

Malaria can be found everywhere and should be found nowhere. Malaria is entirely and completely under human control. Give me the healthiest locality in the world, and I will develop there malaria in twenty-four hours. Give me the most malarious district of the globe, and in time I will remove from it every trace of malaria.Footnote 1
By the second quarter of the nineteenth century, as I have suggested, quinine began to signify the collective curative properties attributed to cinchona barks. In different moments in the century, across dispersed locations, quinine was recognised as the cure of a variety of maladies including fevers, dysentery, sore throat, headache, toothache and impotence.Footnote 2 Mostly such debilities were projected as results, preconditions or expressions of exposure to malaria. It has been shown in existing histories that malaria remained an ambiguous diagnostic category through most of the century. The word malaria could mean a fever-disease as well as a cause behind many diseases.Footnote 3 It surfaced as a commodious label, and was variously flexed and eclectically invoked.Footnote 4 Quinine was cited as the most consistent and effective remedy of maladies associated with malaria. Quinine and malarial diseases were often projected as invariably connected. Quinine was employed as a pharmacological agent in quick-fix diagnostic tests. Whether a malady was malarial could be determined, it appears, from how the suffering body responded to quinine.Footnote 5
Writings about malaria in the nineteenth century were certainly not confined to the English language, but the bulk of it emerged from English-speaking parts of the world, particularly North America, Great Britain and its colonies. One of the recurrent themes in most of these writings was to describe malaria as an insensible, imperceptible, invisible, imponderable ‘mystery’.Footnote 6 Any form of physical unease witnessed almost anywhere could be potentially attributed to malaria. Such projections, however, coexisted with attempts to delimit malaria as tangible and perceptible.
Many existing histories either extend twentieth-century (or even more recent) medical understandings about malaria by analysing the political and economic causes behind historical outbreaks, or draw on these recent medical insights about malaria to retrospectively chart out the patterns of mortalities and events in earlier centuries.Footnote 7 This chapter focuses on the nineteenth century to trace the ways in which malaria itself was reconsolidated as a widely accepted diagnostic category across the imperial world. An analysis of English medical journals, government correspondence, physicians’ memoirs, treatises and books reveals the cultural and political history of how during this period malaria was reinforced as an object of knowledge and governance. Malaria was re-inscribed and sustained in the course of the century through, what Gregg Mitman calls an ‘ecology of knowledge,’Footnote 8 which was occasioned considerably by burgeoning imperial formations. Malaria was not only shaped by, but also, in turn, held together an extensive imperial network. The recurrent nodes which constituted this network included: places dispersed across the distant corners of the colonial world; objects ranging from decaying plants to sun-baked rocks; careers of geologists, meteorologists, chemists, economic-botanists, colonial administrators amongst others; and processes including the production of racesFootnote 9 and regions, circulation of labour, intervention of the state, and the governance of compensation, architecture, pedagogy and revenue. In disparate ways, therefore, Empire and malaria were both co-consolidated by an assemblage of interconnected places, processes, objects and careers. As in the case of cinchona plants I would note here that imperial networks were hardly preordained and inflexible, but were instead ‘becoming with’ the categories they were themselves putting together.
Particularly significant are the various perceived material configurations of malaria. Malaria was often described as invisible and imponderable. At the same time, a range of entities and organisms such as decaying vegetation, friable granite rocks, water casks, mouldy bed sheets, stale mushrooms, dusty old books, refuse of indigo factories and groups of humans described pejoratively as tribes, aborigines, negroes and primitives were shown to personify malaria in contemporary texts. Although themselves immune, they were believed to affect their immediate vicinities with malaria. The material and physical configurations of malaria thus transgressed human–nonhuman binaries.
A history of malaria enables an engagement with continuing scholarly efforts to narrate the relevance of materials and objects in imperial history while retaining a critique of the ways in which scientific knowledge was put together.Footnote 10 Nineteenth-century malaria alerts us to the need for bringing histories of ideas and histories of material inscriptions into a sustained dialogue. While resisting the temptations of biological determinism and denying any possibility for accessing straightforward materiality of objects, historians need to examine the obsessive invocations of materials and objects in contemporary published discourse about malaria.
Such an approach also builds on considerably the literature about spatial history more generally and the production of colonial disease ecologies in particular.Footnote 11 Indeed, malaria reveals the ways in which the various constituents of the nineteenth-century colonial world were conceived as parts of a wider geographical, ecological, medical and environmental paradigm. Distant and diverse locations in Australia, Batavia, Ceylon, India, Sierra Leone or the West Indies were shown to share characteristics peculiar to colonial landscapes. The ‘imaginative geographies’Footnote 12 of colonial landscapes drew upon the extant nineteenth-century stereotypes ascribed to the tropics, the East, hot climates, Torrid Zone, Indian Ocean region and so forth. Yet the recurrent invocation of materials such as rocks, casks, decaying leaves and the politics of race, regions, class or governance in contemporary literature about malaria suggests that the colonial landscapes, as Alan Bewell alerts us, ‘were not simply the product of the ethnocentric inscription of pathologies onto blank spaces’.Footnote 13 Colonial landscapes figured not only as imagined recalcitrant spaces, but also as lived places which various subjects and objects of Empire inhabited and negotiated.Footnote 14
This is certainly not to reduce all histories of malaria to episodes within colonialism. Rather this chapter explores the historical specificities in which malaria acquired exceptional currency in nineteenth-century public cultures within imperial Britain and in the wider colonial world. In so doing, it interrogates the conventional chronologies of scientific knowledge production by revealing the ways in which cures like cinchona plants and the drug quinine did precede and shape understandings about the diagnostic category, malaria. First, the discovery of quinine in the 1820s was followed by the beginnings of unprecedented circulation of the category malaria in English language sources. Secondly, with the establishment of cinchona plantations in European colonies in the mid-nineteenth century, malaria shifted from being considered a predominantly European preoccupation to an almost exclusively colonial concern.
‘Insensible and Imponderable Poison’Footnote 15
By the late 1820s, quinine manufactured commercially in Europe began reaching colonial outposts in India. A letter written by James Low from Calcutta in June 1828 to his brother Alexander Low in Jersey confirms this.Footnote 16 The letter suggests that Alexander Low had followed Pelletier and Caventou's footsteps in extracting quinine from cinchona barks. Quinine manufactured by Alexander Low in Jersey was shipped to Calcutta, where his brother received it. James Low, who otherwise worked for a bank, invested considerable energy in distributing quinine in Calcutta on behalf of European manufacturers. The letter also indicates that James Low acted as a local agent in Calcutta representing a European quinine dealer named Pelletier. It is not entirely unlikely that James Low's employer was the same Frenchman who co-discovered quinine in 1820, and who by the late 1820s was running a business venture known as the Pelletier pharmacy, and had undertaken commercial manufacture of quinine.Footnote 17
James Low noted that the simultaneous arrival of various vessels carrying quinine into Calcutta had led to a ‘glut of that article’, which threatened to bring down the selling price of quinine from Rs. 25 per ounce to Rs. 4 per ounce. Under such circumstances, James Low found it difficult to profitably sell all the quinine he had received from various sources. Thus the commercial interests of Pelletier clashed with those of British manufacturers of quinine like Alexander Low. James Low mentioned that he was caught between his commitments to his brother and obligations towards his employers. The letter also indicates how the East India Company's government in British India had, by then, emerged as a convenient site for disposing of excess quinine. It hints at strategic alliances between higher officials in the colonial government, distributors of quinine in Calcutta, commercial manufactures of quinine in Europe and possibly phytochemists.
A single letter perhaps provides inadequate archival foundation for reconstructing the complex history of trade in quinine in the late 1820s, but it does offer certain revealing suggestions. Within eight years of its discovery, apart from being considered as an alkaloid confined to European phytochemical laboratories, quinine acquired the status of a lucrative item in distant colonial markets. An extensive network of European manufacturers, shipping corporations, colonial distributors and administrators had begun investing in quinine. This converged with a plethora of publications about malaria from within Britain and its colonies. The geologist John MacCulloch's 500-page book was one of the most detailed works on malaria to be published in the wake of the recognition of quinine as a lucrative commercial item. This book was published by Longman, Rees, Orme, Brown and Green in London a year before James Low's letter was written.
Here malaria figures variously as the cause behind myriad expressions of physical unease.Footnote 18 At the same time, MacCulloch defined malaria as an ‘invisible’,Footnote 19 ‘insensible and imponderable poison…’Footnote 20 ‘…which has hitherto eluded all chemical investigation’.Footnote 21 MacCulloch identified malaria along with odour and contagion as the three mysteries that confronted contemporary chemistry,Footnote 22 and lamented the inability of chemical tests to detect its presence as ‘easily as oxygen or carbonic acid’.Footnote 23 The existence of malaria could be gauged retrospectively from its perceived effects on the human body.Footnote 24 Once a particular ‘situation’ was framed as malarial, every form of physical unease witnessed there, MacCulloch argued, could be confidently attributed to malaria.Footnote 25
Malaria, MacCulloch suggested, could remain latent within a body, and manifest itself several years or decades after the body had imbibed it or been exposed to it.Footnote 26 Even when one travelled away from ‘malarial situations’, the body once exposed to malaria, could retain and manifest it.Footnote 27 In MacCulloch's narratives, malaria figured as both invisible and mobile or portable. Malaria could durably attach itself to tangible materials and be transported to distant places along with them.Footnote 28 By referring to theories of motions and currents, and meteorological observations, MacCulloch suggested that “migration or dispersion” of malaria did not necessarily follow horizontal routes.Footnote 29 Like currents, malaria could descend or move vertically upwards.Footnote 30 It rarely moved in a straight line and often adopted capricious and curvilinear paths.Footnote 31 Depending upon the various degrees in strength and direction of winds, MacCulloch argued, malaria could travel varying distances. If malaria did manage to cling on to winds that were rapid, singularly steady, linear and horizontal, MacCulloch argued, it could cover a distance far greater than that between Holland and England.Footnote 32
Malaria was thus perceived as a highly malleable, commodious and fluid category. Diverse varieties of maladies witnessed in eclectically dispersed locations could be conveniently attributed to malaria. MacCulloch thus suggested that malarial diseases could appear anywhere. However, he tried to identify certain ‘situations’ as more malarial than others. Although malaria could travel and cause ill health anywhere, it was generated in specific locations which he termed as most notoriously ‘malarious’. ‘Accurate and minute knowledge of the exact spot and of every spot, productive of malaria’, MacCulloch thought, was the first necessary step towards ensuring protection from malarial diseases.Footnote 33
‘Wetness’ emerged as a constant feature, which in MacCulloch's narrative defined malarial spots. Landscapes bearing tangible traces of water were almost obsessively labelled as malarial; to the extent that a contemporary reviewer suggested that the author might be suffering from ‘professional hydrophobia’.Footnote 34 MacCulloch began by identifying marshlands – whether saline or stagnant – as potential sources of malaria.Footnote 35 He was meticulous in his description of ‘malarial marshlands’. Such marshes, MacCulloch suggested, were characterised by the co-existence of water and living vegetation. Malaria emerged when living vegetation went through the process of decay. He defined ‘decay’ as an intermediate stage ‘between life and absolute decomposition’.Footnote 36 MacCulloch argued that different plants as well as different parts of the same plant were more prone than others were towards decomposition or putrefaction. In the process, these generated poisonous exhalations with varying degrees of impact. By claiming to track the chemical action of decaying vegetations over moist soil, he appeared simultaneously to engage with different disciplines – geology, chemistry and botany.Footnote 37
Malaria, MacCulloch claimed, could also be witnessed in many situations which were not, ‘in a usual lax sense’, defined as a ‘marsh’.Footnote 38 The generation of malaria did not require extensive space,Footnote 39 but could happen in ‘smallest fragments of wet lands’,Footnote 40 in a ‘thousand, unsuspected places…’Footnote 41 ‘…obscure as well as innumerable’.Footnote 42 Thus, various ‘undrained spots’, ‘wet woods’, ‘moist meadows’,Footnote 43 ‘rushy pools’, ‘petty swamps’,Footnote 44 ‘peaty bogs’,Footnote 45 vicinities of mobile water bodies such as mountainous rivers, tide rivers, mangrove rivers,Footnote 46 ‘smallest streams’,Footnote 47 urban drains,Footnote 48 ditchesFootnote 49 and canalsFootnote 50 were labelled as potential non-marshy sources of malaria.
