her husband would be admitted when a vacancy became availableFootnote 3 – though there is no record in the colonial archive of when, if at all, this may have come to pass.

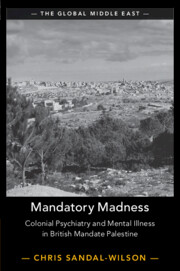
Map 0.1 Map of government and major private mental institutions in mandate Palestine
The story of Zmurud’s encounter with mental illness is just one of the many I have come across in the archive of the British colonial government that ruled Palestine from the end of the First World War until 1948, though that does not diminish the poignancy of her calls for help under harrowing circumstances. These stories unfolded against the backdrop of a pivotal period in the history of modern Palestine. Across three short decades, former Ottoman territories in the Levant were partitioned and parcelled out as British and French mandates under the auspices of the newly created League of Nations; a British administration formally committed to the creation of a Jewish national home in Palestine was imposed against the expressed wishes of the indigenous Arab population; and a Palestinian national movement emerged which, by the late 1930s, was capable of sustaining an unprecedented general strike and years-long revolt against both the British and Zionism. Stories like Zmurud’s are easy to overlook, against the backdrop of these momentous developments and in the knowledge that the mandate period would come to a sudden and dramatic end in 1948 with the establishment of the State of Israel and the Palestinian nakba, or catastrophe, of displacement and dispossession.
Yet these stories – of how people living in mandate Palestine negotiated both mental illness and the colonial state at the same time – are at the heart of this book. They matter in their own right and on their own terms: Zmurud’s petitions, which speak powerfully to the way her and her family’s life had been turned upside down by mental illness, make this plain. These stories also, however, hold out challenges to and possibilities for the study of mandate Palestine, the history of psychiatry, and our understanding of how Palestine connects up to wider regional, imperial, and global histories. By centring the social and cultural history of mental illness in mandate Palestine, Mandatory Madness makes an intervention in each of these three areas. First, it provides a distinctive new account of how mandate officials, European Jews, and Palestinians – Muslim, Christian, and Jewish – interrelated. Stories like Zmurud’s can reveal the intimate ways in which the big political transformations of the period were felt by ordinary Palestinians. But more than this, focussing on these stories brings into view a rich seam of encounters, negotiations, and contestations stretching across colonial state and society, at a register overlooked by the political histories that dominate the scholarship. Second, the book makes the case for shifting the centre of gravity within histories of psychiatry – particularly colonial psychiatry – away from institutions or experts and towards a fuller apprehension of the myriad spaces, actors, and issues which mental illness entangled. Tracing the varied encounters which mental illness engendered requires a rethinking of the archive of the history of psychiatry, too. Third, by locating Palestine firmly in relation to wider regional, imperial, and global contexts, Mandatory Madness challenges the methodological nationalism, the stubbornly national framing of analysis, which still characterises much scholarship on both Palestine and colonial psychiatry. But it also uses the history of psychiatry in Palestine, including its specificities and incommensurabilities, to engage critically in debates around mobility, translation, and globalisation across these distinct fields and to underscore that blockages, and not just connections, structured Palestine’s relationships with wider worlds.
Zmurud’s story gives a sense of what is gained by embracing this more expansive approach to the history of mandate Palestine and psychiatry. Her petitions open up our understanding of where the history of psychiatry unfolds and who its principal characters are, and offer a powerful example of the sustained, consequential negotiations Palestinians undertook with the colonial state around mental illness; her story also provides an oblique avenue of approach to understanding the encounter between Palestine and developments in psychiatric practice globally, by showing how the introduction into the mandate’s mental institutions of new techniques like electro-convulsive treatment was understood and experienced by families like Zmurud’s. To start with this first point about spaces and actors, Zmurud’s husband Nassif was not, after all, confined for long periods of time behind the walls of a mental hospital but spent most of his time at home, even once admitted for outpatient treatment. Nassif’s condition, moreover, was far from a private matter, concerning patient and psychiatrist alone; in one sense intensely personal, it was at the same time highly social, involving his family as well as a range of officials and other actors. Central though psychiatry and mental illness were to Zmurud and Nassif’s story, theirs is one that might easily slip from view if we keep our sight trained too closely on a single psychiatric institution, or the research and practice of a particular psychiatrist or school. Institutional and intellectual histories of colonial psychiatry have been important in revealing the often uneven integration of psychiatric expertise and practice within the wider panoply of colonial rule.Footnote 4 But stepping outside the institution and de-centring the experts makes possible a rich social history of how colonial subjects navigated mental illness, and how the colonial state, in turn, responded.
Zmurud’s story also demonstrates how mental illness prised open a crucial if unstable space for Palestinians to negotiate in meaningful ways with the colonial state. Her husband’s illness profoundly disrupted her family’s life, but she was neither the passive victim of circumstances beyond her control, nor did she meekly defer to the diagnoses and prescriptions of medical experts. When mental illness made its shocking appearance, Zmurud took action. Across the mandate period, mental illness was understood both as an issue affecting an individual’s health and as a potential, if not actual, threat to the safety of families, neighbours, and wider communities. Zmurud made use of this, and sought out any government agencies she believed might hold the power to help her and her children, turning not just to doctors and health authorities but to the police as well. Rebuffed by one set of officials, she tried another, and rather than accept what experts determined, she put forward her own account of her husband’s condition and proposal for his treatment. Zmurud mobilised her community, too, adding their voices to her own to strengthen her calls for help. Her first petition to the High Commissioner was attested by representatives from Jaffa’s Orthodox Christian community, who urged the government to step in and help with the difficult matter of ‘her mad husband’.Footnote 5 Her negotiations with doctors and officials took place on a markedly uneven playing field, and her grasp of the treatment which her husband was receiving seems partial, but her persistence yielded at least some concessions from the mandate government. This was no mean feat. In the wake of war and with the future of Palestine hanging in the balance, it would not have been difficult to overlook the story of a shoe-maker who had ‘lost his mind’ and beat and threatened his wife and children at home. Zmurud worked hard to make sure this could not be ignored, could not be overlooked, either by her community or by the colonial government.
