



Introduction
The existential dimensions and associated questions derive largely from philosophers (e.g. Kierkegaard, Nietzche, and Heidegger) who have developed thoughts over the centuries. This tradition of existential philosophy includes both theistic and secular worldviews and it has been argued that fundamental values and beliefs should have a common label (Breitbart Reference Breitbart2007). Central existential issues are meaning, as well as loss of meaning, in life and dignity, which is important in communication around the existential dimension (Chochinov Reference Chochinov2007; Frankl Reference Frankl1972). Being human has been described as being confronted with the four basic existential challenges: death, meaninglessness, loneliness, and freedom (Yalom Reference Yalom1980).
Existential/spiritual thoughts and emotions often come to the fore when a person or their loved ones suffer from a severe and/or life-threatening disease (Benkel and Molander Reference Benkel and Molander2017; Bolmsjö et al. Reference Bolmsjö, Tengland and Rämgård2019; Chen et al. Reference Chen, Chen and Xiao2022; Karlsson et al. Reference Karlsson, Friberg and Wallengren2014; Sjöberg et al. Reference Sjöberg, Rasmussen and Edberg2022) and can include aspects of illness vs wellbeing related to the loss of the patient’s autonomy, self-determination, and guilt. Existential questions have elements of relationships, social connections, community, and loneliness. These questions can evoke a variety of emotions such as anxiety, peacefulness, despair, hope, and hopelessness (Bolmsjö et al. Reference Bolmsjö, Tengland and Rämgård2019; Chen et al. Reference Chen, Chen and Xiao2022; Deeken Reference Deeken2009; Hvidt et al. Reference Hvidt, Mikkelsen and Zwisler2019; King and Hicks Reference King and Hicks2021).
In palliative care, inclusion of the spiritual dimension is considered important to achieve holistic care. However, there is no general consensus on the definition of spiritual care or what it encompasses. The European Association for Palliative Care (EAPC) reference group for spiritual care has addressed this question and provided the following definition of “spirituality”: “Spirituality is the dynamic dimension of human life that relates to the way persons (individual and community) experience, express and/or seek meaning, purpose and transcendence, and the way they connect to the moment, to self, to others, to nature, to the significant and/or the sacred” (Nolan Reference Nolan2011). This broad definition makes it clear that spirituality can be understood as a wider concept than organized religious practice, with which the term has often been associated. It also indicates that spiritual care is not an exclusive task for chaplains but could be performed by many professionals (Damen et al. Reference Damen, Labuschagne and Fosler2019; Fay and OBoyle Reference Fay and OBoyle2019; Jeuland et al. Reference Jeuland, Fitchett and Schulman-Green2017).
In a Western context, not least in the Scandinavian countries, which are often regarded as highly secular societies, the existential/spiritual dimension in care has been given increased attention and interest, and new ways sought to approach the subject. A post-secular starting point stresses that modernity and “enlightenment” do not automatically result in an absence of spirituality and religiosity. The post-secular concept offers an increased understanding of a society characterized by globalization and pluralism in combination with an increased self-perceived spirituality, with or without religious expressions (Habermas Reference Habermas2006, Reference Habermas2008; Stripp et al. Reference Stripp, Wehberg and Büssing2023). According to Nissen et al. (Reference Nissen, Viftrup and Hvidt2021), spiritual care can be understood as trying to comprehend the patient’s existential orientation, needs and resources in religious, spiritual and secular domains (Hvidt et al. Reference Hvidt, Assing Hvidt and la Cour2022). All three existential domains are surrounded by a cultural context and influenced by, for example, family, social, historic, economic, and educational aspects (Hvidt et al. Reference Hvidt, Assing Hvidt and la Cour2022; Nissen et al. Reference Nissen, Viftrup and Hvidt2021; Walach Reference Walach2017).
“Existential” can therefore be seen as a broad term for issues surrounding people’s experience and way of thinking about life, and in Sweden it is often used as (Browall et al. Reference Browall, Melin-Johansson and Strang2010; Sjöberg et al. Reference Sjöberg, Rasmussen and Edberg2022; Udo et al. Reference Udo, Melin-Johansson and Henoch2014) and argued to be the best suited (Salander Reference Salander2006) term for these matters in a healthcare context.