Examples of ‘malarial situations’ were extended to include locations which were devoid of any form of vegetation. Malaria provided MacCulloch an opportunity to also pathologise a range of quotidian and negligible sites, spaces and objects such as vicinities of ponds in gravel pits,Footnote 51 milldams,Footnote 52 water casks,Footnote 53 the refuse of indigo factories,Footnote 54 garden dunghills,Footnote 55 flax and hemp in the stage of soaking,Footnote 56 bilge water produced from the leakage of sugar in the voyaging ships at the seaFootnote 57 and mud laid bare by the summer heat.Footnote 58 One commentator subsequently hinted that in malaria MacCulloch found a euphemism for ‘fenny or marshy’ counties as well as urban conditions such as ‘neglected drains, ill-conditioned sewers, imperfectly trapped cesspools and overflowing dead wells’.Footnote 59
MacCulloch invoked not only the sciences of chemistry, geology, meteorology, natural history and botany, but also the ‘practical wisdom’ of doctors and farmers.Footnote 60 This meshed with his claim of having access to narratives involving distant places. MacCulloch distinguished himself from ‘domestic and untravelled’ writers.Footnote 61 He frequently cited travelling authors like Francis Buchanan Hamilton,Footnote 62 VolneyFootnote 63 or Captain Smyth.Footnote 64 His narrative thus could engage, for instance, anecdotes involving malaria in Lombardy with those relating to Bengal,Footnote 65 China,Footnote 66 the West IndiesFootnote 67 or North America.Footnote 68
Whence else should fevers come? Do they not thus come in Italy and in Africa? Have they other causes in Rome or Mantua than here? The Thames indeed is not the Congo, nor can we parallel Ostia or Terracina; the fevers do not slay in three days; but the disease is the same, the poison the same, and the same is the cause.Footnote 69
MacCulloch began one of his eleven chapters by advocating: ‘To detail the geography of malaria for the whole world, would be little else than to write a general grammar of geography’.Footnote 70 He intended to construct a ‘map of malaria of the world’Footnote 71 to contribute to the processes of ‘war, colonisation and commerce’, and to the disciplines of political economy and statistics. Despite these grand programmatic statements, his detailed engagement with ‘malarial situations’ drew upon examples predominantly from England and different parts of continental Europe. This is certainly not to overlook his numerous invocations of malarial locations beyond Europe. Such citations, however, were stray and sporadic. Europe appears to have been the focus of his work. He elaborately projected familiar features within British or continental landscapes as potentially malarial. ‘I must almost limit myself to Europe…by such a detail, I may perhaps at length convince our incredulous countrymen that there is such a thing as Malaria under blue skies and amid the perfume of orange flowers’.Footnote 72
Much of his chapter on the geography of malaria was based on one Captain Smyth's accounts of towns located on the shores of the Mediterranean. This geography revealed a long ‘statistical catalogue of towns’Footnote 73 located in France, Sardinia, Sicily, Portugal, Italy, Greece and Spain.Footnote 74 Macculloch located ‘malarial spots’ even in certain parts of Switzerland,Footnote 75 Denmark, Poland, Russia,Footnote 76 Moldavia, Wallachia and Hungary.Footnote 77 Commenting on the prevalence of ‘malarial situations’ in the interiors of France, MacCulloch wrote, ‘so numerous are the tracts and spots of this nature…that an entire catalogue would form almost a geographical grammar of the country.’Footnote 78 The Mediterranean shore of France figured in MacCulloch's narrative as ‘one entire range of malaria from the Pyrenees to the Alps.’Footnote 79 He attributed low life expectancy rates in contemporary Europe (that is, twenty-five in Holland, fifty in England, and twenty-two in certain districts in France) to malaria.
He argued that England continued to remain under the sway of malaria. England's malarial past, he suggested, was enshrined in the statistical and medical history of the two preceding centuries. Malaria was a ‘scourge’ for London as it was for the rest of the country. Oliver Cromwell apparently died of malaria.Footnote 80 In relation to England, MacCulloch described malaria as a ‘Destroying Angel’.Footnote 81 England was ‘comparatively freed from malaria, by industry and attention. However, it was not yet exempt’.Footnote 82 His narrative on the geography of malaria bore extensive references to English parishes, ‘unwholesome districts’,Footnote 83 and ‘fenny peaty counties’.Footnote 84 MacCulloch identified various sites on the borders of the Thames,Footnote 85 river banks about Reculver, on Heron Bay,Footnote 86 Kent in the Isle of Thanet,Footnote 87 Epping Forest in Essex,Footnote 88 and Sussex, Kent, Hampshire,Footnote 89 Cambridgeshire, Somersetshire, Lancashire and HuntingdonshireFootnote 90 more generally as malarial.
He associated malaria with some of the most beautiful European landscapes, and his descriptions reveal considerable poetic moments in the narrative. These scenic landscapes could be deceptive, MacCulloch suggested. Malaria, he thought, could easily mingle with European prosperity, beauty and grandeur. Thus, for example,
…Amidst the splendor and fragrance of the walnut, the olive, the vine, the fig, and the almond, intermixed with jessamines, aloes, roses, myrtles, oleanders, and a thousand aromatic shrubs, in the very bosom of beauty and luxuriance, amid the delights of a spot which poetry would lose itself in celebrating, the miserable and cadaverous natives drag out a wretched existence; dying rather than living where the vegetable world spreads all its colours and odors to summer airs and bright skies.Footnote 91
Italy, the fairest portions of this fair land is a prey to this invisible enemy, its fragrant breezes are poison, the dews of its summer evenings are death. The banks of its refreshing streams, its rich and flowery meadows, the borders of its glassy lakes, the luxuriant plains of its overflowing agriculture, the valley where its aromatic shrubs regale the eye and perfume the air, these are the chosen seats of this plague, the throne of Malaria.Footnote 92
Commenting on the insalubrities associated with the ‘most romantic lakes’ of Switzerland, MacCulloch remarked:
The general purity of the waters of a lake, added to its brilliancy, often to its romantic or picturesque character, and not a little aided by poetical feelings or metaphysical prejudices, commonly remove all suspicion…the physician…the painter or the geologist will discover or even see, along the shores of such a piece of water, the particular ground which is a cause of suspicion or a source of disease…he will see reasons of suspicion, even in the most romantic lakes of an alpine region…Footnote 93
MacCulloch linked malaria to European aesthetics, opulence and splendour, apart from landscapes and demographics. Small wonder then the capitals of various aggrandising European empires in different centuries figured as seats of malaria. MacCulloch projected ‘Imperial Rome’ – the ‘eternal city’,Footnote 94 Athens – ‘the Wapping of Greece,’Footnote 95 Babylon,Footnote 96 Paris,Footnote 97 and London – ‘our own capital’Footnote 98 as victims of malaria. He did not invariably associate malaria with poverty. On the contrary, he understood malaria as ‘death knocking at the door of the opulent to spare the mean’.Footnote 99 Overcrowded situations, streets or habitations, MacCulloch showed, were capable of neutralising the effects of malaria.Footnote 100
He pointed out that residence across successive generations in European ‘malarial districts’ in France and Italy could produce a ‘degeneracy of the races’. The inhabitants of such districts often appeared to suffer from rickets and deformities.Footnote 101 The colour of their skin mostly turned sallow or yellow, or appeared stained with different hues and livid.Footnote 102 ‘Personal beauty’ in women, MacCulloch thought, dwindled prematurely. They appeared unhappy, stupid, apathetic, melancholic and insensible.Footnote 103 These adversely affected the ‘moral conditions’ of the people, and the ‘moral life’ of the inhabitants of such districts, MacCulloch argued, was ‘frightful’. Infanticides, abortion, drunkenness, want of religion, gross superstitions and assassinations were frequently encountered in these European ‘malarial districts’ as a result of enduring exposure to malaria.Footnote 104
Malaria thus featured in this 1827 book as an elusive and invisible diagnostic category which could be deployed to ascribe medical connotations to a diverse range of predominantly European sites and situations including stagnant marshes, industrial wastes or spectacular Swiss lakes. Malaria could be invoked to explain not only a variety of debilities like fevers, impotency or idiocy, but also moral and racial degenerations, ugliness and the general absence of public order.
The ‘First Book’ and Its Author
MacCulloch's book was published at a time when the invocation of malaria as a diagnostic category in the English language was acquiring unprecedented recurrence. A foray into the overlapping worlds of bureaucratic correspondence, journal articles, reports on the health of the army, medical manuals, treatises and monographs uncover such trends. It is possible to locate stray references to the expression malaria in medical literature written in the English language before the nineteenth century. However, most medical historians who have written on malaria in early-modern England and North America continue to engage in conscious acts of retrospective diagnosis. These works have tended to ascribe malaria with connotations, which the category acquired in the late nineteenth and early twentieth centuries, and were hardly known or in use earlier.Footnote 105 Such histories suggest that ‘chills and fever’, ‘fever and ague’, ‘estivo-autumnal fever’, ‘marsh fever’ and ‘jungle fever’ were different ways to describe the same disease.Footnote 106 Thomas Sydenham, Robert Talbor, James Lind, John MacCulloch and experts on the germ theory figure in these works as characters, who in different centuries contributed collectively towards knowledge of a continuous and unchanging disease.Footnote 107 These works have been authored by various scholars ranging from social historians of demography like Mary DobsonFootnote 108 to a group of archaeologists, who by conducting DNA tests, claim to have excavated traces of plasmodium falciparum and malaria in a Roman villa in the mid-fifth century AD.Footnote 109 It might be misleading anachronistically to situate commentators invoking various categories in different contexts as part of the same teleological narrative on malaria. Failing to appreciate the changing meanings ascribed to a category in specific historical periods is equally problematic. This chapter recognises malaria as a commodious category of knowledge, a flexible diagnostic label and a significant ordering principle. Unprecedented textualisation, circulation and firmer entrenchment of the word malaria in English language sources beginning in the late 1820s should have a history of its own. The publication of John MacCulloch's Malaria in 1827, seven years after the discovery of quinine, constitutes a crucial moment in that history. In the next year MacCulloch published another book on the same subject.Footnote 110
Malaria, which surfaced in English texts from the 1820s onwards, inherited the older meanings associated with the Greek word miasma and Italian word mal'aria in vogue in the earlier centuries.Footnote 111 This was enabled in a decade marked variously by a ‘revival of interest in Hellenistic culture’Footnote 112 in Britain, ‘a revival of classical humoral aetiological theory’Footnote 113 and a ‘renewed Hippocratism,’Footnote 114 and an appreciation for its foundational tenets of ‘Airs, Waters and Places’. At the same time, the increasing relevance of malaria as a credible category in the following decades was further enabled not only by the global proliferation of print markets, but also by concerns about agricultural improvement, labour circulation, colonial governance and stagnation in industrial Britain. The emerging disciplines of economic botany, geology, chemistry, meteorology and medical topography found in malaria a problem worth exploring.
