

Some display a marked degree of dullness or stupor; others sharpness and cunning more allied to the tricks of monkeys than the acts of reasonable men.Footnote 1
When John Campbell published his reminiscences of thirty years’ experience as a prison medical officer in 1884, his comments on the traits of prisoners, quoted here, encapsulated the change in attitude towards prisoners that dominated penal policy in the late nineteenth century. Prisoners, once perceived as redeemable, were now regarded as unreformable, incorrigible, and of poor mental and physical stock. From the late 1850s onwards, fuelled by accusations that prisons were not deterring repeat offenders and that crime was increasing and becoming more brutal, British and Irish legislatures and publics expressed increased disquiet about the effectiveness of their prison systems. The flagship convict prisons, Mountjoy and Pentonville, lost their ‘model status’, and their significance as emblems of rehabilitation diminished, while the aims of spiritual reformists were dismissed as naïve and ineffectual.Footnote 2 Prison policy shifted away from disciplinary regimes emphasising reform towards the rigorous enforcement of expressly punitive regimes, including the separate system of confinement. This involved all prison officers, but placed prison medical officers in a particularly challenging position. As they strove to recreate themselves as experts in prison medicine and to enhance their professional status, they were also implicated in imposing new and severe systems of discipline, which proved detrimental to the physical and mental health of many prisoners, and ‘debasing to the mental faculties’.Footnote 3
The hardening of attitudes towards prisoners was evident in two influential commissions of inquiry into convict and local prison systems. The 1863 Royal Commission established to Enquire into the Operation of Transportation and Penal Servitude in Convict Prisons in Britain and Ireland and the 1863 House of Lords Select Committee on Prison Discipline in England (Lord Carnarvon’s Committee) collated detailed evidence from prison governors, medical officers, chaplains and inspectors, and made wide-reaching recommendations for changes in penal policy. The Carnarvon Committee was particularly important; its recommendations shaped legislation, including the 1865 English Prison Act, while the outlook of the witnesses exemplified the tone of late nineteenth-century penal policy and the direction of subsequent legislation. Under new rules introduced from the 1860s onwards, separate confinement remained intrinsic to the English prison system, but became more penal with greater emphasis on the uniform enforcement of hard labour and strict adherence to meagre dietary scales.Footnote 4 To incentivise good behaviour, a version of the mark or ‘stage’ system, which had been a feature of convict prison discipline in Ireland from the 1850s, was introduced to English convict and local prisons allowing for ‘the possibility of [prisoners’] promotion to a less arduous stage by obedience and docility’.Footnote 5 Following the death of Joshua Jebb, Chairman of the Directorate of Convict Prisons, in 1863, Sir Walter Crofton, former Director of the Irish Convict Prisons (1854–62), worked with the Home Office on the 1865 Prison Act, developing a version of the progressive system for English prisons.Footnote 6 There was support for a similarly punitive penal policy in Ireland, although it was not always implemented in the form of legislative changes. The 1865 English Prison Act, for example, was not extended to Irish local prisons. However, from the 1860s, a shift towards a more penal approach characterised the work of the Inspectors General of Prisons, Dr John Lentaigne and J. Corry Connellan, and their successors.Footnote 7
Alarming statistics on recidivism fuelled the growing dissatisfaction with reformist penal policy and advocates of rehabilitation. Increasingly, prison administrators became preoccupied with halting the growth of the prison population and deterring reoffending.Footnote 8 The Habitual Criminals Acts of 1869, shaped by Crofton, introduced harsher sentencing for repeat offenders and extended police supervision of released prisoners in England and Ireland.
There was also a push from senior government and prison officials, notably Sir Edmund Du Cane, Chairman of the Directorate of Convict Prisons, and Crofton, for greater levels of centralisation and uniformity in implementing penal policy and regulations, and this underpinned the reconfiguration of administrative structures and the drive for nationalisation.Footnote 9 The 1877 Prison Acts centralised the English and Irish prison systems, further eroding the autonomy of local bodies, including the Justices of the Peace and Grand Juries responsible for managing local prisons.Footnote 10 In England nationalisation resulted in the establishment of the Prison Commission under Du Cane. Holding the post of chair until 1895, his term was associated with the implementation of strict prison policies and harsh prison conditions, an approach extensively criticised during Gladstone’s 1895 Departmental Committee on Prisons. In Ireland, the 1877 Act created the General Prisons Board, initially chaired by Crofton, who was succeeded in October 1878 by Charles F. Bourke, one of two Inspectors General of Prisons. Bourke’s brother, Richard Southwell Bourke (Lord Naas), was Chief Secretary for Ireland from July 1866 to September 1868, and an influential voice in shaping penal policy.Footnote 11 Among other aims, nationalisation was intended to rationalise prison estates and produce significant economies, and soon after its introduction, several local prisons were closed and staff dispensed with.Footnote 12
Increasingly prison medical officers became more fully occupied in providing medical attention to prisoners and more directly involved in imposing prison discipline. Prison rules outlining the roles of prison surgeons, developed in the late eighteenth and early nineteenth centuries, were tightened in the 1860s and 1870s, as legislation and prison regulations expanded the duties and responsibilities of prison medical officers. As discussed in Chapter 2, the first sets of regulations charged doctors with regularly visiting prisoners and convicts, especially those placed in separate confinement, to watch out for the adverse effects of the regime. The 1865 English Prison Act, directives from the Home Office and the Chief Secretary’s Office, and published rules and regulations for individual prisons, required doctors to attend prisons at least twice a week and to examine each prisoner during these visits.Footnote 13 At Mountjoy Convict Prison, a single full-time resident medical officer, Dr James W. Young, was appointed in 1867 to replace two non-resident medical officers, the high-profile Dr Robert McDonnell at the main prison and Dr Awly Banon at Mountjoy Female Prison.Footnote 14 The status of some appointees became more prestigious. Dr David Nicolson, who worked as Medical Officer at Woking, Portland, Millbank and Portsmouth Prisons before moving to Broadmoor Criminal Lunatic Asylum in 1876, became a leading authority on prison medicine and criminal psychology.Footnote 15 Although there was no direct equivalent to Nicolson in Ireland in terms of his professional profile, after his departure from Mountjoy, McDonnell served on the 1884 Royal Commission on Prisons in Ireland, while Dr Hercules MacDonnell, Medical Officer at Dundalk Prison, published on penal policy and, as discussed below, was a vocal critic of the 1877 General Prisons (Ireland) Act.
More generally, by the second half of the century, prison medical officers were emerging as a discrete professional group, notably in convict prisons, where ‘they had common professional interests, served a common authority, participated in a recognizable career structure, and evolved for themselves a distinct professional ethos’.Footnote 16 Many, like John Campbell and Robert McDonnell, had transferred to prison service following careers in the army and navy, but increasing numbers devoted their entire professional careers, particularly in the convict service, to prison medicine.Footnote 17 In line with an increased emphasis in dealing with mental disorder as an aspect of their workload, a small number moved between employment in criminal lunatic or public asylums and prisons. A prison appointment provided a reliable salary and in some cases accommodation, for some in the locales where they had been raised.Footnote 18 Dr William Ralph Milner, the son of a local surgeon, who qualified in 1838, was employed as apothecary to Wakefield Dispensary before being appointed resident surgeon to the convict department of Wakefield Prison in 1847 at a salary of £200.Footnote 19 The surgeons and doctors employed by local prisons in Ireland had typically served as town dispensary doctors; in 1852 the physician to County Donegal Gaol, Dr Robert Little, had been employed as doctor to the Letterkenny Dispensary, while Dr Thomas Dillon, the magistrate for County Mayo, was the physician for the County Gaol, surgeon to the County Infirmary and former surgeon to Westport Dispensary.Footnote 20
The career of Dr William Augustus Guy, an authority on prison medicine and prison diet, has been summarised in detail by Anne Hardy, who explains that, unlike many of his contemporaries, he came to the prison service with a set of deeply embedded views and principles. He was an established sanitarian, who had served as Professor of Forensic Medicine and then Dean at King’s College London, before taking up the post of Superintending Medical Officer at Millbank Prison between 1859 and 1865.Footnote 21 Guy was responsible for introducing a new dietary to English prisons in 1864, directed at reducing food allowances, and held ‘unyielding views on the discipline required to achieve social justice’, forged by his loathing of idleness and waste.Footnote 22 According to Hardy, the contrast with Dr Robert Gover, who succeeded Guy at Millbank and served as Medical Inspector of Local Prisons and Superintending Medical Officer of Convict Prisons after 1877, was stark.Footnote 23 Commencing as assistant surgeon at Portsmouth in 1857, and then resident surgeon under Guy at Millbank, Gover spent his entire career in the prison service, and was noted for his pragmatic and humane approach.Footnote 24 According to ex-convict Henry Harcourt, who provided detailed evidence to the 1878 Penal Servitude Commission, including details of prison medical officers’ cruelties, ‘a more humane and better man does not exist than Dr Gover’.Footnote 25 Nonetheless, Gover advocated the use of the treadwheel, not least as a guard against shirking, and was vigorous, as shown in Chapter 5, in his efforts to root out the feigning of mental disorder. Dr Patrick O’Keefe, Medical Officer at Spike Island and Mountjoy Convict Prisons from the 1870s, was less popular among prisoners. Prior to his appointment, Inspector Murray had expressed a preference for ‘an Irishman, and one if possible who has had some experience in the practical working of a Poor Law rural district’.Footnote 26 Citing the positive results derived from the employment of Dr James Young, Resident Medical Officer at the Mountjoy Convict Prison, Murray cautioned against a ‘naval or military practitioner’.
These gentlemen … rarely if ever possess that faculty of individualization which should distinguish the medical officer of a convict prison, and they are not habituated to exhibit, whether through feeling or from assumption, the soothing, interested manner which acts so powerfully upon the temperament of the great body of Irish Convicts, whether male or female.Footnote 27
While Young was praised for his kindness, O’Keefe was criticised by Convict E.F. for ‘inhuman cruelty’ in keeping ‘poor maniacs in perpetual cells until reason had become undermined from hunger, flogging, and deprivation of the air of heaven’.Footnote 28
Prison medical officers varied in terms of their commitment to prison work, evidenced by the frequent complaints about their neglect of paperwork, poor record keeping and failure to attend the prison regularly or to absent themselves, noted by magistrates and prison administrators. At Spike Island, Dr Jeremiah Kelly was severely reprimanded by Crofton following the death of a convict who was treated by a hospital attendant in Kelly’s absence. On further investigation, Crofton discovered that Kelly was in the habit of leaving the prison for several hours during the night.Footnote 29 In turn, prison surgeons grumbled about their expanding workloads and inadequate recompense. F.A. Bulley, surgeon to Reading Gaol, complained in 1853 that his quadrupled workload following the introduction of the separate system had not been matched by a salary increase. Caring for 187 prisoners and 22 officers, he received only £80 per annum compared with the surgeon at York who had a similar number of prisoners but was paid £300. In response to Bulley’s request, the magistrates argued that he devolved too much work to his assistant to warrant a salary increase, noted that there were complaints about his tardiness and failure to complete registers and reports, and threatened him with dismissal.Footnote 30 In 1882, the salaries of Irish prison doctors ranged widely from £60 for medical officers at smaller local prison like Castlebar, County Mayo, to £200 for the medical officer at Cork Male and Female prisons, while Young, who served Mountjoy Male and Female Prisons, had a salary of £360.Footnote 31
In the years after nationalisation, new and detailed schedules of responsibilities for prison medical doctors were developed, although positions at local prisons remained part-time and non-residential.Footnote 32 By mid-century epidemic diseases had largely vanished from prisons, but the space this created in terms of prison medical officers’ workloads was amply filled with cases of mental breakdown. Increasingly, doctors were also required to implement and support the prison’s disciplinary practices, to make judgements on the amount of food prisoners required, and determine whether prisoners were mentally and physically fit for labour and punishment.Footnote 33 Dr Quinton claimed in his autobiography outlining his career as a prison medical officer that by the late nineteenth century detailed medical examinations were made on reception and great care taken in assessing prisoners’ ability to undergo hard labour; this, Quinton suggested, represented a sea change and commitment that many long-serving prison surgeons were not willing to accommodate.Footnote 34 Prison regulations also charged prison staff with guarding against the unnecessary infliction of cruelty on physically and mentally ‘weak’ prisoners and with maintaining the health of prisoners within the testing prison environment. Joe Sim contends that the constraints these regulations placed on prison medical officers, often referred to as ‘dual loyalty’, hampered the ability of prison medicine to work either independently or benevolently. It produced tensions between doctors’ status as employees of the prison system and their roles in monitoring and approving the disciplinary aspects of the prison regime, and the obligation to care and lobby for the health of their prisoner patients.Footnote 35 Martin J. Wiener has also highlighted the ‘disciplinary face of Victorian public medicine’, arguing that there was an affinity between Victorian punishment and medicine.Footnote 36 In this chapter, we consider the repercussions of these regulations for medical officers’ management of the mental health of their charges, and ask whether and how deeply medical officers were implicated in the imposition of disciplinary regimes that resulted in or exacerbated mental breakdown. Our research demonstrates significant variation in the ways individual prison medical officers working in England and Ireland implemented discipline and responded to mental breakdown among prisoners, a topic examined in detail in the second section of this chapter.
Simultaneously, medical and psychiatric opinion on the nature and cause of criminality became more penal in the late nineteenth century, as faith in the potential for reform began to evaporate. Penologists and social commentators were disheartened by failed efforts to reform and rehabilitate, and they were, like prison administrators, alarmed about the high level of reconviction. By the late nineteenth century, seeking explanations for past failures and new ‘remedies’, penologists and psychiatrists researched and published on scientific criminology and the relationship between crime, degeneracy and mental unfitness. Rejecting the theories of Caesar Lombroso and other continental criminologists on the ‘born criminal’, they emphasised the ways in which criminology in the British Isles varied in approach.Footnote 37 Criminologists and psychiatrists in England and Ireland did not, as Forsythe has shown, ‘begin to search around for human apes or tribal types for they did not apply a rigid theoretical framework to their descriptions’.Footnote 38 Rather, as Campbell’s comments at the opening of this chapter demonstrate, they imperfectly absorbed a version of positivist science and evolutionary theories as they became disillusioned with reform. By the 1880s they, along with other social commentators, began to argue that criminality and mental capacities were ‘relative constitutional fixedness’.Footnote 39
This chapter also assesses the implications of the altered medical and penal landscape for the mental condition of prisoners in local and convict prisons in late nineteenth-century England and Ireland. While McConville has acknowledged that concerns about the relationship between disciplinary regimes and mental distress in local prisons influenced penal policy, there has been limited analysis of the implications of the refashioning of prison discipline on the minds of prisoners.Footnote 40 Wiener has argued that after the debates on the relationship between the separate system of confinement and mental breakdown in the 1830s and 1840s, interest in and commentary on the issue dissipated until the 1870s.Footnote 41 Yet disquieting rates of mental disorder continued to be reported in local and convict prisons and were discussed in various official inquiries examining prisons and penal policy as discipline was strictly enforced after the 1860s.
This chapter examines the changing role of the prison medical officer and considers whether the constraints of dual loyalty, alongside overwhelming workloads in environments ill-suited to medical and psychiatric care, overpowered the potential of medical officers to pursue regimes mindful of prisoners’ wellbeing, instead becoming ‘integral to the control and disciplinary apparatus of the modern prison’.Footnote 42 The first section examines the debates around the implementation of changes to penal policy in the late nineteenth century, with a particular focus on the contributions of influential prison medical officers as well as senior prison officials and reformers. It investigates whether those charged by the state with responsibility for prisons and for the minds of prisoners were troubled by the gap between the stated aim of penal policy – that the ‘ordinary condition’ of prisoners did not allow gratuitous suffering or danger to life and health – and the reality of the institutions they managed. It also considers whether, as penal policy evolved, there was debate and conflict among prison administrators regarding their responsibilities for prisoners’ mental wellbeing.
