


Unhealthy dietary intakes are risk factors for cardiovascular diseases and some forms of cancer1, which are the most common causes of mortality in Western countriesReference Murray and Lopez2, Reference Michaud, Murray and Bloom3. High levels of energy intake play a role by contributing to overweight and obesityReference Hu, Manson, MJ, Colditz, Liu and Solomon4, Reference McCullough, Feskanich, Rimm, Giovannucci, Ascherio and Variyam5. Total fat and saturated fat intakes supply energy which contributes to overweight and obesity, and saturated fat influences blood levels of harmful (low-density lipoprotein) cholesterol1. In an effort to achieve reductions in morbidity and mortality, dietary guidelines have been developed that endorse a suitable energy intake and promote low consumption levels of total and saturated fatsReference McCullough, Feskanich, Rimm, Giovannucci, Ascherio and Variyam5, Reference McCullough, Feskanich, Stampfer, Rosner, Hu and Hunter6.
Until recently, the mainstream thought was that most determinants of dietary intakes occurred within the individual. Taste preferences, habit, nutrition knowledge, intentions, attitudes, outcome expectancies, self-efficacy and a number of other individual-level factors were considered primarily to drive what people eatReference Armitage and Conner7, Reference Glanz, Lewis and Rimer8. However, these determinants were found to explain only a small portion of the variance in dietary intakesReference Glanz, Kristal, Tilley and Hirst9. Recently, there has been a growing interest in the role of the environment in influencing people's dietary behaviour. This social ecological view of health emphasises that individuals interact with their environmentsReference Giles-Corti and Donovan10 and that characteristics of the environment influence their health behaviours.
The rising prevalence of overweight and obesity is one of the major public health concerns today. Changes in dietary and physical activity behaviours are thought to underlie this trend. The determinants of these changes are less well known. Since Swinburn and Egger introduced their ecological paradigm for understanding obesityReference Swinburn, Egger and Raza11 and argued that an increasingly ‘obesogenic environment’ contributed to the trends, there has been great popularity in examining whether environmental factors are associated with obesity-related behaviours.
A number of position papers and narrative reviews have identified environmental factors associated with the obesity epidemicReference Wansink and Kim12, Reference Pollard, Greenwood, Kirk and Cade13; however no systematic review has examined the role of environmental factors in dietary intakes. For example, the increasing densities of fast-food restaurants and convenience stores are thought to promote unhealthy food choicesReference Booth, Pinkston and Poston14. Media marketing of high-fat foods, their low prices and the greater range of convenience foods available are considered to be contributing factorsReference Swinburn, Egger and Raza11, Reference Booth, Pinkston and Poston14. The increased participation of women in the workforce has resulted in a greater reliance on convenience foods and less structured meal patterns, contributing to less healthy dietary intakesReference Banwell, Hinde, Dixon and Sibthorpe15. The greater variety of foods available in supermarkets may contribute to populations deviating from their traditional diets, adopting less healthy intakes, and portion sizes have increasedReference Banwell, Hinde, Dixon and Sibthorpe15. The presumed importance of these environmental determinants of unhealthy dietary behaviours have resulted in strong appeals for a better understanding of the role of environmental factors in dietary intakes and environmental interventions.
We conducted a systematic review of studies on environmental factors associated with energy, total and saturated fat intakes to summarise the current scientific evidence. We aimed to address which environmental factors have been examined in relation to these dietary outcomes to date, and identify issues for future research.
Methods
For the purposes of this study, the environment was defined as everything outside the individualReference Sallis, Owen, Glanz, Lewis and Rimer16. A framework used in previous researchReference Kamphuis, van Lenthe, Giskes, Brug and Mackenbach17 that identifies four categories of environmental factors related to health behaviours was used to classify different environmental factors during the review process. The framework shares common features with ecological modelsReference Cohen, Scribner and Farley18, Reference Hovell, Wahlgren, Gehrman, DiClemente, Crosby and Kegler19, stressing the importance of multiple types of environmental influences. The four categories that form this framework are:
1 Accessibility and availability. Including physical and financial accessibility of products and shops that are needed for an (un)healthy diet (e.g. access to shops, and availability of high-fat foods and less healthy snacks).
