



Public health education campaigns, including mass media and social marketing campaigns, aim to increase knowledge and awareness of the importance of specific health behaviours, with the ultimate goal of promoting public health(1,Reference Carins and Rundle-Thiele2) . These campaigns can lead to positive health behaviour changes or prevent negative changes, often with small but measurable population-level effects(Reference Wakefield, Loken and Hornik3–Reference Snyder5). Nutrition education campaigns typically aim to communicate general healthy eating messages, alter consumption of specific nutrients or foods or raise awareness of national food-based dietary guidelines (FBDG), and are often combined with messages about increasing physical activity(Reference Hawkes6). However, education campaigns are generally associated with increased awareness and understanding of healthy eating concepts more than improved uptake of behaviours or health outcomes(Reference Keller and Lang7–11). Indeed, a Canadian study found that use and knowledge of the information in national FBDG were low(Reference Vanderlee, McCrory and Hammond12). This highlights the need for effective mass media campaigns to increase knowledge of intake recommendations and encourage healthy behaviours.
Mass media and social marketing campaigns may have relatively small effect sizes in terms of behaviour change(Reference Snyder, Hamilton and Mitchell4), but the population impact can be considerable given their reach. Effective campaigns typically include well-designed messages based on formative research and have sufficient frequency and reach to be recalled by the target audience(Reference Abroms and Maibach13). Broad-reaching campaigns with opportunities for multiple exposures are critical given the cluttered information environment in which consumers receive frequent marketing messages from the food industry, which can often conflict or distract from public health messaging. At the same time, achieving broad reach can be expensive given the cost of implementation. One of the key questions in evaluating mass media campaigns is the extent to which consumers can recall the campaign or its key messages. Message recall is an important outcome as it represents a relatively ‘objective’ measure that is uninfluenced by social desirability bias(Reference McGuire14). Message recall and recognition tasks do not simply measure ‘exposure’; they also reflect a consumer’s level of cognitive processing, which is associated with comprehension and attitudes. Indeed, greater understanding of a message leads to improved message acceptance and recall. As a result, message recall is often used as an indicator of advertising reach and impact(Reference McGuire14–19).
Given the call for further monitoring and evaluation of education campaigns and FBDG(11,20) , the current study aimed to examine awareness and recall of healthy eating campaigns across the five countries examined in the International Food Policy Study (IFPS): Australia, Canada, Mexico, UK and the USA. A brief overview of the campaigns implemented in each country prior to or during the study period (November to December 2018) is provided below. Related literature available from published campaign evaluations is also included, when available. The date of the latest revisions to each country’s FBDG is also provided for context.
Australia
In Australia, approximately one hundred campaigns and programmes focused on diet and healthy living were implemented either by the Australian Federal Government, state and territory governments, or large health-related non-governmental organisations (NGO) in the decade preceding the study, 90 % of which continued into 2018. These included LiveLighter®, a healthy lifestyle promotion and education programme implemented in Victoria, Western Australia, and to a lesser extent, Northern Territory and Tasmania that encouraged individuals to eat healthily, be active and maintain a healthy weight, including, among other aspects, the use of graphic imagery designed to elicit shock(21). An early evaluation found that the majority (54 %) of respondents were aware of the LiveLighter campaign, with higher recall among parents and adults with overweight(Reference Morley, Niven and Dixon22). A later study found higher post-campaign awareness (67 %), including high viewership among respondents residing in areas of low socio-economic status (SES). It also found increased knowledge of the health risks of sugar-sweetened beverage (SSB) consumption, decreased SSB consumption among frequent SSB consumers as well as overweight SSB consumers, and an overall reduction in sugary food intake(Reference Morley, Niven and Dixon23). Another study examined the LiveLighter® Sugary Drinks campaign, which centred around the visceral ‘toxic fat’ that accumulates around organs and leads to negative health consequences. The study reported general campaign success, with a significant decrease in frequent SSB consumption and increased knowledge of the health risks of SSB intake in Victoria compared with South Australia (control state)(Reference Morley, Niven and Dixon24). The healthy lifestyle campaign Make Healthy Normal, implemented in New South Wales, was associated with high campaign recognition (45 %), yet only 9 % of respondents could freely recall the campaign(Reference Kite, Gale and Grunseit25). Qualitative research found high familiarity with the Go for 2&5 fruits and vegetables (FV) campaign, which was implemented in all states except Victoria, but poor understanding of serving sizes and low acceptance of the recommended number of servings(Reference Carter, Pollard and Atkins26). The most recent Australian Dietary Guidelines were revised in 2013 and include the Australian Guide to Healthy Eating, a plate-based model to depict recommended foods. While the Australian Dietary Guidelines underpin nutrition policy in Australia and form the basis of the majority of nutrition education material produced and delivered by Australian governments, at the time of writing there had been no major nationally coordinated media campaigns to promote the 2013 Australian Dietary Guidelines. In addition, Nutrition Australia (a national NGO and not-for-profit organisation) produced a healthy eating pyramid that also reflects the Australian Dietary Guidelines, first released in 1982 and most recently updated in 2015(27,28) .