The second section of the chapter focuses on medical expertise and knowledge production, and assesses the responses of English and Irish prison doctors to the positivist turn in the field of criminal justice and the specific problem of the habitual criminal in terms of their day-to-day practices. Assessments of English criminology by Neil Davie, Stephen Watson and others have focused on debates on the theories of the criminal mind, and the feeble-minded, and how they could be traced, observed and defined.Footnote 43 Our sources, which, alongside official reports, include the archives of individual prisons, underline the challenges presented to medical officers by the ‘lunatic criminal’, in a context shaped increasingly by anxiety about the rise in recidivism, high prison populations and failure to reform. Medical officers became ever more assertive in identifying themselves as experts in prison medicine, and, as Chapters 4 and 5 also explore, in understanding and dealing with mental illness in prison. As Hardy has pointed out, this was challenging work. ‘I am completely at the mercy of these men,’ Brixton Prison’s Medical Officer noted in 1882, alluding to the lack of cell accommodation for ‘troublesome mental cases’.Footnote 44 Most prison medical officers received little formal or practical training in psychiatry and few had experience of working in lunatic asylums.Footnote 45 Yet, as the second section of this chapter demonstrates, prison medical officers formulated a specific taxonomy and classification of mental illness related to lunatics who were also criminals. Local and convict prisons became sites of knowledge production, as prison medical officers developed distinct medical categorisations, which embedded prisoners’ criminality and ‘criminal natures’ in their mental conditions and states. We draw on prison medical officers’ descriptions and correspondence about their prisoner patients, and on what became an extensive medical journal literature, which oftentimes dealt deftly and dismissively with continental criminal anthropology, before moving on to the practicalities of management, and to individual cases and examples to explore the everyday management of mental health in prison.
I The Hardening of Penal Policy and Practices
Diet, Labour and the Separate System of Confinement
The two major parliamentary commissions of 1863, reviewing prison regimes in local and convict prisons, encapsulated the shift in tone and approach to late nineteenth-century penal policy. Throughout the 1850s the rigour of the separate system as implemented in convict prisons had been toned down under Jebb’s chairmanship of the Directors of Convict Prisons, and prisoners’ mental and physical health was reported to have improved under this modified regime.Footnote 46 Some early adaptations of the separate system had aroused criticism, not least an experiment at Reading Gaol, implemented by Chaplain Field and aimed at enhancing prisoners’ reading and comprehension skills. It was fiercely criticised by the Visiting Justices and Prison Inspectors, and in 1854 penal labour was reasserted at the gaol.Footnote 47
In 1857 and 1864 amendments to the Penal Servitude Acts sought to reinforce the disciplinary regimes in convict prisons. With the death of Jebb in 1863, an influential barrier to the assertion of punitive and deterrent disciplinary ethos in convict prisons was removed.Footnote 48 More stringent implementation of the separate system of confinement was advocated, with the 1863 Royal Commission on Transportation and Penal Servitude concluding that penal servitude was not ‘sufficiently’ dreaded. Witnesses noted, for example, that the average convict spent less than nine months in separate confinement and insisted that the period of separation be implemented fully and ameliorated only when there was a threat of physical or mental injury to convicts.Footnote 49 The Commission recommended reversing many of the modifications introduced in the 1850s and advocated for the introduction of separation for able-bodied convicts at the public works prisons at Chatham, Portsmouth, Portland and Gibraltar, and Dartmoor and Woking Invalid Prisons.Footnote 50 The system of granting marks or credit for good conduct adopted in Irish and English convict prisons was criticised as was the practice of granting convicts marks for diligence in Irish prison schools.Footnote 51 The Commissioners noted differences in the administration of penal servitude legislation in England and Ireland, and commended the ‘formidable’ rendering of the separate system under Crofton’s system in Ireland. In addition to the operation of intermediate prisons, and the supervision of holders of tickets of leave, in terms of the implementation of the separate system during the probationary stage at Mountjoy, they specifically praised the lower, meat-free diet provided during the first four months in separation and limiting work to oakum picking in the first three months.Footnote 52 These rigorous elements of the separate system, they argued, increased the ‘wholesome effect’ on the minds of prisoners.Footnote 53 The Commission sought greater severity in sentencing penal servitude convicts, the introduction of the ‘progressive’ or ‘mark system’ in English prisons, and tighter implementation of the separate system. Colonel Edmund Henderson, who succeeded Jebb as Chairman of the Directorate of Convict Prisons in 1863, implemented many of these recommendations; the provision of ‘extra diets’ was prohibited except on medical grounds, hammocks in separate cells were substituted with plank beds, and convicts were to spend the full nine months in separation except in cases of serious injury to mental or physical health.Footnote 54
Lord Carnarvon’s 1863 Select Committee was particularly important in shaping policy in local and borough county prisons. Witnesses were quizzed on the high levels of recidivism among prisoners, poorly trained staff and substantial variations in the implementation of regulations. Prison inspectors and other medical and lay experts on penology identified local prisons as particularly problematic, repeatedly criticising them for failing to impose rigorous and uniform systems of discipline, though it was acknowledged that sentences in local prisons were too short for the full application of the separate system. They were also accused of overfeeding prisoners and lax supervision of ticket-of-leave prisoners.Footnote 55 When published, the recommendations of the Carnarvon Committee reinforced the social function of prison while its reformative aim was downplayed.Footnote 56 The ‘moral reformation of character’, Carnarvon insisted, was ‘greatly assisted by a preliminary course of stringent punishment’.Footnote 57 While retaining the separate system as the basis for penal discipline in local prisons, Carnarvon sought to configure specific elements of the regime, notably prison labour, diet and the environment of the cell, to heighten the punitive experience.Footnote 58
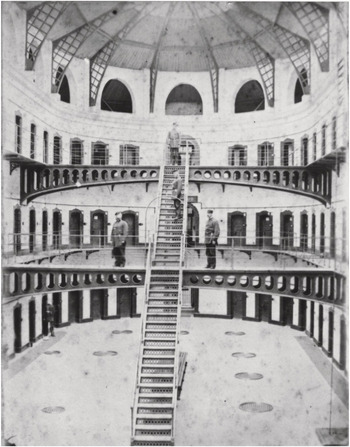
Carnavon’s recommendations set the tone for debate on local prisons across England and Ireland, and specifically shaped the English Prison Act of 1865.Footnote 59 In Ireland, Corry Connellan, Inspector General for Prisons, advocated in 1863 for the introduction of many of the committee’s recommendations to local prisons. He helped draft a Prisons (Ireland) Bill in 1866, which, if implemented, would have consolidated legislation relating to prisons in Ireland and introduced elements of the 1865 English Prison Act.Footnote 60 The Chief Secretary for Ireland, Lord Naas, was an influential proponent of the bill, but, while reaching a second reading in the House of Lords, it fell foul of the extremely busy parliamentary sessions in 1866 and 1867 and did not pass into legislation. Nonetheless, the separate system was scheduled for implementation in local prisons as provision expanded in the 1860s, including the opening in 1863 of a new east wing with over 100 cells for separate confinement at Kilmainham Gaol, Dublin (Figure 3.1).
The remit of the Carnarvon Committee was wide-ranging, and specific aspects of penal discipline, notably what constituted hard labour, prison diet and the conditions and implementation of separate confinement, were forensically examined. The effectiveness of these aspects of prison discipline was debated during subsequent inquiries into English and Irish penal policy over the next three decades, including the 1878 Commission on the Penal Servitude Acts (the Kimberley Commission), and the 1884 Royal Commission on Irish Prisons, which reviewed the implementation of prison legislation in local and convict prisons. Primarily concerned with balancing the punitive and reformative aims of imprisonment, prison officials, penologists and a small number of ex-prisoners debated the deleterious impact of the new disciplinary regimes on prisoners’ physical and mental health in their evidence to these inquiries. In addition, as the duties of prison medical officers were reconfigured and bolstered, some medical officers highlighted the challenges of aligning their roles and responsibilities in safeguarding the mental health of prisoners with the increasingly penal approach of the prison environment.
The push for uniform and rigid application of prison discipline across the prison estate in the 1860s and 1870s was partly a response to high-profile reports, including those of physiologist and social reformer, Dr Edward Smith, that highlighted the uneven implementation of prison discipline.Footnote 61 In the late 1850s Smith had surveyed the effects of prison discipline on prisoners’ health in English county gaols, and his analysis of the dietary requirements of prisoners on hard labour were submitted to the Carnarvon Committee and published in the final report.Footnote 62 His work, reported in the Lancet in 1858, revealed uneven enforcement of hard labour across the English prison estate, and in some instances he found ‘no labour at all’.Footnote 63 Smith observed disparities in the types of labour designated as hard labour; in one prison, ‘oakum-picking was no labour … and hard labour in another’.Footnote 64 He also claimed women were placed at the crank and treadwheel in some prisons, although George Laval Chesterton, Governor at Cold Bath Fields Prison in Clerkenwell, had complained that women, who ‘could not expect the same chivalrous sympathy accorded to their more morally upright sisters’, did not work at the treadwheel.Footnote 65 Considering the implementation of the separate system in local prisons, Smith reported strict enforcement of all elements in some prisons, including prisoners being compelled to wear masks when moved around the prison, while elsewhere ‘hundreds of prisoners sit together in the room picking oakum’.Footnote 66 He also drew attention to the varied punishments inflicted on prisoners, noting unequal application of corporeal punishments including whipping by officers using the ‘cat’.Footnote 67 In his evidence to the Carnarvon Committee, Smith sought absolute uniformity of prison punishments, and claimed prisoners were idle for long periods of each day. He suggested they perform not less than 7½ or 8 hours of work a day when serving hard labour sentences, and a minimum of 10 hours a day for other prisoners.Footnote 68
The imprint of Smith’s findings can be identified throughout the report and recommendations of the Carnarvon Committee, which rejected oakum picking, and forms of industrial occupation, originally intended to improve prisoners’ minds as well as punish them, as ‘light’ or ‘immediate’ labour, and only accepted punitive work at the treadwheel and crank as ‘hard labour’ proper (Figure 3.2). Shot drill was permitted when local authorities needed to supplement the treadwheel and crank.Footnote 69 In designating these three forms of work as ‘hard labour’, they explicitly rejected the positive impact of industrial labour on prisoners’ minds as ‘much less penal, irksome, and fatiguing’ in favour of punitive hard labour intended to make prisoners’ experiences more unbearable.Footnote 70 In Ireland, Connellan advocated Carnarvon’s recommendations, lamenting the lack of ‘punitive labour’ in local prisons, which, he argued had been imperfectly replaced by industrial labour, a change he dismissed as futile. With the publication of the Report of the Carnarvon Committee, he sought its reintroduction to county prisons, and suggested the separate system be extended to prison hospitals to prevent communication among patients.Footnote 71

Figure 3.2 Middlesex House of Correction: male prisoners on treadmill. Wood engraving by W.B. Gardner, 1874, after M. Fitzgerald
Several witnesses to the Carnarvon Committee were troubled by some of the proposals. Dr John George Perry, Inspector of Prisons for the Southern and Western Districts and the Medical Inspector of Prisons in England and Wales, emphasised the dangers of the treadwheel to prisoners’ health. He sought its abolition ‘on account of the inequality of its operation’, ‘its injurious effect upon the health of many of the prisoners’, and ‘when unproductive, a waste of labour which might be better bestowed’.Footnote 72 Major William Fulford, Governor at Stafford Prison, however, suggested to the committee that he already had the powers to impose a deterrent and severe regime, which in his view should combine hard labour with a low diet and use of the whip:
If I had the means of giving every man who is sentenced to hard labour in Stafford prison the full amount of discipline I am empowered to do by Act of Parliament, for two years, no man alive could bear it: it would kill the strongest man in England.Footnote 73
Other witnesses referred specifically to the ‘irritating’ impact of the crank and treadwheel on the minds of prisoners, with some prisoners finding unproductive work ‘disheartening’, ‘depressing’ and leading them to despair.Footnote 74
Nonetheless, work at the treadwheel was selected as the preferred form of hard labour and prison officials sought its implementation across local prisons. In Ireland, there was variation in the form of hard labour depending on conditions at individual gaols, and the treadwheel was not systematically introduced. However, by 1880, it was implemented at Castlebar, Clonmel, Richmond, and Galway and Cork Male Prisons. At other local prisons, male inmates picked rope junk or oakum, worked at shot drill, which, according to Priestley, was virtually ignored in English local prisons, or broke stones.Footnote 75 In prisons with a sizeable female population, such as Belfast, Kilmainham, Cork and Grangegorman, women usually worked at picking rope or oakum.Footnote 76 After nationalisation those confined at Mountjoy Male Prison were employed at mat making and picking coir in cells, while convicts in Mountjoy Female Prison made bedding and clothing, and did the laundry for other prisons and institutions.Footnote 77 By 1882, however, Frederick Richard Falkiner, Recorder of Dublin, criticised the continued use of the treadwheel and shot drill in some prisons, as well as ‘the almost valueless oakum and hair picking, and the mat making’ in others.Footnote 78 Alongside the deferral of legislative reforms, for him the persistence of such prison labour was evidence of the deterioration of the Irish system, once praised as ‘the best solution of the convict problem, and a model for imitation in Europe and America’.Footnote 79
Most parliamentary commissions on prisons were preoccupied with the relationship between prison diet, punishment and discipline, and several witnesses highlighted the potentially negative effects of reduced diet on the minds of prisoners. Jebb stressed the importance of a ‘good diet’, which Reverend W.L. Clay had dismissed as ‘belly bribes’ for prisoners serving long sentences at Pentonville Prison in his evidence to Carnarvon’s Committee, arguing it counteracted the ‘depressing influences of separate confinement’.Footnote 80 An advocate of separate confinement, Jebb insisted the separate cell had a ‘very corrective effect upon the mind of a prisoner’.Footnote 81 As early as 1849, as discussed in Chapter 2, Jebb had, however, become concerned that a severely reduced diet could damage the mental as well as physical health of convicts.Footnote 82 Dietary modifications to reduce costs at Wakefield Prison, he claimed, were a false economy given that ‘imprisonment injudiciously prolonged after unequivocal symptoms of failing health had appeared or an insufficiency of diet’, rendered the convicts mentally and physically depressed and unfit for transportation, and was thus a long-term drain on prison resources.Footnote 83 Two years earlier, William Milner, Medical Officer at Wakefield Prison, had become concerned about the ‘unmanageable’ delusions among prisoners in separate confinement, and in response had increased dietary allowances and periods of exercise, modifications that appeared to have benefited the prisoners.Footnote 84
The importance of a ‘sufficient’ diet was stressed by Inspector Perry, who commented on the restorative and medicinal use of diet by prison surgeons not only to ‘treat disease but to prevent it’. He sought extra dietary allowances to restore the constitutions of enfeebled and physically debilitated prisoners, especially vagrants.Footnote 85 Nonetheless, there were those who advocated for sparser dietary scales, including Fulford at Stafford, on the grounds that prisoners on shorter sentences were not required to perform hard labour.Footnote 86 Concerns about prisoners becoming too enfeebled and physically incapacitated to work on release, the threat of epidemic disease outbreaks in prisons, and maintaining prisoners’ capacity to perform labour, prompted the Carnarvon Committee to defer any proposals for a national, uniform dietary scale for local prisons, and concluded that prison diet was not to be used as an instrument of punishment.Footnote 87
The quality and quantity of prison diet in Ireland was also scrutinised in the 1860s. As in England, diet in local prisons was sparser than in convict prisons; nonetheless, these dietary scales had been criticised for their generosity when compared to the diets of the average agricultural labourer, workhouse dietaries and the sparser diets implemented in English local prisons. A lower dietary scale was introduced in 1849, and further reductions implemented in 1854 for prisoners aged fifteen years and under, to align prison and workhouse diets for that age group.Footnote 88 Cautioning against further reductions, in 1863 the Irish lawyer and politician Edward Gibson insisted that once a fair, ‘sufficiently penal’ diet had been agreed, diet should be ‘regarded as a medical question’. ‘The system of starving crime into surrender’, Gibson argued, if it went below the limit necessary for health, would prompt expensive hospital admissions, with prisoners liable to become burdens on the rates once released. Consequently, the ‘superiority’ of prison food ‘must again be asserted’.Footnote 89 The 1863 Commission on Transportation and Penal Servitude recommended that the practice of not providing meat during the first months in separation in Irish prisons be extended to English convict prisons, and, while they did not advocate for the reduction of diet for convicts working in association in public works prisons, they suggested some experimentation ‘to ascertain whether any reduction can safely be made’.Footnote 90