2 Social conditions. These arise from inter-personal interactions and include social relationships (e.g. family/marital status), social support and psychosocial stressors such as relationship difficulties.
3 Cultural conditions. These are the result of non-personal interactions or engagement with a larger group of people, such as culture-specific eating patterns, health value orientations, food experiences in childhood and cultural participation.
4 Material conditions. These include the financial situation (e.g. household income), material and social deprivation, and unfavourable working, housing and neighbourhood conditions (e.g. neighbourhood deprivation). These may affect behaviour through one of the previous environmental factors. For instance, a person's budgetary situation may partly determine their access to products and facilities. Living or working in an unfavourable environment might induce stress, which may relate to indifference concerning a healthy diet.
Search strategy
The current study was conducted within a larger study reviewing the literature of environmental factors associated with energy, fat, fruit and vegetable consumption among adults. Therefore, literature searches were conducted for a broader range of outcomes than those presented here, and included keywords for fruits and vegetables. Results on environmental factors associated with fruit and vegetable intakes can be found elsewhereReference Kamphuis, Giskes, Wendel-Vos, de Bruijn, Brug and van Lenthe20.
A review protocol based on guidelines from the Cochrane Reviewer's HandbookReference Higgins and Green21 was used. Studies conducted among human subjects between 1 January 1980 and 31 December 2004 were located by searches of several major databases (i.e. PubMed, Human Nutrition, Web of Science, PsychInfo and Sociofile).
Broad search terms were used in the database searches to ensure that all potentially relevant articles entered the screening process. Each database was searched using database-specific indexing terms; suitable terms were selected from lists of the database indexing system. For databases that did not have their own indexing terms (i.e. Human Nutrition and Sociofile), we searched for keywords in titles. The sensitivity of searches was tested by seeing whether they located several key articles. Searches located 20 653 potentially relevant titles (7440 in PubMed, 8325 in Human Nutrition, 4828 in Web of Science, 58 in PsychInfo and two in Sociofile). Detailed search strategies for each database can be found at http://mgzlx4.erasmusmc.nl/pwp/?ckamphuis.
Inclusion criteria
To be included, studies must have been published in English and conducted among a population-based sample of adults (i.e. studies examining disease or patient subgroups, and those conducted among participants below 18 years or above 60 years of age were excluded) and they must have quantified dietary intakes. In addition to this, studies must have been conducted in an established market economy as defined by the World Bank22, and the dependent variable(s) must have been energy intake, total/saturated fat intakes or fruit and vegetable intakes. Intervention studies and studies with a research design that made it impossible to decipher associations between environmental factors and the outcome behaviours were excluded.
Title scanning
The title screening process was performed by two reviewers (K.G. and C.K.) and took place in three steps. First, the titles located from the search results were scanned, to exclude those outside the scope of the current study. Then the abstracts of all titles were examined by the reviewers. At this step, each reviewer produced a list of suitable articles. These lists were then combined, and both reviewers examined the pooled list independently. They read all study abstracts in the pooled list, and each produced a ‘short list’ of suitable articles. Discrepancies between reviewers in the ‘short lists’ were discussed, and a consensus was reached on whether or not the article(s) in question would be incorporated. A total of 55 articles were identified for inclusion at this stage. The reference lists of these articles were scanned and the selection of studies from the reference lists followed the same procedure outlined above. Another 12 publications extracted from reference lists were included in the review.
Data extraction and summarisation
The reviewers extracted data from half of the studies each. The study's details (i.e. the environmental factor(s) and dietary outcome(s) examined, whether environmental factors were objectively measured or self-reported, sample size, response rate, factors adjusted for in the analyses and the associations found) were summarised in data extraction tables.
In studies where sufficient data were available, effect sizes (ES) were calculated to interpret the magnitude of association of the environmental factors and make comparisons between studies. The formulae of CohenReference Mullen, Simons-Morton, Ramirez, Frankowski, Green and Mains23 were applied, adjusting for sample size. The magnitude of the ES were also interpreted according to the guidelines of Cohen, with cut-off points of 0.2–0.5 for small ES, 0.5–0.8 for moderate ES and >0.8 for large ES.