In order to meet patients’ existential needs, both theoretical and practical knowledge about what the existential dimension includes is required by researchers and teachers as well as clinicians. The views of healthcare professionals on the existential dimension of end-of-life care in a highly secular context need further exploration. Therefore, the overall aim of this study was to investigate how professionals, caring for people approaching death, perceive the existential dimension of care.
The research questions were: What does the existential questions encompass? What are existential needs and how are they identified? What is existential care? Is the existential dimension in care important?
Method
A mixed method design including a digital survey with open- and closed-ended questions was used (Tashakkori and Teddlie Reference Tashakkori and Teddlie2003). Due to a lack of suitable precursors, the questionnaire was developed by the researchers, and it contained a total of 27 questions in Swedish (19 main questions with 8 supplementary questions) plus 7 demographic questions The Swedish word for existential was used in the questions, aimed at including spiritual, religious, and secular issues of an existential nature. To meet the study’s objective, questions were asked about existential issues, needs and care. The questionnaire was pilot tested on healthcare professionals and minor adjustments were made subsequently.
Data collection
The survey was sent by mail to 38 managers of healthcare professionals at specialized palliative care units (P), an oncology clinic (O) and municipal (M) healthcare within home care and a nursing home in western Sweden. Units were selected based on the care of people at the end of life (life-threatening illness and/or elderly).
If the managers accepted the unit’s participation in the study, they were asked to forward the questionnaire by mail to all the staff at the unit who were involved in the care of patients, regardless of whether the person was subordinate to the manager. Information on the number of mailings from the managers was not requested and the response rate cannot therefore be estimated. By answering the survey, the respondents gave their consent.
Data were collected between October 2021 and April 2022. This study was approved by the Swedish Ethical Review Authority (No. 2021-00956; date of approval: 17/03/2021).
Data analysis
Descriptive statistics were applied to closed-ended questions. For open-ended questions, a qualitative descriptive approach was used to obtain a rich, straight description of the professionals´ perception of the existential dimension of care (Bradshaw et al. Reference Bradshaw, Atkinson and Doody2017; Neergaard et al. Reference Neergaard, Olesen and Andersen2009). All researchers read the open-ended questions independently so that a picture could be obtained of common opinions among the participants. All the authors then analyzed the data to identify themes, phrases, and important features. The most common findings were described and compared against each other, and supporting quotes were linked. An analysis was performed jointly by all the authors to interpret the results as objectively as possible. Any discrepancies were discussed until a common conclusion was reached.