Mexico
Several mass media campaigns focusing on healthy eating and physical activity were implemented prior to or during the study period. The primary campaign was Chécate, Mídete, Muévete (Check, Measure and Move), a national campaign which aims to prevent overweight and obesity through healthy diet, physical activity and regular physical check-ups(Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29). Chécate, Mídete, Muévete was originally introduced in 2013 as part of the broader PrevenIMSS programme, conducted by the public healthcare agency Instituto Mexicano del Seguro Social (IMSS). Later, the campaign was scaled up at the national level and adopted by other governmental healthcare providers, including the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE) through the PrevenISSSTE programme, and the Secretaría de Salud (Ministry of Health). A 2016 study found 11 % awareness of the Chécate, Mídete, Muévete campaign, whereas a report by the Ministry of Health indicated that 57·4 % of survey respondents knew of the campaign(30). In the latter study, among those aware of the campaign, comprehension of campaign concepts ranged from 13·5 % for the ‘Check’ component to 53·1 % for the ‘Measure’ component and 85·1 % for the ‘Move’ component(30). Both studies found higher awareness among women(Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29,30) . Higher awareness was also found among those with higher education, those with overweight or obesity(Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29), adults aged 20–39 years and those residing in urban centres(30). The Mexican FBDG, which feature a plate model, were last revised in 2015(31).
United Kingdom
Numerous mass media campaigns were implemented by national and regional health authorities in the UK in the years preceding the study. While some were implemented specifically in Scotland or Northern Ireland, the majority were conducted across the UK. These included Change4Life, a national diet and lifestyle campaign conducted by the National Health Service which comprises several diet-related sub-campaigns (e.g., 5 A Day, Sugar Swaps, 100 Calorie Snacks – 2 a Day Max) aimed at parents and families(32). A randomised trial found that Change4Life was associated with a high level of interest and awareness (75–96 %), but few changes in attitudes or behaviours(Reference Croker, Lucas and Wardle33). The UK dietary guidelines (Eatwell Plate) were rebranded as the EatWell Guide in 2016(34).
United States
In the USA, the primary campaign was the Obama administration’s 2010–2018 Let’s Move, a national programme which focused on physical activity and dietary habits(35). The US FBDG (MyPyramid) were rebranded as MyPlate in 2011(36).
Several studies have examined nutrition education campaigns in the USA. Community-based mass media campaigns have been associated with positive dietary changes, including reductions in saturated fat and cholesterol(Reference Stern, Farquhar and McCoby37) and shifts from high- to low-fat milk(Reference Reger, Wootan and Booth-Butterfield38) in US intervention compared with control communities. However, public education campaigns aiming to increase FV consumption have led to increased intake only in specific sub-samples, such as Hispanic and non-smoking respondents or Spanish speakers(Reference Stables, Patterson and Dodd39,Reference Backman and Gonzaga40) . Regarding campaign awareness, a 2007 study found that < 10 % of respondents were aware of the National Cancer Institute’s Fruits and Veggies – More Matters national campaign and associated serving recommendation. In comparison, the former 5 A Day campaign had greater reach (29 % familiarity), and campaign awareness was associated with following the serving size recommendation(Reference Erinosho, Moser and Oh41).
Canada
In Canada, no major dietary campaigns took place in the years leading up to the study. The 2015 Nutrition Facts Education Campaign, which aimed to increase understanding of the serving size and percent daily value on prepackaged foods, was the most recent national dietary campaign(42). A 2016 study reported low knowledge of the percentage daily value messaging communicated in the campaign(Reference Cormier, Vanderlee and Hammond43). It was announced that revisions to Canada’s FBDG would be implemented shortly after the current study period, in January 2019(44).