Striking though her story may be, Zmurud was not alone in being moved by mental illness to enter into such critical negotiations across state and society. Over nearly three decades of British rule, mental illness engendered and sustained complex, consequential interactions within Palestine. Stories of these encounters often reach us in their most compelling form through petitions like Zmurud’s, and with good reason: for all the raw emotion of the human tragedies they convey, these were highly crafted pieces of writing, carefully calibrated to move the state to action. But encounters with mental illness are woven through a dizzying array of archival material: sometimes sensationalised, as in newspaper reportage of criminal insanity trials; at other times, buried beneath the deadening prose and statistics of the department of health’s annual reports. These archival traces reveal that encounters around mental illness played out across a range of spaces and involved a wide cast of actors; they took hugely varied forms. Some, as in the case of Zmurud and her husband, were unspectacular, unequal, often unrewarding negotiations about the care of the mentally ill, initiated and kept going by families who, in their desperation, demanded that the colonial government reach into their homes and take over responsibility for their relatives. If these negotiations offer an insight into what Claire Edington has called the colonial micropolitics of psychiatric care,Footnote 6 and telegraph wider contestations over the nature of mental illness and efficacy of particular therapeutic responses, not all encounters around mental illness played out at such an everyday register. Others unfolded more publicly: in the mandate’s courts, for instance, where judges, lawyers, and witnesses – expert and lay – debated the mental responsibility and legal culpability of defendants in full view of the press and public, and where what was at stake was not simply the fate of the accused individual but the relationship between the law and other forms of psychiatric and social knowledge.
At a different level again, the British authorities found themselves grappling with the specificities of mental illness and psychiatry in Palestine. Some of the dynamics of this encounter find parallels across the colonised world, as colonial states and their medical experts struggled with the question of how cultural difference might affect the expression and treatment of mental illness. In Palestine, unusually, the most systematic attempt to come to terms with this was not through any specialist research but rather through the enumeration of the ‘insane’ population in the 1931 census. Other dynamics were unique to Palestine, most obviously the immigration of hundreds of thousands of European Jews across this period and the concomitant development of voluntary provision for the mentally ill, provision which often outstripped the government’s own. Another peculiarity, no less important, was a set of institutions, understandings, and laws inherited from Palestine’s former rulers, the Ottomans, an inheritance the British more often retained and adapted than uprooted and replaced. A growing body of scholarship highlights the continuities which suture together the histories of Ottoman and British Palestine.Footnote 7 Extending this into the realm of psychiatric encounters furnishes us with not only a fuller appreciation of Ottoman legacies, but also a distinctive angle of approach to global histories of science and medicine, where a commitment to transcending national or even imperial boundaries has not always entailed reflection, as Anna Tsing puts it, on ‘struggles over the terrain of circulation and the privileging of certain kinds of people as players’.Footnote 8 Rather than locate global connectivity in networks of European experts alone,Footnote 9 from the vantage point of mandate Palestine inter-imperial exchange entangled a non-European empire and its European successor, and regional connections established in the late Ottoman period were sustained as much by patients and their families travelling for treatment as by Arab medical doctors and nurses seeking training and professional development.
Encounters around mental illness in mandate Palestine rippled up and down these multiple registers of experience, a testimony to both the polyvalency of mental illness itself as a term always open to negotiation and contestation, and its productive versatility as a lens of analysis which can carry us across the thresholds of social, cultural, or political history. Tracking psychiatric encounters through these layers provides a strikingly different perspective on this crucial period in Palestine’s history. It de-centres and re-contextualises the land purchases, political manoeuvrings, and insurgencies and counter-insurgencies that have served in more teleological political histories as milestones on the road to the end of British rule, the partition of Palestine and establishment of the State of Israel, and the displacement of hundreds of thousands of Palestinians in the nakba.Footnote 10 If a focus on psychiatric encounters opens up vital space for social and cultural history and makes it possible to take the mandate period on its own terms rather than as merely a prelude to 1948, it also reimagines the sites, actors, and indeed sources of the history of psychiatry. Finally, following patients, as well as psychiatric ideas and practices, as they travelled not just within but beyond the borders of the mandate reveals both the connections and the disjunctures which structured Palestine’s position relative to wider regional, imperial, and global contexts. Stories like Zmurud’s, in other words, form a rich tapestry of interactions around mental illness within which state and society are knitted together in sometimes unexpected ways, layers of history and registers of experience often held apart are instead crosshatched into connection, and the threads of certain stories stretch out towards Lebanon, Egypt, and India – or hang loose, trailing off into unknown, uncertain outcomes.
Re-Entangling the Histories of Mandate Palestine
While there is now a growing body of scholarship on the history of psychiatry and the sciences of the mind in the Middle East,Footnote 11 its geographic coverage has been uneven. To date, to the extent that scholars have alighted on the history of mental illness in mandate Palestine at all, they have largely approached it as the story of the struggle of a group of European Jewish psychiatrists to establish their own private clinics, professional organisations, and ultimately the foundations of the future Israeli mental health service after 1948.Footnote 12 Within this scholarship, the history of the mandate’s engagements with mental illness is given little attention, except insofar as the colonial government’s provision is represented as a kind of foil, as forming a parallel if inferior system to that being evolved by and for the Yishuv, Palestine’s Jewish community.Footnote 13 And the history of Palestinian encounters with mental illness and psychiatry is afforded even less weight. In part, this is a result of the privileging of particular kinds of sources as constituting the archive for writing a history of psychiatry in Palestine, above all the publications – whether research articles in medical journals, conference proceedings, or reports by professional societies – of psychiatric experts. In part, it also follows from the adoption of a teleological framing that works backwards from the establishment of the State of Israel and an Israeli mental health service, and thus approaches the history of psychiatry in the mandate period not on its own terms but rather as subsumed within this bigger national story.
Mandatory Madness does not seek to underplay the significance of private Jewish provision: it is an undeniably important dimension of this history and indeed distinguishes Palestine from other colonial contexts. For most of the mandate period, private Jewish provision not merely rivalled but outstripped government provision both in terms of its bedstrength and the kinds of treatment available. Across Palestine’s major cities with significant Jewish populations – cities like Jerusalem, Jaffa, Tel Aviv, and Haifa – private psychiatric institutions proliferated, especially after 1933, when the Nazis came to power in Germany and precipitated the flight of large numbers of European Jewish psychiatrists to, among other destinations, Palestine. Private Jewish provision predated the mandate’s own efforts in this field, too: the earliest institution to tend to the ‘insane’, the Ezrath Nashim home in Jerusalem, opened its doors for the first time in the 1890s, when the Ottomans still ruled. Ignoring this history to focus exclusively on the mandate’s provision, or on Palestinian engagements with mental illness, would not only be impossible, but produce an equally partial understanding of the period.