From 1863 the disciplinary regime applied to penal servitude convicts in separation became more punitive, and by 1878 the Kimberley Commission concluded that the sentence was ‘generally an object of dread to the criminal population’.Footnote 91 Dietary privileges, including those allowed at Mountjoy Convict Prison, were abolished and the reduced diet for convicts during the first three months of their sentences was enforced.Footnote 92 These changes prompted concern from penologists, including Crofton, who defended the relatively generous dietary scales for convicts against criticism from the Board of Superintendence of Dublin City Prisons on the grounds that convicts were required to preform hard labour.Footnote 93 In 1863, Reverend Charles Bernard Gibson, Chaplain at Spike Island, also warned against reducing convict diets further, but he reasoned that depriving convicts of employment during their first months in ‘solitary cells’ was more damaging as it deprived ‘the mind of its proper food’.Footnote 94 Responding to these concerns, a medical committee, comprising the eminent physician Dr William Stokes, Dr John Hill, the Poor Law Medical Inspector, and Dr William M. Burke, Medical Superintendent at the General Register Office, were appointed to inquire into dietary scales in Irish county and borough gaols.Footnote 95 On their recommendation, in 1868 prison governors were ordered to improve the quality of the food.Footnote 96 In their final published report, the commissioners highlighted the tensions inherent in the role of the prison surgeons. It was, they noted, inconsistent ‘with the character and the objects of medical science, that the Surgeon should be compelled to watch for the time when the punishment can be no longer endured, and so virtually to become, in his own capacity, an assistant to the execution of a sentence’.Footnote 97
The nationalisation of both prison systems under the 1877 Prison Acts reopened the debate on prison diet. The Acts enabled prison boards to further enforce the punitive and disciplinary regimes in both convict and local prisons. Rationalisation, frugality and disciplinary rigour preoccupied Du Cane and Charles Bourke, and Du Cane established a scientific committee on prison diet, which reported in February 1878.Footnote 98 Comprising Henry Briscoe, Inspector of English Prisons, Dr Robert Gover, Medical Officer at Millbank Prison, and C. Hitchman Braddon, Medical Officer at Salford Hundred County Prison, it was charged with considering whether changes to prison discipline brought in under the 1877 Act necessitated new dietary scales, especially in cases when the period prisoners spent at hard labour was reduced. The committee members framed imprisonment as a ‘physiological rest’ when the ‘struggle for survival is suspended’, with prisoners guaranteed food and other necessities. Considering the psychology of prisoners, they contended that ‘Tranquility of mind and freedom from anxiety are leading characteristics of his [the prisoner’s] life. From the moment that the prison gates close behind him, the tendency, in most cases, is to lessened waste of tissue; he lives, in fact, less rapidly than before.’Footnote 99 Labour exacted on inmates in local prisons, they argued, was not ‘excessive’, while ‘wholesome’ work, whether mental or physical, was not normally lethal. ‘Worry’, however, was more dangerous, as it was a ‘rust, which eats into the blade and destroys it’, although prisoners, ‘as a rule’ were free from it.Footnote 100 The committee’s published report repeatedly referenced the ‘mental peace’ and tranquillity of life in prison, which was characterised as a protected and insulated existence, with prisoners free from the emotional strife that can ‘exhaust the vital energies’ in everyday life. The prisoner ‘rarely experiences domestic grief or disappointment; and, as a general rule, he has no pride capable of receiving a wound’.Footnote 101 While briefly acknowledging that ‘the restraints of discipline’ and the loss of liberty could be irksome and a ‘severe trial’, and ‘that what appears to us to be peace and order may to the inmates be often indistinguishable from gloom and monotony’, the overall tone of the report minimised the difficulties of prison life.Footnote 102 Deviating from the 1868 recommendations of the medical committee on Irish dietary scales, Du Cane’s committee did not highlight any potential tension in the role of the prison medical officers and instead reiterated the importance of the judgement of the prison doctor in deciding whether prisoners should be allocated extra allowances of food.Footnote 103 The committee recommended that prison medical officers retain discretionary power to approve extras, and, while noting that diet should not be diminished where health was damaged, they cautioned against prison doctors allocating too liberal a diet.Footnote 104
A modified version of English prison diet, scheduled for Irish prisons under the 1877 Prison Act, was delayed owing to disagreement among the Irish medical profession on its suitability. However, a second medical commission, established by the Irish General Prisons Board in 1880, concluded the new scales were ‘sufficiently liberal’. As with the English commission, they agreed prison doctors should be permitted to make minor alterations for ‘diseased’ prisoners, but disapproved ‘of any interference with the dietary scales as laid down for healthy prisoners’.Footnote 105 They also introduced amendments to the convict prison diets at Spike Island and Mountjoy Male and Female Prisons.Footnote 106 The 1884 Royal Commission on Irish Prisons claimed that changes to prison diet contributed to increased expenditure.Footnote 107 Nonetheless, the Commission recommended enhanced dietary allowances for specific classes of prisoners owing to the inferior bodily condition of Irish prisoners, whose previous habits, poor quality of foodstuff and their ‘generally low physical condition of health render them more susceptible to the effects of prison discipline’.Footnote 108 Despite earlier attempts by the General Prisons Board to halt such practices, the Commission noted that medical officers frequently prescribed improved diets as a prophylactic against illness among ‘juvenile offenders, nursing mothers, and aged prisoners … although as a matter of fact such prisoners are in excellent health’.Footnote 109
While debates on prison diet and the implementation of hard labour dominated discussions of penal discipline in the late nineteenth century, other aspects of prison discipline, which affected prisoners’ mental and physical health, were critically reviewed, including hammock-style bedding, which had been used in separate cells since the implementation of the separate system. Following Carnarvon’s recommendations, hammocks, believed to be too comfortable, a ‘self-indulgence’, were replaced with plank beds usually without any mattress, for inmates serving the first stage of sentence.Footnote 110 Inspector Perry, however, warned against their widespread use, as they caused repeated sleepless nights and impaired mental and physical health.Footnote 111 In 1884 the leading Irish nationalist parliamentarian Charles Stewart Parnell, who viewed prison diet and the treadwheel as too severe a punishment, noting the ‘semi-starved’ aspect of the prisoners at Kilmainham Gaol, described the plank bed as a ‘punishment attended with physical torture’.Footnote 112 Society, Parnell argued, was not entitled ‘to enfeeble the bodies of prisoners in order to reform their minds, or with a view of maintaining discipline amongst them’.Footnote 113 Dr Hercules McDonnell, echoing Parnell in his objection to the plank beds, insisted ‘punishment should not include cruelty, nor should it impair health’. He argued against their use ‘in long term sentences … from a moral point of view. It engenders a mental state of resistence [sic] to authority, and renders the prisoner less amenable to discipline or the better influences which ought primarily to be cultivated.’Footnote 114
MacDonnell was one of many detractors of the revised disciplinary regimes of the 1860s and 1870s and the relentless drive to impose a uniform punitive system. Witnesses at Carnarvon and subsequent committees cited the potential damage the harsher disciplinary regimes could inflict on prisoners’ spirits, and ultimately their minds, and their implementation elicited further debate on the link between the separate system of confinement and incidences of mental disorder and distress in prisons. In their critiques, prison medical officers, chaplains and other prison officials explicitly connected mental disorder among prisoners and convicts to the new punitive prison regimes, and modified versions of the separate system were introduced to some local prisons in England and Ireland. Proponents of the new penal regimes, meanwhile, persistently argued that many prisoners entered prison predisposed to mental weakness and were constitutionally unable to withstand its rigour or benefit from it, rather than blaming the regime for prompting mental breakdown and insanity.
In 1863 a number of key prison administrators, including Inspector Perry, Herbert Voules, the Inspector for the Northern District, and Edward Shepherd, Governor at West Riding Prison, Wakefield, objected to various measures proposed for local prisons, citing the potential for damage to the minds of prisoners. Perry, for example, contended that prisoners found unproductive labour such as the treadwheel and the crank demoralising, degrading and irritating, having a ‘prejudicial effect on the temper of the men’ and ‘resulting in ‘insubordination produced by irritation and despair’.Footnote 115 Jebb, who acknowledged the ‘depressing influence’ of unproductive labour, also downplayed it, insisting that ‘some prisoners will resist anything that is disagreeable to them’.Footnote 116 Such commentary highlighted an enduring ambiguity: on the one hand, prison administrators commented on the harm inflicted on prisoners by prison discipline and environments, and, on the other hand, demonstrated a persistent faith in the overall efficacy of prison discipline and in the separate system. Voules agreed that ‘unproductive employment’, such as the treadwheel, led to the degradation and irritation of the minds of prisoners and that separation was a ‘severe punishment’ to prisoners.Footnote 117 Yet he insisted that the separate system was ‘the only safe foundation of prison discipline … it forces a man to reflect; it makes him feel that employment is a boon … and it separates him from [the] contaminating influence of other prisoners’.Footnote 118 In 1863, Jebb suggested the ‘depressing influences’ of separation were partly a consequence of the reduced amount of exercise required of convicts while working at a trade, but that ‘any deleterious effect’ on prisoners would be mitigated with sufficient fresh air and exercise.Footnote 119 Dr Clarke at Pentonville, however, noted that prolonged periods in separation produced a ‘debilitating effect upon men’, and in 1870 observed that the moral influence of solitary confinement was, ‘if not hurtful to the mind, at least negative for good’.Footnote 120 However, defending the separate system, Dr William Guy, Medical Superintendent of Millbank Prison, observed:
Our system of separate confinement does not appear to affect the mind injuriously. I do not mean to say that a prisoner who comes into prison upon the verge of unsoundness of mind, might not develop into full unsoundness in that time, partly because of the separation; but I am of opinion, also that a prisoner should expect that this may happen to him, and that the possibility of unsoundness must be taken into account as one of the results of his being in prison at all.Footnote 121
Irish prison staff showed similar disquiet and ambivalence. In 1862 Dr Maurice Corr, Medical Officer at Philipstown Prison, which housed a large number of invalids, noted the ‘great irritability and total destitution of self control’ among prisoners whose ‘mental disease’ was ‘generated and fostered in prison’, while Michael Cody, Roman Catholic chaplain at Mountjoy Male Prison, objected to subjecting prisoners to separate discipline for eight months.Footnote 122 Disagreeing with the Directors of Convict Prisons in 1869, at a time when the prison population at Mountjoy had declined by two-thirds, Cody argued ‘that to subject the prisoners to the separate discipline for eight months is calculated to injuriously affect them mentally as well as physically’ as the regime had ‘the effect of gradually causing depression of spirits, nervousness, eccentricity, and causing, what is most to be deplored, loss of that controlling power by which man governs his imagination, course of thought, and inferior appetite’.Footnote 123
Despite these concerns, and the disastrous experiences at Pentonville in the 1840s, in the late nineteenth century support for separate confinement remained entrenched among senior prison officials. Medical Inspector Dr Gover, commenting favorably on conditions in Millbank Prison in 1870, noted that among the 27 convicts certified as insane, 25 were sick on admission and two had histories of mental illness. Defending the disciplinary regime, he observed that ‘No case came under my observation, of which it could be said that the mental disease had been brought on by the discipline of the prison.’Footnote 124 In 1874 Millbank’s chaplain described separate confinement, ‘as the only chance’ of bringing prisoners under ‘moral or religious influence’, insisting the prison’s regime had no injurious mental or physical consequences. While acknowledging that strict implementation of separation for the whole sentence of penal servitude was harmful, he advocated in favour of minimum association among prisoners as ‘the most successful in its reformatory and deterring effects on the criminal’.Footnote 125
Despite Hercules McDonnell’s criticisms, there was greater acknowledgement during the 1884 Royal Commission on Irish Prisons of the dangers the separate system posed to prisoners’ minds. Captain John Barlow, Director of Irish Prisons, under questioning from Dr George Sigerson, conceded that ‘The cellular discipline of Mountjoy would I suppose tend to develop insanity.’Footnote 126 Sigerson claimed ‘the number of male convicts becoming insane at Mountjoy would exceed three times’ the number found in prisons that were not operating the separate system.Footnote 127 The final report criticised prison medical officers for failing to rigorously examine prisoners on reception to identify incipient diseases, especially symptoms of mental illness, and recommended reception wards be provided in prisons to allow for the close observation of prisoners on admission. With early identification such prisoners could be quickly removed to hospitals, or carefully observed, and so ‘prevent the infliction of punishment for breaches of discipline committed by prisoners suffering from nervous irritability, who really are more properly subjects for medical treatment than for punishment’.Footnote 128
‘A Servant of the Board’? Medical Officers and Prison Practices and Regimens
While the degree of uniformity originally sought by senior prison officials, including Du Cane, was never realised, cumulatively the legislative and policy changes of the 1860s and 1870s had a striking impact on prison life and prisoners. McConville has suggested that conditions in English local prisons were especially harsh with little support for the reformative objective of imprisonment. For inmates the prison environment became more taxing, rigorous, and in some instances brutal, especially in prisons that were overcrowded, insanitary and the physical infrastructure dilapidated.Footnote 129 Conditions in Irish local prisons were likewise severe, and, in terms of sanitation, often dangerous, though, as Beverly Smith has argued, it is unclear whether these conditions reflected a coherent penal policy or the General Prisons Board’s bad management.Footnote 130 Officers in some local prisons struggled to maintain discipline and order, and their efforts to implement prison regimes could be fierce and relentless, especially when managing irritable, destructive and violent prisoners, many of whom were described as mentally ill-equipped and unable to withstand prison discipline. There were also instances of neglect, cruelty and poor management by badly trained staff.
As noted above, the 1865 English Prison Act tightened regulations to ensure regular medical visitations to local prisons, while in the early 1860s individual boards of superintendence of county gaols in Ireland published bye-laws and detailed schedules of doctors’ duties and responsibilities. Overall in both settings, these expanded regulations required prison medical officers to attend prisons regularly, to examine every prisoner each week, and to visit daily sick prisoners on extra diet and those confined in punishment cells, recording treatments in journals and report books. They were also required to attend prison staff and their families, to supervise and train hospital warders, inspect the entire prison building on a regular basis, report structural faults in prison ventilation and drainage, and to assess the quality of bedding, clothing and food, and when necessary, implement public health measures to prevent the spread of infectious diseases.Footnote 131 They were also to investigate prisoner deaths. Finally, the regulations enforced doctors’ active involvement in the administration of prison discipline, requiring them to adjudicate on prisoners’ fitness for hard labour and punishments. The regulations specifically outlined prison medical officers’ duties in terms of safeguarding the minds of prisoners, and watching for signs of mental deterioration or other adverse health effects related to the disciplinary regime. Doctors were to report cases to the prison governor with directions for treatment, which usually included extra food and exercise. They were also permitted to consult medical advisors from outside the prison. These duties and regulations not only placed prison doctors under considerable pressure, they also involved them in the disciplinary aims of penal regimes, regardless of whether or not they endorsed these.