A reflection of this wider interest was the claim both in contemporary history and in historiography about malaria being a relatively new category in the early nineteenth century. Historians who have written on malaria in early modern England, Spain or North America have themselves acknowledged the rarity of the ‘term malaria’ in contemporary medical literature. Juan Riera Palmero and Anastasio Rojo Vega have suggested that the ‘term malaria was totally unknown in eighteenth-century Spain’.Footnote 115 Erwin H. Ackerknecht has pointed out that the ‘Italian word malaria was not introduced into English medical literature until the first half of the nineteenth century’.Footnote 116 Mary Dobson and Richard Wrigley have in their own works suggested that ‘the word achieved popular usage in the English language’Footnote 117 after the publication of MacCulloch's work on malaria. One of MacCulloch's biographers has called him ‘the precursor of the discipline of Malariology’, and credited him with ‘the introduction of the word malaria’ into English scientific writing.Footnote 118
Quite curiously, MacCulloch projected himself as the pioneer of English writings about malaria. According to him, ‘the truest account of the nature of malaria would be an acknowledgment of utter ignorance’.Footnote 119 He suggested that malaria could have been sporadically invoked in the past. However, it remained an ‘unseen and unknown’ category.Footnote 120 He claimed to be the author of the first full book-length study of malaria in English.Footnote 121 Malaria constituted a ‘subject’, he argued, that had ‘never before been submitted before an English public’.Footnote 122
Soon after publication, MacCulloch's work was widely reviewed and cited in essays written or published from distant locations. One Dr Hardy published an article titled ‘On the Malaria and the Medical Topography of Oudypoor’ (in British India) in the Transactions of the Medical and Physical Society of Calcutta in 1831.Footnote 123 In the same year Transylvania-based physician Charles Caldwell's Essays on Malaria and Temperament was published from Kentucky in the United States.Footnote 124 Otherwise considerably critical of MacCulloch's work, these authors reconfirmed his claim to being one of the earliest to write on malaria in English. Much later in the century, Thomas Wilson, an official working for the Dutch government, authored a treatise called An Enquiry into the Origin and Intimate Nature of Malaria. Describing MacCulloch as the proponent of ‘the theory of universal malaria’Footnote 125, Wilson showed how ‘prior to the appearance of MacCulloch, no one had given to the theory of malaria any definite form’.Footnote 126 ‘It can scarcely be said that any author prior to MacCulloch ever considered this matter from a philosophical or physiological point of view…’.Footnote 127 In the 1880s and even later, journals published in Bengali from distant Calcutta continued to recognise MacCulloch as the first English author about malaria.Footnote 128
Engendered by contemporary commercial, political and institutional cultures, the nineteenth century thus witnessed not only a new energy of writing and publishing about malaria, but also the need to discover a first original author. Emphasising the originality of the ‘first’ author, citing him as an inheritor of received knowledge, revealing him as respectable, and constantly referring back to him; all these taken together underscored the credibility and significance of MacCulloch, of the subsequent authors and of the category malaria itself.
Biographical entries on MacCulloch published in the nineteenth century and later projected him as a man of many facets. Perhaps it was helped by the fact that he had established himself as a prolific author much before his works on malaria were published. It is possible to suggest that his enduring credibility as an author provided the category malaria renewed currency in nineteenth-century Britain and beyond. The work on malaria was published eight years before his death, and was one of his last works.
Writing on malaria was one amongst his several other significant identities. One of his biographers has pointed out how he was eclectically trained in different disciplines.Footnote 129 Although he studied medicine at Edinburgh University in the 1790s, he developed considerable interest in chemistry, natural history, geology, botany, mineralogy, mathematics and zoology. Despite his formal training as a doctor, he was for much of his professional career a geologist, at a time when geology was being institutionalised in industrial Britain with the participation of mining interests, land surveyors, canal builders, coal prospectors, drainage experts, mineral assayers, quarrymen and civil engineers. MacCulloch joined the Geological Society of London in 1808. In 1811 he was commissioned by the Board of Ordinance to locate alternate sources of limestone for use in British gunpowder mills to those in Belgium. He returned to Scotland to determine the most appropriate types of rocks, searching for silica-free limestone for millwheels. In 1814, he was appointed geologist to the Trigonometrical Survey, which was then engaged in preparing a one-inch topographical map of Scotland. Between 1814 and 1821, he was engaged in examining the geology of about hundred Scottish peaks and compiling a geological map of West Scotland. He narrated his activities and revelations as a geologist in a series of publications. Much before the publication of his first work on malaria in 1827, he had already published most of his seminal works on geology. These included A Description of the Western Isles of Scotland, including the Isle of Man (1819), A Geological Classification of Rocks (1821) and The Highlands and Western Isles of Scotland (1824). The second book acted as a textbook of geology in the East India College for ten years.Footnote 130 A 4-mile-to-an-inch geological map of Scotland prepared by MacCulloch appeared posthumously in 1836. It is considered to be the first official geological survey of any country in the world.Footnote 131 Although intensely criticised for considerable topographical and geological inaccuracies, it was not superseded for many years.Footnote 132 Two years after his death while on honeymoon to Cornwall in 1835, his Proofs and Illustrations of the Attributes of God was published, which revealingly argued that geological evidence revealed the work of God in creation.Footnote 133 This image of the pioneer English writer about malaria as a God-fearing man of science is comparable to the devout Christian beliefs of John Eliot Howard, the most widely celebrated Victorian authority on quinine.
MacCulloch's career bore revealing overlaps with contemporary colonial projects. He was an industrial geologist employed by the British government to work in Scotland. He suggested in The Highlands and Western Isles of Scotland (1824) that the Highlanders were ‘indolent and lazy’, lacked ‘military propensities’ and should be cleared from the land.Footnote 134 This met with vigorous criticism. He taught chemistry and geology to the cadets of the East India Company at the East India College at Addiscombe from 1814 until his death in 1835, and received financial support from the East India Company towards publishing his books, including A Geological Classification of Rocks (1821) and A System of Geology (1831). These were intended as practical reference works for engineering field officers in India, and acted as textbooks for the courses he offered at Addiscombe.Footnote 135
Writing about Macculloch in the late 1850s, Thomas Wilson recalled that he ‘moved in the best circles’.Footnote 136 As early as 1801, he was elected fellow of the Linnean Society.Footnote 137 He served as the president of the Geological Society of London between 1816 and 1818, and was elected Fellow of the Royal Society in 1820.Footnote 138 Well before the publication of his work on malaria, he had thus established himself as a versatile and prolific writer. In addition to his nine major books, he had written about seventy-nine scientific papers. These addressed topics as diverse as geology, the art of making wine, marine fishes and crabs, Greek fire and indelible ink.Footnote 139
His reputation lent significant currency to the category malaria in the English language. This shows why his work on malaria was reviewed in locations as distant as Kentucky in the United States and Rajputana in British India within two years of its publication. The significance ascribed to men like MacCulloch in contemporary British culture is explained by the curious ways in which these careers linked apparently disparate worlds of natural history, geology, medicine, Industrial Revolution, romanticism and colonialism.Footnote 140 Perhaps this is why within thirty years of its publication, as the Dutch official Thomas Wilson suggested, MacCulloch's book had found many sympathisers in different departments of the English government including the sanitary board.Footnote 141 MacCulloch's views on malaria found acceptance amongst a network of diverse interests represented by the government, medical faculty and sewer makers.Footnote 142 ‘Supporting and maintaining the theories of MacCulloch’, Wilson suggested, emerged as one of the viable ways of ensuring ‘lucrative official appointments’.Footnote 143 Inspired by MacCulloch's analysis of malaria, the government had launched extensive schemes in the late 1850s towards ‘improving’ the drainage of the city of London.Footnote 144 MacCulloch's theory of malaria, Wilson observed, had received significant government appreciation since his death in 1835. MacCulloch was very uncertain about the effectiveness of his denunciation of open sewers, undrained streets, untrapped cesspools and overflowing dead-wells. Execution of such projects entailed damage to the proprietors of London residences. MacCulloch had even solicited counsel from a ‘distinguished barrister’ apprehending legal retaliation from propertied interests in London.Footnote 145 Contrary to his apprehensions, Wilson showed, MacCulloch's book on malaria had begun enjoying patronage from the political establishment in London by the 1850s.
Thus, both MacCulloch and his book resonated in a range of publications about malaria in the decades that followed. Even when reviewed, contested and ridiculed, MacCulloch's work featured as a point of reference for the next half-century.Footnote 146 Many of the impressions conveyed in the book were modified over the course of the century, but the category malaria was retained as a credible way of defining land, landscape and people in distant locations. The use of the expression malarial in the English language proliferated. This converged with the crystallisation of the image of MacCulloch as the author who published the first full-length book on malaria. The book was followed by publications from a dispersed network of authors on the subject. These authors hailed from diverse contexts and pursued different sets of interests. They included medical professors based in Kentucky,Footnote 147 British Indian bureaucrats from Rajputana,Footnote 148 officials working for the Dutch government,Footnote 149 physicians working for the US army,Footnote 150 and editors of medical journals in the vernacular.Footnote 151 Such authors published in scientific journals,Footnote 152 bureaucratic correspondences,Footnote 153 book-length treatises,Footnote 154 medical reports of national armies,Footnote 155 and Bengali journals.Footnote 156 Most of these authors were engaged in reciprocal acts of quoting and citing from one another's works, and in the process they appeared to endorse each other's credibility as authors on malaria. These in turn vindicated the proliferation of malaria as a medical term. Recurrent projections of MacCulloch as the first English author on malaria were related to such efforts of deriving legitimacy.