By adopting a more capacious approach to what the history of psychiatry entails, focussed less on psychiatric institutions and experts than interactions, Mandatory Madness brings the mandate government, the Yishuv, and Palestinians together into a single analytic frame instead. The last two terms appear – like the better-known pairing of Arab and Jew – to denote two mutually exclusive groupings. Yet while their use may be unavoidable, not least as categories adopted by actors at the time, it is important to clarify that these are not neutral or unproblematic descriptions. The position of Palestine’s Sephardi or Mizrachi (‘eastern’) Jews brings this sharply into focus. Former Ottoman subjects, they spoke Arabic with their Muslim and Christian neighbours and were deeply divided on the subject of Zionism, with some joining anti-Zionist protests in the early years of British rule. For their part, European Jewish émigrés were also ambivalent about their ‘backwards’, ‘native’ co-religionists. Yet over time, both as a result of the evolution of a set of Zionist parastatal institutions that claimed, with the mandate’s blessing, responsibility for all of Palestine’s Jewish population, and as a consequence of the failure of Arab nationalists to maintain a clear distinction between Zionism and Jews more generally, these categories did come to form an oppositionary binary. As Ella Shohat puts it, ‘[f]or the first time in Sephardi history, Arabness and Jewishness were posed as antonyms’.Footnote 14 Rather than straightforward descriptions, the terms Arab and Jew, Yishuv and Palestinians, should be treated as denoting protean, contested, and at times overlapping groupings, though in this book I have tried, either through context or through additional qualifiers, to clarify my own usage as far as possible, and, more than this, to highlight how encounters around mental illness at times worked to reinforce and at others served to undermine the hardening boundaries between these categories.
Attending to how mandate officials, European Jewish émigrés, and Palestinian Arabs – Muslim, Christian, and Jewish – engaged with the question of mental illness challenges existing accounts on two key points. In the first place, a shared lens of analysis reveals that government and private provision for the mentally ill, rather than forming separate and parallel systems, were inextricably entangled; the history of one simply cannot be understood in isolation from the other. European Jewish psychiatrists, including those who ran their own private clinics, appeared before the mandate’s courts, testifying to the mental capacity of defendants; they were appointed to inspect and report on criminal lunatic wards; they offered an interpretation of the returns of the ‘insane’ population in the 1931 census. In turn, the mandate government – while attempting in general to avoid assuming responsibility for private institutions – stepped in when these institutions stumbled and their patient populations threatened to spill out onto the streets, either with an offer of subsidies and a demand for reform, or by expanding their own provision.
This dynamic, indeed, can be seen as driving the history of the mandate government’s provision. In 1922, when the first government mental hospital opened outside Bethlehem, it did so in part to relieve the beleaguered Ezrath Nashim institution; in 1932, a second government mental hospital was established, again outside Bethlehem, for much the same reason; and in 1944, a third and final such government hospital, this time near Jaffa, opened and immediately took in all the patients at a nearby private mental institution teetering on the brink of collapse. Knitting these systems together at another level still, patients continuously circulated between private and government hospitals, especially as the costs of private treatment mounted and families turned to government institutions for financial respite. From the vantage point offered by psychiatric provision, colonial and Zionist state-building projects in Palestine appear as enmeshed and often mutually reinforcing, rather than wholly distinct, enterprises.Footnote 15
A second way in which Mandatory Madness departs from existing framings of the history of psychiatry in mandate Palestine is by moving beyond an exclusive focus on the mandate and the Yishuv, above all by writing Palestinians back into this story. Like Zmurud, who mobilised both her community and the government when mental illness intruded on her family’s life, Palestinians – Muslim, Christian, and Jewish – participated actively in the making of this history in myriad ways. They acted as petitioners seeking succour for their relatives, and as plaintiffs, defendants, and witnesses in criminal insanity trials. They were also the doctors, nurses, and hospital attendants whose labour allowed government mental institutions to function and who worked – frequently in the face of indifference on the part of their employer, the mandate’s department of health – to cultivate psychiatric expertise. But writing Palestinians back into this history also dramatically refigures its parameters, by provincialising psychiatry and its medicalised offerings of cure or confinement. The therapeutic trajectories Palestinian families charted for their relatives exceeded both the psychiatric hospital and the colonial archive, as they pursued – often simultaneously – medical and non-medical options alike, in ways which trouble any sharp distinction between the modern and the premodern or the secular and the sacred. And even within the walls of the mental hospital, Palestinian patients might carry with them contrapuntal understandings of their experiences, transforming this site into a space animated, fractured, even haunted by dissonant registers: the psychiatric, the otherworldly, the somatic, the political.
As well as recovering the agency of Palestinians, zooming out from the mandate and the Yishuv reveals the importance of both regional connections and Ottoman legacies to this history. Palestine is often represented as exceptional, not least as the only case in which the League of Nations’ Permanent Mandates Commission endorsed settler colonialism by incorporating the Balfour Declaration, with its commitment of British support for ‘a national home for the Jewish people’, into the mandate text.Footnote 16 Without eliding all of Palestine’s stubborn specificities, widening the camera lens can bring into view how the history of mandatory psychiatry was embedded in the larger regional context. Palestinians travelled for treatment at the Lebanon Hospital for Mental Diseases at Beirut before and after the post-war partition of the region, and the vast majority of aspiring doctors in mandate Palestine had little choice but to make similar journeys north for medical training at the American University of Beirut, as their late Ottoman predecessors had done. And it was not only European Jewish émigrés who pipped the British to the post by transplanting psychiatry to Palestine before the First World War; knowledge of the psy-sciences was already independently circulating across Ottoman Arab territories through scientific journals like al-Muqtataf from the last decades of the nineteenth century onwards.Footnote 17 Their expectations primed by a long visual and literary tradition of representing Palestine as a timeless, biblical ‘Holy Land’,Footnote 18 the British may have arrived imagining that in Palestine, as elsewhere in the colonised world, they would discover a population for whom psychiatry was a novelty and mental illness – commonly understood as an unfortunate by-product of industrial modernityFootnote 19 – a rarity. As it turned out, however, many of their newly acquired subjects were less psychiatrically naïve than the British had fantasised, and came to demand more from their new rulers than the miserly sum set aside for health in the mandate’s budgets allowed.
Taken together, recognition of the interdependency of government and private provision, on the one hand, and of Palestinian psychiatric agency, on the other, warns against assuming too sharp a break between the histories of Arabs and Jews in this period. Far from remaining within the closed circuit of government provision, at least some Palestinians sought treatment for relatives in private Jewish institutions, as well as beyond the borders of the mandate. And large numbers of European Jewish patients were admitted to government mental hospitals, to be treated by Arab doctors and nurses alongside Arab patients. By the end of the mandate period, certainly, the history of psychiatry had been partitioned, along with historic Palestine, as psychiatric patient populations were reordered down ethno-religious lines and government mental institutions were parcelled out between Israel and Jordan. But across the preceding decades, entanglement rather than separation characterised this history, and even after 1948, not all these ties were immediately or fully shredded. In the 1990s, in an attempt to break out of a pattern within the historiography of attending exclusively to either the Arab or Jewish ‘side’ of this story, labour historians pioneered a ‘relational’ approach to the period, which emphasised the mutually constitutive nature of these histories, and put the interactions between them front and centre.Footnote 20 But it is not only in the field of labour history that such an approach is possible. Reconstructing and tracking the interactions generated by mental illness uncovers a new relational history of Palestine, in which Arabs, Jews, and indeed the British mandate seldom negotiated the question of mental illness in isolation from one another.