Many prison doctors in England and Ireland, like prison governors, transferred from military careers into the prison service and would have been used to a working environment that stressed discipline and order, though increasingly by the second half of the century they devoted their entire careers to prison medicine. They pressed regularly for improved conditions and salaries, framing these requests as being beneficial to the prisoners they cared for. In Ireland, the Association of Gaol Surgeons, with Dr Hercules MacDonnell as Honorary Secretary, was formed to lobby for the interests of the profession as the duties of prison medical officers were expanded under the 1877 Act without, they argued, appropriate remuneration.Footnote 132 In 1882, these duties, as originally laid out in the legislation, were partly amended, but the Association continued to pursue a campaign against the General Prisons Board, lasting several years. Acrimonious and bitter, it highlighted the hostility prison doctors felt towards the Board, which was accused of ‘insidious encroachment’, ‘illiberality’ and ‘attempted bullying’.Footnote 133 To improve relationships, the 1884 Royal Commission on Irish Prisons recommended the appointment of a Medical Inspector to the General Prisons Board, and a year later Dr Frederick McCabe, Local Government Inspector, commenced in post. Though complimentary about McCabe, the Medical Press and Circular claimed that he and the prison ‘medical department’ had been ‘subordinated’ by making the post holder ‘a servant of the Board’, compromising McCabe’s capacity to act and comment independently.Footnote 134
In much of their early correspondence with local prison governors, the General Prisons Board vigorously enforced new prison rules, demanding that prison officers, including surgeons, adhered to the new orders, prompting the resentment of prison medical officers.Footnote 135 Medical officers were frequently admonished for interfering with or ignoring the decisions of the Board, and exceeding their powers. In May 1880, following the death of prisoner J. Connors after an attempted suicide, the Board rebuked the Governor at Waterford Prison for exhibiting ‘a great want of judgment … in not requiring the prisoner to be visited frequently during the night after he had been placed in muffs & that it was considered he attempted suicide’.Footnote 136 The Board subsequently drafted a circular requiring that prisoners under mechanical restraint be visited at night and medical officers called on to regularly attend prisoners who attempted suicide.Footnote 137
The work of medical officers was complicated further by varied prison populations and conditions for inmates. While it is unlikely that the many prisoners serving short sentences spent prolonged periods in separation, its implementation remained the aim of prison officials.Footnote 138 As some English prisons were closed or amalgamated, others saw a rise in numbers and overcrowding in the late nineteenth century. Liverpool Borough Prison had a particularly large number of female committals, many ‘professedly prostitutes’.Footnote 139 On 20 September 1869, 1,097 male and female convicts were confined in 1,001 cells certified for separate confinement at Liverpool and two-thirds of the 12,785 admissions that year were recommittals.Footnote 140 The persistent problems of overcrowding and reoffending among female prisoners had first emerged in the 1850s.Footnote 141 By 1877, the prison’s Roman Catholic minister, Reverend James Nugent, an ardent temperance reformer, observed that among the 4,571 females under his charge in that year, only 648 had never before been in prison.Footnote 142 Some 1,310 were committed after being found drunk or accused of riotous conduct, and 1,555 for disorderly behaviour on the streets. Nugent, in his final report for the prison before his retirement, observed:
Drink is making terrible havoc upon the female population of this town; not only demoralizing the young, and leading them step by step into crime and the lowest depths of vice, but destroying the sacred character of family life, and changing wives and mothers into brutal savages.Footnote 143
Flagging up the close association between excessive drinking and mental breakdown, Nugent observed that ‘Not a week passes without some one being brought to the prison whom drink has maddened and robbed of all female decency, whose language and actions are so horrible that they seem no longer rational beings, but fiends.’Footnote 144 In 1898, Dr W.C. Sullivan and Dr Stewart Scholar, the latter Deputy Medical Officer at Liverpool Prison, reported on the link between alcoholism and suicidal impulses as revealed in 142 cases of persons charged with attempted suicide and remanded in Liverpool Prison. They argued that women’s ‘generative organs’, were ‘peculiarly susceptible to the alcoholic poison’, which produced ‘emotional alterations of the personality’ that could prompt suicidal tendencies.Footnote 145
In Ireland, the local prison population declined in the decades immediately after the Great Famine. In his evidence to the 1878 Commission on the Penal Servitude Acts, Reverend Lyons, Roman Catholic Chaplain at Spike Island, when pressed on whether he believed prison discipline acted as deterrent, was ambivalent and instead argued that during the Great Famine ‘The kind of people who were convicted were peasantry who had no notion of ever committing a crime.’Footnote 146 Nonetheless, there was anxiety about high rates of reoffending. The Inspectors General of Prisons in Ireland, concerned at the expansion of the local prison population, noted a 5.5 per cent increase in committals between 1862 and 1863, when they totalled 33,940, highlighting a rise in short sentences and a troubling growth in recommittals especially among women.Footnote 147 Frederick Falkiner observed in 1882 that among prisoners in custody for the January quarter of his court sittings, 76 per cent of the male prisoners had previous convictions; the average was five each while three had been imprisoned more than twenty times.Footnote 148 Among women the average number of previous convictions was seventeen.Footnote 149 Falkiner further noted that ‘with these unfortunates, men and women, the coming and going in this world is from the streets to the prison, from the prison to the streets, and back again with the certainty of recurrent tides – more contaminating and more contaminated with every flux and reflux’.Footnote 150
By the final decades of the nineteenth century, there was a ‘remarkable decrease’ in the size of the English and Irish prison populations.Footnote 151 Yet, while the overall figures supported claims that there was ‘a decline in the spirit of lawlessness’, the high rates of recommittals, especially for minor offences such as those related to alcohol, remained a cause of disquiet among prison officials.Footnote 152 At some prisons, not least Liverpool, the sheer size of the prison, combined with frequent overcrowding, the large numbers of prisoners on short sentences, and the high rates of recommittals, especially among women, prompted harsh responses from overburdened prison staff, including its medical officers working to rigorously implement new prison regulations.Footnote 153 In 1866, the Visiting Justices imposed work on the treadwheel or crank as first-class hard labour of the ‘most penal kind’ for able-bodied male adults, employing extra officers to enforce this. Other prisoners, including women, were set to oakum picking.Footnote 154 By 1868, prisoners were placed on the treadwheel for five hours during the first month of their sentence, and Liverpool’s Governor subsequently increased this to six hours a day, and then seven hours.Footnote 155 The treadwheel accommodated forty-five prisoners who were compelled to ascend 9,240 feet daily, and by 1876 a daily average of 148 male prisoners worked on it.Footnote 156
For prisoners, especially those serving their first sentences, hard labour was felt keenly, and authors of prison memoirs and some prison officials highlighted its mental as well as physical toll. In 1850, William Hepworth Dixon evoked the mental anxiety associated with hard labour, ‘the dull, soughing voice of the wheel, like the agony of drowning men – the dark shadows toiling and treading in a journey which knows no progress – force on the mind involuntary sensations of horror and disgust’.Footnote 157 Uninitiated prisoners dreaded the treadwheel and were said to find it ‘very irksome and severe’; in his evidence to the 1878 Kimberley Commission, Captain Henry Kenneth Wilson, Governor of Maidstone Gaol, described it as a ‘very unfair punishment’.Footnote 158 The Manchester Merchant, confined to Kirkdale Gaol in the late nineteenth century, ‘pitied the treadwheel men as they went out to their labour’; after a spell on it, it was not unknown for ‘big, strong fellows’ to be ‘led away crying’.Footnote 159 ‘One Who Has Tried It’, who served time in a local prison in England in the 1890s, referred to being in a ‘bath of perspiration’ and feeling ‘quite crushed’ when he returned to his cell after his first experience on it.Footnote 160 Governor Wilson, however, ‘noted that experienced prisoners preferred the wheel to picking oakum’, which was a dirty, slow job.Footnote 161 The rope was covered in tar and the strands were difficult to prise apart. Usually set as ‘task’ work, inexperienced prisoners fell behind, resulting in punishments, reduced diet or loss of marks, prompting intense feelings of mental anxiety.Footnote 162 Experienced prisoners shared ‘tricks’ to mitigate hard labour; one prisoner advised ‘One Who Has Tried It’ on how to ride the treadwheel, ‘to sway the body from right to left’ and allow the ‘rising wheel to assist the upward movement’, and explained he should use a nail, smuggled into the cell, for oakum picking.Footnote 163
Prisoners’ capacity to withstand hard labour was also related to their physical condition when committed, and in the late nineteenth century, prison staff and penologists commented on a marked deterioration in prisoners’ physical and mental states, with many ill-equipped to withstand the regime. The Liverpool Visiting Justices estimated that 10 to 15 per cent of prisoners were ‘unfit for hard labour of first class on account of bodily health’.Footnote 164 Considering the zeal at Liverpool for the new prison regime and for maximising the use of the treadwheel, this may have been a conservative assessment. Dr Francis Archer, Surgeon at Liverpool, who was responsible for assessing all prisoners, noted in 1869 that one-fifth of prisoners – 399 out of 2,023 – sentenced to hard labour on the treadwheel were unfit and excused from hard labour on medical grounds.Footnote 165 Acknowledging that hard labour at Liverpool was of a ‘more severe character’, Archer and Governor Jackson did not introduce the new dietary scales proposed by the Carnarvon Committee.Footnote 166
At Wakefield Prison, the ‘physical tests’ introduced by the Visiting Justices to assess the condition of prisoners demonstrated they ‘were now in feebler condition, bodily and mental, than had been the case some years back’.Footnote 167 In 1871, the prison surgeon reported prisoners’ health as ‘good’, noting only ‘one suicide, three pardons on medical grounds, and three cases of insanity’, who had been found insane after admission and removed to a lunatic asylum.Footnote 168 Three years later, there were two suicides, and twelve removals to the lunatic asylum, an increase from ‘an average of three for the previous seven years’.Footnote 169 At Liverpool, the prison surgeon reported ‘11 deaths from natural causes, and one case of suicide by hanging, and three pardons on medical grounds’ in 1876.Footnote 170 The General Prisons Board also commented on the impoverished state of Irish prisoners in the 1870s, noting their poor physical and mental conditions and linking them to bad harvests and the agrarian distress of 1879 and 1880.Footnote 171 In 1886 Dr Hercules MacDonnell noted that
our criminals suffer from periods of semi-starvation, prolonged fits of intoxication, bad housing, clothing, and many other hygienic defects, it can be readily understood why prison regime does not cause any appreciable deterioration. Cleanliness, regularity, and a sufficiency of food account for this.Footnote 172
Similar comments were made about ‘the deterioration of female criminals’ in the late nineteenth century, with Miss Pumfrey, Lady Superintendent at Winchester convict refuge, acknowledging in 1878 that most of her charges were habitual criminals ‘the residuum … of the criminal population’.Footnote 173 In Liverpool particular concern was expressed at the persistently high numbers of female admissions, well over half, 12,518 of the 21,602 admissions in 1884.Footnote 174 Efforts to rehabilitate ‘unhardened’, young female prisoners centred on releasing them into female refuges run by religious orders. At Liverpool Nugent, inspired by his campaign to protect young women against ‘vicious lives’, removed Roman Catholic women to a Magdalen Asylum run by the Good Shepherd religious order and to similar institutions in Canada.Footnote 175 Towards the end of their sentences, women were transferred to the convict refuges at Winchester and Goldenbridge, Dublin, run by Protestant and Roman Catholic religious orders.Footnote 176 While the refuges in England only held prisoners, a ‘principal point’ of the Goldenbridge institution was that convict women mixed with women who had never been sentenced, a system Du Cane doubted to be beneficial for the ‘free’ women.Footnote 177
Refuges were intended to imitate the workings of the intermediate prisons for men, with the women prepared for release through work.Footnote 178 In England female convicts were transferred to refuges nine months prior to discharge while in Ireland they were transferred for a sixteen-month period. The Sisters of Mercy, the order that managed Dublin’s Goldenbridge refuge, refused the admission of infirm convicts from Mountjoy on the grounds that physical illness added to the difficulties in reforming women, while the burden of accommodating sick, infirm prisoners added to expenses.Footnote 179 Such women, apparently small in number, were released on licence, which Barlow implied was preferable to languishing in a refuge too infirm to work.Footnote 180 Even with the establishment of female refuges, opportunities for reform and rehabilitation were limited, especially as most women served short prison terms.Footnote 181
Given the enfeebled condition of male and female prisoners, medical officers questioned the utility and impact of repeated punishments for misdemeanours and bad behaviour in terms of prisoners’ mental health. They queried whether repeated punishments were an effective means of forcing prisoners to amend behaviour, or of convincing them to accept imprisonment as an appropriate sanction for their crimes. Medical officers adjudicated on prisoners’ fitness to undergo punishments, including the implementation of bread and water diets, confinement in dark cells and inflicting corporeal punishment while also guarding against unnecessary cruelty. Prison visiting justices, governors, surgeons and chaplains were required to be alert to the ‘mind or body of prisoners[s] injuriously affected by discipline or treatment’, while at Liverpool the governor was to ‘see that all insane prisoners are removed from prison as speedily as the law allows’.Footnote 182 As the 1867 medical commission on diet in Irish prisons noted, however, the speed with which prison doctors and others intervened to protect the mental and physical health of prisoners was determined by rules that permitted them to do so only when injury or impairment had been inflicted.Footnote 183
In 1866, Dr Robert McDonnell at Mountjoy Male Prison, who would later describe himself as leaning ‘too much towards the side of humanity’, argued that prolonged punishments could have a ‘maddening effect’, the prisoner is ‘irritated by it; and if there is any tendency to mental disease, this irritation becomes highly injurious’.Footnote 184 Chaplain Cody, commenting on the decline in the number of punishments in 1869, noted: ‘to punish a man for petty infractions of rules, arising from human infirmity, inadvertence, strong provocation, or other extenuating cause, has an evil effect on the minds of the majority of the convicts. When the prisoner was treated like a man, and he conducted himself like a man; he was docile and manageable.’Footnote 185 Often prisoners who attempted suicide had been repeatedly punished for disruptive behaviour, including earlier suicide attempts. Patrick Byrne, a twenty-one-year-old prisoner who commenced his sentence of six months’ hard labour for larceny at Clonmel Prison on 2 June 1887, committed suicide one month later by hanging himself with a bed strap tied to one of the bars of his cell window. He had been placed on a punishment diet on five different occasions in June for talking to other prisoners. The coroner’s inquest found that he had been temporarily insane at the time of the attempt although the medical officer did not refer to any abberant behaviour in his report.Footnote 186 These difficult and disruptive prisoners refused to comply with prison discipline, and were repeatedly punished, sometimes over several years. While a minority of cases were transferred to asylums, for the most part they were suspected to be cases of malingering and carefully observed by the medical officers.Footnote 187
The difficulties faced by prison medical officers in managing disruptive and dangerous behaviour among prisoners, often related to mental illness, were highlighted in an inquest report into the death of a convict at Spike Island in 1870. The convict had died of ascites, and, according to the report of the Medical Press and Circular, the jury had expressed, ‘in the strongest terms, their “total disapproval of the frequent punishment he suffered in cells, on bread and water for several days in succession, during his imprisonment in Spike Island”’.Footnote 188 The unnamed convict had been transferred by McDonnell from Mountjoy Prison as unfit for cellular discipline, but not as an ‘invalid’ although he had been suspected of suffering from epilepsy. McDonnell had kept him in the prison infirmary for several months as the ‘only means of keeping him from the system which might have been injurious to him’.Footnote 189 Defending the actions of Dr Jeremiah Kelly at Spike, the Medical Press and Circular noted that Kelly had not received the ‘convict as a sick man, nor had he any reason to know that he was unfitted for the usual bread-and-water discipline of Spike Island’.Footnote 190 The article also reflected on the difficult position of Kelly and McDonnell in relation to the prison authorities when advocating for or protecting the health of their charges. Citing the example of McDonnell, described as ‘an inconveniently compassionate medical officer’, who, they argued, had been removed from his position at Mountjoy for the ‘fearless discharge of his duty’ in defending untried Fenian prisoners from excessive punishment, the article speculated that the same fate might befall Kelly had he countermanded orders to punish the convict. The jury’s censure of Kelly, ‘for undue severity of punishment’, provided, they argued, the opportunity for prison authorities ‘to shift their responsibility to Dr Kelly and expurgate themselves by throwing him overboard’.Footnote 191 The article sought enhanced protection for prison medical officers who, in discharging their duties and responsibilities in relation to prisoners, were liable to be ‘McDonnellized’ or made to ‘suffer for official sins’.Footnote 192