Results
Participants
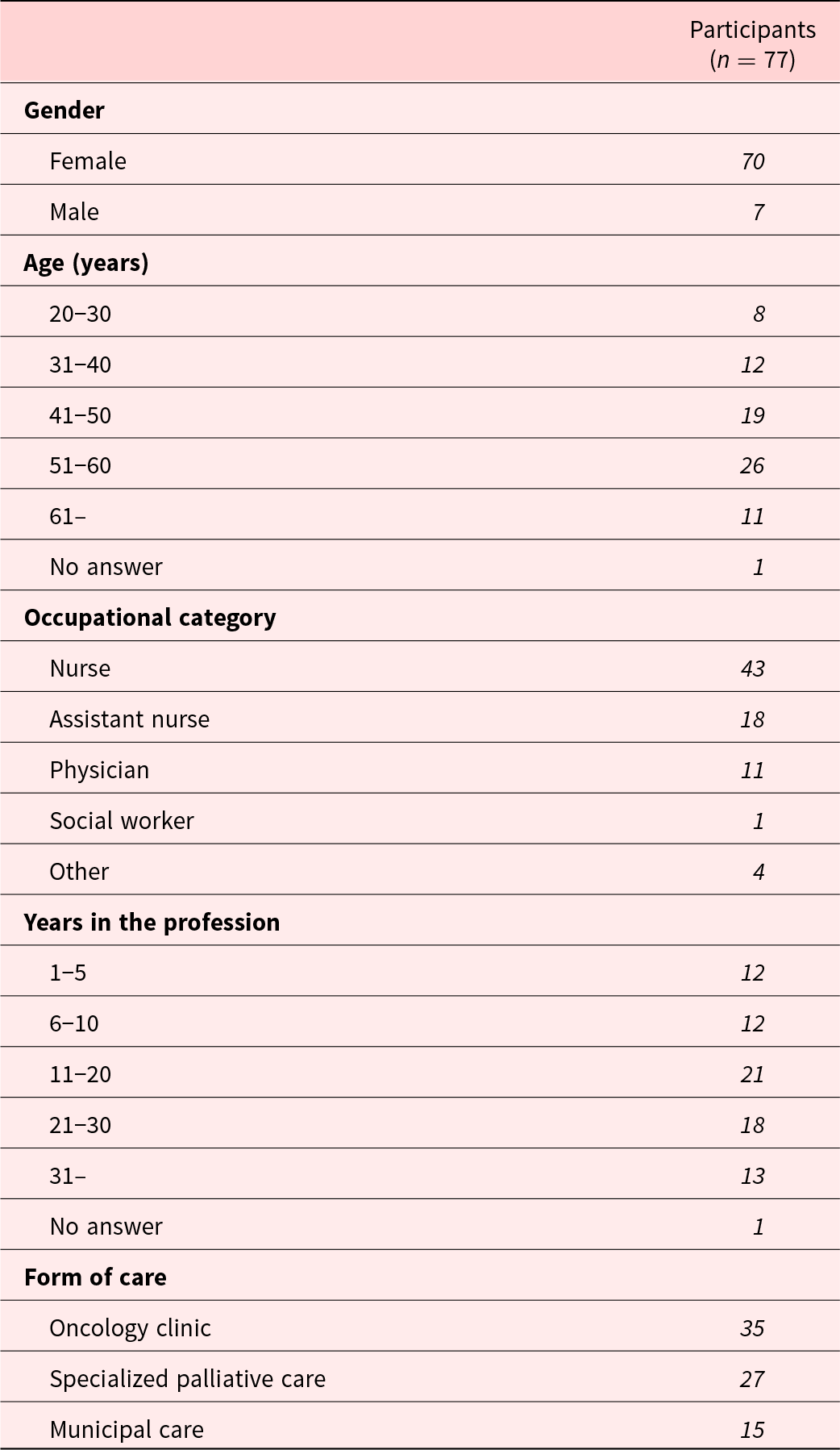
A total of 77 persons answered the survey. The respondents were physicians, registered nurses, assistant nurses and social workers. Their ages varied from 20 to 65 years and their number of years of employment between 11 and 30. Males were underrepresented. For more details, see Table 1. This is the presentation of the results from a part of the survey that focuses on the research questions that were mentioned in the introduction. The results are divided into open-ended questions and closed-ended questions. The summary of the analysis of the responses to the open-ended questions is presented under three headings: existential questions, existential needs, and existential care.
Table 1. Demographic data
Existential questions
When asked what the existential questions encompass, the professionals’ answers covered a broad spectrum. While some mentioned a specific issue, others’ answers included a wide range of subjects.
“Questions about what it is like to be human.” (P)
The most prominent answers were the meaning of life, thoughts about life and death, and life after death. Quite commonly, spirituality, faith, and religion were mentioned. Additionally, some connected culture and philosophy to the existential questions. Professionals also included thoughts about loneliness, relationships, guilt, and shame in their answers.
“Thoughts about existence, life, death, afterlife, what happens thereafter, faith/doubt/fate, the meaning of life, why did it end up like this? etc. The questions ‘how’ or ‘why’ in relation to something greater…” (M)
The answers were sometimes formulated as a question, i.e. why do things happen? what happens after death?, and what is the meaning of life?
Existential needs
Existential needs were expressed as centered around having the opportunity to communicate, sharing their thoughts and experiences, and being seen and heard.
“To be seen and heard in the place where I am. To be respected for my own wishes and thoughts. To be able to reflect together with someone without being judged. To laugh or cry.” (P)
Experiencing a sense of meaning was commonly said to be an existential need. The importance of relationships to other persons was mentioned, often in terms of closeness, love, trust, coherence, and a sense of belonging.
Some specifically referred to existential needs as spirituality and/or practising their religion and need for rites and ceremonies.
“Examining the needs of the guest/patient through senses, presence, and questions and conversations.” (P)
When asked how to identify existential needs, the professionals pointed to verbal communication about the issues mentioned above, for example a patient wanting to talk about faith or the meaning of life.
Professionals also said that they identified potential existential needs when patients had a large number of questions about illness and treatment and were expressing worry and anxiety.
There were also non-verbal expressions that the professionals interpreted as existential needs, such as body language expressing anxiety or pain, or the patient avoiding contact with others.