At last one man, a shrewd, intelligent and influential observer, a man of genius, gave to the whole question a new phasis. Since his day his hypothesis has undergone a variety of modifications, as was to be expected, in no way, however, affecting the practical deductions originally drawn from it by its author.Footnote 157
Retention of the category malaria by subsequent authors, by itself, was related to such efforts to establish legitimacy. These authors appeared to cling on to a word associated with an established figure. MacCulloch himself, however, began both his books on the subject by referring to two closely related terms, that is, malaria and miasma. According to MacCulloch, his consistent use of the Italian word, malaria, instead of the ‘Greek expression miasma’ was one of ‘preference’.Footnote 158 However, he did not provide justifications behind such preference. Nor did he elaborate on any technical distinction between these two terms. He appeared uncertain and was silent about the distinctions between them. From the 1830s onwards he was recognised as an authority on malaria and not miasma. Similarly, authors in English who claimed to follow MacCulloch's pioneering lead projected themselves as experts on malaria and not miasma. Later in the century, some of these authors tried to distinguish between these two categories. They tried to justify the recurrent usage of one term over the other. Malaria according to these authors conveyed certain connotations which could not be subsumed within the expression ‘miasma’. Most of these efforts were witnessed from the 1850s.Footnote 159 As late as 1881, Joseph Edwards, a physician based in Philadelphia, wrote:
The word malaria has been derived from the two words mal aria i.e. bad air…the word miasm has a different origin, being derived from the Greek…a stain, I contaminate…although Dunglinson in his medical dictionary refers the definition of the word malaria to miasm or miasma and so confound the two…they are distinct…while malaria…is a comprehensive term for atmospheric impurities of various kinds; miasma conveys the idea of an effect and not a cause, it is a stain, a contamination of some portion of the human body…the only relation that they can possibly hold together is that of cause and effect, malaria or bad air being the cause and miasma or contamination being the effect of this cause…Footnote 160
MacCulloch remained an archetypal writer on malaria in English for much of the nineteenth century in other ways. His claims to being the first author on malaria in English ironically converged with his attempts to project it as an established explanatory category in Europe.Footnote 161 ‘Hundreds of writers’ including ‘Lancisi, Sennert, Orlandi, Platner, De Baumes, Zimmerman, Pringle, Lind, Blane, Jackson’, he argued, ‘explained this subject…sufficiently’.Footnote 162 He associated malaria with certain significant events in European military history.Footnote 163 Malaria figured not only as a cause of disease, but also as a factor which determined the fates of decisive battles and expeditions. Discussions about malaria, Macculloch pointed out, were not confined to the savants in Europe, but had occurred across classes and beyond Europe. ‘Through out the world it is a fact known to the vulgar, and even to less enlightened nations; familiar to the Negroes of Africa, familiar to the lower orders of France, Italy, Holland and not less known to at least our own rural population’.Footnote 164
Similarly, subsequent writers followed MacCulloch to project malaria as a credible diagnostic category which had endured several centuries. Narrating long histories of malaria seems to have been one recurrent way of achieving this. These writers appeared able to trace the category in the writings of legendary medical writers and literary figures of previous centuries. For example, a Philadelphia-based physician R. La Roche described malaria as a ‘long admitted efficient agent’ and devoted a chapter towards locating the ‘antiquity of this opinion’.Footnote 165 Medical writers from Hippocrates and the Galenics,Footnote 166 down to Ramazzini and LancisiFootnote 167 in the seventeenth century, argued La Roche, had commented on the same disease-causing entity, which in the nineteenth century was known as malaria. Thus, while MacCulloch's narrative on the ‘antiquity’ of thinking about malaria began with Lancisi, La Roche's ended with him.
Like MacCulloch himself, many subsequent writers who published in the first half of the century, appeared simultaneously invested in many disciplines.Footnote 168 Knowledge about malaria was thus accessed, framed and articulated in the language of different disciplines. Thomas Herbert Barker, a British physician based in Bedford, won the Fothergillian Prize Essay for 1859 from the Medical Society of London for On Malaria and Miasmata.Footnote 169 It summarised the different ways in which geologists, meteorologists and the organic and inorganic chemists were engaged in addressing the ‘profound mystery’ called malaria. This explains how different definitions of malaria could co-circulate around the nineteenth century. Barker pointed out, for instance, that chemists like Samuel Metcalfe defined malaria as inorganic poisons, which resulted from the decomposition of organic matters.Footnote 170 Metcalfe appeared to add that malaria constituted organic matter in the gaseous state, in the forms of carbonic acid, carburetted hydrogen, phosphuretted hydrogen and ammonia. Malaria then, according to these chemists, could reveal itself to chemical analyses.Footnote 171 Barker's book suggested how the 1850s witnessed beginnings of the cell origin or germ theories of malaria. He referred to Pettenkofer and Grainger, who explained malaria in terms of animal effluvium. ‘Effluvium consists of organic matter, a protein compound in a most minutely divided form and therefore adapted, in a special manner to enter the blood, to diffuse itself rapidly and extensively’.Footnote 172 Amongst the geologists, Barker referred to Sir Ranald Martin, who projected high temperature in a ferruginous soil as favouring the generation of malaria.Footnote 173 Martin also appeared to explain malarial situations in terms of the electrical conditions of the atmosphere.Footnote 174 Such coupling of meteorological observations with geological references was, according to Barker, reflected in other writings as well.Footnote 175 Most meteorologists appeared to explain malaria in terms of season, climate, barometrical pressure, hygrometrical state, temperature and elasticity.Footnote 176 MacCulloch, as I have already noted, claimed to derive insights from chemistry, botany, geology, meteorology and geography. Following him, subsequent writers on the subject pursued the definition of malaria through different disciplines and arrived at diverse answers.
Colonising Malaria, Malarial Colonies
To understand malaria, MacCulloch suggested, one needed to explore its possible geographies. In his narrative, he frequently cited anecdotes about malaria relating to various places. Some of these locations and landscapes kept recurring in MacCulloch's account as particularly malarial. Throughout his book he projected continental Europe and England as the heartland of malaria, although sporadically and rarely he referred to Africa, West Indies, and certain sites in India, North America and even China.
Many later nineteenth-century authors adopted his anecdotal style of writing about various places, peoples and objects. That the geographies of malaria were undergoing significant mutations, however, had become evident by the 1850s. Published geographies of malaria began gradually to shift away from Europe and to bear uncanny overlaps with the emerging geographies of colonial cinchona plantations. The global geographies of European empires, cinchonas and malaria seem to have overlapped to a considerable extent and in significant ways by the third quarter of the nineteenth century. Until the1840s, as I have suggested, cinchonas were predominantly confined to the networks of circulation between ‘natural forests’ in South America and sites within Europe and North America. Surviving images and relics associated with cinchonas and malaria from the first half of the nineteenth century or even earlier invoke objects, landscapes and people related almost exclusively to Europe.
The jar (see Figure 2.1) is amongst a collection of containers of cinchona barks that have survived from the eighteenth and early nineteenth centuries, and which were in use in different parts of Europe.Footnote 177 Similarly, the sketch (see Figure 2.2) published in the Penny Magazine and the lithograph (see Figure 2.3) drawn by Français in the first half of the nineteenth century refer to European landscapes, figures and attires while describing malaria. By the time Maurice Sand (1823–1889) painted his allegorical work ‘The ghost of the swamp’ (Figure 2.4), explicit references to European people and landscapes had begun to fade at least in certain sectors of visual culture, even as the iconography of malaria continued being dominated by European artists.
Figure 2.1 Image of ‘Albarello drug jar used for cinchona bark, Spain, 1731–1770’.
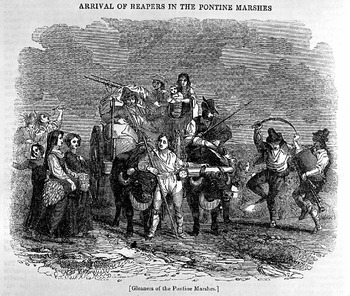
Figure 2.2 Sketch with the note ‘Gleaners of the Pontine Marshes. These people suffered from malaria when working on the Marshes’, Penny Magazine, 1837, vol. 6, 337.
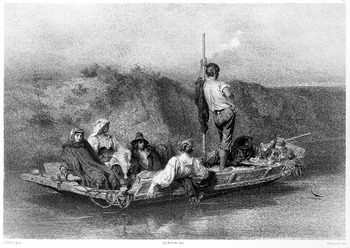
Figure 2.3 Lithograph of ‘A group of people adrift in a boat, perhaps suffering from malaria’. Lithograph by Français after A. E. Hébert, 1850.
Figure 2.4 ‘An allegory of malaria’. Reproduction of an engraving after M. Sand (1823–1889) c. 1850s.
The 1840s witnessed the beginnings of most sustained proposals for the establishment of cinchona plantations in the Dutch, French and British colonies.Footnote 178 In the 1850s, cinchona seeds and plants from the ‘natural’ cinchona forests in South America had been transported to many of these colonies. By the 1860s, experimental plantations had been set up in Dutch Java, French Algeria and British India, Jamaica and Ceylon (see Figure 2.5). These enabled unprecedented circulation of the cinchonas between different parts of the colonial world.Footnote 179 Such locations included Algiers, Burma, Ceylon, India, Java, Jamaica, Mauritius and Wellington. These newer destinations of cinchonas and quinine were described as places precisely in need of such commodities. In the emerging medical geographies, these locations appeared to abound in particularly malarial situations. The official files which documented the transfer of cinchona plants and seeds were one of the earliest and most consistent sites projecting, for instance British India, as a predominantly ‘malarial’ landscape – a land of death, fever and disease.Footnote 180
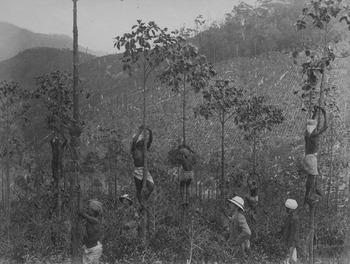
Figure 2.5 Reproduced by the kind permission of the Syndics of the Cambridge University Library. Royal Commonwealth Society Library, Photograph collection of John Abercromby Alexander, Shelfmark: RCS/Y303E_47. (No infringement of copyright intended.) This photo describes local inhabitants engaged in the cinchona plantations in Ceylon (most probably in Peradeniya), circa 1880–1890.
This is however not to suggest that the mid-nineteenth century indicated an absolute shift in the perceived geography of malaria. References to sites within Europe did not disappear altogether.Footnote 181 Nor was every colonised location described as absolutely exempt from the effects of malaria before the colonial transfer of cinchona seeds and plants.Footnote 182 MacCulloch himself made tangential references to non-European sites. It has been already suggested how MacCulloch's career as a writer, geologist and lecturer were intimately tied to the East India Company. Such associations could not have left his world view unaffected. Many of his books were published with support from the East India Company. In the nineteenth century, then, writing about malaria in English was never completely dissociated from colonial concerns.
However, mid-century onwards malaria found itself unprecedentedly entangled with colonial lands, landscapes and people. In contemporary texts which commented on malaria, references to the ‘mountainous jungles of India’, ‘impenetrable mangrove forests’ in the West Indies, alluvial plains in Algiers,Footnote 183 ‘natural prairies of French Guiana’, ‘arid deserts of Peru and Spanish Guiana’, Antigua, Barbados, Dominica, Bahamas, Tobago, the Pigeon Islands, Senegal, the coasts of Coromondal, Malabar, the deserts of Arabia,Footnote 184 the coasts of Africa,Footnote 185 ‘vessels en-gaged in the West Indian, South American or African trades’,Footnote 186 winds blowing along the coasts of Ceylon or Sierra Leone or BataviaFootnote 187 featured more regularly than ever before.