The new rules introduced after nationalisation heightened the anxieties of Irish prison medical officers who argued that the regulations further compromised their capacity to protect the ‘health of prisoners under their charge’.Footnote 193 In a submission to the 1884 Royal Commission on Irish Prisons, the Association of Gaol Surgeons highlighted the tension between surgeons’ responsibilities to their prisoner patients and ensuring the disciplinary function of prison sentences was not ‘unduly mitigated’.Footnote 194 They also emphasised the potential damage to professional reputations should they miss cases of malingering.Footnote 195 The Association’s Honorary Secretary, Dr Hercules MacDonnell, expanded on these points in his address to the Statistical and Social Inquiry Society of Ireland in May 1885, which was also forwarded to the General Prisons Board and published in the Daily Express.Footnote 196 MacDonnell stressed that while ‘neither the diet nor surroundings should be such as to make imprisonment agreeable … punishment should not include cruelty, nor should it impair health’.Footnote 197 In his review of prison regimes in Belgium, Germany and Italy, published in 1886, he reiterated the point that ‘Punishment must be deterrent. Loss of personal liberty and deprivation of all usual enjoyments act under this head. Under no circumstances should this partake of the character of vengeance.’Footnote 198
As shown in Chapter 2, allegations of cruelty, abuse of power by prison officials and severe punishments, involving excessive infliction of crank work, repeated floggings and dangerous restriction of diet, resulting in several suicides, were unmasked at Birmingham and Leicester Gaols in the 1850s. While casting a long shadow over the nineteenth-century prison, the scandals did not undermine support for the separate system or the authority of prison officers, and while prison officials such as Inspector Herbert P. Voules suggested the investigation would deter prison officials from over-severe measures, in case they faced ‘another Birmingham inquiry’, there were other instances involving severe implementation of disciplinary regimes.Footnote 199 At Liverpool, punishments become more commonplace, and the annual report for 1869 listed ‘stoppage of diet’ for 818 male and 35 female prisoners, alongside confinement in solitary or dark cells for 579 males and 1,131 females and whipping for six male prisoners.Footnote 200 The Wakefield justices noted that there had been no cases of corporal punishment for prison offences for seven years despite the steady rise in committals, especially cases of drunkenness. However, in 1876 there were 453 punishments by bread and water in dark cells, and 1,305 by bread and water in light cells.Footnote 201 In the annual report for 1876 they noted ‘three punishments by whipping, 2,386 by solitary or dark cell, and 553 by stoppage of diet’ were carried out that year. Though only two were reported to be insane on committal, eight prisoners were removed to lunatic asylums and there were 47 deaths in the prison.Footnote 202
After nationalisation, punishments could entail confinement in punishment cells, dietary punishment, birching, deprivation of marks and demotion of prisoners who, through good behaviour, had progressed through the various stages or classes. Medical Officer Dr Quinton supported the implementation of dietary punishments for ‘unruly prisoners’, acknowledging that he knew ‘nothing approaching a scientific excuse for its use, except the principle upon which a horse has its oats reduced in order to tame his spirit’.Footnote 203 In Ireland, the numbers punished for offences between 1878–79 and 1879–80 rose from 10,475 to 13,304, a significant increase according to the General Prisons Board. The Board speculated that it was caused by ‘the exercise of a closer supervision, and the enforcement of a stricter discipline, and an increased amount of industry, as the officers have become more familiar with the operation of the new rules and system’.Footnote 204 Under the new regulations ill-conducted or idle prisoners could be placed on a bread and water diet for three days only followed by an interval of a ‘stirabout’ diet and then returned to the bread and water diet. Officially, the period on punishment diets was not to exceed fifteen days and such prisoners were not required to perform labour.Footnote 205
Incorrigible and disobedient prisoners, who refused to work on the treadwheel, were flogged or birched. In 1887 Surgeon Hammond at Liverpool ordered prisoner Joseph Leeane be given twelve strokes of the birch rod for refusing to work at the wheel. Leeane argued his sentence was unjust and insisted hard labour was not ‘proper punishment’ for his crime of begging.Footnote 206 Hammond frequently rejected prisoners’ requests for mitigation on grounds of poor health, declaring prisoners fit to work on the wheel and being quick to punish prisoners he suspected of feigning insanity.Footnote 207 As discussed in Chapter 5, prisoners went to great lengths to secure mitigated conditions, including feigned suicide attempts. On 26 May 1893, a sixteen-year-old prisoner, James Allender, undergoing a sentence of nine months’ hard labour, was threatened with further birching if he made a second attempt at suicide. On the first attempt he tried to hang himself with a rope made from oakum, and when found assaulted the warder, insisting he would ‘break a pane of glass and then cut my throat’. On inquiring into the incident, Allender admitted to the Governor he ‘never intended to do anything to myself as sure as there is a God in Heaven’. His punishment was twelve strokes with a birch rod, and Dr Beamish, the prison medical officer, commented that Allender was ‘not strong but was fit to be birched’.Footnote 208
By the late nineteenth century, there was growing distaste for corporal punishment and the infliction of pain, on moral as well as rational grounds, and by the time of the Gladstone Committee of 1895, the view that ‘every form of punishment is objectionable’ was more widely endorsed.Footnote 209 By then, the use of the ‘entirely dark cell’ had been discontinued in Ireland and there was evidence of a decline in corporal punishments in local prisons after 1893.Footnote 210 While the Report of the Gladstone Committee opposed corporeal punishment, especially in the case of habitual criminals, individual prisons resisted these changes. In the case of Liverpool, a deputation of the Visiting Committee petitioned the Home Secretary, in July 1898, for permission ‘to retain the power to order such corporal punishment as hitherto allowed’.Footnote 211
II Medical Expertise and Knowledge Production
Medical Management of Mental Disorder in Convict and Local Prisons
Prison doctors, working in environments shaped by deterrence, adopted various treatment and management strategies when dealing with prisoners experiencing symptoms of delusion, mania and depression of spirits. These varied across the prison estates and depended on conditions within individual prisons and individual doctors’ practices. Prisoners were typically retained in prison while their mental states were monitored and assessed, moved in and out of prison hospitals, kept under cellular observation, or placed in cells with fellow prisoners who watched over them. These measures were not always successful; at Chatham prison, one convict committed suicide in the prison hospital, ‘under the eyes of … fellow prisoners’.Footnote 212 He had shown symptoms of melancholia for several days and had been admitted to the prison hospital for observation.Footnote 213 At Mountjoy, Dr James W. Young, McDonnell’s successor, assisted by the chief prison warder, closely watched those on probation for signs of mental distress. When ‘a tendency to insanity in a prisoner’ was observed, the warder reported the prisoner to Young, who, with the governor’s approval, authorised more ‘open air exercise’. Commenting on Young’s system of observation at the Kimberley Commission in 1878, convict E.F., who had been held at Mountjoy and Spike Island Prisons, claimed ‘dozens of men … who had been decidedly affected in the head, have by this simple arrangement been able to complete their sentence, learn a trade, and must have become good members of society’.Footnote 214 By the 1880s, the Prison Medical Inspector for Ireland was required to testify that prison medical officers implemented systems for observing prisoners and identifying those unfit for the regime.Footnote 215
Overburdened prison medical officers struggled to manage convicts and prisoners whose mental and physical decline was accompanied with eccentric, erratic and violent outbursts, particularly in England where prisoner numbers and the number of such cases were higher. Despite the impact on their workloads, the medical officers devoted time and effort to treating individual cases to halt further deterioration. Convict William Williamson, also known as John O’Hare, a forty-nine-year-old American, serving a five-year sentence for larceny at Mountjoy, was in poor physical condition on his admission in October 1882. Described as ‘spare’ in frame, he was transferred to Maryborough Invalid Prison in September 1885. His medical sheet, which travelled with him as he was moved around the prison estate, records an extensive list of weekly prescriptions intended to bolster his physical and mental health. By March 1887, Williamson was repeatedly fed with a stomach pump, as he was no longer eating, and he was transferred to Dundrum Asylum in April 1887.Footnote 216 Another convict, thirty-four-year-old James Slattery, serving a five-year sentence at Mountjoy, was described on committal in December 1881 as stout and strong. Following his removal to Spike Island, his health declined, he became ‘febrile’ and was diagnosed with bronchitis. He was then transferred to Maryborough Invalid Prison, as a ‘spare’ and ‘weak’ prisoner in October 1884; by then his weight had fallen from 160 to 141 pounds. Discharged from Maryborough in November 1885, he was back at Mountjoy in January 1887, and a month later was reported to be abstaining from food. After being fed with a stomach pump throughout February, he was discharged to Dundrum Asylum in April 1887.Footnote 217
This level of attention was not unique to the convict system or the smaller Irish prison estate. In July 1901 the Visiting Committee at Liverpool Prison heard a complaint from prisoner John Pearson about medical treatment for his bad chest. Pearson claimed he had not been ‘sounded’ and had received only ‘occasional doses of medicine’, though the Deputy Medical Officer, Dr Frank A. Gill, insisted he had visited Pearson forty-three times over three months.Footnote 218 At that time, the prison was dealing with many disruptive prisoners; male and female prisoners broke up their cells, were violent, refused to work, and assaulted officers.Footnote 219 Even so, prison staff explored several options to secure the safe removal of another prisoner, Albert Halliwell, who was reported to be an epileptic, including a medical discharge. Halliwell had not experienced any epileptic fits while in the prison, and the medical officer argued he could not certify him insane and remove him to an asylum. In an effort to resolve the question of Halliwell’s care, Liverpool officials contacted the Prison Commission enquiring whether it would bear the cost of 7 shilling 6 pence a week to pay for his care at an epileptic colony near Liverpool. The colony was full and instead it was suggested that Halliwell be pardoned on medical grounds and transferred to a ‘suitable home’. By June 1905, however, it was reported that a suitable destination for Halliwell could not be found and it is unclear whether he was discharged on medical grounds without accommodation.Footnote 220
Prison medical officers also conducted detailed investigations into attempted suicides. These provoked great concern among prison officers as they indicated a failure of the prison to safeguard its inmates. Mountjoy Prison saw frequent suicide attempts, though prisoners were often suspected of feigning.Footnote 221 The Governor of Galway Prison reported two separate suicide attempts in December 1884 and January 1885. One of these, John Burke, protesting against the prison diet, tied his trouser braces together, and fastened one end to the handle of the bell in his cell and the other tightly round his neck. Burke, who was on the first scale of the third-class diet, had complained of hunger to Medical Officer Dr R.J. Kinkead, who on weighing him concluded that he had gained five pounds while confined. Kinkead insisted that Burke’s suicide attempt was not genuine but carefully staged to ensure he would be seen, and was an attempt to secure ‘increased diet, or to be placed in association’.Footnote 222 While it is unclear what happened to Burke, his suicide attempt prompted the medical officer to recommend that bell handles be removed from prison cells and replaced with electric bells. Kinkead also suggested the hooks and chains that supported hammocks be replaced with ‘solid supports from the wall’.Footnote 223 The ubiquity of suicide attempts led the Chairman of the General Prisons Board to order safety netting for local prisons in 1885, particularly for institutions where ‘gallery railings are not sufficiently high to prevent prisoners committing suicide’.Footnote 224
As Halliwell’s case suggests, a small number of prisoners, in a poor condition and with little hope of improvement, were eventually discharged on medical grounds. Chapter 2 has investigated the caution surrounding medical discharges at Pentonville in the 1840s, and by the late nineteenth century, pardoning and releasing prisoners on medical grounds was still unusual. In 1891, for example, only one convict was released from Irish convict prisons on the grounds of physical illness, while six were transferred to the Dundrum Criminal Lunatic Asylum.Footnote 225 These cases received only a perfunctory reference in official records. In 1884 the prison inspectors deftly noted two male and nine female prisoners were pardoned on medical grounds at Liverpool Prison, while in 1885 twelve prisoners were discharged on medical grounds, though no details were given.Footnote 226 When details were noted, life-threatening physical ailments such as respiratory or heart diseases were recorded and women were also discharged in the final months of pregnancy.Footnote 227 In 1886 Dr Gover estimated that the rate of medical releases among convicts was only 1.9 per 1000.Footnote 228 Objecting to such releases, he claimed prisoners survived for longer periods when retained in prison hospitals, as most were discharged without resources or into the care of relatives with limited means.Footnote 229 In Ireland, authorisation for medical releases was at the discretion of the ‘Judge of the Court by whom such Prisoner was committed’, and in June 1880 the General Prisons Board felt compelled to remind Kilmainham Prison’s Medical Officer of the regulation, suggesting that releases had taken place illegally.Footnote 230
While prison medical officers devoted significant time to assessing and managing prisoners’ physical health, the ubiquity of mental breakdown among prisoners added significantly to their workload. It involved differentiating between a range of complex symptoms, keeping prisoners under medical observation in prison hospitals, or in individual cells with other inmates for weeks, sometimes months. Campbell reproduced some of the conditions of a lunatic asylum at Woking, including a hospital diet, sometimes supplemented by extra items, close attendance of inmates, and provided insane prisoners with books and crafts to occupy them. He noted that such occupation occasionally resulted in cures and prisoners were returned to convict prisons.Footnote 231 For some prison doctors, however, holding potentially insane prisoners in prison was undesirable. Dr Hercules MacDonnell, for example, expressed concern about the lengthy detention of the insane in prisons lacking provision for care and specialised medical treatment.Footnote 232
In England, convicts showing symptoms of insanity were removed to Millbank, which was utilised as a form of collection and assessment centre for the close observation of such prisoners, and, as discussed in Chapter 5, to check for signs of feigning. Criticising the length of time convicts were kept at Millbank – up to three to four months during which time the convicts had no employment – the 1878 Kimberley Commission insisted that the detention period be shortened and convicts required to work, especially as ‘one third’ of those sent there were ‘found not to be really insane’.Footnote 233 Following a period of medical assessment at Millbank, these convicts were then removed to different institutions; for example, among 54 convicts under medical observation at Millbank in 1861, nine were removed to Bethlem Hospital as insane, fifteen to invalid prisons, nine kept in association on medical grounds, five removed to able-bodied prisons, and a further nine remained under medical observation. One Irish convict, returned to Millbank from Bermuda owing to his mental condition, was subsequently sent on to Spike Island.Footnote 234
The removal of prisoners showing signs of mental disorder to public works prisons and invalid prisons burdened prison medical officers with the difficult task of distinguishing those inmates who were unfit for or unable to withstand the full rigour of prison discipline from the ‘truly’ insane. Unlike prisoners certified insane, those diagnosed as weak-minded or invalids were retained in prison, although the full rigours of the separate system of confinement and hard labour were ameliorated. Significant numbers accumulated; Dr William Guy, reported that some 200 convicts ‘unsound in mind … and yet not deemed quite fit for the lunatic asylum’ were confined at Millbank in 1869.Footnote 235 Divisions or wings of individual prisons served as repositories for mentally ill prisoners at various points during the late nineteenth century, including Woking Invalid Prison, which opened in 1859, and where, in 1874, a separate wing was designated for male lunatic convicts to alleviate pressure on Broadmoor. Prior to that only a small number of prisoners with mental diseases were transferred there; Campbell noted only fifteen cases during 1863.Footnote 236 Woking and Parkhurst contained specific divisions devoted to accommodating weak-minded and ‘imbecile’ convicts. Parkhurst, a prison for juveniles from 1838 to 1863, catered for prisoners invalided as weak-minded or imbecile from 1869; by 1882 there were around 140 prisoners confined at Parkhurst.Footnote 237 Woking Invalid Prison remained the main repository for invalid convicts in the late nineteenth century. According to Campbell, by the 1870s there were almost 200 mentally ill prisoners, the majority weak-minded, in the prison.Footnote 238 Owing to concerns about the legality of retaining the insane in prisons, the wing catering for male lunatic convicts at Woking was closed in 1888.Footnote 239
In Ireland, after 1855 weak-minded convicts were deposited in Philipstown Prison, and, following its closure, by December 1863 they, along with the aged and other invalid prisoners, had been removed to Spike Island, which held 901 convicts in that year.Footnote 240 In 1861, when Philipstown was scheduled for closure, there were ten certified lunatics awaiting accommodation at Dundrum among the 145 convicts, and ‘large numbers of invalid and other prisoners labouring under deficient intellectual powers with great irritability and total destitution of self-control’.Footnote 241 Dr Maurice Corr, Medical Superintendent at Spike Island, noted that in some cases the illness had ‘commenced with curable weakness of intellect, and terminated in dangerous incurable insanity’, insisting that the growth of ‘mental disease’ had been ‘generated and fostered in prison’.Footnote 242 Weak-minded convicts were usually separated from other convicts at public works prisons such as Spike Island and Dartmoor, a practice endorsed in the Report of the Kimberley Commission in 1878 following the presentation of evidence that the eccentric behaviour of the weak-minded prisoners aggravated the other inmates.Footnote 243