Results
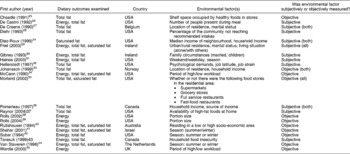
Twenty-seven of the 67 studies selected for detailed review were excluded because they were design/theoretical papers or only mentioned environmental factors in their Discussion sections. Nineteen articles were excluded because they did not examine energy, total fat or saturated fat intakes; therefore, 21 articles remained in the current review. Table 1 summarises the country where the study was conducted, the environmental factor(s) examined and their measurement. Most studies examined more than one dietary outcome, and were conducted in the USA (n = 11), UK/Europe (n = 6) or Canada/Australia/Israel (n = 4). Just less than half of the studies (n = 9) measured the environmental factors objectively. All studies were cross-sectional. Only one study used multilevel analysesReference Diez-Roux, Nieto, Caulfield, Tyroler, Watson and Szklo24; census block districts were the area level used in these analyses. All remaining studies were individual-level analyses.
Table 1 Details of included studies
The studies examined 81 associations between intakes and environmental factors, of which 41 were significant. Table 2 briefly summarises the associations found between environmental factors and each of the dietary intakes. This table shows that associations between environmental factors and intakes have been examined mostly for total fat consumption (39 associations were tested) compared with energy and saturated fat consumptions (22 and 20 associations were tested, respectively). Relatively few associations tested the potential influence of cultural factors on dietary intakes. There was little replication of studies testing the same hypotheses; often two associations were tested in different samples (e.g. men and women) from the same study.
Table 2 Summary of associations found in the reviewed articles
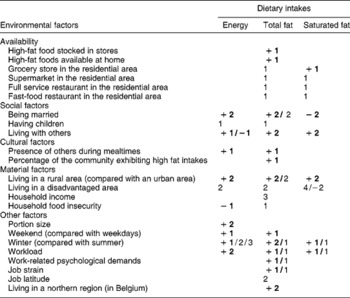
The numbers of significant effects found for the combination determinant–dietary outcome are given in bold; numbers not in bold are the number of non-significant effects found for the combination determinant–dietary outcome, or for which information on significance was not available.
+ indicates a positive association between environmental determinant and dietary outcome. – indicates a negative association between environmental determinant and dietary outcome.
Tables 3–5 detail the study characteristics and findings for each dietary outcome more extensively. For brevity, the following sections only describe findings for environmental factors for which two or more associations were tested.
Table 3 Results of studies examining environmental factors associated with energy intakes
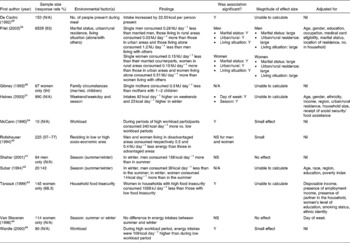
N/A – not available; Y – effect was statistically significant (P ≤ 0.05); NS – effect was not significant.
Table 4 Results of studies examining environmental factors associated with total fat intakes

N/A – not available; Y – effect was statistically significant (P ≤ 0.05); NS – effect was not significant.
Table 5 Results of studies examining environmental factors associated with saturated fat intakes

N/A – not available; Y – effect was statistically significant (P ≤ 0.05); NS – effect was not significant.
Associations between environmental factors and energy intakes
Table 3 details the characteristics and findings of studies examining associations between environmental factors and energy intakes. Fourteen of the 22 associations examined in these studies demonstrated a significant relationship between the environmental factor and energy intakes.
No studies looked at associations between availability factors (such as types of stores available and what they stocked) and energy intakes. The influence of social factors (i.e. being married, having children or living with others) on energy intakes was examined in a number of studies. Living with others demonstrated large associations with energy intakes that differed in direction for men and womenReference Friel, Kelleher, Nolan and Harrington29. One study found that men living alone had lower energy intakes than those living with others; however, lower energy intakes were found among women that lived with others. The same study found that marital status was strongly associated with energy intakes; intakes were higher among married participants compared with their single counterpartsReference Friel, Kelleher, Nolan and Harrington29.