Even while promising to comment on malaria in Europe, most texts in the 1850s lost focus and ended up devoting substantial parts towards describing colonised situations. Thomas Wilson, for instance, began by promising to write about malaria which he had observed in Belgium and Holland. However, he devoted significant parts of the book to describing the Ionian Islands, the Ireland Islands in the Bermudas, and lakes and the margins of streams in Upper Canada and the West Coast of Africa.Footnote 188
As in the case of cinchona plants, malaria began to acquire a wider variety of colonial authorities from the 1860s. The decade witnessed the resurgence of a gush of publications about malaria from colonies such as British India. At the same time, the projection of most colonised locations as malarial landscapes acquired overwhelming consistency. Most of these texts were written in the colonial world, and their authors claimed recurrently to have known malaria in its ‘hotbeds’. The germ theories of malaria, for instance, were established by officials working for colonial governments in Formosa, Amoy, parts of Algeria and India in the 1870s. C. F. Oldham's What is Malaria? And Why Is It Most Intense in Hot Climates?,Footnote 189 William Moore's ‘Malaria vs. More Recognisable Causes’Footnote 190 and Joseph Fayrer's ‘Malaria’Footnote 191 were amongst the most significant contributions on malaria in the 1870s and 1880s. It is perhaps not entirely accidental that all these authors had been highly placed colonial officials, serving the British government in India. Revealingly, Oldham's book was dedicated to the then Secretary of State for India, the Duke of Argyll.
From the early 1870s, malaria attracted the attention of medical journals published from British India, such as the Indian Medical Gazette, with remarkable regularity. Distant corners of the British Empire and beyond – Queensland, Northern Australia, Virginia, Bengal,Footnote 192 Massachusetts, Natal,Footnote 193 French Algeria,Footnote 194 Assam, British GuianaFootnote 195 – figured in these articles, as significant spots in an eclectically dispersed and yet intimately connected world of malaria. These articles configured, compared and publicised such locations as abound in malarial situations, which could be rescued precisely through regimes of improvement and circulation of quinine.Footnote 196
These simultaneous invocations of distant place-names, it may be argued, were enabled by intricate overseas colonial, commercial and military networks, which reinforced a spectacular circulation of personnel and texts in the second half of the nineteenth century. Dispersed geographies of malaria resulted from journalistic reports, scholarly articles and memoirs written by diverse groups of mobile men: physicians in charge of ships carrying immigrant labourers from Calcutta to Port Natal;Footnote 197 transferable officials like John Meredith and G. Dodds, who held assignments in places ranging from British Guiana to Assam, from Borneo to Hong Kong;Footnote 198 physicians and soldiers travelling with the British army, who were engaged in British America, the Mediterranean, Ceylon, Australasian colonies, China, Japan, India, West Indies, Western Africa, St Helena, Cape of Good Hope and Mauritius.Footnote 199 These reports were eventually published in widely circulating and extensively cited journals, Annual Medical Reports of the British Army and bureaucratic correspondence. A report, an article or a memoir concerning dispersed colonial frontiers could be read and invoked in distant locations. Thus, by the 1870s malaria aroused the curiosities of an ever-growing variety of publishers, authors and readership spread across the colonial world. There malaria was alleged to acquire forms, extents, ferocities and resilience unthinkable elsewhere.
The persisting imagination of malaria as a flexible diagnostic category was reinforced and extended further in scholarly treatises, books, journal articles, journalistic accounts, bureaucratic reports which were produced in the colonies from the 1870s onwards. In his book on malaria published in 1871, C. F. Oldham, who had been an Assistant Surgeon to Her Majesty's Indian Forces and Surgeon In-charge of the Dalhousie Sanatorium, proposed a distinction between the prevalence of malaria in hot and cold climates.Footnote 200 In cold climates, Oldham suggested, malaria was prevalent in ‘certain situations, specific localities and particular seasons’;Footnote 201 mostly in autumnFootnote 202 and in ‘low and swampy’ areas.Footnote 203 In hot climates, Oldham suggested, malaria knew no bounds, and could reveal itself in diverse landscapes in every part of the ‘habitable globe’ and beyond.Footnote 204
Malaria is found in the swamp and in the sandy desert; in the dense forest and the cultivated plain; on the lofty mountain and in the alluvial delta, scarcely raised above the level of the sea; in the fertile valley and amongst bare, sun-baked, rocks; in an atmosphere saturated with moisture and where the air is so hot and dry that no dew is formed, all vegetation are burnt up.Footnote 205
Most of Oldham's examples of ‘hot climatic conditions’ were derived from colonised or previously colonised locations. Referring to a range of travel writings, Oldham suggested that in Ceylon, Java, the Malayan Archipelago, New Guinea, Gilolo, OrinocoFootnote 206 and at an altitude of 4000 feet and upwards in the Himalayas,Footnote 207 malaria could be most prevalent in the rainy season. In contrast, he showed that in the lower ranges of the Himalayas, the hill ranges or table lands of Southern India or in the ‘oases of the Sahara, as in Algiers’ the effects of malaria were most intense in the ‘hottest and driest seasons’.Footnote 208 Quoting David Livingstone's account on the ‘elevated regions of Central Africa’, Oldham pointed out how malarial fever was found to be prevalent amongst the ‘negroes’ in the ‘middle of winter’.Footnote 209 Unlike MacCulloch, Oldham labelled ‘dry’ locations devoid of any vegetation as potentially malarial situations. He believed that malaria could ‘coexist with barrenness and intense drought’. Oldham thus extended the geography of malaria to include ‘hot and arid’ regions of Venezuela,Footnote 210 desert tracts of Western Rajputana including Marwar, Jaisalmir, Bickaneer,Footnote 211 the flat, dry and sandy military stations at Jacobabad and Mean Meer,Footnote 212 and the sun-baked rocks of Aden,Footnote 213 Gibraltar and the Ionian Islands.Footnote 214 Malaria in the hot colonial climates, according to Oldham, revealed itself indiscriminately across an eclectic variety of seasons, weather, landscapes, altitudes and soil textures.
Malaria, it was argued, could thrive extensively in the colonies independent of vegetation and conditions of wetness. Malaria began being associated with a myriad range of colonial objects. Oldham described friable granite rocks encountered in Hong Kong and Amoy, magnesium limestone in Sindh and ferruginous rocks in Southern India as particularly generative of malaria.Footnote 215 Such suggestions were elaborated further in successive articles published in the Indian Medical Gazette. An anonymous reviewer of Oldham's work acknowledged the prevalence of not one but several malarial poisons: marsh poisons, granite poison, sandstone poison, limestone poison, clay poison and black soil poison.Footnote 216 In July 1874, C. A. Gordon, a Deputy Surgeon General working for the British Indian Government, published an article titled, ‘The Hygiene of Malaria’ in the same journal. He mentioned how malarial fevers could be contracted from inspecting musty hay or consulting old books.Footnote 217 Similarly, James Henry Salisbury associated ‘malarial germs’ with damp and mouldy bed sheets, bedding and clothes tightly packed in trunks, dust that adhered to old books and edible objects like mushrooms.Footnote 218 Malaria was construed as an enigmatic and usually invisible diagnostic category, which could nonetheless be embodied in a variety of forms and objects in the colonies. Malaria not only occupied place-names inscribed on the surface of medical texts, but also allegedly inhabited the depths of colonial landscapes, permeating the spectacular worlds of minerals, rocks, forests, deserts, coasts, winds, vessels, as well as everyday objects.
Salisbury's Macnaughton Prize-winning book, Malaria, was published in 1885 in New York, where he was a practicing physician. It laid the foundation of what was eventually known as ‘the Cryptogrammic origin of malarial fevers’. A reading of his book suggests that writing about malaria in the colonies did not necessarily entail residence in such locations. Nor were such writers always officials in the colonial bureaucracy. Even figures like Salisbury who worked in Cleveland and New York seems to have had access to stories narrated by travelling physicians and officials spread across the colonial world. His book drew upon narratives about Kingston in the West Indies, Nepal, Malwa, Peru, Brabant, New South Wales, the Southern Ocean, Tongataboo, Ovalau, the island of Soloo in the West coast of Africa, lower Egypt, Singapore, Sierra Leone, Batavia and Malacca, Zanzibar, St Lucia, Ceylon, Barbados and Mauritius.Footnote 219
Publishing about malaria in the colonies and in Europe did not necessarily constitute mutually exclusive worlds. The same authors often wrote in journals published in Europe as well as in its colonies. European journals like Edinburgh Medical Journal,Footnote 220 the British Medical JournalFootnote 221 and the LancetFootnote 222 frequently published articles about colonial malaria, as much as journals published from within the colonies. British officials serving the Empire in India often published medical memoirs from London-based firms. A. T. Macgowan, a physician with the British army, for instance, wrote about malaria in Kanpur during the Sepoy Mutiny in 1857. It was published and distributed by the same firm in London.Footnote 223 In 1880, E. G. Russell published an extensive treatise on malaria encountered while on duty in Assam. This book was eventually distributed from London, Madras, Bombay and Calcutta.Footnote 224 It is clear that publishers based in London were committed to circulating narratives about malaria involving different corners of the Empire. Similarly, authors based in the colonies appeared keen to share their insights with an informed home audience. Thus Joseph Fayrer, J. W. Moore and George Dodds, all colonial officials, often read out essays on colonial malaria to the Epidemiological Society of London or the Medico-Chirurgical Society of Edinburgh.Footnote 225
By the 1870s, malaria was projected as an exclusively colonial concern. This converged with attempts to describe locations within Europe as almost free from malaria. Malaria was shown as a contemporary reality for much of the colonial world in the 1870s. In contrast, malaria figured as an attribute of an embarrassing past, which England had left behind. To get rid of malaria, it was suggested, the colonies had to experience a similar set of historical processes. These included regimes of improvement and the circulation of different varieties of cinchonas. Articles published in the English journals from British India tended to associate malaria with known figures and periods in British history. An editorial published in the Indian Medical Gazette in October 1873 claimed that malarial fevers ‘raged like a plague’ during the sixteenth century reformation and during Thomas Sydenham's lifetime, a century later.Footnote 226 In 1876, T. E. Brown, the Principal of the Medical School in Lahore, published an article titled, ‘On the References to Intermittent Fever in Shakespeare’. He noted frequent allusions to the diseases attributed to malaria and expressions like ‘marsh-air on a dewy night’ or ‘bogs and fens’ in the writings of Shakespeare. This he contrasted with the relative absence of such references in contemporary English literature.Footnote 227 He attributed such change to the ‘improvements’ of the drainage network initiated in Elizabethan England.Footnote 228 Such impressions were also conveyed in articles published in England. In 1885, The Medical Times and Gazette of London published an anonymous article titled, ‘The Improvement of Malarious Countries’. It suggested in detail how measures of ‘improvement’ had substantially diminished the effects attributed to malaria all over Italy.