Study objectives
The objectives of this descriptive study were to: (1) test differences in awareness of healthy eating campaigns among respondents in the five countries, including by socio-demographic factors; (2) identify the campaign key messages mentioned by respondents and (3) identify the specific campaigns recalled by respondents. Given the greater presence of mass media campaigns in Australia, Mexico and the UK compared with Canada and the USA, higher awareness and campaign recall were expected in the former three countries.
Methods
Data are from the 2018 IFPS, conducted in Australia, Canada, Mexico, the UK and the USA. Data were collected via self-completed web-based surveys with adults aged ≥18 years. Respondents were recruited through Nielsen Consumer Insights Global Panel and their partners’ panels. Email invitations with unique survey access links were sent to a random sample of panelists within each country after targeting for demographics; panelists known to be ineligible due to age or country of residence were not invited. Potential respondents were screened for eligibility and quota requirements using age, sex and minimum device screen size (to restrict respondents from completing the survey on a smartphone). Surveys were conducted in English in Australia and the UK; Spanish in Mexico; English or French in Canada; and English or Spanish in the USA. Median time to survey completion was 40 min.
Respondents provided consent prior to completing the survey. Respondents received remuneration in accordance with their panel’s usual incentive structure (e.g., points-based or monetary rewards, chances to win prizes). A full description of the study methods can be found in the IFPS: Technical Report – 2018 Survey (Wave 2)(Reference Hammond, White and Rynard45).
Measures
Socio-demographic variables included country (Australia, Canada, Mexico, UK, the USA), age (continuous), sex at birth (male, female), ethnic group (majority, minority, unstated), highest level of education (low, medium, high, unstated) and perceived income adequacy (assessed by inquiring about the respondent’s ‘ability to make ends meet’; very difficult, difficult, neither easy nor difficult, easy, very easy). Original item wording is available in the IFPS 2018 survey. Country-specific measures for education and ethnicity were used in each country; coding of these measures is available in the IFPS: Technical Report – 2018 (both available at www.foodpolicystudy.com/methods); see Table 1 for coding of response options.
Table 1 Weighted sample characteristics, 2018 International Food Policy Study (n 22 463)

* Ethnicity was categorised as ‘majority’ if participants identified themselves as ‘white’, predominantly English-speaking or non-Indigenous; criteria were based on the most appropriate terminology in each country.
† Education was coded as low, medium or high according to country-specific criteria related to the highest level of education completed.
‡ Respondents with implausible height and/or weight were grouped with unstated BMI.
BMI classification was based on reported height and weight (underweight (<18·5), normal weight (18·5–24·9), overweight (25·0–29·9), obese (≥30))(46). Those with missing or implausible values were classified as unstated because there are potentially important differences among those who do not report their height and weight in population-level surveys(Reference Read, Lewis and Halbesma47).
Awareness of healthy eating campaigns was assessed by asking, ‘Do you remember seeing any educational messages or campaigns on healthy eating from the government or health authorities in the past 12 months?’ (yes, no, don’t know, refuse to answer). For the purposes of this paper, health authorities included international agencies such as the WHO, as well as country-specific health-based NGO.
Recall of healthy eating campaigns was assessed using an unaided recall technique(Reference Niederdeppe48). Those who responded ‘yes’ to the question above were asked, ‘Can you briefly describe the message or campaign?’ (open-ended).
Data analysis
A total of 28 684 adults completed the survey. After excluding 5860 respondents for missing region of residence or poor data quality (including failing to select the current month from a list), the analytic sample comprised 22 824 respondents. A sub-sample of 22 463 (Australia: n 4083; Canada: n 4238; Mexico: n 4064; UK: n 5466; the USA: n 4612) was included in the current analysis after excluding respondents who refused to answer the campaign recall question (n 28) or had missing data on ethnicity or education (n 333). Data were weighted with post-stratification sample weights constructed using a raking algorithm with population estimates from the census in each country based on age group, sex, region, ethnicity (except in Canada) and education (except in Mexico). Estimates reported are weighted unless otherwise specified.
Content analysis was conducted such that the first author coded all open-ended descriptions of healthy eating campaigns and developed a coding scheme based on unique keywords that emerged from responses. A second investigator independently coded 20 % of all English-language responses and 100 % of French responses, and a third investigator coded 100 % of Spanish responses. Inter-rater reliability, calculated using joint probability of agreement, was 91·1 % (English and French: 95·3 %; Spanish: 86·0 %); remaining discrepancies were resolved via discussion.