Only one study examined associations between cultural factors (the presence of others during mealtimes) and energy intakes, while a number of studies looked at material factors. Urban/rural residence demonstrated a large association with energy intakes; men and women living in rural areas had greater energy intakes than those in urban areasReference Friel, Kelleher, Nolan and Harrington29. In a study that contrasted the energy intakes of men and women living in areas with different socio-economic characteristics, no differences were foundReference Rutishauser, Wheeler, Conn and O'Dea40.
Other potential determinants of energy intakes that were examined in other studies were portion size, weekday/seasonal variations in intakes, and associations between workload and energy intakes. Two studies demonstrated strong direct effects between portion sizes and energy intakesReference Rolls, Morris and Roe38, Reference Rolls, Roe, Kral, Meengs and Wall39. Seasonal variations in intakes were measured in countries differing considerably in their climate (USA, Israel and Europe), and mixed associations were seenReference Haines, Hama, Guilkey and Popkin31, Reference Shahar, Yerushalmi, Lubin, Froom, Shahar and Kristal-Boneh41, Reference Subar, Frey, Harlan and Kahle42, Reference van Staveren, Deurenburg, Burema, de Groot and Hautvast44. Two studies found small differences in mean energy intakes between winter and summer, one found that intakes were marginally lower in winter among menReference Subar, Frey, Harlan and Kahle42 while another study among men found that energy intakes were slightly higher in winterReference Shahar, Yerushalmi, Lubin, Froom, Shahar and Kristal-Boneh41. A study among women found no seasonal variation in energy intakesReference van Staveren, Deurenburg, Burema, de Groot and Hautvast44. Greater energy intakes have been associated with higher workload in two studies, but the magnitude of these effects was smallReference McCann, Warnick and Knopp34, Reference Wardle, Steptoe, Oliver and Lipsey45.
Associations between environmental factors and total fat intakes
Studies examining associations between environmental factors and total fat intakes are described in Table 4. Sixteen of the 39 associations tested reached statistical significance.
There were no associations between availability factors and total fat intake that were replicated. A number of studies examined potential social determinants of fat intakes. Marital status and living situation demonstrated large effects on fat intakes in an Irish studyReference Friel, Kelleher, Nolan and Harrington29 and showed that being married or living with others was associated with higher fat intakes compared with being single or living alone. However, a Belgian study found no association between marital status and fat intakesReference De Craene, De Backer, Kornitzer, De Henauw, Bara and Rosseneu27.
There were no replicated associations tested for any cultural factors and total fat intake. However, a number of studies examined associations with material factors. A US study found that living in a rural area was associated with a higher fat intake, and the Es of this relationship was largeReference Friel, Kelleher, Nolan and Harrington29. However, a Norwegian study found no significant urban/rural differencesReference Johansson, Thelle, Solvoll, Bjorneboe and Drevon33. Fat intakes in relation to the socio-economic characteristics of the residential area were examined in one study, but no significant association was foundReference Rutishauser, Wheeler, Conn and O'Dea40. Two studies examined the economic circumstances of households in relation to fat intakes, and took a number of confounding factors into account, but found that household income was not associated with fat intakesReference Johansson, Thelle, Solvoll, Bjorneboe and Drevon33, Reference Pomerleau, Pederson, Ostbye, Speechley and Speechley36.
The majority of studies examined associations with other factors. There were mixed findings about seasonal variations in fat intake. Two small studies (one in Israel and one in Europe) demonstrated higher fat intakes in winter compared with summerReference Shahar, Yerushalmi, Lubin, Froom, Shahar and Kristal-Boneh41, Reference van Staveren, Deurenburg, Burema, de Groot and Hautvast44; however, a US study found very marginal differences in fat intakes between seasonsReference Subar, Frey, Harlan and Kahle42. Three studies examined associations between work conditions, such as psychological demands, job strain and workload, and fat intakesReference Hellerstedt and Jeffery32, Reference McCann, Warnick and Knopp34, Reference Wardle, Steptoe, Oliver and Lipsey45. One study found no association between psychological demands and job strain and women's fat intakes, whereas men with high psychological demands and high job strain consumed more fat than their counterparts with low psychological demands and low job strainReference Hellerstedt and Jeffery32. A small study showed a positive relationship of moderate magnitude between workload and fat intakesReference McCann, Warnick and Knopp34, whereas another study found no association between work stress and fat intakesReference Wardle, Steptoe, Oliver and Lipsey45. Location of residence also showed a relationship with fat intakes in a Belgian study, which illustrated significant regional differences in fat consumptionReference De Craene, De Backer, Kornitzer, De Henauw, Bara and Rosseneu27.