It is noteworthy in connection with the malaria in Rome that only one case of actual perniciosa was admitted into the Santa Spirito hospital during the year 1884; only two during 1883, and that only one case of malarious melanaemia has been available for research there during the past winter showing very clearly the improvement of late years in regard to malaria.Footnote 229
However, the most detailed and overt statement came from Joseph Fayrer in a paper read out to the Epidemiological Society of London. Malaria, he observed:
In the tropics as they are now…have been in Europe in past times. Read Pringle's valuable work, Lind, Ferguson, Macculloch, and others of that time and at a subsequent date; or go back further, and read Lancisi and Sydenham, and you will see that not the coast of Guinea or the Nepal Terai can give you anything much worse than Europe did in those times…Footnote 230
Fayrer added:
Once we were a very suffering people, and lost two kings, a queen, a cardinal, a lord Protector, and many other great people, from a disease that is now almost unknown,…Why this change? It comes of better drainage, better houses, better food, better personal and general hygiene, and therefore it is full of encouragement for other countries; and are we not now profiting by this experience, and gradually diminishing disease everywhere?Footnote 231
Thus malaria figured as one of the cultural tropes which emboldened imperial discourse to argue that the colonies were characterised by a temporal lag. Imperial literature about malaria tended to reconfirm the notion that contemporary British India was a reenactment of historical predicaments which Europe had already encountered and resolved in the past. To that extent, the spectre of malaria empowered imperial ideologies to condemn the colonies to what Dipesh Chakrabarty calls ‘the waiting room of history’.Footnote 232
Such impressions were not always confined to texts written by British authors located in India or elsewhere. English articles written by Bengalis employed in the colonial government's medical service shared similar insights.Footnote 233 Similar claims were also put forward in certain books and journals published in the vernacular. For example in the late nineteenth century, Bengali medical journals like Swasthya and Chikitsa Sammilani began projecting contemporary England as completely free of malaria, while admitting its intense malarial past.Footnote 234
In contrast, in successive editorials the Swasthya described malaria as a relatively recent feature in the history of Bengal, unknown ‘thirty to thirty five years earlier.’Footnote 235 Suburban locations like Burdwan, Katwa or Kalna, which until recently were considered healthy places had over time, they argued, emerged as malarial localities.Footnote 236 Such articles tended to situate malaria within the emerging historical geographies of Bengal. One such article published in Chikitsa Sammilani described the recent decline of urban centres at Gaud, Lakshanabati, Subarnagram, Jessore and Birbhum, and ascribed it to malaria.Footnote 237
Such overlapping conceptions about the shifting geographies of malaria in accounts written in different languages might appear startling.Footnote 238 However, writings in Bengali did not necessarily indicate a radical act of dissent. Nor did they inevitably constitute a counter-discourse to official correspondence. Writing about malaria in Bengali, as I will explore in the epilogue, addressed a different set of audiences and cultural assumptions; pursued dissimilar political purposes, and, adopted a unique set of stylistic approaches and linguistic strategies. Nonetheless, most of these nineteenth-century Bengali authors were part of the colonial bureaucratic and pedagogical network. The editor of the journal Swasthya, Durgadas Ghosh, for instance, had been a colonial Civil Surgeon based in Cooch Behar. Many of the contributors to these journals held medical degrees from the Medical College of Calcutta.Footnote 239 Doyal Krishen Ghosh who was an Assistant Surgeon in Hooghly published one of the very few Bengali books on malaria in the late nineteenth century.Footnote 240
In the same year, 1878, Amritalal Bhattacharya's Jvar Chikitsa (The Treatment of Fevers) was published. It was written as a textbook for Bengali medical students at the Campbell Medical College, one of the very few medical schools set up in nineteenth-century Calcutta, which taught aspiring doctors in the Bengali language. Bhattacharya had been trained at the Medical College in Calcutta. He acknowledged in his preface that his comments on malaria were entirely based on class lectures delivered by one of his professors at the Calcutta Medical College, Dr Smith.Footnote 241 Unsurprisingly then Bengali authors acknowledged MacCulloch as the first author on malaria in English.Footnote 242 Most nineteenth-century Bengali authors about malaria were drawn from amongst those who had been co-opted within the entrenched networks of British colonial bureaucracy. As local custodians of knowledge about malaria, they asserted themselves as ‘medical authorities’ in relation to their intended vernacular audiences. Their limited polemics with European authors were overshadowed by the rather consistently pedagogical stance they adopted towards their potential readers in Bengali.
Malarial Governance: Intervention, Compensation, Circulation
By the mid-nineteenth century, malaria was increasingly embroiled not only with colonial places – landscapes, objects, climates – but also implicated within networks of governance and the global circulation of labour. Malaria, on various occasions, enabled the deeper penetration of the colonial state into the interiors of British India to appear legitimate. In 1856–1857, for instance, the Edinburgh Medical Journal published an article by one J. Bettington, who was engaged in the task of drafting revenue reports in Western India. Bettington recommended certain measures of ‘improvement’ in resisting the effects of malaria in the jungle talooks of the southern Mahratta country. These included the construction of wells in the jungle districts of Dharwar, Belgaum, Kolapoor, Sattara, Puna, Nagur and Candeish and bringing these areas under cultivation.Footnote 243 This, he predicted, would result in a ‘great improvement of the revenue’.Footnote 244 However, he observed that the wells required regular cleaning to remain free from the accumulation of noxious plants, refuse and mud. Effective cleaning, he argued, would necessitate European supervision: ‘Experience proves that neither the people, nor the heads of villages, nor the heads of districts, will trouble themselves about such matters, unless compelled by standing-orders, rigidly enforced under the personal supervision of European officers in their tours through the country’.Footnote 245
Further, the need to identify severely malarial localities provoked state-initiated efforts to measure the size of organs internal to the human body.Footnote 246 The Indian government published a report titled ‘Prevalence of organic disease of the spleen as a test for detecting malarious localities on hot climates’ in 1868, written by T. E. Dempster, a Surgeon of the 1st Brigade Horse Artillery. The object of inquiry was whether irrigation canals in northern India left their immediate vicinities ‘malarious’, by comparing the ‘irrigated’ and ‘unirrigated’ districts on both banks of the river Jumna, from Hardwar to Meerut.Footnote 247 The difficulties of this investigation, Dempster thought, ‘were insurmountable’.Footnote 248 He found the ‘native's account’ of the healthiness of his own town or village, even for a season, ‘the loosest and most vague.’ Nor could he access ‘the medical statistics of several localities under examination’. He lamented the absence of any record of diseases, deaths, births and population to which he could refer. However, he claimed that he compensated for such difficulties by ‘touching the body’Footnote 249 of the inhabitants in the relevant localities. He observed, ‘The native inhabitants of unhealthy districts in India, often carry in their own persons a record of past suffering, which can at all times be easily read, and which no one can falsify or suppress. This is the enlargement of the spleen…’.Footnote 250 The connection between malarial diseases and the size of the spleen, Dempster believed, was close to mathematical precision. About his revelations during the examinations he wrote:
Although the intimate connection between malarious fevers and organic disease of the spleen is established beyond doubt, it never was supposed that these diseases bear an exact proportion to each other, or that the number of enlarged spleens in any particular situation should correspond precisely with the number of attacks of fever suffered by its inhabitants.Footnote 251
At each place, Dempster and his colleagues selected 20 children and 20 adult males. These included members of ‘all castes’ and a group of agricultural labourers.Footnote 252 They classified five different degrees of size of spleen in every locality. Based on such classifications they identified some localities as more malarial than others.Footnote 253 Dempster mentioned that enlargement of the spleen seldom carried any form of visible external manifestation. He described enlargement of the spleen as the ‘least formidable of all organic diseases of the viscera…it may consist with every outward appearance of health and vigour…strikingly healthy looking men and children were found with decided enlargement of the spleen’.Footnote 254 The subjects were selected, Demspter wrote, not from amongst the sick, but the ‘going about population of the town or village under inspection.’ In the absence of any external manifestations, the detection of an enlarged spleen or the identification of a malarial locality became almost entirely the examining physician's prerogative. ‘No case was ever registered as “spleen”, unless I had so distinctly felt the enlarged organ…’.Footnote 255 The suspicion of malaria thus empowered the administrative apparatus of the state to intervene into the depths of colonised bodies.
The identification of interior localities within British India as malarial brought its obvious benefits for the colonial state: Malaria legitimised various degrees of government intervention, reinforced the relevance of myriad projects of agricultural improvement, enabling in turn the unhindered functioning of the revenue machinery. At the same time, protecting the ‘native subjects’ as well as officials from malaria in such localities began to be considered as amongst the responsibilities of the colonial governments. By the 1870s, officials posted in ‘isolated stations in malarious districts’ began to demand diverse forms of monetary compensation from the government.Footnote 256 The fear that the effects of malaria were most harmful close to the soil inspired particular forms of architecture in the colonial frontiers by the 1860s.Footnote 257 In the 1940s, the living quarters of managers of tea plantations in Assam, for example, continued to be raised substantially above the ground to provide security to the vulnerable residents from the collective threats of wild animals and malaria.Footnote 258 These were presumably inspired by existing practices in other parts of the world where tabernacles were raised for the shared purpose ‘to avoid malaria and for watching against robbers who rob the crops’.Footnote 259
Malaria featured in narratives of circulation of migrant labour from one British colony to another. This is revealed in the various ways in which the Mauritius fever – an epidemic attributed predominantly to malaria in that colony in late 1860s – was reported. In a mammoth report drafted for the Sanitary Commission of Mauritius, Charles Meldrum explained Mauritius fever in terms of the excessive immigration of ‘coolies’ from India. Immigrants from British India were considered crucial to the economy of Mauritius. They were employed as cheap labourers in the sugar estates, as domestic servants, gardeners, hawkers, carriers and grazers.Footnote 260 Meldrum claimed that from 1834 to 1865, the population of Indian immigrants had increased from 84 to 245700. This increase, he pointed out, corresponded with the greater prevalence of malarial fever in the island. Fifty-six vessels had carried 20283 Indian coolies into Mauritius from Calcutta, Madras and Bombay in 1865 alone.Footnote 261 Meldrum quoted one Dr Reid, who claimed to observe the ‘notorious proclivity of the Indian race to febrile disease, and the special tendency brought from their own land of many of them to malarious fever’.Footnote 262 Earlier reports written by government officials in Mauritius also cited immigration of labourers from British India as a cause of Mauritius fever. Health officers based in Port Louis frequently suggested that the ‘coolies’ brought their propensity towards malaria from home. Such propensities were nurtured and further intensified in the ‘dangerously overcrowded depots’ in the ports at Bombay, Madras and Calcutta.Footnote 263 The ‘coolies’ were each allowed a space of 24 superficial feet in the depots. It resulted in overcrowded conditions in the depots. These conditions, it was suggested, continued during the voyage. Thus, malarial fever was carried into the island along with the immigration of labourers from India. Such impressions were even shared by higher officials representing the British Indian government. In 1864, for example, Dr Leith, the Secretary to the Government of India wrote to the Secretary of State recommending the extension of the minimum space allocated for each labourer in the depots from 24 to 54 superficial feet.Footnote 264
Such recommendations met with stiff resistance from the Colonial Office, the Emigration Board and the War Office Sanitary Commission. Officials representing the Emigration Board did not consider the recommendation economically viable.
I feel bound, in the interest of the West Indian Colonies and Mauritius, to submit that no sufficient grounds have been shown for requiring them to provide depot accommodation to an extent that would necessarily add largely to the cost of emigration, and might eventually make it too expensive to be continued.Footnote 265
Officials within the Emigration Board tried to argue that the allocated space for emigrant labourers was sufficient. Prisoners in British India were each allocated a space of 36 superficial feet, while the ‘native servants in military cantonments’ were offered a minimum space of 50 feet. The emigrant ‘coolies’ were thus allowed a space, which was much more constricted in comparison to ‘servants and prisoners’ in India. However, such discrepancy was defended on behalf of the Emigration board.