A History of Psychiatry without Case Files
In Emile Habibi’s satirical classic The Secret Life of Saeed: The Pessoptimist, the narrator is sent ‘strange letters’ which relate the surreal life of the eponymous anti-hero, a Palestinian refugee who ends up acting as an Israeli informant after 1948. Towards the end of the novel, the narrator tracks down the author of these letters first to Acre, and then to the mental hospital housed in the same building that had served as a notorious prison during the mandate period. After expressing astonishment to the hospital’s staff that a shrine to those executed by the British on the site commemorates only members of a Jewish paramilitary organisation, and not the Arabs whom they hanged as well, the unnamed narrator attempts to discover who the mysterious Saeed might really be. Together, they search the hospital’s records, trying to discover Saeed in among all the patients admitted since the founding of the state, but are unable to find anyone with that name. They then look for similar names, and ‘find one that looked suspicious’: Saadi. But that is all the hospital’s records yield; the only additional information the narrator is able to glean from the hospital staff about his elusive correspondent is that a woman had recently visited the hospital from Beirut to ask after him – and that he had died the year earlier.Footnote 21 The archival trail has gone cold.
For historians, as for Habibi’s narrator, the search for patients among the records of the mandate period can be a frustrating one. Zmurud’s story is a case in point. Although she had been reassured by the mandate government that her husband Nassif would be admitted as soon as a bed in the mental hospital at Jaffa became available, I have been unable to find any document in the colonial archive which would allow us to ascertain when – or if – this ultimately took place, let alone a case file with which to continue this story. In this respect, Nassif’s case is typical. With the notable exception of files relating to criminal lunatics, patient case files do not appear to have survived. They are not to be found among the many other records of the mandate’s department of health held by the Israel State Archives today. Nor are any records on site in Bethlehem at what was at the time the first government mental hospital, and which has continued since 1948 to operate as a psychiatric hospital under first Jordanian rule and, after 1967, Israeli occupation.Footnote 22
Alongside the limited survival of patient case files in the archive, historians must contend with a decidedly uneven body of published material. While European Jewish psychiatrists and other experts published research based on their clinical experiences in private institutions in Palestine, no parallel set of publications about mental illness was produced in this period by the Arab doctors who made up the majority of the staff of the mandate’s department of health. These lacunae and imbalances in the kinds of sources which have been the anchors of most institutional and intellectual histories of psychiatry are in part responsible for the existing scholarship’s portrayal of this history, as one in which European Jewish psychiatrists are the principal actors, the mandate government a bit player, and Palestinians off-stage entirely. In the absence of these conventional sources, historians appear to have concluded that the history of psychiatry in mandate Palestine is itself non-existent and have focussed their attention on the Yishuv instead. Just as historians of decolonisation in the region have innovated methodologically when faced with inaccessible or absent archives,Footnote 23 so too does Mandatory Madness contend that embracing a less conventional, more eclectic body of sources – even from within the colonial archive – can uncover an expansive, ultimately richer history of psychiatry in mandate Palestine.
Rather than treat the limited survival of case files and the uneven publication of psychiatric research simply as an obstacle to recovering this history, or as evidence of its absence, accounting for this archival state of affairs can also be itself revealing. The asymmetry in research publications, for instance, is an important reminder that bringing the mandate, the Yishuv, and Palestinians into the same frame of analysis should not obscure their stark differences, or imply an equivalency. The first was a colonial state, sanctified in international law under the cover of a different name but able to marshal troops and resources from across the British empire in moments of need. The second was welded across this period into a state-in-waiting, complete with its own self-governing institutions, by a highly organised political nationalist movement and with the recognition and practical support of the mandate. Meanwhile the third was an indigenous population who had been colonised in the wake of profound wartime political and social dislocation and whose political rights were never, in spite of their tireless efforts to organise, afforded international recognition. These and other differences crucially shaped the conditions within which psychiatric and medical expertise was cultivated and validated. Put simply, while European Jewish psychiatrists and other specialists working in private institutions had the freedom to select clinically interesting patients, trial new methods of treatment, and publish their findings, the department of health – the most important though not the sole employer for Palestinian Arab doctors across the period – invested little in developing Palestinian psychiatric expertise, instead abetting conditions of work at government mental institutions that restricted opportunities for research or any other kind of specialist development.
The lack of psychiatric research published by those employed in the mandate’s department of health marks Palestine out from other colonial contexts. While ambitious French and, to a lesser extent, British psychiatrists often found in the colonies a laboratory that they could use to push the limits of the field, establish their reputations, and ultimately return to the metropolitan medical stage feted as pioneers,Footnote 24 Palestine was different. It sat in contrast to medical services elsewhere in the British empire, where western-trained doctors drawn from the colonised population only gradually replaced Europeans in the interwar decades in India, or the post–Second World War decades across much of sub-Saharan Africa.Footnote 25 Instead, from the start the majority of the employees of the department of health were former Ottoman subjects who had received medical training in Beirut, Istanbul, Damascus, and CairoFootnote 26 – though across this period the highest ranks in the department were filled exclusively by Europeans. Allocated a paltry 4 per cent of government expenditure most years, the health department prioritised tackling infectious diseases – above all malaria – over providing hospital care,Footnote 27 and certainly over nurturing psychiatric expertise.