Associations between environmental factors and saturated fat intakes
Studies examining associations between environmental factors and saturated fat intakes are shown in Table 5. Nine of the 20 associations tested were statistically significant.
Similar to the situation reported for energy and total fat intakes, no associations with availability factors were replicated. Studies that examined potential social determinants found that single adults had moderately higher saturated fat intakes than their married counterparts, and that these differences were largeReference Friel, Kelleher, Nolan and Harrington29. The same study found a large positive association between saturated fat intake and living alone; participants that lived alone had higher intakes compared with those living with othersReference Friel, Kelleher, Nolan and Harrington29.
No studies examined associations between saturated fat intakes and cultural factors; however, a number looked at the potential influence of material factors. Living in an urban area was associated with higher intakes in one studyReference Friel, Kelleher, Nolan and Harrington29, and the differences in intakes between urban and rural areas were large in magnitude. The influence of living in a deprived neighbourhood was examined in two studiesReference Diez-Roux, Nieto, Caulfield, Tyroler, Watson and Szklo24, Reference Rutishauser, Wheeler, Conn and O'Dea40; both found no significant differences in saturated fat consumption between people residing in socio-economically contrasting areas. A US study found that household income was positively related to saturated fat intakes among men and womenReference Diez-Roux, Nieto, Caulfield, Tyroler, Watson and Szklo24.
A number of other studies looked at the potential influence of other factors on saturated fat intakes. A study among men in Israel showed that saturated fat intakes were moderately higher in winter compared with summerReference Shahar, Yerushalmi, Lubin, Froom, Shahar and Kristal-Boneh41. However, no significant seasonal differences in saturated fat intakes were seen among women in The NetherlandsReference van Staveren, Deurenburg, Burema, de Groot and Hautvast44. Of two studies examining the influence of working conditions, one showed that workers consumed slightly (but significantly) more saturated fat during periods of high workloadReference McCann, Warnick and Knopp34, but the other found that intakes were not different during periods of high work stressReference Wardle, Steptoe, Oliver and Lipsey45.
Discussion
We performed a systematic review of the literature examining associations between environmental factors and energy, total and saturated fat intakes. Potentially relevant environmental factors from social–ecological models for health behaviours (such as availability, social, cultural and material conditions) were relatively understudied in relation to these specific dietary outcomes – research has predominantly focused on other environmental influences (i.e. season/day of the week variation, work-related factors). Few studies have examined the specific environmental factors that have been implicated in the obesity epidemic, such as fast-food/convenience stores, marketing of unhealthy foods and larger portion sizes. Therefore, it is too premature to conclude that the environment does or does not play an important role in unhealthy dietary behaviour among the adult population at the current time.
Both the public and health professionals have a great deal of interest in the presumed impact of the food environment on weight gain and health. However, our systematic review indicates that these notions are currently not well supported by scientific evidence. The evidence base in this area still needs to grow before extensive investment in developing environmental interventions to bring about dietary change can be justified. How can we tackle this?