In one case…occupation is more or less permanent, and in the other it lasts only a few days…when a migration depot is not full the people have the advantage of the unoccupied space. They are unrestricted in their movements during the day and night…An Indian prisoner, on the other hand, although he may have 36 superficial feet of superficial space, yet from necessary condition of security is less favourably placed.Footnote 266
Officials in the Emigration board suggested that the minimum superficial spaces allocated for the emigrant Indian labourers in the depots in Bombay, Calcutta or Madras were in parity with related provisions in other contexts. For instance, the London common lodging houses apparently allowed a minimum space of 33 superficial feet by 6.5 feet in height, or 115.5 cubic feet. The Imperial Passenger's Act required on board-ship allowance of 15 superficial feet by 6 in height or 90 cubic feet per adult. British depots in Plymouth and Birkenhead allowed about 222 cubic feet per adult. The Indian Emigration Act of 1864 made provisions on board-ship of only 10 superficial feet by 5.5 feet in height, or 55 cubic feet per adult, while West Indian Emigration made 12 superficial feet mandatory. These figures were elaborately quoted in correspondence between different members of the Emigration board. Emigrant coolies leaving Indian ports for Mauritius were allocated a minimum space of 24 feet by 12 in height or 288 cubic feet. Officials representing the Emigration board argued that it was not only sufficient, but also ‘more than five times the minimum cubic allowance on board-ship’. Such allocations of space for Indian coolies bound for Mauritius was not only projected as sufficient, but also desirable. Writing to a colleague in the Emigration board, S. Walcott referred to one Dr Pearse. He described Pearse as one of the ‘most experienced and able medical officers’, a veteran of twelve voyages to Australia in medical charge of emigrants, and six voyages with upwards of 2570 ‘coolies’ from India to the West Indies. In a letter written to Walcott, Pearse argued that ‘the warmer and closer (within reason) the coolies lie at night the better for them’.Footnote 267
Officials representing the War Office Sanitary Commission and the Emigration Board differed from the health officers at Port Louis and certain senior bureaucrats serving the government of India. They suggested that Mauritius fever and conditions of accommodation for the labourers in the depots were unrelated. Instead, they argued that the fever could be attributed to local malarial situations within Mauritius itself.Footnote 268
Correspondence about Mauritius fever reveals how a malarial event could be explained in terms of both local circumstances as well as mobile and portable agents. A particular event associated with malaria could be analysed differently by diverse sets of officials. Thus the aetiology of a malarial epidemic both sustained and was produced by questions of race, class and labour, and the exigencies of colonial economy. The epidemic further occasioned fault-lines and tensions between different colonial governments within the British Empire to be exposed, when Mauritian and Indian bureaucrats blamed one another for the event.
Regions and Races
Malaria was not just ascribed to local circumstances or circulating labourers. Widely dispersed locations across the extensive colonial world were believed to share myriad malarial situations. In contemporary bureaucratic correspondence or scientific writings, such locations converged to constitute overlapping geographical ‘regions’. These regions stood for both geopolitical zones and disease ecologies. Distant constituents within such regions, it was claimed, shared propensities towards similar diseases. Thomas Barker in 1859 described how ‘regions of disease corresponded with seasons and zones of climate’. He divided ‘the surface of the globe’ into three ‘belts or zones’. Malarial diseases appeared most intense and concentrated in what he called ‘the torrid zone or belt’.Footnote 269 Within the ‘torrid zone’, Barker identified the Gulf of Mexico, the West India islands, the northern portion of South America, India, Borneo, Ceylon, the Gulf of Guinea, Madagascar and Mozambique as ‘the principal centres’ of such diseases.Footnote 270 Barker appeared less certain about the ‘perpendicular distribution’ of malarial diseases. However, he observed that in Mexico they were prevalent at an elevation of 7000 or 8000 feet; and in South Eastern Asia they ceased at an elevation of 6000 or 7000 feet above the sea level. Barker proposed a connected and shared natural history of diseases which recurred across the torrid zone when he argued that the manifestation of malarial diseases at one location could indicate the beginnings of similar outbreaks in distant locations.
The same morbid appearances are reproduced with the utmost constancy and regularity in a thousand places at once, wherever the same causes of insalubrities are met with, only they are more intense, continuous and prolonged in some places than in others…Similarity of geological formation indicates a similarity in the diseases of a country, as seen in the localities visited by malarial fevers.Footnote 271
Such insights found reflection in Meldrum's collection of reports describing the causes of the Mauritius fever. The malarial epidemic was attributed to meteorological conditions, which were not peculiar to the island, including absence of floods, prevalence of intense periods of drought and fluctuations in rainfall. The period from 1864–1868, it was reported, was characterised by a ‘remarkable absence of hurricanes’ all over the Indian Ocean region. Meteorological conditions witnessed in Mauritius were also prevalent ‘in other places bordering on the Indian Ocean’. Potentially malarial situations, it was suggested, could be almost simultaneously witnessed in places as far as Mauritius, Rodrigues, India, South Africa and the Australian colonies.Footnote 272 Such regions did not only share with Mauritius the ‘abnormal weather’ supposedly prevalent in the island between 1864 and 1868, but also experienced like Mauritius remarkable death rates.Footnote 273 These reports suggested that during this period conditions of ill health were not confined to islands bordering on the Indian Ocean region, but extended to ‘considerable portions of the globe’ including Malta, Gibraltar, the West Indies and certain parts of Southern Europe.Footnote 274 Such extensive manifestation of malarial diseases, it was conjectured, could be attributed to periodic mutations on the solar surface, which simultaneously affected meteorological and demographic conditions in different parts of the world.Footnote 275 Mauritius fever, it was suggested, could hardly then be described as a ‘local’ event.
By the mid-nineteenth century, composite geographical categories designated collectively as regions were thus constituted of distant and diverse forms of landscapes. The literature about malaria drew upon and consolidated contemporary regional formations. Malaria was consistently associated with some amongst these overlapping regional categories, including, as I have noted, ‘torrid zones’, ‘hot climates’ and ‘Indian Ocean region’. The tropics constituted another such category.Footnote 276 George Dodds, a British doctor who held various official assignments in Asia, read out a paper entitled, ‘Tropical Malaria and its Sequels’ to the Medico-Chirurgical Society of Edinburgh on 4 April 1888.Footnote 277 Dodds’ description of tropical malaria echoed Oldham's comments about malaria in hot climates. In the tropics, Dodds argued, malaria was most intense and omnipresent, and could acquire vigorous and various forms.
It has the power of drifting along from its source for a considerable distance, and to be able to roll up the sides of mountains and along ravines, and yet can be stopped by a high hedge, a grove of trees or even by a mosquito curtain. It prefers low levels and yet can be found also on the tops of mountains. It coexists with vegetation, and is found in arid wastes, utterly devoid of any vegetable growth.Footnote 278
Malaria was tied intimately to notions of race as much as conceptions of region. Malaria sustained the perceived correlations between composite geographical categories and racialised collectives of humans. Writers on malaria such as Dodds began by commenting on the vulnerability of Europeans in the tropics. He described malaria as more or less confined to the tropics, and in so doing proposed a radical shift from the geography of malaria conceived by MacCulloch half a century earlier. He considered Europe as almost free from malaria. Most malarial patients in Europe, Dodds thought, were those who had returned from Europe's various ‘tropical and subtropical possessions’. Most of them appeared to carry ‘malarial taints’ in their bodies. Thus, malaria in Europe, Dodds argued, was a predominantly ‘Anglo-Indian’ disease.
As long as the European lives within the tropics…that asthenic condition inevitably overtakes every European or at least every Anglo Saxon…He never gets acclimatized, and is as liable to sunstroke after a residence of a dozen years as he was during the first week of arrival. Almost everyone who has resided in the East has imbibed the malarial poison…Footnote 279
Colonialism necessitated, it was argued, the uncontrolled exposure of Europeans to myriad malarial situations in the tropics. The vulnerability of Europeans to malaria, according to authors like Thomas Wilson, was an effect of Europe's many imperial ventures in the nineteenth century. Wilson compared nineteenth-century European empires with ancient Rome, which had also ruled over ‘many nations and races’. However, ‘they met with no race with whom the Romans could not freely amalgamate’.Footnote 280 Malaria, argued Wilson, was thus unknown in ancient Rome. Unlike the ancient Roman Empire, nineteenth-century European colonialism involved ‘the attempt to occupy by a white race a tropical country, and a land inhabited by coloured men’.
The problems presented by the modern history of a European race attempting to hold India by the sword, to colonise the American world from the Polar sea to the Land of Fire, to inhabit if not to cultivate, the insalubrious Antilles, the banks of the Orinoco, or of the still more dreadful Senegal, Gambia and Niger, nowhere occur in Roman or Grecian history…Footnote 281
…However distant these lands lie, their malarious condition has an influence over the European family of nations, an influence…though originating in the obscure and unknown East, has shown itself at times at Rome and Moscow, London and Paris…Footnote 282
Such exposure to the landscape, climate and people in tropical India, Africa and America, Wilson feared, would eventually result in the extinction of the European race. Behind this fear lay an implicit emphasis on the superiority of the ‘European race’. European bodies were projected as sophisticated, tender and delicate. In hostile and rough tropical situations, the exalted forms of European life, it was apprehended, could undergo decay and degeneration. ‘Extinction seems the sure result of all their efforts, whether they unite with the native races or not. If they unite, their purer blood soon disappears in the stream of a darker population; if they spurn the union…malaria speedily exterminates their race and name’.Footnote 283
Nineteenth-century English scientific literature rarely referred to the colour of malaria, but stray references indicate how malaria was associated with different colours in the course of the century. MacCulloch did not refer to the colour of malaria. He however suggested that malarial patients in Europe turned flabby and acquired yellow stains on the body.Footnote 284 From the mid-nineteenth century, malaria was increasingly projected as brown or black in various sources. For instance, Justin von Liebig described water-bearing taints of malarial putrefaction as brown.Footnote 285 An anonymous editorial published in the Indian Medical Gazette in 1873 referred to marshy water in the vicinities of Melbourne as ‘brown as brandy’.Footnote 286 In the late 1880s, Dodds claimed that Europeans, who lived long in ‘malarious districts’ acquired ‘anaemia with brownish tint of skin’.Footnote 287 E. A. Parkes, Professor of Hygiene in the Army Medical School at Netley, published an article in the Annual Report of the Medical Department of the British Army in 1868. He referred to one Dr Massey, who was employed by the Army Medical Department in Jaffna, and claimed to have tracked the colours of ‘particles of malaria’. ‘Massey observed…the well known power trees exert in stopping the transit of malarial particles. He found the leaves of these trees greatly affected with black rust’.Footnote 288 By the mid-nineteenth century, malaria had emerged as predominantly a colonial concern. It is suggestive that by then malaria began to be associated more with brown and black than any other colour.