“Conversation, clinical look, reading situations, body language and facial expressions.” (O)
Some pointed to loved ones as a source of information about the patient’s existential needs. By discussing the patient in the professional care team or using symptom assessment forms, the patient’s existential needs could be identified.
Existential care
Regardless of the care context in which the participants worked, most described existential care as needing a holistic view, such as “seeing the human being as a whole, body and soul together.” (M)
Existential care was most often said to be connected to communication. Care could be achieved through conversations, with listening and being responsive to the patient’s reflections and opinions being a key element. When necessary, the professionals said they would refer to a suitable professional inside or outside the team (e.g., social worker, spiritual care provider) or give the patient the chance to practise their religion. Existential care in the form of communication also included sharing moments in the present without doing anything.
“Trying to create a permissive space, asking open questions and waiting. This usually leads to the person approaching the thing that is bothering them.” (P)
Some mentioned that communication around existential issues requires courage, to dare to ask questions and to dare to stay put.
Existential care was sometimes described as ordinary care intervention performed by professionals. This could include physical care, helping the patient with daily activities, as well as considering the person’s expressed needs in care planning. Thus, medical care is also described as part of existential care.
“To help find a meaning, to give hope, to facilitate so that the person can clear up ambiguities, to support in Activities of Daily Living [ADL], where necessary, to relieve suffering, e.g. pain, to help to provide security.” (O)
Many participants were of the opinion that existential care was something that they already performed, albeit not in a very structured way. Existential care was considered a matter of attitude and responsiveness.
“not only to care for the person’s wounds but also to care for the person’s concerns or questions about life, death, guilt, spirituality.” (P)
Importance of the existential dimension in care
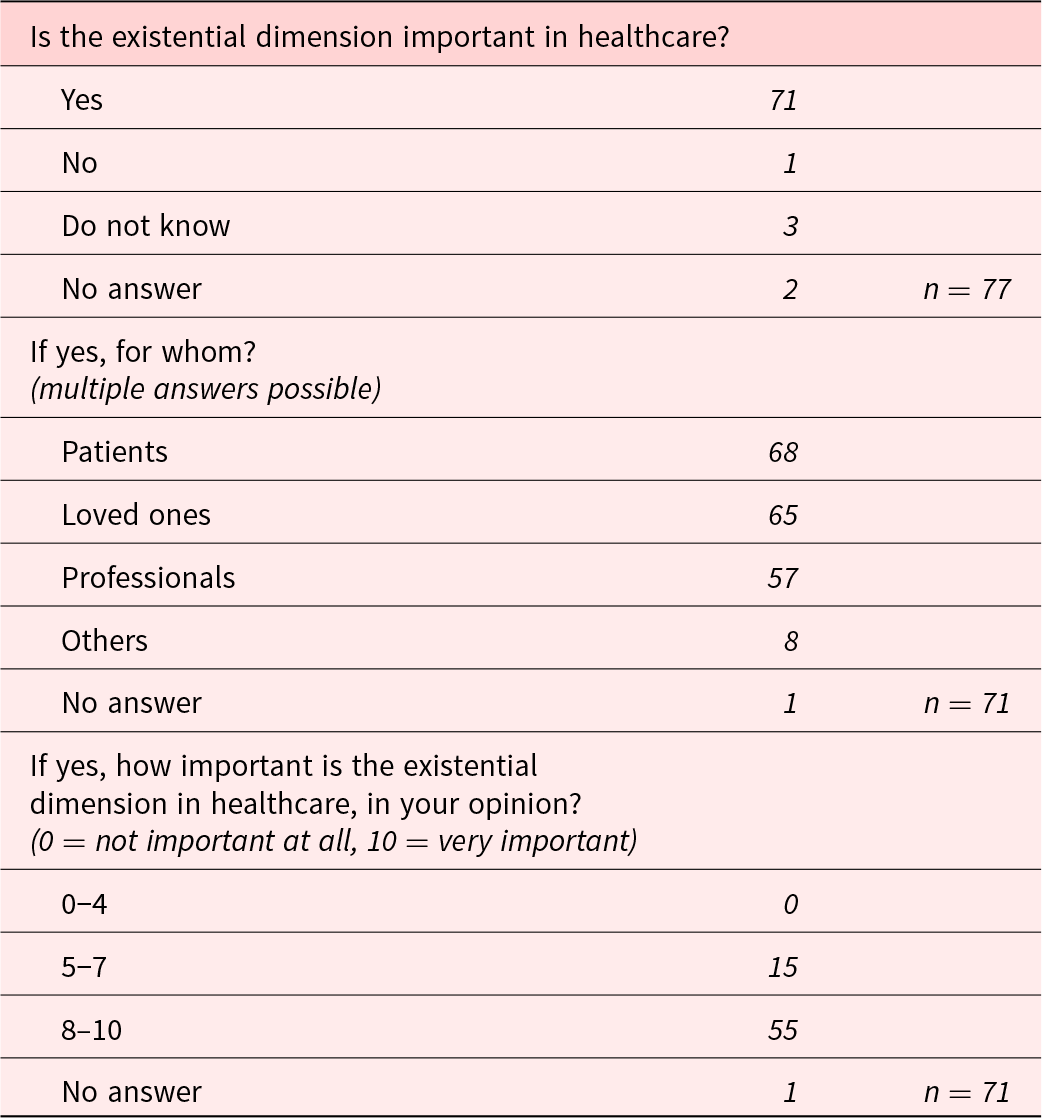
The results of the closed-ended questions regarding the importance of the existential dimension in healthcare are presented in Table 2. A large majority of the respondents (71/77 = 95%) considered the existential dimension important for patients, loved ones as well as professional carers. When asked to rate the importance of the existential dimension on a scale of 0–10, the majority (55/71 = 78%) answered 8–10. No significant differences in responses were found when comparing professionals from the three different forms of care.