This is made clearest by the career of the doctor who was in charge of the government’s only mental hospitals for most of the period, Dr Mikhail Shedid Malouf. Malouf – a central, albeit elusive, character in this book – started out working as an ophthalmologist, before being given responsibility for the first government mental hospital in 1925. Rather than receiving support from the government to develop his expertise by, for instance, taking specialist training abroad, he appears to have had to learn on the job. Whether as a result of a lack of formal qualifications or simply time, he never drew on his extensive clinical experience to publish, and so, besides a handful of reports produced for the government and the occasional interview, frustratingly little exists by way of his writing. This situation did not change even in the 1940s, when Palestinian Arab doctors working in the department of health, voluntary clinics, and mission hospitals came together to form the Palestine Arab Medical Association and launched their own Arabic-language medical journal in 1945. In spite of their enthusiastic support for the cultivation of specialist knowledge, psychiatry was not on their radar. It never featured, for instance, among the articles published by Palestinian doctors in the association’s journal, where the focus – as for the health department – was on either infectious diseases like malaria or infant and maternal health.Footnote 28
The picture was very different for European Jewish psychiatrists and other medical doctors in Palestine. While some were employed by the department of health, the large number of doctors arriving from Europe to Palestine from 1933 onwards meant that out of both necessity and desire, many more practised privately – if they were lucky, that is, and were not forced into other forms of work entirely.Footnote 29 Already by 1920, the growing community of European Jewish doctors in Palestine had established a Hebrew-language medical journal, Harefuah, which did – by contrast to the journal of the Palestine Arab Medical Association – publish a number of articles on psychiatry, particularly in the 1940s as new forms of treatment like electro-convulsive therapy were introduced in private Jewish mental institutions. In this respect, European Jewish psychiatrists resemble settler colonial scientists elsewhere, who took advantage of what Richard Keller has called the ‘unique opportunities for experimentation and innovation’ offered by settler colonies like French Algeria.Footnote 30 A well-established body of scholarship approaches Zionism as a settler colonial movement,Footnote 31 but this framing can obscure as well as illuminate. Harefuah, as Sandra Sufian has noted, was one strand in the larger project of evolving a distinctively Hebrew medicine, complete with its own Hebrew medical dictionary.Footnote 32 This knowledge production was thus less aimed at international audiences, with a view to securing glittering careers elsewhere, than at a national constituency, itself under construction at the time – marking a point of distinction between psychiatric research in Palestine and in other settler colonial contexts in the same period.
If reflecting on the unevenness of published research can reveal something about expertise and the conditions under which it was enabled or constrained, patient case files – the other archival mainstay of histories of psychiatry – raise different issues. Except in relation to ‘criminal lunatics’, who were institutionalised in prison lunatic wards and who were necessarily the subjects of scrutiny and correspondence by multiple government branches, patient case files do not survive, whether destroyed as a result of routine bureaucratic practices or any number of upheavals across the past century. But even those case files which do survive, for so-called criminal lunatics, can frustrate as well as illuminate, and their use requires careful methodological as well as ethical deliberation.
An example that illustrates some of these issues is the relatively chunky file relating to Abraham P. Although judged a criminal lunatic by the courts, Abraham had been admitted to the government mental hospital at Bethlehem in 1926, rather than one of the mandate’s prisons, where the majority of criminal lunatics were detained. Most documents in his file are short summaries of the findings of a medical board which convened each year to examine his health and chart any improvement in his condition. Interlaced with these, albeit with decreasing frequency as the years dragged on, is correspondence from his wife, Haya, communicating through a lawyer. In 1929, for instance, she wrote to request that her husband be examined, in the hope he would be deemed fit for discharge. But the examining board found him to be ‘dull, apathetic, slow in speech, slightly negativistic’; he ‘[s]till believes that at times the hospital food is either adulterated or poisoned’; and, when asked why he went to the toilet up to twenty times a day, he told them, ‘I don’t know but I was forced by certain internal ideas or impulses to go there.’Footnote 33 He was not recommended for release. Haya visited the hospital, and in another letter through her lawyer in February 1930, claimed she had been told that her husband would be released in the next few months.Footnote 34 But this turned out not to be accurate. The medical officer in charge of the hospital, Dr Malouf, reported that, far from improving, Abraham’s condition ‘is tending to deteriorate and that it is unlikely to improve in the near future’.Footnote 35 Over the next fourteen years, a medical board was convened annually to examine Abraham; each time, they found him to be not fit for discharge from the hospital, having failed to improve. When he arrived in the government mental hospital in 1926, he was around thirty years old; by the time of the final entry in his file, when he was examined in February 1944, he would have been nearly fifty.Footnote 36
Abraham’s file is in many ways rich in the kinds of details that historians of psychiatry have productively used in their research. We learn about his particular fear of being poisoned; we get a sense of his wife Haya’s struggle to have him released, in a striking counterpoint to Zmurud’s equally determined efforts to have her husband admitted; we are even tantalised with the prospect of hearing him speak, as his explanation for his behaviour is given in quotes in the report. But his file is also riddled with issues. It only starts in 1929, but we know he was in the hospital from 1926; it ends in 1944, but we do not learn whether he was released or died, if indeed this represents the end of his time in the institution at all rather than an accident of record-keeping or archival survival. Like so many similar files in the archive, his file is bookended by mysteries. Reading his file, we never learn why or on what charge Abraham had been detained as a criminal lunatic in the first place; indeed, in spite of the length of the file – over fifty pages – we learn remarkably little about Abraham at all across the two decades he spent within the government mental hospital, beyond whether his condition was judged to have improved or not on a year-by-year basis, a stark reminder that these files were produced through set processes for a particular purpose.
But Abraham’s file also raises questions around contemporary archival practice and the ethics of doing this historical research, too. At least when I first accessed his file, his full name was left unredacted. While this is not in itself unusual or problematic, the Israel State Archives – which holds the vast majority of records produced by the mandate governmentFootnote 37 – also did not ask researchers accessing this file to sign the kind of agreement promising to respect patient anonymity which other archives holding sensitive medical records make a requirement for access; instead, this and many other medical and health files were made freely available to all online in an unredacted form. It is my decision, then, informed by reflections on the ethical as well as methodological challenges of working with such sources,Footnote 38 particularly where unfettered access to these sensitive patient records might perpetuate the extreme vulnerability of the subjects of colonial psychiatry into the present,Footnote 39 to give only Abraham’s first name and an initial – a practice I repeat for every patient encountered in Mandatory Madness, as well as for close family members like Zmurud – in order to preserve a degree of anonymity.
Rather than approach the absence of patient case files and the uneven corpus of published research as an obstacle, then, Mandatory Madness reads these lacunae and asymmetries for what they can reveal of the history of mental illness in mandate Palestine. But it does not remain fixated on these sources as the sole foundations of any history of psychiatry. Instead, it turns to a range of archival and published sources, from census reports, court records, and folklore research, to English-, Hebrew-, and Arabic-language newspapers, memoirs by police officers, and petitions from Palestinian families. While a careful reading of these and other sources – including budgets, disciplinary proceedings, and architectural plans – can shine a light on the inner workings of mental institutions otherwise left dark by a dearth of patient case files, drawing on this more eclectic mix of sources is generative rather than only substitutionary. These sources embody and make possible the more expansive social history of psychiatry in Palestine which is at this book’s core. They take us outside the walls of the institution and delineate a history of mental illness that takes place across encounters in the courtroom, the prison, the home, and the street as much as the hospital. They take us beyond the mandate’s borders, too, to those sites outside Palestine that nonetheless played key roles in this history, whether as alternative options for psychiatric treatment, centres for training, or models to be emulated: the Lebanon Hospital for Mental Diseases outside Beirut is the most important example of all three. In recent decades, historians of colonial psychiatry have produced rich, compelling portraits of particular institutions and colonial contexts, but – with notable exceptionsFootnote 40 – have paused at the hospital’s boundaries or the colony’s limits. Broadening out what counts as the archive of colonial psychiatry and mental illness not only makes it clear that mandate Palestine most certainly has a story to be told, but it also shifts the centre of gravity within this story, placing interactions and entanglements across as well as within borders at the heart of the action.