Figure 2.6 indicates that discussions about European vulnerability in the tropics coexisted with assertions of the immunity of the colonised ‘primitives’ from the effects of malaria. The ‘tribes in the Terai and other forest districts of India’, the ‘negroes in some parts of the coast of Guinea’Footnote 289 and ‘the deadly regions of Central America’, the ‘aborigines’ inhabiting the ‘virgin forests’ of Java, the Malaya Peninsula, and ancient Mexico, were considered immune from the effects of malaria.Footnote 290 Various explanations were offered to explain such examples of ‘racial immunity’ from malaria, such as the colour and texture of the skin. Thus wrote Oldham in 1871, ‘One of the obvious peculiarities of the negro as compared with the European is his thick, oily, skin, rank to a degree…it is possible that the skin of the Negro does, from its thickness and oiliness, help to protect him from malarious disease’.Footnote 291 In the last quarter of the nineteenth century, such racial immunity from malaria was also explained by invoking the theory of natural selection.Footnote 292 Groups of people, who had inhabited tropical and therefore malarial regions from ‘remote ages’, it was suggested, tended to acquire ‘collective acclimatisation’. In such regions, malaria, it was claimed, swept away from each generation individuals whose specific resistance was the feeblest; it spared only those who could offer strongest resistance. This, over generations, paved the way for a ‘collective specific resistance in a race’.
Figure 2.6 © British Library Board. ‘Group of Nepalese: fishermen, etc.’
Such perceived immunity amongst those who were collectively mentioned in various imperial narratives as primitives was attributed to their crude and uncivilised physical constitutions. Their compatibility with malaria was cited as corroboration of anthropological accounts, which described them as less-than-humans, whose unsophisticated existence resembled animals more than any form of human culture. They were referred to as primitives because it was suspected that they continued to be caught up in a ‘state of nature’. ‘Men in a state of nature’, Thomas Wilson thought, ‘seem to resist malaria’.Footnote 293 An anonymous article published in the Medical Times and Gazette London in May 1885 argued that such resistance could be observed amongst the ‘savage men’, ‘the negro race’ and the ‘lower animals’.Footnote 294 A few decades later a senior medical bureaucrat in the British Indian government reflected similar prejudice when he wrote that malarial parasites were ‘as natural amongst primitive races as flea infestation is to a dog’.Footnote 295
Nonetheless, the so-called primitives were recommended subjection to colonial regimes of improvement and doses of quinine broadly for two reasons. It was suspected that although the ‘primitive races’ withstood malaria themselves having imbibed it across generations, they could infect the non-immune communities.Footnote 296 Commenting on colonial northern Australia at a later period Warwick Anderson has shown how the non-white population were projected in scientific texts as ‘“natural” careers of dangerous tropical pathogens’.Footnote 297 Moreover, such absolute immunity from malaria, nineteenth-century authors lamented, could hardly be witnessed any more. Exposure to European notions of civilisation and domesticity seemed to contaminate the pristine ‘state of nature’ inhabited by the ‘aborigines’ and the ‘natives’.Footnote 298 It was argued, for instance, that the advent of specific remedies preserved the ‘weakly resistant’, and acted against the ‘benefits’ offered by ‘natural selection’. It resulted in ‘marked deterioration of race in malarious countries’.Footnote 299 The ‘natives of Newfoundland and Canada’Footnote 300 and ‘dark races’Footnote 301 including the ‘negroes in Africa’,Footnote 302 the Coles, Gonds and other ‘tribes’ inhabiting the jungle-regions in India,Footnote 303 ‘the non-Aryan races of Assam’Footnote 304 began featuring in various reports as victims of malaria.
Thus, immunity of the so-called primitives from malaria in tropical locations could no longer be described as absolute. They began to appear as relatively more immune to malaria only when compared to the greater vulnerability of the Europeans. However, the propensity of such ‘races’ to malaria manifested itself whenever they were made to travel from one region to another. Immunity acquired by these ‘primitives’ was projected as not only relative, but also contextual.
In the moist and sultry climate of the West Indies, the negro thrives…more deadly the climate to the white race, the better does it suit the negro. Transferred to a cooler climate, however, the African loses his advantage over the white man; the liability to malarious disease become equalized and something more…the negro after a lengthened residence in a cooler climate, becomes more susceptible to the diseases of the tropics. The Negroes, who went out from England with the Niger expedition, suffered much less from fevers than the white men, but very much more than their countrymen who had never left the coast…Footnote 305
Such impressions found wider currency from the 1870s, and were reflected in a range of sources. George M. Sternberg, an influential physician employed in the US army, for instance, wrote in 1884, ‘Negroes born in Africa are much less susceptible to malaria than are their descendants born in more temperate and cooler climates’.Footnote 306
Thus, by the mid-1870s, ‘primitives’ were incorporated amongst the potential victims of malaria. Oldham suggested in 1871: ‘No race has yet been discovered, which is proof against malarious disease; though all do not suffer alike in the same climate’,Footnote 307 Individuals belonging to every race, such statements suggested, were likely to benefit from regimes of improvement and the consumption of quinine. Such suggestions were revealing because, as I will show, the 1870s also witnessed the beginnings of attempts to define, manufacture and circulate pure quinine as an item of mass consumption in various British and Dutch colonies. Besides, with emphasis on British India in general and Bengal in particular, I will point out in what follows, how the intimate histories of malaria and quinine played out not only in the policies of the imperial state, but also in the vernacular markets in land, print and drugs.
Conclusion
In the half-century following 1827, when John MacCulloch's book about malaria was published, the category attracted the attention of various layers of commentators. The intellectual history of nineteenth-century malaria presents the curious case of a medical problem, which was addressed and shaped by, apart from medics, a range of geologists, chemists, meteorologists, natural historians, sanitary officials and colonial administrators. At the same time, writers about malaria, as I have suggested, were not only drawn from the Europeans. By the 1870s, for example, Bengalis employed in various capacities in the colonial bureaucracy had begun authoring articles and books on malaria in English as well as Bengali. It has been noted in existing histories that subordination and authority are relational and subjective positions.Footnote 308 In relation to their intended vernacular audience, writers of Bengali texts on malaria commanded a position of authority, even when they claimed to derive information from English textbooks. Their pedagogical tone was restricted within their spheres of ambition and influence set by the Bengali print market.
In contrast, Bengali writers in English found themselves at the bottom of the hierarchy of authors on malaria, pleading often with superior officials in the colonial bureaucracy or with European writers for their share of recognition. Gopaul Chandra Roy, for example, was the author of the most extensively cited English book on malaria written by a Bengali in the nineteenth century. Articles published by him later in his life vented his desperation for recognition and patronage from European authorities and the state.Footnote 309 Such examples can be multiplied. In June 1882, the Indian Medical Gazette published a review of J. W. Moore's ‘Malaria vs. Recognisable Climatic Influences’, written by one K. D. Ghose, a Bengali trained in one of the medical colleges set up by the colonial government. Ghose began his article by proposing the following apology: ‘Ten years residence and active practice in the most notoriously malarious district (Rungpore) in malarious Bengal is the only apology for coming out of this place of obscurity to take arms against such an authority as Dr Moore…My hand trembles, when I hold my pen against the voice of one whose authority is well recognised…’.Footnote 310 These authors projected themselves as marginal medical men who were deferential to their superiors in the world of knowledge about malaria. Thus, wrote a Hospital Assistant from Barishal in a letter to the editor of the Indian Medical Gazette in the same year: ‘The Hospital Assistants have very limited knowledge either of book or practice…they only follow the steps of higher medical authorities…I being a man of same rank and position crave permission to state faithfully about my practical experience…I feel shame for my inability to produce a paper…’.Footnote 311
Thus, malaria revealed various layers of authorities in the nineteenth century. Accordingly, many conceptions about the causes and cures of malarial diseases coexisted. By the third quarter of the century, for instance, an extensive range of plants was associated with malaria. These either figured as generative of malaria or were believed to neutralise its effects. In an article titled ‘The Hygiene of Malaria’ published in July 1874, Surgeon General C. A. Gordon summarised a catalogue of such plants. He mentioned the papaw in East Africa, the Manchineel tree of the West Indies, certain species of the Rhus encountered in America and China, and mangrove, tamarind, neem, oleander and narcissus as plants generative of malaria. Gordon included the sunflower, the eucalyptus, Pistia Stratiotes, ‘several species of the natural order Myrtaceae’ amongst plants with prophylactic influence. These plants, Gordon observed, were being planted in the Gold Coast, in Cuba, Algeria, Australian Colonies, in Corsica, Jamaica and India to stave off malaria.Footnote 312
However, the relationships between various extracts of cinchona barks and malarial diseases appear to have been most invariable, consistent and enduring in course of the century. In significant ways, as this book is in the process of highlighting, cinchona plants and their extracts could engender crucial transformations in the history of the diagnostic category, malaria. Although English writings on malaria did not begin in the 1820s, the discovery of quinine stoked an unprecedented gush of publications about malaria by the end of the decade. Besides, by the middle of the century, the cinchonas ceased to be confined within South American ‘natural forests’ and networks of circulation in Europe. Thousands of such plants and seeds were transported to the emerging colonial plantations in Dutch Java, French Algeria and British India. This coincided with a shift in the geographies of malaria: from a predominantly European disease to an almost exclusively colonial concern.
MacCulloch's comments and examples were predominantly associated with European locations, landscapes, beauty, grandeur and richness. Malaria, thought MacCulloch, was ‘death knocking at the door of the opulent to spare the mean’.Footnote 313 His book was not initially intended for a colonial audience. However, in the decades that followed, it was received and reviewed extensively in colonial locations. By the mid-nineteenth century, malaria was defined in terms of colonial poverty, hunger, filth, insanitation, overpopulation and overcrowded ways of living. In the second half of the century, malaria was projected as almost exclusively associated with hot climates, tropical regions, torrid zones and the Indian Ocean belt. Such recurrent categories coalesced in a range of sources and almost revealed the map of European empires. The colonies, it was suggested, could be rescued only through intense regimes of improvement and extensive distribution of quinine.
Nonetheless, malaria did not absolutely disappear as a governmental concern within Europe.Footnote 314 Medical statistics, however, revealed sharply declining figures for malarial patients and victims within European states like Italy in the 1880s.Footnote 315 This could be sharply contrasted with statistics available for colonial locations like Bengal in the same decade. Quoting official annual mortality figures for Bengal between 1883 and 1887, the Bengali journal Swasthya (Health) suggested that 5,067,205 persons apparently died of diseases attributed to malaria within those five years.Footnote 316 In the next chapter, I will examine the production of a specific malarial locality in the British Empire, and reveal how knowledge about a particular locality and an epidemic were simultaneously put together.
In this chapter I have hinted at how histories of nineteenth-century malaria can variously expose relationships between objects and imperial formations. First, malaria itself was an object of knowledge and governance re-inscribed by the exigencies and apparatuses of imperial rule. Malaria found itself intimately entangled in imperial conversations about colonial capital, migrant labour, cultures of intervention and compensation, and questions of race, regions, class and improvement. At the same time, malaria, in turn, consolidated Empire by reinforcing connections between a network of distant places, materials, professions and processes. Finally, in the imperial texts malaria was believed to personify in decaying vegetation, friable granite rocks, water casks, mouldy bed sheets, stale mushrooms, dusty old books, refuse of indigo factories and groups of humans pejoratively described as colonised tribes, aborigines, negroes and primitives. Although described as immune from the effects of malaria, these objects and groups of humans were perceived to signify and circulate malaria. Thus imperial embodiments of malaria transgressed the boundaries between humans and nonhumans; subjects and objects. Distinctions between wild animals and native robbers, primitives and parasites, lower animals and negroes were systematically blurred in the imperial narratives about malaria.







 Open access
Open access