In 1872, as invalid prisoners accumulated in Spike Island, prison inspectors and officials sought alternative, separate accommodation for them. Their proposals included the construction of a purpose-built building at Spike Island, erecting two iron huts in Mountjoy Male Prison garden, and redesignating Smithfield Prison in Dublin as a dedicated invalid prison similar to Woking.Footnote 244 Though these proposals were not implemented, Inspector Barlow and Crofton persisted in advocating for a separate institution for weak-minded convicts, and by 1878 the local prison at Maryborough was repurposed as a prison for invalid, weak-minded and imbecile male convicts. In 1884 the Royal Commission on Irish Prisons specified that in ‘every case where there are unmistakeable signs of disease, mental or bodily, such as would warrant transfer to an invalid prison, the convicts should be at once moved to Maryboro’, so that the disease may be checked in its earlier stages’.Footnote 245 From July 1885, Maryborough was constituted solely as an invalid prison for male convicts, having ceased to operate as a local prison, although by 1887 the prison also housed convicts removed from the recently closed Lusk Intermediate Prison.Footnote 246 Among the 57 convicts held at Maryborough on 31 March 1886, thirty were serving penal servitude sentences and another ten were serving life sentences, suggesting that most had been in separation for a portion of their sentence.Footnote 247 Campbell also noted the ‘great number’ of invalid prisoners at Woking who had been subjected to ‘long-continued solitary confinement’. Describing the ‘ulterior effects’ of the separate system to be ‘in many cases, most injurious’, he recalled that convicts who had been subjected to the regime frequently ‘gave evidence of impairment both bodily and mental, marked by great depression, a semi-idiotic expression and the dilation of the pupils’.Footnote 248
Weak-minded or imbecile convicts comprised the largest group of ‘mental cases’ at Woking; in 1861, among its 786 convicts, Woking received 130 such cases from Millbank and a further 116 from Dartmoor.Footnote 249 While ‘pretty manageable’, Campbell reported that they also displayed eccentric habits, were liable to fits of excitement and to break out.Footnote 250 Convicts invalided owing to physical conditions also suffered from ‘impairment of mental facilities’, and at the temporary Invalid Convict Depot at Lewes, established in 1857, the medical officer noted in 1860 that ‘the mental faculties of most of the paralysed men were a good deal impaired’.Footnote 251 Convict M.E. at Lewes, for example, was suffering from ‘paralysis and debility’ when received in 1859. The medical officer described his habits on admission as ‘dirty’, and he walked with difficulty. As his mental condition deteriorated, he became noisy, violent and excitable, experienced delusions, such as ‘fancying himself the proprietor of large estates’, and he was eventually removed to a lunatic asylum.Footnote 252 Aged and infirm convicts were ‘frequently very peculiar and eccentric’, while those reported to have dementia were said to become violent, intractable and disruptive, prompting their removal to asylums.Footnote 253 In 1863 Campbell transferred nine such cases to the private lunatic asylum, Fisherton House.Footnote 254 Among those invalided for physical ailments, he contended that their persistent insubordination, violence and other conduct was inconsistent with sound minds.Footnote 255 While at Woking convicts with ‘disorders of the intellect’ required constant medical supervision, including those whose mental and physical health improved under the regime. Some invalided convicts were noted to be quiet and amenable for long periods, yet liable to ‘break out when least expected’.Footnote 256 Campbell regarded the physical and mental diseases of invalided convicts to be linked to their criminality, a product of ‘depraved habits, intemperance, and hereditary predisposition’ and their long careers in vice and crime, alongside their bad tempers and disgusting propensities, rendered them more unmanageable than ordinary lunatics.Footnote 257
The burden on medical officers employed at the large public works prisons, such as Spike Island and Dartmoor, and at invalid prisons, was especially heavy, owing to the sheer numbers and categories of prisoners held there. John Campbell, when Medical Officer at Dartmoor Prison in the 1850s, claimed healthy men were a minority.Footnote 258 Dr R.E. Power, who had been Assistant Surgeon at Portsmouth Prison for five years, and then Medical Officer at Dartmoor, where he supervised an assistant surgeon, dealt with nearly 1,000 convicts, as well as ‘500 women and children’ and 200 officers.Footnote 259 Conditions at the public works prisons were exacting and severe, with healthy prisoners working in association outdoors for long hours at heavy labour, excavating earth, quarrying and undertaking other arduous tasks. Invalid prisoners, including the weak-minded, were usually employed at ‘sedentary’ tasks.Footnote 260 Defending conditions at Dartmoor, with its damp, foggy and stormy climate, Campbell insisted that the invalid class, ‘greatly enfeebled by long standing diseases’ and possessed of constitutions undermined by ‘intemperance and other depraved habits’, benefited from the ‘elevated position’ of the moor.Footnote 261 He described the regulation that required medical officers to classify prisoners according to fitness for different kinds of work, as a tax on medical men’s knowledge and expertise because of the ‘diversity of … physical and mental condition’ and the large number of prisoners.Footnote 262 He also sought increased allowances of food for men at public works labour, to ‘compensate for the wear and tear of the body’.Footnote 263 Austin Bidwell, sentenced to penal servitude for life in 1873, and transferred to Chatham prison after a year in separation at Pentonville, described his amazement when he first witnessed a convict work party: ‘their famished, wolfish looks – thin, gaunt and almost disguised out of all human resemblance by their ill-fitting, mud-covered garments and mud-splashed faces and hands … the weary, almost ghastly spectre march I had witnessed constantly haunted me’.Footnote 264
Labour at these prisons was often enforced through punishment and prisoners were frequently suspected of malingering. The evidence of convict E.F. to the Kimberley Commission highlighted the brutal treatment of convicts at Spike Island and the deleterious impact on convicts’ minds. E.F., convicted in 1875 and released early on medical grounds in 1878, claimed punishments were ‘the order of the day at Spike Island’ and prisoners were threatened, starved and flogged. He described the prison staff at Spike as ‘inferior’ to those at Mountjoy, and in their interactions with prisoners, ‘more irritating and annoying, and growling at [prisoners] unnecessarily’.Footnote 265 He dismissed Medical Officer Dr Patrick Kelly as a ‘dispensing doctor’ who inflicted ‘inhumane cruelty’ by placing ‘poor maniacs in perpetual cells until reason had become undermined from hunger, flogging and deprivation of the air of heaven’.Footnote 266
Labelling, Taxonomies and Knowledge Production
Drawing on their work assessing, diagnosing and managing numerous cases of mental disorder, medical officers increasingly laid claim to extensive and unique expertise in understanding mental illness in the context of the prison. Some, including Gover, Campbell and notably Nicolson, published on the topic, producing a sizeable body of literature. They critiqued the expertise of asylum doctors, including their evidence in court, and argued that their experience enabled them to distinguish between true and feigned insanity. As prison psychiatry emerged as a discrete field of activity and prison doctors asserted their expertise, they developed a separate taxonomy to describe the range of mental conditions they encountered in prisons. Their concern was primarily diagnosing and labelling the conditions they observed, and less with treatment, although some prisoners were reported to have recovered while in the prison hospital and the timely removal of convicts out of separation could limit the damage inflicted on the minds of prisoners. In 1867 McDonnell described two prisoners, who he noted to be ‘“dangerous,” and of frenzied passion and irritability’, who had been ‘reclaimed’ by removing them to the prison hospital, where they received ‘judicious moral and physical treatment’.Footnote 267
The emergence of a discrete language and set of categories to describe the minds of prisoners can be traced to the years following the introduction of separate confinement. Thereafter prisoners, whose violent and erratic behaviour prompted speculation among staff about their mental state, were recorded and described by prison surgeons in specific terms. Prisoners were noted to be ‘sullen’, ‘irritable’, ‘obstinate’, ‘passionate’, ‘impatient’ and ‘dull’, as well as delusional.Footnote 268 At Pentonville ‘irritability’ was used to denote a more general prevailing mood among the convicts and within the prison, as well as the absence of self-control in individual cases. In his report for 1849 Dr Owen Rees described, in reference to the general condition of the prisoners, ‘that there is an “irritability” observable which I have never before observed in men confined’.Footnote 269 In 1855 Governor Grace at Philipstown also noted the ‘troublesome state’ of the prison, which he linked to the irritable, violent and uncontrollable passion of prisoners, including juveniles.Footnote 270 Conditions of the mind were closely observed and recorded; at Pentonville prisoners demonstrated ‘sullen obstinacy’, a combination of ‘cunning and weakness’, ‘knavery and almost imbecility of mind’, while those removed from Mountjoy to public works prisons on medical grounds had ‘great nervousness’, ‘irritability’, and were ‘exciteable’ and ‘eccentric’.Footnote 271 John Daughton, an eighteen-year-old convict who had spent nine months in separate confinement in Mountjoy Prison, and then transferred to Philipstown in February 1858, was described by the medical officer as ‘sullen’, ‘morose’ and ‘very eccentric’, while Andrew McQuirk, imprisoned in January 1861, was reported to be ‘excitable, ‘mischievous’ and ‘irritable’.Footnote 272 Medical officers commented on the condition and health of the minds of prisoners who persistently broke rules, yet seemed indifferent to repeated punishments. In considering suicide attempts, McDonnell related the case of prisoner J. Murphy, who had become excited, refusing to declare his religious denomination. He was sent to the punishment cell on a bread and water diet, and McDonnell ‘soon satisfied myself that the prisoner was not insane, but simply irritated to an extreme degree by a punishment that did not appear just to him’.Footnote 273
The labels used to describe women reflected the gendered conceptualisation of mental disorder and criminality. Women’s ‘irritability’ involved ‘a restiveness and a longing for some change or variety of circumstance’ that could only be gratified through misconduct.Footnote 274 David Nicolson commented that the ‘unreasonable acts of destruction’ committed by women in prison ‘doubtless arise strange and pleasurable feelings of a triumphant nature’ as the prisoner was ‘temporarily in command of the situation’.Footnote 275 The violent outbursts of female prisoners, referred to as ‘breaking out’ in English prisons, perplexed and disturbed prison medical officers. In Ireland prison doctors noted similar behaviours among women, although use of the phrase ‘breaking out’ was not widespread. In 1873 Nicolson commented that ‘Female convicts are not only liable to give way to destructive emotions when disappointed or irritated; but they afford, in what has been termed their “breakings-out”, an illustration of a state of mind whose aspect is even more distinctly morbid’ than among male convicts.Footnote 276 This violence was distinguished in the opinion of prison doctors from that observed among female patients in lunatic asylums, consisting ‘of a frantic outburst, in which destructiveness is the main feature, a special partiality being displayed for the shivering of window panes and the tearing of blankets and sheets into fragments’.Footnote 277
In his evidence to the 1878 Kimberley Commission, Dr Henry Westwood Hoffman detailed his management and treatment of women considered to be ‘bordering on insanity’ at Fulham Female Refuge, where women worked in association following transfer from Millbank and Woking (Figure 3.3). Drawing on the example of convict Hughes, who, he argued, was not of sound mind yet at other times was ‘perfectly rational’, Hoffman explained that despite her difficult behaviour she was not a fit case for punishment or suitable for transfer to Millbank. Hughes was ‘quarrelsome, irritable, jealous, and not amenable to discipline’, and, while she did not suffer from delusions, he argued that when she ‘breaks out, she is not responsible’.Footnote 278 She had been sent to two lunatic asylums for treatment, one of which was Broadmoor, but when her behaviour ‘passes off’ she was released. While he could not decide whether Hughes was insane he did not suspect her of feigning insanity.Footnote 279 Despite his heavy workload, Hoffman was reluctant to request a second opinion from Millbank’s medical officers, insisting his locum tenens provide it.Footnote 280 As discussed in Chapter 5, prison doctors alleged that women planned these destructive outbursts, which were prompted not by ‘provocation, angry excitement or disappointment’, but by a desire for change.Footnote 281 That these destructive impulses were more often provoked by trivial causes among women, Nicolson argued, was ‘attributable to functional causes which present themselves in connection either with the normal menstrual flow or with its derangement’ and women’s need for companionship with some prisoners deliberately ‘getting into trouble in order that she may be near to her “pal”, and bear her company in punishment’.Footnote 282 While their behaviour was regarded as outrageous, manipulative and distinctly unfeminine, it could also be interpreted as an expression of women’s agency and resistance to the prison environment and routine .Footnote 283

Figure 3.3 Woking Convict Invalid Prison: a woman prisoner in solitary confinement. Process print after P. Renouard, 1889
In developing a distinct set of categories to explain such mental conditions and psychiatric states, medical officers linked criminality and criminal behaviours with prisoners’ apparent inability to adapt to, or benefit from, the discipline of the prison. They also drew on specific characteristics and dispositions, as well as environmental factors, commonly evoked in general rhetoric on criminal behaviour in the late nineteenth century. Consequently, prison psychiatric categories were connected to familiar tropes that characterised criminals as inherently violent, quick tempered, duplicitous, sly, lacking in self discipline and control, and childlike. In 1870 Gover argued that among female prisoners with symptoms of mental distress ‘hereditary defects’ were ‘doubtless … aggravated by the influence of bad example and vicious training’, and mental illness caused by a loss of self-control and excess passion.Footnote 284 When assessing the case of convict Richard Murphy, alias Thomas Doyle, who had ‘feigned’ suicide in his cell, McDonnell at Mountjoy concluded that Murphy belonged to
that class of cases which are unquestionably of a nature most difficult for a medical man to deal with … cunning, deceitful, passionate, and impatient of control yet in my judgement having naturally bad disposition complicated by a certain admixture of disease which tends to make the mind more fretful, irritable, and uncontrollable … such disease should be treated as firmly yet as gently as the circumstances … will admit.Footnote 285
Murphy’s ‘cunning’ and deceitfulness were simultaneously characteristics of his criminality and of his mental condition. While disciplined and punished for their ‘criminal’ traits, the behaviour of these inmates also prompted medical officers to debate the impact of frequent punishment on the minds of prisoners, and to explore the relationship between punishment and prisoners’ mental capacity to improve and comply with prison rules. At Mountjoy, McDonnell warned against punishing prisoners in cellular confinement suffering from forms of ‘mental disturbance’ that fell short of ‘insanity’, arguing such treatment resulted in them becoming ‘irritable, peevish, sullen, morose and gloomy, liable to burst into passion on the most trifling provocation, fancy everyone to be an enemy and quite unable to control their bursts of frenzy’.Footnote 286
Highlighting the cases of two convicts, J. Croughwell and Patrick Maher, McDonnell insisted repeated punishments had not only failed to improve their behaviour, but had also led them into the ‘most miserable condition’. Such convicts, McDonnell argued, fancied that they were ‘without a kindly feeling from anyone; wronged and misunderstood by all the world; friendless and in despair. This is doubtless the condition which leads onto suicide.’Footnote 287 Convict Croughwell, fifteen years old when he was convicted of robbery in October 1851, was originally sentenced to ten years, and then given an additional four years’ penal servitude for assaulting a prison officer. His conduct was reportedly very bad, and he acquired a spectacularly long punishment sheet.Footnote 288 Between November 1857 and May 1859, he attempted suicide three times, and, while repentant and well behaved in hospital, McDonnell felt he was not fit for the disciplinary regime at Mountjoy and recommended he be removed to an associated prison.Footnote 289
In the case of Patrick Maher, who attempted suicide in June 1863 and was violent towards the warders, McDonnell first placed him in a padded cell and then transferred him to the prison hospital. McDonnell concluded Maher’s life was not in danger, and that he was sane and fit for punishment. When dealing with such cases, however, McDonnell argued that the wrong type of punishments prompted or exacerbated morbid feelings, leading to further suicide attempts. ‘The slow class of punishment’, such as the curtailment of diet or close cellular confinement, made ‘a prisoner like Maher moody and sullen’.Footnote 290 Punishments ‘of short duration’, including corporal punishment, were more suitable as it was less likely to contribute to mental disorder.Footnote 291 ‘Viewing punishment in its medical aspect (psychological)’, McDonnell argued that prisoners should believe the punishments inflicted on them were fair, commensurate with the misdemeanour and deserved. In the absence of ‘a clear conception of his guilt’, prison staff risked prompting mental distress among prisoners: ‘the punishment becomes an extreme source of mental irritation.… In the one case, he bears his punishment and is the better of it, in the other, he is irritated by it; and if there is any tendency to mental disease, this irritation becomes highly injurious.’Footnote 292
Campbell also warned against dietary punishments, especially when repeated frequently, and applied to weak-minded prisoners. Not only did these punishments fail to deter; they impaired prisoners’ minds and bodies, especially among those with a hereditary tendency to diseases such as scrofula, which laid the foundations for maladies of a fatal nature.Footnote 293 Contrasting the criminal or convict class with that of the habitual offender and semi-imbecile, Campbell argued that ‘encouragement and punishment seem alike ineffectual in restraining … [the] bad dispositions’ of the latter.Footnote 294 Nonetheless, medical officers argued there were some benefits in punishing such prisoners, and again these were understood in the context of their criminal natures. In 1873, David Nicolson justified punishments on the grounds that ‘fear in its moral aspect’ did not restrain prisoners; rather ‘the selfish fear or dread of physical chastisement and pain, more or less immediate, with which he will be visited’ was effective when managing volatile prisoners prone to emotional outbreaks.Footnote 295