Psychiatry and Politics in Mandate Palestine
Since the early 2000s, Palestinian researchers, practitioners, and activists have been at the forefront of critiques of the potentially depoliticising effects of psychiatric diagnoses like post-traumatic stress disorder, which threaten to reduce pain and suffering to an individual pathology by ignoring the political as well as social determinants of health.Footnote 41 While this body of work makes a powerful argument for the need to reckon with the impact of political events and structures on mental and emotional health, and reframe responses to trauma to include demands for justice, linking together politics and mental health remains a difficult undertaking for historians.Footnote 42 This is not least because it raises a thorny issue of retrospective diagnosis, which most are loath to stretch their source base to attempt. One approach historians have found more comfortable as well as productive has been attending to the political commitments and effects of psychiatrists producing knowledge within colonial contexts. At one end, much attention has been given to figures like the ethnopsychiatrist J. C. Carothers, commissioned by the Kenyan government during its brutal suppression of the anti-colonial Mau Mau revolt in the 1950s to provide a psychological explanation of the uprising, an explanation which placed more emphasis on the mal-adaptation of the colonised subject than on dispossession and political disenfranchisement.Footnote 43 At the other end of the political spectrum, Frantz Fanon famously laid the blame for mental disorders in Algeria’s war of independence squarely at the feet of the French: it was colonialism, ‘a fertile purveyor for psychiatric hospitals’, which drove the colonised subject mad.Footnote 44
Mandate Palestine produced neither a Carothers nor a Fanon. As we have seen, those working within the mandate’s mental institutions did not publish much at all, whether for specialists or wider audiences. They did not, by contrast to Palestinian mental health practitioners today, draw on their expertise or clinical experience to diagnose the pathologies of occupation.Footnote 45 And even among those European Jewish psychiatrists who published both internationally as well as in Harefuah, any engagement with political questions took place at a different register. Rather than deploy the psy-sciences to legitimise or critique British rule, a more pressing political question for this group, as Sandra Sufian has demonstrated, was understanding what high rates of mental illness among Jews in Palestine meant for the Zionist promise that aliya or immigration to Palestine would redeem the mentally, as well as physically, ‘degenerate’ Diaspora Jew.Footnote 46
The relationship between psychiatry and politics in mandate Palestine, then, might appear to be less direct than in other contexts. But it is nonetheless important. In the first place, although psychiatric experts themselves were not mobilised either for or against the mandate, psychiatric modes of thinking were taken up into politics anyway. As Sloan Mahone highlights, it was not only medical experts who understood and sought to realise the political possibilities offered by the psy-sciences in the early twentieth-century colonial world.Footnote 47 In Palestine, too, ideas of irresponsibility drawn from the social sciences as well as the sciences of the mind seeded themselves in the prose of counter-insurgency produced by officials assigned the task of explaining ‘disturbances’ over the mandate’s three-decade span. And the single most significant example of mental illness being put to work to reinforce the logic of colonial rule came from the pen not of a psychiatrist nor even a medical doctor, but rather a mathematician: the superintendent of the 1931 census. In the census, enumerators were tasked with recording rates of ‘insanity’ alongside other kinds of infirmity in the population. Yet another kind of psychiatric encounter ensued, this time between enumerator and enumerated, at the doorway of the home. The census superintendent mobilised the returns of the ‘insane’ population produced through these encounters to argue that Palestine’s three putative communities perched on distinct rungs in the ascent to modernity: the Muslim population farthest from modernity, the Christian population somewhere in the middle, and the Jewish population the closest and thus the best qualified to support British developmentalist ambitions in the country.Footnote 48
Psychiatric encounters speak to the political history of the period in other, sometimes surprising ways, too. During the great Palestinian revolt that rocked the foundations of British rule across the late 1930s, for instance, petitions reveal that even as relations between the mandate and its Palestinian subjects reached a nadir, families continued to write to the government to request that it step in and relieve them of responsibility for caring for mentally ill relatives. At the same time, against a backdrop of the criminalisation of nationalism and the targeting of the conditions of everyday life as part of British counter-insurgency strategy,Footnote 49 courts struggled to determine what was pathological in criminal insanity cases: was it defendants’ behaviour, or the wider context of violence in which they found themselves?
Precisely because the intersections between psychiatry and politics were often indirect, the rest of this section provides an outline of the political history of this period by way of orientation. Before the First World War, Palestine was ruled by the Ottomans for centuries, though not as a single administrative unit: Acre and Nablus in the north were incorporated into a province centred on Beirut, and – as admissions data from the Lebanon Hospital for Mental Diseases suggest – not a few Palestinians continued to look to Beirut when seeking out treatment for relatives in the decades after the British and French partitioned the Levant. Palestine shared in many of the broader transformations of the late nineteenth- and early twentieth-century Ottoman empire.Footnote 50 But there were also specificities at play here. The particular attention commanded by Palestine as a ‘Holy Land’, for one thing, made it – and Jerusalem above all – the site of notable investment by missionaries, resulting in a proliferation of schools, hospitals, and other institutions.Footnote 51 The mandate owed multiple debts to these mission foundations: not only were many of the staff of the health department educated at mission schools, but the buildings which housed the first two government mental hospitals at Bethlehem had originally been constructed by mission organisations.