First, there is a need for more theoretical growth in this area before our knowledge can be advanced by further research. Research on environmental factors associated with dietary intakes needs to develop beyond the phase of merely reporting associations between environmental factors and dietary intakes. The relationship between the environment and how it influences food choice needs to be conceptualised. There needs to be some more empirical thought given to which environmental factors are most likely to be related to dietary intakes, i.e. are they accessibility and availability issues, social factors, cultural conditions and/or material factors? There needs to be some consideration given to the pathways/mechanisms by which environmental factors are likely to influence intakes. Most studies included in the review examined associations between environmental factors and dietary intakes without stating clear hypotheses regarding the underlying mechanisms. Being aware of the mechanisms by which environmental factors influence dietary intakes is necessary so that the research can be translated into effective interventions among the population. For example, does the actual environment influence people's behaviour, or are people's perceptions of the environment a stronger influence? Another question is whether the environment operates directly on dietary behaviour, or whether its influence is mediated through other environmental-level factors (e.g. urbanisation or area deprivation) or individual-level factors (e.g. self-efficacy or nutrition knowledge). Existing conceptual models are of some assistance, but these are still in their formative stages. Some ecological theories of health behaviour may also offer some direction; however, they are also limited as they list and categorise potential environmental factors but do not specify how they influence behaviourReference Brug, Oenema and Ferreira46. Further development of this theory is necessary to facilitate the formation of recommendations for health practitioners and for deriving hypotheses to be tested in subsequent research. We should also take advantage of knowledge from other fields of research such as sociology, urban geography and economy, as these fields know much about the consequences of physical and/or social deterioration in neighbourhoods. Fields such as economics have a stronger knowledge about the effects of advertising and the way people spend their money. Cross-fertilisation of knowledge from different fields may be the key to growth in this area.
Furthermore, the influence of the environment needs to be examined in relation to other ‘traditional’ (i.e. individual-level) determinants of dietary behaviourReference Kremers, Visscher, Seidell, van Mechelen and Brug47. No known study has simultaneously looked at the relative influence of (and interaction between) environmental and individual-level factors on dietary behaviour. Examining the relative influence of factors at different levels is an important step to help determine where research to understand how dietary behaviour, and interventions and resources to bring about behaviour change, could be best targeted.
Stronger study designs will also help to unravel the relationship between the environment and dietary behaviour. All the studies in the current review were observational and examined cross-sectional associations between environmental factors and dietary intakes. These study designs provide an indication of significant associations, but are limited for examining causal relationships between the factors of interest and dietary intakesReference French, Story and Jeffery48. Longitudinal and experimental study designs would enable environmental determinants (rather than correlates) of dietary behaviour to be identified. The use of ‘natural experiments’ (e.g. examining intakes of residents before and after the opening of a takeaway food store, or making cross-country comparisons to examine the influence of cultural factors) may offer opportunities to examine the influence of environmental factors that are difficult to manipulateReference Petticrew, Cummins, Ferrell, Findlay, Higgins and Hoy49.
Our search strategy only located studies that were published in peer-reviewed journals and referenced in electronic databases; therefore, they may be influenced by publication bias. We tried to minimise this by also performing searches in smaller and more specialised databases. The studies included in the review tested 81 associations, of which 41 were found to be significant, suggesting that publication bias may have played a role in the current study with an over-representation of studies showing significant effects. Other limitations that may have influenced the study findings were differences in the conceptualisation, measurement and summary of the environmental determinants and/or dietary intakes in the different studies. Even though strict inclusion criteria were used, environmental or dietary intake measurements sometimes differed markedly between studies, and may have contributed to variation in the associations found.
The findings of this review suggest that there is currently insufficient evidence to conclude that environmental factors do or do not influence obesogenic or unhealthy dietary behaviours. Further research needs to examine the environmental factors that the current literature implicates as part of an obesogenic environment, as we found few studies that examined these factors. The evidence base in this area still needs to grow in the ways mentioned above, before practice recommendations can be made or extensive investment in developing environmental interventions to bring about dietary change can be justified. Examination of environmental factors associated with dietary habits preceding energy and fat intakes (such as food choice and habits) may help to unravel further whether the environment influences health outcomes through dietary behaviour. Additionally, study replication is necessary to confirm or disprove the findings of previous studies.
Acknowledgements
Sources of funding: K.G. is supported by an Australian National Health and Medical Research Council (NHMRC) Sidney Sax International Post Doctoral Fellowship (grant identification number: 290540). The project was funded by the Netherlands Organisation for Health Research and Development. K.G. conceptualized and wrote the manuscript.
Conflict of interest declaration: None.
Authorship responsibilities: K.G. and C.K. searched for and synthesised the manuscripts. The remaining co-authors offered valuable input and feedback on the manuscript.
Acknowledgements: The authors wish to thank Gert-Jan de Bruijn for his useful comments on an earlier draft of the manuscript.