Prison officers also questioned the efficacy of punishing female prisoners and their mental capacity to withstand punishments, while simultaneously expressing shock at their extreme and unfeminine behaviour. Reflecting on his time as Assistant Chaplain at Millbank Prison in the 1860s, Reverend James Francis noted the women there ‘were in a most excited, irrepressible condition; I never saw anything like it’.Footnote 296 He claimed the dark punishment cells were ‘continually full with raving, screaming women’ who were noisy and disruptive when excited, kicking on doors and disrobing sick prisoners held nearby.Footnote 297 Crofton contended that ‘irritable’ women, subjected to repeated punishments while in strict prison discipline, fared better when removed out of separate system and transferred to refuges.Footnote 298 Special measures were introduced to manage female convicts who were perceived to be especially unsuited for separate confinement. In 1869 Dr Young rejected the new dietary scales introduced in 1868, instead placing women at Mountjoy on a diet with greater quantities of milk and bread. He observed that ‘after long periods of confinement, [the diet] was loathed by the prisoners’ owing to the lack of variety, and ‘great quantities of the bread rejected. This led to insubordinate conduct, malingering, and punishment.’Footnote 299 From 1878 women at Mountjoy were kept in strict separation for four months, though specific measures were introduced to mitigate aspects of the separate regime, especially for women who were susceptible to extreme and volatile outbursts when punished.Footnote 300 Second-class female convicts were permitted to work and sit in their cells with the doors opened on alternate days, allowing them to observe prison activities. Women were also granted more generous remissions for good conduct than men.Footnote 301 Captain Barlow, Director of Convict Prisons, for example, was reluctant to cut women’s hair, a practice permitted for hygienic or disciplinary purposes, as he found it had a very negative effect; the women found it ‘very cruel’ and for some he feared it would make them ‘half mad’.Footnote 302
In England there was similar disquiet among prison doctors and staff dealing with female convicts and ambiguity concerning women’s capacity to endure the disciplinary regime. Hoffman at Fulham Female Refuge objected to placing women on bread and water punishments, arguing only ‘strong’ women could withstand it for more than two days and that women fared better in terms of behaviour and temperament on their usual diet while punishment diets ‘hardened’ women.Footnote 303 Superintendent Pumfrey at the Winchester Refuge complained that some women arrived in very enfeebled physical health as well as in ‘bad’ character, once again blending their medical condition with their alleged criminal dispositions. Describing one woman transferred to the refuge, Pumfrey noted how she ‘never knew her mother and was regularly dragged out of the slums’. She had behaved ‘very badly’ while in Woking Prison and arrived at Winchester in very poor health, which Pumfrey attributed to her being placed on punishment diet of bread and water, confined to the dark cells and with her ankles fastened together in ‘hobbles’.Footnote 304
By embedding contemporary ideas on the intrinsic deviant inheritance of criminals, and their poor morals and character, with psychiatric categorisations of mental illness and insanity in the prison context, medical officers, however, largely defended prison regimes, arguing they did not cause mental collapse among prisoners whose criminality was evidence of an inferior mental condition. They argued the expertise in identifying the traits and symptoms of this ‘admixture’ of criminality and insanity resided with them, with their extensive experience of observing both the insane and the criminal. As Wiener has contended, from the late 1860s English doctors in regular contact with criminals developed a scientific conception of the criminal, though their heavily inflected physicalist ‘scientific reinterpretation of criminality’ dissipated in the early 1870s.Footnote 305 Yet those working in prisons continued to speculate on the specific forms of mental disorders they encountered. Major Arthur Griffiths, Deputy Governor at Millbank Prison from 1870 to 1872, described the particular challenges of this work, contending that prisoners were liable to special and exclusive phases of insanity that included strange and intense delusions, religious mania, claims of persecution, exaggerated destructive tendencies, curious attempts at suicide and persistent feigning.Footnote 306
Dr David Nicolson, his experience built up at several convict prisons and subsequently Broadmoor, published his theories of the criminal mind in the 1870s. Wiener noted that Nicolson moved away from the ‘oversweeping claims of the physicalists’, which were present in the articles he published between 1873 and 1875, to a position from which he argued only a minority of criminals possessed distinctive physical characteristics.Footnote 307 In his understanding of delusions, Nicolson differentiated between ‘ordinary’ delusions experienced by all human beings and the ‘special delusions’ experienced by many prisoners. These arose in the particular circumstances of prison life, and Nicolson connected them with the irritable condition of the criminal mind.Footnote 308 Delusions of the ‘irritative type’ were most often found among prisoners, who claimed they were unjustly punished or treated, or believed their food had been poisoned. Such delusions, he argued, were more common in men than women, and expressed through vigorous resistance to authority, and demonstrations of resentment, threats, food refusal and ‘personal violence’.Footnote 309 Arising from ‘irritation and feelings of resentment’, these delusional prisoners were especially dangerous and careful precautions were advocated.Footnote 310 Prisoners’ minds were unable to withstand the ‘irksome experiences’ of prison life and disciplinary regimes, especially separate confinement, the pressure of ‘labour’ was distasteful, and eventually the ‘chronic grumble’ assumes ‘mastery’.Footnote 311 Nicolson insisted that through closely observing the workings of ‘diseased’ minds, prison medical officers and those experienced in prison psychiatry were able to study, test and sort ‘phenomena’ in the context of their uniform and standard prison experience, and develop new psychiatric knowledge beneficial to practice outside the prison.Footnote 312
Much of the debate on psychiatric conditions in prisons in the late nineteenth century occurred in the context of concerns about high rates of recidivism and habitual criminals. By the 1880s, official statistics suggested that the inexorable climb in criminality had at least slowed, if not halted, yet the reasons for persistence of criminal behaviour among some groups continued to preoccupy penologists and prison doctors. Though estimates vary, some reports suggest that between 1888 and 1892 recommittal rates to English local prisons rose to 48 per cent.Footnote 313 In Ireland among the 29,916 confined between 1879 and 1880, only 18,183 had never been in prison, 818 had been committed over twenty times, and 1,041 confined between twelve and twenty times.Footnote 314 Frederick Falkiner noted the physical and mental weakness of this class of prisoner, observing that they were unable and unlikely to benefit from reformative regimes. He sought harsher and longer sentences, insisting that ‘habitues in street crime cannot maintain reform in the streets’.Footnote 315 Barlow, who had responsibility for the Registry of Habitual Criminals under the 1871 Prevention of Crimes Act, which followed the 1869 Habitual Criminals Act, described criminals in Irish prisons as ‘the dregs of the towns, a different class of men altogether’.Footnote 316 In 1878, William Fagan, Director of Convict Prisons for England, with responsibility for Millbank, Wormwood Scrubs, Brixton and Portsmouth prisons, and George Clifton, Governor of Portland Prison, referred to prisoners as being ‘the waste of all the large towns and of London particularly’. Their prisons were populated with the ‘thieves and the worst description of men from the large cities, broken down in constitution from vice and debauchery’.Footnote 317 Dr Henry Francis Askham, Medical Officer at Portland, who had previously served at Dartmoor and at Woking Female Prison, also observed in 1878 that ‘As a class they are greatly deteriorating.’Footnote 318
The implementation of the Habitual Criminals Acts, which imposed harsher penalties and sentencing for repeat offenders, who were usually confined in local prisons, rendered this cohort of offender more visible to prison authorities, and prompted further commentary on the mental and physical ‘quality’ of prisoners. At Woking, Campbell asserted, many of those first received as lunatic criminals were of an ‘insubordinate type’ and had pursued ‘a life-long career of crime and deception, spending most of their time in prisons, asylums and workhouses’. He absorbed stereotypical criminal traits into his emerging psychiatric categories. ‘Even in the more favourable or hopeful cases’, Campbell argued, ‘it must be remembered that we had to deal with lunatics that were also criminals, and it was sometimes difficult to discriminate between these two elements of character.’Footnote 319 In urban prisons, a large proportion of habitual offenders were committed on drunk and disorderly charges, leading Dr Moore, Belfast Gaol’s Medical Officer, to advocate for ‘habitual drunkards’ to be committed to prison for an indefinite period, only to be released when cured.Footnote 320 Dr Rogers, Medical Superintendent at Rainhill Lunatic Asylum, exemplifying the position adopted by some asylum psychiatrists on habitual drunkards, argued they fell into the category of criminals with limited responsibility. He opposed committing such ‘poor persons to prison’, insisting they required treatment and that it was ‘unjust’ to punish them.Footnote 321 Echoing Moore’s demands in the 1890s, the Visiting Committee at Liverpool Prison, contending with a large number of repeat offenders, many of whom were convicted for drunk and disorderly offences, however, wrote to the Home Office pleading for a system of reformatory detention, as ‘Criminals – like lunatics – should be detained till they are cured.’Footnote 322
Regarded as irredeemable and hopeless cases, the ‘habitual’ criminals’ alleged dislike of hard labour was interpreted as an indication of mental weakness, as well as being further evidence of innate criminal propensities. Director Fagan claimed that the ‘rough working criminal’ preferred separate confinement over public works prisons. Labour in separation, Fagan insisted, was of a ‘milder industrial labour, with perhaps a touch of the wheel or something of that sort’.Footnote 323 The prisoner in separation was not driven the same way as on public works labour, and preferred the ‘idleness’ of separation.Footnote 324 Campbell argued the habitual or ‘casual’ criminal was ‘so thoroughly debased and hardened as to resist any system of treatment’.Footnote 325 Repeat offenders, he claimed, laboured under physical defects, with an inherited propensity to criminality and vagrancy from childhood. So ‘degenerate in body and in mind’ they were unable to earn a livelihood and determined to ‘persist in their evil courses’, rendering prison discipline and reformation futile.Footnote 326 Inspector Gover explicitly linked their resistance to prison discipline to the condition of their minds, observing in 1870 that ‘The moral obtuseness of habitual criminals graduates insensibly into insanity, and a similar remark would apply to those prisoners who habitually commit breaches of discipline.’Footnote 327
In the late nineteenth century prison medical officers increasingly categorised prisoners and convicts who refused to work, resisted or were unable to conform to prison discipline, and seemed impervious to repeated punishments, as ‘weak-minded’. From the 1860s, as Davie argues, the term weak-minded was not a ‘clearly defined medical condition’. Rather it was used as a ‘pragmatic means to identify inmates considered incapable of bearing the punishment regime’, although, as Saunders demonstrates, there was agreement among psychiatrists that the weak-minded were ‘not capable of being certified as insane’.Footnote 328 Amid heightened anxieties about recidivism, high-profile prison doctors, such as Guy at Millbank, linked criminal weak-mindedness to repeat offenders.Footnote 329 Medical officers repeatedly stressed that weak-minded habitual offenders had an inordinate dislike of ‘honest industry’ and of public works. They should be separated from casual and first offenders, and prevented from returning to their homes on release. Instead, it was recommended that they be secluded in a separately designated ‘refuge’ or, in the case of habitual offenders in Ireland, forced to emigrate.Footnote 330
While not perceived as being as dangerous as other categories of convicts, weak-minded convicts and prisoners were observed to be prone to irresponsible and eccentric behaviour, and
peculiarly subject to sudden and ungovernable outbursts of temper and passion, to commit strange and eccentric acts of violence, to irritate their fellow prisoners and are easily excited by them, and are not amenable to the ordinary influences of self-interest or fear of punishment.Footnote 331
At Spike Island Prison, Medical Officer Jeremiah Kelly recommended ‘eccentric’ and ‘slightly weak-minded’ convicts, unfit for separation and labour, to be permitted to work in association, while the ‘weak-minded’ worked in association at picking oakum.Footnote 332 Kelly referred to these convicts as ‘irresponsible’, ‘troublesome’ and ‘unmanageable’; they committed acts of insubordination and restraint was ‘absolutely’ required.Footnote 333 In his evidence to the 1878 Kimberley Commission, Dr Henry Roome, at Parkhurst Prison, noted the weak-minded formed a large proportion of the habitual criminal class and were a constant annoyance and ‘perplexity’.Footnote 334 Inspector Barlow reported that the weak-minded were a ‘constant cause of misconduct’, committed small offences and acts of insubordination.Footnote 335 Campbell also noted the ‘eccentricities’ of Woking’s weak-minded convicts, although he argued the ‘great majority’ of these prisoners were harmless and some were ‘even industrious’.Footnote 336 Observations by Campbell and others on the annoyance the weak-minded caused fellow inmates gave support to those advocating for separate prisons or prison wings for weak-minded convicts.Footnote 337
In day-to-day practice and management, decisions relating to weak-minded convicts and prisoners and their disposal were muddled and haphazard. While Barlow argued such convicts were not to be punished as they were not responsible for their actions, at the same time he noted that ‘doctors cannot certify them as mad, but they are certainly irresponsible’.Footnote 338 Some weak-minded prisoners were well treated, such as Kate Moroney, an inmate of Limerick Female Prison in 1895. Previously committed on several occasions to a lunatic asylum, as a ‘weak-minded’ patient, in prison she was confined to bed on beef tea and two glasses of whisky.Footnote 339 There are more examples, however, of severe treatment. Patrick Gordon, a thirty-year-old convict sentenced to seven years’ penal servitude in November 1881 for breaking and entering, was noted to be ‘obscene’ and ‘eccentric’ on his committal to Mountjoy. Gordon had been convicted on ten previous occasions since June 1875. According to the medical report drawn up by Drs Young and Minchin when Gordon was transferred to Dundrum Lunatic Asylum in 1882, soon after his committal they had observed ‘evident symptoms of weak-mindedness’, laughing on unsuitable occasions and ‘quite idiotic in his deportment’. Despite claims that such prisoners were not punished, Gordon had been frequently placed in close confinement on a reduced diet for various offences related to unruly behaviour, including destroying prison clothing.Footnote 340 As his behaviour deteriorated, the punishments became more severe and in May 1882 he was held in close confinement on a punishment diet for seven days. Concluding that because of his state of mind it was ‘impossible to subject him to the discipline of a prison’, he was removed to Dundrum Asylum in July.Footnote 341 Oscar Wilde recorded the cruelty of punishing the weak-minded and the reactions of fellow prisoners while confined at Reading Gaol from 1895 to 1897. In one of the letters he published in the Daily Chronicle following his release, Wilde described one prisoner, a soldier, as ‘silly’, ‘noisy’ and ‘half-witted’; he was frequently punished, placed in solitary confinement and flogged. Following one such flogging, recommended by the doctor who suspected the soldier of feigning, Wilde observed the man at exercise:
His weak, ugly, wretched face [was] bloated by tears and hysteria almost beyond recognition.… He was a living grotesque. The other prisoners all watched him, and not one of them smiled. Everybody knew what had happened to him, and that he was being driven insane – was insane already.Footnote 342
The unpredictable volatility of weak-minded prisoners, who were otherwise docile and quiet, was repeatedly commented on, as in 1894 when twenty-three-year-old Jemima Overend, convicted for vagrancy and held in Belfast Female Prison for three months with hard labour, was reported to be ‘disorderly’. She ‘attempted to damage her utensils, and threatened to break her window & cell furniture’.Footnote 343 With a history of abusive language and of damaging her cell, she had been confined to the punishment cell on bread and water diet several times. In February 1894 the acting medical officer, Dr E.C. Bigger, had her restrained in muffs, describing her as ‘one of those eccentric and weakminded individuals who sometimes becomes violent without any provocation, and settles down again, and goes on quietly for some time’.Footnote 344 Nonetheless, Bigger certified her as fit for restraint, confinement and the punishment diet. In 1886 Governor A.C. Bulkeley at Maryborough described invalid convicts as ‘notoriously troublesome’ who ‘usually commit breaches of prison discipline’.Footnote 345 In spite of the link made between invalid and weak-minded convicts and habitual criminality, among the 57 convicts held in Maryborough on 31 March 1886, 25 had never been in prison before, and only six had been confined more than six times.Footnote 346
Determining whether weak-minded inmates were eligible for removal to ‘specialist’ facilities depended on the type of sentence they were serving as well as their medical diagnosis. Convicts serving penal servitude sentences were removed to Woking and Marybourgh Invalid Prisons, where they received less severe treatment. Prisoners not serving sentences of penal servitude, who were ineligible for transfer to invalid convict prisons, languished in local prisons or were transferred to other quasi-penal institutions. One such case was prisoner Michael Quinn, who came to the notice of the Irish General Prisons Board in 1884. Quinn, arrested while concealed in a farmer’s outhouse, was in poor physical condition, covered in vermin, and unable to give an account of himself. Tried for vagrancy at Athboy Petty Sessions, he was committed to Kilmainham Prison where the medical officer determined he was ‘undoubtedly weak-minded’ and listed him as an ‘imbecile’ on the prison record. While confined, Quinn was ‘not be required to do much work’ and was ‘allowed a bed’. On encountering Quinn at Kilmainham, Inspector Bourke determined he was not ‘a fit subject for confinement in a prison’, and, presumably because he was not charged with a serious offence, released Quinn from custody to the South Dublin Union workhouse.Footnote 347