Alongside missionary efforts, of course, what also marked out Palestine as distinctive was its centrality to the Zionist movement. Zionism, a political movement cohering by the end of the nineteenth century around the idea of securing self-determination and escaping anti-Semitism in Europe through the creation of a Jewish national home in Palestine, found concrete expression in these decades in the first two aliyot, that is, waves of migration by European Jews to Palestine.Footnote 52 Beginning in the 1880s, and continuing up to the end of the mandate in 1948, aliyot profoundly reshaped Palestine’s demographics. In 1922, around a tenth of the total recorded population was Jewish;Footnote 53 towards the end of the mandate, that proportion had risen to a third, from 84,000 to 554,000, a change driven largely by migration.Footnote 54 Even before the dramatic leap in numbers across the 1930s and 1940s, European Jewish migrants were reshaping Ottoman Palestine in other ways: it was in the late Ottoman period that Tel Aviv, a new city to the north of historic Jaffa, started life. This was also a foundational period for the emergence of consciousness around a specifically Palestinian form of national identity, though this did not, as Michelle Campos has shown, preclude the simultaneous investment by Palestine’s Muslims, Christians, and Jews in other forms of identification, including as Ottoman citizens.Footnote 55
With the Ottoman entry into the First World War, events were set in motion that would result in the British occupation of Jerusalem by the end of 1917 and the north of Palestine the year after; the establishment of an interim civil administration in 1920; and finally the confirmation of British rule in the novel configuration of a mandate of the League of Nations in 1922. The mandate system appeared to break with pre-war European imperialism by recognising only a mandatory power’s administrative control, rather than sovereignty, over territories seized during the war, and by specifying the intended outcome of this arrangement: self-rule, once a period of ‘tutelage’ had elapsed. Like other territories of the dismembered Ottoman empire shared out between the British and French, Palestine was classed as an ‘A’ mandate, that is, understood as having ‘reached a stage of development’ which warranted provisional recognition of its existence as an independent state, and which – it was envisaged – would mean a relatively short period of ‘advice and assistance’ by the mandatory power before it was judged ‘able to stand alone’.Footnote 56
That Palestine was a mandate mattered. This was less to do with the generic architecture of the mandates system, which required mandatory powers to submit regular reports to representatives of different member states sitting on the Permanent Mandates Commission in Geneva, and which allowed mandatory subjects to petition the Commission over the head of the mandatory power – though a number of historians have shown that Palestinians made inventive use of these mechanisms.Footnote 57 Nor, as Mandatory Madness demonstrates, was the mandate particularly consequential for the management of mental illness: more often than not, the mandate government took its cues from other points of reference – from other British colonies, particularly India and Egypt, and Ottoman legacies – rather than Geneva, and conformed to an empire-wide pattern of underinvestment in psychiatric provision. Where the mandate did, however, matter was in its incorporation of the text of the 1917 Balfour Declaration. This wartime declaration committed Britain to supporting the creation ‘in Palestine of a national home for the Jewish people’, on the condition that this should not ‘prejudice the civil and religious rights of existing non-Jewish communities’. In reducing the majority of Palestine’s population to ‘non-Jewish communities’ with civil and religious but not, crucially, political rights, it inaugurated a process of reordering as a result of which Palestinian Jews were split off from their Muslim and Christian neighbours, and ‘Arab’ and ‘Jew’ emerged as the ascendant and antagonistic categories into which the population of Palestine could ultimately be partitioned.Footnote 58
With the text of the mandate committing the British state to facilitating Jewish immigration and settlement on the land,Footnote 59 even before it was confirmed it had become a lightning rod for Palestinian opposition: riots against Zionism and British rule broke out in 1920 in Jerusalem, and the following year in Jaffa, too. The mandate also gave official recognition to the Zionist Organisation, founded at the end of the nineteenth century, as a public body that would advise and co-operate with the administration in the creation of a Jewish national home. Under the coordinating leadership of the Jewish Agency, as it became towards the end of the 1920s, a set of parastatal institutions evolved that went on to form the sinews of the State of Israel after 1948. This included the Vaad Leumi, the Jewish National Council, which organised its own health committee to coordinate the activities of two of the most important Zionist medical agencies: the Hadassah Medical Organisation, which was established in the United States on the eve of the First World War to promote health initiatives in Palestine, and the Kupat Holim, which provided medical insurance to workers in the Histadrut, the federation of Jewish workers in Palestine.Footnote 60 In addition to this role, the Vaad Leumi’s health department – led across this period by Dr Avraham Katznelson – advised, berated, and negotiated with the mandate department of health, including around provision for the mentally ill. The colonial archive bulges with his correspondence, alternately excoriating the government’s failure to provide enough beds for psychiatric cases and intervening on behalf of Jewish families to request that their relatives be urgently admitted to government institutions for treatment. Denied similar recognition of their political rights, and boycotting elections for legislative institutions which the government tried to set up on the grounds that participation would require an acceptance of the terms of the mandate, Palestinian Arabs by contrast faced a much more challenging road to organising. By the 1930s, however, Palestinian nationalist politics had entered a new phase, with the formation of the Istiqlal (‘independence’) party, and the adoption of new strategies to mobilise workers and peasants to exert pressure on the British, including through strikes.Footnote 61
Rumbling beneath these developments were profound socio-economic dislocations, as a crisis of Palestinian landlessness and impoverishment deepened, driven by Zionist land purchasing on the one hand, and the failure of the British to address agrarian taxation and indebtedness on the other.Footnote 62 With ever-increasing numbers of Palestinians pushed to precarious existence at the urban margins by deteriorating conditions in the countryside, an incident involving the holy places in Jerusalem in 1929 sparked the first serious revolt since the establishment of the mandate, and led to bloody communal violence in Jerusalem’s Old City, Safad, and Hebron. Less than a decade later, an even more significant episode of anti-colonial rebellion unfolded. Starting in April 1936 with a general strike that was sustained for an unparalleled six months, the great revolt evolved into a countrywide armed uprising which was only suppressed in the second half of 1939 as a result of a British counter-insurgency effort entailing, at its height, the deployment of tens of thousands of British soldiers to Palestine on the eve of the Second World War. The great revolt and its suppression left few areas of life untouched, including the provision of healthcare. In 1938, armed men broke into the government mental hospital at Bethlehem and murdered a Jewish member of the hospital’s staff. Iron shutters and iron doors were subsequently installed to secure the staff dormitories,Footnote 63 and two British police officers billeted at the hospital at night.Footnote 64 While a striking number of Palestinians continued to approach the mandate on behalf of mentally ill relatives even across these fraught years of insurgency and counter-insurgency, some at least were not reassured by the security measures put in place at government hospitals: admissions to the Lebanon Hospital for Mental Diseases from Palestine spiked in this period.
During the great revolt, the British had moved beyond tinkering with immigration quotas to propose a more radical solution to the Palestine question: partition.Footnote 65 Recommended in the first place by the Peel Royal Commission in 1937, it was dropped in favour of restrictions on Jewish immigration in 1939 that aimed to ensure a degree of political quiescence in Palestine during the Second World War. The majority of Zionists were willing to put on hold their opposition to this policy in order to concentrate on the war effort against the Nazis, and so the years of the war marked a period of relative quiet in Palestine and indeed saw the expansion, in important if uneven ways, of psychiatric provision and expertise. It was against the backdrop of one of these developments, the opening of a new mental hospital near Jaffa in 1944, that Zmurud dared to hope that her husband might be admitted as a patient; conversely, it was following the piloting of new kinds of treatment during the war years that the government responded in a quite different way to how she imagined, offering electro-convulsive therapy to him as an outpatient. With the war’s end, opposition to the continued restriction of Jewish immigration escalated into a Zionist paramilitary campaign aimed at dislodging the British by force.