Table 2. Importance of the existential dimension in care
Discussion
This study shows a high level of agreement among the responding healthcare professionals that the existential dimension is an important issue in care. In its broadest definition, this dimension can be seen as a concept for issues surrounding people’s experience and way of thinking about life. This could include the meaning of life, death and dying, guilt, relationships, loneliness, and how a person perceives themself, which is in line with previous findings in diverse cultural contexts (Delgado-Guay et al. Reference Delgado-Guay, Palma and Duarte2021; Hvidt et al. Reference Hvidt, Mikkelsen and Zwisler2019; Vehling and Kissane Reference Vehling and Kissane2018).
Despite the fact that Sweden is often referred to as a secular country, this study shows that religious beliefs and spirituality are still a part of the existential dimension, in line with reports from other Scandinavian countries (Hvidt et al. Reference Hvidt, Assing Hvidt and la Cour2022, Reference Hvidt, Mikkelsen and Zwisler2019; Stripp et al. Reference Stripp, Wehberg and Büssing2023) which may reflect the post-secular understanding of a modern society (Stripp et al. Reference Stripp, Wehberg and Büssing2023). Examples of existential issues from religious, spiritual, and secular domains (Hvidt et al. Reference Hvidt, Assing Hvidt and la Cour2022; Nissen et al. Reference Nissen, Viftrup and Hvidt2021) were all mentioned by the participants.
Besides direct verbal expressions by patients, loved ones or the care team, the identification of existential needs could also be indirect through the interpretation of the underlying meaning of verbal and non-verbal expressions. The link between the physical and the existential dimension was revealed by professionals as understanding some expressions of physical pain or anxiety as existential needs, as has been described in this study. Thus, existential needs are often a product of an interpretive process.
Conversation has been described as central to existential care (Fay and OBoyle Reference Fay and OBoyle2019; Gijsberts et al. Reference Gijsberts, Liefbroer and Otten2019; Kestenbaum et al. Reference Kestenbaum, Fitchett and Galchutt2022; Tornøe et al. Reference Tornøe, Danbolt and Kvigne2014), as was the case in this study. The participants stressed the importance of listening attentively, daring to stay put in difficult conversation, asking questions and acknowledging the dignity of the patient’s questions. Healthcare professionals can identify existential needs when they are expressed clearly in words by the person, for example, explicitly wanting to talk about the meaning of life or asking for contact with a religious service or representative for secular spirituality. The professionals also experienced presence with a patient as important non-verbal communication signaling “I am here for you.”