As the case of prisoner Quinn highlights, medical officers utilised both ‘imbecile’ and ‘weak-minded’ to describe this category of prisoner. Saunders notes the term ‘imbecile’ was ‘convenient shorthand for prison officials when describing prisoners who refused to conform to the model of stoical acceptance demanded of them by the penal regime’.Footnote 348 According to psychiatric categorisation, in the last quarter of the nineteenth century, ‘idiots were at the lowest end of the ability range, followed by imbeciles and finally the “weakminded” at the end of the range nearest normality’.Footnote 349 Prisoners described as ‘imbecile’ accumulated in convict and local prisons, alongside the mentally ill and the weak-minded, prompting medical officers to speculate on the nature of their mental states, how to manage them, and whether prison discipline had the potential to improve their minds. In 1874, there were eighteen convicts described as ‘imbecile’ and requiring ‘special treatment’ working in the oakum room at Spike Island, and a further ‘12 to 20 others on the Public Works and in the Garden Party who are considered more or less imbecile or weak-minded but not to such an extent as to unfit them altogether from the works’.Footnote 350 Gover estimated there were 140 imbecile convicts in 1880 at Parkhurst and a further 40 at Woking.Footnote 351 Florence Maybrick, who was sentenced to fifteen years’ penal servitude, served at Liverpool, Woking and Aylesbury prisons, observed female prisoners in Woking who ‘hover on the borderland of insanity for months, possibly for years’.Footnote 352 Advocating separate institutions for weak-minded convicts, and noting that weak-minded, epileptic and consumptive prisoners were not isolated at Woking, Maybrick’s comments reflect the challenges this group of prisoners presented:
They are recognized as weak-minded, and consequently they make capital out of their condition, and by the working of their distorted minds, and petty tempers, and unreasonable jealousy, add immeasurably not only to the ghastliness of the ‘house of sorrow,’ but are a sad clog on the efforts to self-betterment of their level-minded sisters in misery.Footnote 353
By the end of the century, prisoner W.B.N. described Parkhurst Prison as ‘half a hospital and half a lunatic asylum’, owing to the invalids and weak-minded prisoners who were brought from other convict prisons when their condition was considered serious. In 1900 a new hospital wing at Parkhurst was designated for criminal lunatics when Broadmoor became too full.Footnote 354 W.B.N. described the ‘great many who are more or less touched in the top story, or who succeed in making it believed that they are so’. They were the ‘weak-minded’ or ‘balmies’, of feeble intellect or partially demented. By the end of the nineteenth century, it was estimated there were about ninety at Parkhurst, and many, W.B.N. added, were difficult to manage and very offensive to staff and prisoners.Footnote 355
Defining an imbecile as someone labouring under an ‘original congenital defect’ and ‘incapable of recovery’, in evidence to the 1882 Commission on Criminal Lunacy, Gover claimed that such prisoners, when released into ‘ordinary life’, were frequently reconvicted to local prisons, where, serving short sentences, the condition of their minds was not diagnosed.Footnote 356 In these cases imbecility was ‘not so marked as to constitute insanity’, and these prisoners were not certified as criminal lunatics.Footnote 357 Only imbeciles who were also habitual criminals and serving penal servitude sentences were removed to Parkhurst where, Gover claimed, they would be ‘better treated’.Footnote 358 Those held in local prisons were detained, but, he insisted, not punished, as medical officers, recognising that these prisoners suffered mental or physical defects, moderated the prison discipline, although he also acknowledged ‘it may take some little time to ascertain whether a man is an imbecile’.Footnote 359 Gover opposed the removal of criminal imbeciles to local workhouses, claiming they were ‘the most treacherous and dangerous set of men you can imagine’, ‘savage and thoroughly intractable’, while others were ‘very easily influenced, and tractable’.Footnote 360 Gover sought their removal from workhouses, as well as prisons, arguing that while the minds of some imbeciles could be improved when placed in the correct environment in a special institution, in the case of criminal imbeciles, there was no hope of recovery.Footnote 361 When confined in convict prisons these inmates were subjected to a modified form of discipline, yet, Gover insisted, they were not completely unfit for the disciplinary regime.Footnote 362
In evidence to the 1882 Commission on Lunacy, Broadmoor’s Medical Superintendent, Dr Orange, also argued that in Broadmoor the uncertain ‘moods and tempers’ of imbeciles resulted in dangerous and unpredictable behaviour.Footnote 363 Orange claimed the mental conditions of ‘weak-minded’ and ‘imbecile’, while recognisable to medical men, were not as clearly defined as lunacy although there were some similarities such as deficient powers of self-control.Footnote 364 As imbeciles who were also habitual criminals already ‘constantly in the habit of committing a crime’, these deficiencies were grounds for detaining them.Footnote 365 While agreeing with prison medical officers that punishing these convicts would not influence their behaviour, Orange proposed they be trained and managed along lines ‘adopted to influence children’, to alter and improve their behaviour.Footnote 366
As Orange’s comments imply, psychiatrists and prison medical staff disagreed on the distinction between lunatics and imbeciles in the prison context. During the 1882 Commission on Criminal Lunacy, Guy and Dr Arthur Mitchell, Deputy Commissioner of Lunacy for Scotland, clashed over the operation of the Lunacy Acts as they related to imbeciles and over Guy’s advocacy of a separate institutional provision, a National Imbecile Asylum.Footnote 367 Guy and Mitchell submitted separate memoranda on the subject to the Commission, both emphasising their expertise in understanding the minds and nature of imbeciles, Guy in the context of the convict prison and Mitchell in his role on the Lunacy Board for Scotland visiting adult imbeciles ‘at large’ and in asylums and prisons over ‘12 or 14 years’.Footnote 368 In his submission Guy elucidated on his interpretation of criminal imbecility as defined under the Criminal Lunatics Acts, arguing that the legislature drew a clear distinction between ‘persons suffering from unsoundness of mind, other than those styled indifferently idiots or imbeciles’, and those ‘who suffer from imbecility of mind’. He noted that ‘The one class are [sic] made inmates of the asylum with a view to the protection of life and property, the other as unfit for penal discipline.’Footnote 369 Guy argued that criminal imbeciles constitute most of the ‘beggars, thieves, mendicant thieves, tramps and vagrants’ who ‘infest our thoroughfares and fill the minds of the weaker, more helpless members of society with constant apprehension’. Echoing Gover’s evidence to the Commission, and combining definitions of the criminal nature of imbecility with psychiatric diagnosis, Guy described imbeciles as ‘dangerous to life and property’, incurable and not amendable to improvement through education.Footnote 370 On this basis, Guy argued all imbeciles, not only those who committed crimes or were found unfit for penal discipline, should be placed in safe custody. Criminal behaviour, including dangerous or serious crimes such as rape, he contended, were embedded in the criminal imbecile’s nature, the majority of whom were habitual criminals. As their criminal natures did not cease with the termination of the penal sentence, he justified the retention of criminal imbeciles in institutions under the remit of the convict prison system.Footnote 371
Emphasising his expertise as a psychiatrist, Mitchell opposed Guy’s proposal for a separate imbecile asylum, and objected to retaining imbeciles in institutions after the expiration of sentences on the grounds that such a measure would deny their legal rights. Once prisoners ceased to be criminals and, by Guy’s logic, they could not be defined as lunatics under the Criminal Lunatics Acts, medical men, Mitchell insisted, had no legal grounds to detain them. In his critique of Guy’s categorisation of imbecility as inherently criminal, Mitchell countered that Guy’s experience of prison medicine, and of imbeciles in prison, had resulted in him studying the ‘very worst of them’, which were ‘a mere handful of the whole body’.Footnote 372 Imbeciles, Mitchell argued, were not ‘malicious destroyers of property’ but could be easily ‘led to abstain from doing wrong’, as many had been ‘trained to vicious practices by vicious sane persons’. Rejecting Guy’s ‘dark view of imbeciles’, he also argued that environmental factors such as poverty and neglect were the main drivers of their criminal behaviours.Footnote 373 In a commentary on a census of imbecile and weak-minded prisoners held in convict prisons on 14 December 1879, and published in the 1882 Commission report, Mitchell drew attention to the varied uses and definitions of the terms ‘weak-minded’ and ‘imbecile’ convicts employed by prison governors, medical officers and chaplains in their assessments of individual cases.Footnote 374 He picked up on previous histories of poverty and neglect and the ‘guilelessness’ of criminal imbeciles, a point Griffith had also noted in his assessment of imbeciles who he described as ‘tools’ of ‘others more intelligent and more designing’.Footnote 375
In developing these psychiatric categories, medical officers, including Guy and Mitchell, related particular forms of mental disorder to specific crimes, again focusing on habitual criminals. In 1869, Guy, in an analysis of the English convict prison population, concluded that ‘men who suffer from diseases of the mind and nervous system are especially addicted to sexual offences, to arson and to acts of violence other than burglary; also in a less marked degree to cattle stealing’. He attributed ‘sexual offences, the fire-raisings and the burglaries’ to weak-minded male convicts, crimes of violence to the epileptic.Footnote 376 Commenting on a case of acute mania at Woking in 1869, Campbell also noted that the young male prisoner had ‘some peculiarity of manner … together with a conviction for arson, which is a crime suggestive of mental weakness’. The prisoner, who had been seized in a sudden manner while in the oakum room and had an aversion to food, was very violent and had been in a ‘febrile excitement’.Footnote 377 Gover noted that criminal imbeciles were ‘wayward and impulsive’, ‘grown-up’ children addicted to wandering, acts of mischief and of cruelty such as arson.Footnote 378
This individualised and practical orientation of prison medicine distinguished the work of Campbell, Guy, Nicolson and MacDonnell from their continental counterparts. Rejecting theories of the ‘born criminal’ and generalisations on the nature of the prisoners’ minds, developed by the Lombrosian school and based on surveys of prison populations, prison medical officers emphasised the importance of treating and assessing individual prisoner patients in their quest to understand mental disorder among prisoners and manage such cases in challenging prison environments. Largely unsympathetic to theories that criminals were predetermined or programmed to commit crime, those who had some sympathy with these arguments in the early 1870s, such as Nicolson, rebuffed scientific claims that hereditary defects, including insanity and criminality, were identifiable by anatomical or physiological stigmata. Instead they stressed the ‘value and influence of domestic and social environment, and of education and training, in moulding and forming the character’.Footnote 379 In 1899 MacDonnell, also dismissing Lombrosian theories, noted that ‘environment and example are two large factors’ in the production of crime.Footnote 380 As discussed above, prison medical officers devoted considerable time to managing and treating individual cases, prescribing drugs and enhanced food allowances, and, in some cases, force-feeding prisoners. They stressed their unique experience and access to such cases, which Guy noted provided him with ‘the special information which nearly seven years of office as medical superintendent of a convict prison, with a daily attendance subject to few interruptions, could not fail to have afforded me’.Footnote 381
This emphasis on individual case studies was repeatedly enforced, with Nicolson arguing in 1895 that ‘Each case must be taken on its own merits, and above all, and first of all, the man must be allowed to speak for himself, and to give his own “reason for the hope that is in him”’.Footnote 382 He dismissed the ‘criminological method’ as ‘useless’ and ‘misleading’ in daily practice and, citing statistics on juvenile reformatories, disagreed with claims that the majority of criminals could not be reformed and emphasised the significance of environmental factors such as poverty as motivating factors.Footnote 383 Ever wary of attacks on their professional status, there were also concerns that the generalised methodology of these theories reduced the function of the prison doctor to a technician who sorted prisoners according to several degenerate categories and institutions rather than providing individual diagnoses.Footnote 384 Arguing that prisoners were ‘not passive victims of hereditary’, Guy claimed the majority retained responsibility and the capacity to ‘prefer thieving, with all its concomitant risk, to more reputable, if more laborious, modes of maintaining themselves’.Footnote 385 In his extensive publications, he sought a prestigious and expert role for prison doctors, who were uniquely positioned to understand the minds of prisoners, one that went beyond stamping ‘“criminals” as lunatics or quasi-lunatics, or to place them on a special morbid platform of mental existence’.Footnote 386
Pentonville’s Medical Officer, Dr John Baker, adopted a similar position in the 1890s. He characterised Lombroso’s theories as ‘extravagant views held by a section of continental criminologists’ and concluded that attempts to identify ‘physical and psychical’ stigmata among English felons do not ‘warrant the assumption that there exists a special criminal type or a distinct criminal neurosis’.Footnote 387 From his close work in prison, he linked forms of mental disorders with specific crime noting, for example, ‘the violence of epileptic insanity, the proneness of general paralytics to acts of petty larceny, the dangerous nature of delusional insanity, and the aimless crimes of dements’.Footnote 388 Baker suggested that the arsonist had a ‘defective mental capacity’ or was ‘weakminded’ and that there was ‘a general relation of acts of incendiarism to the various forms of insanity’.Footnote 389 Baker went on to claim that prisons removed ‘dangerous and insane criminals’ from society and ‘annually eliminated [them] from the ranks of the community’, thus underlining the important role played by prison medical officers.Footnote 390
Conclusion
By the end of the nineteenth century, vocal critics inside and outside of prisons highlighted the high incidences of mental illness among prisoners, and the excessively harsh aspects of prison discipline, including the separate system of confinement as it then operated in prisons in England and Ireland, which they argued could be harmful to the minds of prisoners. In 1894, Reverend William Morrison, chaplain at Wandsworth Prison between 1887 and 1898, claimed insanity rates in English local prisons had reached 113 per 10,000 between 1875 and 1877, increasing to 226 per 10,000 in 1890–92.Footnote 391 These high figures may in part have reflected a greater willingness by medical officers to diagnose prisoners as insane towards the end of century. Witnesses to the 1895 Gladstone Committee criticised the treatment of insane prisoners, while members of the Howard Association claimed that prisons produced an ‘undue amount of insanity’ among inmates, and these criticisms, among others, prompted the dismantling of the Du Cane system in England and, as examined in Chapter 6, the eventual decline of the separate system.
Such claims did not go uncontested, and, in response to allegations that the separate system produced mental disorders, prison commissioners, administrators and staff repeatedly defended the regime, insisting that prisoners were likely to be insane on admission, had a hereditary predisposition to insanity, were weak-minded or were feigning insanity.Footnote 392 In his report for the year 1897, Dr Herbert Smalley, the Medical Inspector of English Prisons, denied that ‘prison is a manufactory for the production of lunacy’, while Dr A.R. Douglas, an ally of Smalley’s, argued that the high incidences of mental disorder among prisoners was a consequence of the ‘material which is subjected to the penal environment’.Footnote 393 Although the first-time offender might initially experience feelings of depression, nonetheless, he argued, ‘this individual is of sufficient mental calibre to have enabled him to take up to the time of his arrest a fairly successful part in the battle of life, it is absurd to suppose that this depression should deepen in intensity and become acute Mental pain’.Footnote 394 In the case of recidivists, however, prison was a ‘normal condition’ and while some ‘take their imprisonment as a matter of course’, others ‘make it their business to give as much trouble as they can’.Footnote 395 In a robust defence of prison medical officers, the Journal of Mental Science argued that prisoners, owing to inherent mental weaknesses, had already demonstrated their inability to adapt to non-penal environments and ‘oscillated’ between asylums and prisons.Footnote 396 ‘Depression must constantly follow imprisonment’ owing to ‘minds so ill-developed and ill-balanced, and often already depressed by anxiety arising from fear of detection in wrong-doing’ and ‘the sudden withdrawal of habitual excitation (mental or physical)’. While in prison ‘depression is often exaggerated by their low physical powers and by onanism’.Footnote 397 The social role of the prison was emphasised as the ‘beneficial results of the healthful [prison] regime and withdrawal from excesses’ outweighed any negative results.Footnote 398
Prison officials and medical officers made similar comments on the ‘quality’ of prisoners in Ireland. In 1905 a report of the medical committee appointed to inquire into removals of prisoners to Dundrum Asylum, noted that ‘by parentage, education and association’, prisoners’ ‘minds are impregnated and identified with ideas and habits of a vicious and criminal nature which show themselves during sane not less than during insane periods’. The medical committee, which included David Nicolson and Dr George Plunkett O’Farrell, Inspector of Lunatic Asylums in Ireland, also argued that the management of such cases in prisons required an ‘extension of the area of sanity so as to include prisoners for whom ordinary penal discipline has to be relaxed and enables prisoners of this exceptional type to be detained in prison’.Footnote 399 While acknowledging that such prisoners were unable to withstand the full rigour of prison discipline, the medical committee regarded them as primarily as criminals who were also lunatics, a distinct label and category examined in Chapter 4. Meanwhile, over the last quarter of the nineteenth century, the professional confidence of prison medical officers had steadily grown, and rooted in decades of close observation of individual cases of mental illness in the prison, many published widely on the topic, advocated for their professional interests and contributed to official debates on penal policy. Though still negotiating a pathway through the complex demands of providing medical care on the one hand and complying with the requirements of prison discipline on the other, prison medical officers were confidently asserting a role as ‘the recognised and responsible protector of the prisoner from any harsh treatment that may tend to his physical and mental detriment’.Footnote 400 They also increasingly laid claim to the advancement of professional psychiatric practices and the production of new knowledge that could be applied outside as well as inside the prison.
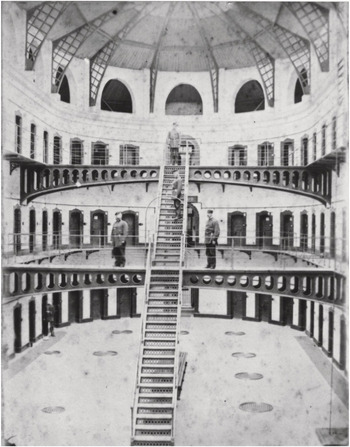



 Open access
Open access