Exhausted by the war, and under international pressure to allow unrestricted Jewish immigration to Palestine as the horrors of the Holocaust became more fully known, in 1947 Britain passed the question of Palestine on to the new United Nations to resolve. In November 1947, the UN voted in favour of partitioning Palestine into two states: a Jewish state comprising much of the coastal plains including Jaffa, Tel Aviv, and Haifa, as well as stretches of territory in the interior to the north and south; and an Arab state, comprising the hilly interior of the country including Nablus, Hebron, and Ramallah – but not an internationalised Jerusalem – as well as stretches of the coast around Acre in the north and Gaza in the south. But events on the ground quickly overtook this plan: first, as civil war between the Yishuv and the Palestinians broke out even in advance of the British withdrawal in May 1948; and then as the newly established State of Israel defeated the armies of neighbouring Arab states and seized a much greater portion of territory than envisaged in any previous partition proposal. Across both phases of the war for Palestine, 750,000 Palestinians were displaced in what became known in Arabic as the nakba, or catastrophe, while those parts of Palestine which remained in Arab hands were divided between Jordan in the West Bank and East Jerusalem, and Egypt in the Gaza Strip.Footnote 66
While 1948 marked the moment at which the State of Israel was able to bring together and transform a patchwork of voluntary and government mental institutions into the foundations of a national mental health service, the opposite was true for the Palestinians. Though Jordan inherited a government mental hospital in Bethlehem, the history of provision for Palestinian mental health fragmented after 1948. Across the 1950s and 1960s, the World Health Organization assumed some responsibility for arranging and funding medical training regionally, while the United Nations Relief and Works Agency footed the bill for Palestinian patients who, like generations before them, found their way to the Lebanon Hospital for Mental Diseases for treatment. The psychiatric partition of Israelis and Palestinians was shadowed, in other words, by a fragmentation in responsibility for Palestinian mental health. Entanglement as a thread which had knitted the history of psychiatry together across the mandate period snagged and unravelled. To track these diverging histories past 1948 would require different frameworks, different archives, and engagement with a different set of questions about psychiatry’s transformation in an unevenly decolonising worldFootnote 67 – in short, another book.
Encounters around Mental Illness in Mandate Palestine
Mandatory Madness unfolds across three loosely chronological parts; each chapter within these parts focusses on a particular kind of encounter around mental illness. Part I covers the opening years of British rule in Palestine, from wartime occupation to the census of 1931, and tracks the early efforts of Palestine’s new rulers to understand and manage mental illness. Both chapters in this part reveal the extent to which British actions and knowledge around mental illness were shaped by the legacies of the Ottoman past; subject to debate and critique among a wide range of actors; and driven by developments and pressures on the ground. The first chapter reconstructs the dynamics of the initial encounter between the British and the question of mental illness in Palestine. Far from recapitulating a familiar narrative about the colonial introduction of psychiatry, it instead offers a multi-layered account of the opening of the first government mental hospital at Bethlehem, in order to highlight how the British were in fact latecomers to an ongoing history of psychiatry in Palestine. Well before the British occupation of 1917, Palestinians had recourse to a range of medical and non-medical options for the management of the mentally ill, and those existing understandings, experiences, and institutions crucially shaped how the British responded to mental illness across these formative years. The second chapter takes us to the start of the 1930s, to explore the colonial production of knowledge on mental illness. It does so not through the writings of any psychiatric expert, but rather through the report of the 1931 census and its extensive analysis of the return of the ‘insane’ population. Rooted in a very particular encounter around mental illness – between enumerator and enumerated – the census report’s analysis and the debates surrounding it reveal how the question of mental illness could be used to locate both Palestine and its different communities in relation to empire, development, and modernity.
Part II, which centres on the 1930s and 1940s, is threaded together by a focus on a set of negotiations around mental illness between the mandate government and Palestinian – Arab and Jewish – families. Taken together, these chapters reveal families to have exercised a considerable degree of agency in relation to the management of their mentally ill relatives. The third chapter takes as its subject the petitions which flooded the mandate government from the 1930s onwards, seeking the admission of relatives to the government’s mental institutions. These petitions are read both for what they reveal about the often complex therapeutic strategies pursued by families and as carefully crafted arguments about mental illness and the state’s obligations to its subjects. The fourth chapter turns to the encounters around mental illness which played out in the colonial courtroom. Criminal insanity defences forced mandate judges, medical experts, and lay witnesses alike to engage in debate about what forms of behaviour and thought were evidence of mental illness and what should, by contrast, be considered normal, ‘rational’, and therefore punishable for a given defendant. Neither ‘insanity’ nor – as the fifth chapter demonstrates – ‘criminality’ were stable categories in 1930s and 1940s Palestine. Particularly in the 1940s, mandate officials worried that the families of the mentally ill were staging criminal offences in order to have their relatives smuggled into institutional care through the back door as criminal lunatics. By working closely with case files from the rich archive of the criminal lunatic section at Acre, this chapter delves into the more complex dynamics which sometimes surrounded individuals’ routes in and out of this institution, and attempts to recover their experiences of this space.
Part III focusses on the final decade of the mandate period, and shifts the emphasis away from encounters between state and society towards understanding how novel forms of psychiatric expertise and practice were negotiated by different groups within Palestine across the 1940s. The sixth chapter traces two major developments in this transformative decade: the opening of the third and final government mental hospital at Jaffa in 1944; and the cultivation of expertise around wartime trauma and mental nursing. In both instances, investment was driven as much by colonial subjects and crisis as by British design, and built figuratively as well as literally on the foundations of the past. The seventh and final chapter brings us, at the end, to the encounter between patient and psychiatrist, and between Palestine and new methods of psychiatric treatment developing globally. Across the 1930s and 1940s, a set of therapies that used work, drugs, and electricity to intervene on the body to cure the mind were introduced into private and government mental institutions in Palestine. Though these techniques tantalised with the promise of transcending context through their universal applicability, this chapter highlights instead how they travelled to and were deployed within Palestine in a highly uneven way. The book closes with an epilogue, focussed squarely on 1948. By reconstructing a series of psychiatric encounters that attended the end of the mandate period, the epilogue draws out the profound rupture both of this moment and the processes of partition, erasure, and pathologisation which surrounded it. This rupture radically diminishes the possibilities for continuing any unitary, entangled history of psychiatry within the territory of what had once been mandate Palestine.