Historically, the holistic care that pervades palliative care encompasses four dimensions: physical, psychological, social and existential/spiritual. However, this compartmentalization can be misleading as all dimensions intersect, as this study has shown, and perhaps especially so for the existential dimension. When asking healthcare professionals, it becomes obvious that existential care is embedded in, for example, physical care, in which the existential dimension can be hard to discern objectively. In this study, concrete actions are perceived as existential care. This can be when helping patients with their daily activities, for example, assistance in taking a shower. A vulnerable situation such as this can raise existential questions of which the professional needs to be aware. This also means that the existential dimension of care is closely connected to other caring efforts that are made. In other words, when a professional takes care of someone’s body, they take care of their soul. The care could also involve helping patients to practise their religion and culture, in line with previous studies (Harrop et al. Reference Harrop, Noble and Edwards2017). This means that all care can have an existential aspect and that all professionals potentially perform existential care but may not always be aware of it.
Many professionals used the word “dare” when commenting on existential care, indicating that it can be experienced as a risky issue. There may be several reasons for this, for example that healthcare professionals have the attitude that they should solve problems, which is often not possible with existential issues. Alternatively, it could be a fear of incompetence: doing something for which they have no training or education, or that the subject triggers the professional’s own existential questions and fear (Fay and OBoyle Reference Fay and OBoyle2019; Soroka et al. Reference Soroka, Collins and Creech2019; Udo et al. Reference Udo, Melin-Johansson and Henoch2014).
Existential questions about death and dying are common in the care of patients with life-threatening diseases. Nonetheless, it is well known that healthcare professionals are often reluctant to talk about it due to fear, as mentioned above. As a consequence, patients are deprived of communication even in the case of positive existential experiences surrounding death exemplified by the common and transcendental end-of-life experience of meeting deceased loved ones (Kerr et al. Reference Kerr, Donnelly and Wright2014; Nyblom et al. Reference Nyblom, Arnby and Molander2021, Reference Nyblom, Molander and Benkel2022).
Existential care could be perceived as exclusive to certain professions, such as chaplains, resulting in others hesitating and not perceiving their own work as existential care (Best et al. Reference Best, Butow and Olver2016; Jeuland et al. Reference Jeuland, Fitchett and Schulman-Green2017). Team work, which is essential in palliative care, can play an important part in identifying a patient with existential needs (Fernando and Hughes Reference Fernando and Hughes2019). Since all professionals in a team have conversations with the patient, they can share their assessments of patients’ existential needs with each other to determine who is the best suited professional to assist with the specific questions.
This study has both limitations and strengths. The survey language was Swedish, which excluded non-Swedish-speaking people who may have given a different perspective on the research questions. Males were underrepresented, as were young professionals and professions other than nurses. The Swedish society is regarded as highly secular which could limit transferability outside Scandinavia. Choosing a qualitative descriptive approach has the advantage of data analysis remaining close to what is reported by the participants. Most of the professionals had worked for more than 10 years and were likely to have been familiar with the subject and the terminology, which could have influenced the result. Despite the mentioned limitations, the study showed a strength in that coherence in the answers was found despite participants being professionals in different care contexts; oncology, municipal care, and specialized palliative care.
Conclusion
This study shows that there was a high level of agreement among the responding healthcare professionals that the existential dimension is an important issue in care. Existential questions can encompass a broad spectrum focusing on the meaning of life, thoughts about life and death, and life after death. Even if a country is regarded as secular, existential questions are present though not exclusively as a religious or spiritual concern. To be able to give existential care, a healthcare professional needs to identify the existential needs. This identification could potentially be done by all occupational categories.
The most prominent content matter in existential care was found to be communication including listening and daring to stay put, existential care integrated in physical care and care given by religious representatives.
Although existential care often centers around verbal communication, it can also be mere presence without words, with the intent of existential support. Several participants considered existential care a matter of attitude and responsiveness, with many expressing the necessity of daring to approach the subject.
The connection between the physical and existential dimension becomes tangible in the respondents’ view on existential care. In other words, a professional who takes care of someone’s body also takes care of their soul. When needed, referrals were made to specific professions such as spiritual caregivers.
While the results suggest that most participating healthcare professionals were familiar with the existential concept and identifies existential needs, future research should focus on patients’ own understanding of the topic and expressed existential needs.
Acknowledgments
The authors thank the participants for taking the time to provide their views on the research question.
Author contributions
All four authors have made equally significant contributions to this work, including developing the article and providing feedback on multiple versions of the article. Conceptualization: C.B., I.B., U.M., and S.N. Funding acquisition: I.B., U.M., and S.N. Writing: C.B., I.B., U.M., and S.N. Review and editing: C.B., I.B., U.M., and S.N.
Competing interests
The authors declare no conflicts of interest.



 Open access
Open access