Investigators in each country identified lists of campaigns a priori using a structured search strategy. Investigators searched the websites of governments and health authorities responsible for health and nutrition, as well as Google and Google Scholar, to identify campaigns related to healthy eating that took place in a 5-year period preceding and immediately following the study (2015–2020). For each campaign identified, investigators listed the campaign name, dates, agency or organisation, website, key messages and any other associated campaign elements. Recall of specific campaigns was determined by matching respondents’ open-ended responses to the keyword lists and information collected in the search strategy.
Recall of keywords and specific campaigns were reported using descriptive statistics. An adjusted logistic model regressed awareness of a healthy eating campaign (1 = yes; 0 = no/don’t know) on country, adjusting for age group, sex, ethnic group, education level, perceived income adequacy and BMI classification. Adjusted OR are reported. After stratifying the data by country, separate binary logistic regression models were also conducted to evaluate differences in awareness of healthy eating campaigns across levels of each of the aforementioned socio-demographic variables. Analysis was conducted using SAS Studio release 9·4.
Results
Sample characteristics in each country are shown in Table 1. Approximately half the sample was female (51·3 %), 80 % were part of a majority ethnic group and over one-third (34·8 %) had a high education level.
Overall awareness of healthy eating campaigns
A total of 21·5 % (4824) respondents across all countries reported seeing a public health campaign on healthy eating in the past 12 months. General awareness of healthy eating campaigns varied significantly by country. As shown in Table 2, respondents in Mexico (50·9 %) were significantly more likely to report seeing a healthy eating campaign compared with those in the UK (18·2 %), Australia (17·9 %), the USA (13·0 %) or Canada (10·2 %). Respondents in both Australia and the UK were also more likely to report seeing a campaign than respondents in Canada or the USA, whereas there was no difference between those in Australia and the UK. Respondents in the USA were more likely to report seeing a campaign than respondents in Canada.
Table 2 Proportion of respondents who reported seeing a healthy eating education campaign, among all respondents (n 22 463)

AOR, adjusted OR; ref, reference group.
Binary logistic regression model tested for odds of reporting seeing a healthy eating campaign (yesv. no/don’t know).
Significant effects (P < 0·05) are indicated in bold.
The model also revealed several socio-demographic differences in campaign awareness. Overall, males (22·8 %) and those with medium (19·5 %) or high (30·3 %) education levels were significantly more likely to report seeing a campaign than females (20·2 %) and those with low education levels (15·4 %), respectively. Those classified as having unstated BMI (29·9 %) were significantly more likely to report seeing a campaign than those with normal weight (20·9 %), with no differences observed between other BMI classifications (P > 0·05). As age increased, respondents were significantly more likely to report seeing a campaign. There was no main effect of ethnic group or perceived income adequacy (Table 2).
As shown in Table 3, when examining socio-demographic differences in campaign awareness in each country separately, the same basic pattern of results emerged, with some exceptions. For example, significantly higher likelihood of awareness among males compared with females was found only in Canada, Mexico and the USA. Significant differences in awareness by education were observed, whereby likelihood of awareness was significantly higher in those with a high level of education (except in Canada) or medium level of education (except in Canada and Mexico). Differences by BMI classification were also observed in all countries except Mexico: compared to those with normal weight, those with unstated BMI were significantly more likely to report seeing a campaign. Additionally, in the UK, those with overweight were significantly less likely to report seeing a campaign than with normal weight. As per above, there was no effect of income adequacy in any country. Significantly higher likelihood of awareness was also observed among older respondents in the UK and among minority groups in the USA.
Table 3 Proportion of respondents who reported seeing a healthy eating education campaign, among all respondents in each country (n 22 463)

Ref, reference group,X 2, chi-squared test.
†Separate logistic regression models were conducted in each country, testing for odds of reporting seeing a healthy eating campaign (yesv. no/don’t know). Proportions that are significantly different from the reference group are bolded and indicated with asterisks (*P < 0·05, **P < 0·01, ***P < 0·001); significantχ 2 tests (P < 0·05) are also indicated in bold.
Key messages mentioned by respondents
Of the 4824 respondents who reported seeing a campaign, 3711 provided ‘valid’ responses. The remaining responses were nonsensical (n 106), irrelevant comments or qualitative campaign feedback (e.g., ‘Great’) (n 319), did not specify the message in the campaign (n 473) or described the source but not content of the message (n 215). Figure 1 shows the top ‘keywords’ mentioned in open-text responses by the subgroup of respondents who provided a ‘valid’ answer when asked to describe the message or campaign they saw. Online supplementary material (Supplemental Table 1) shows frequencies of all identified keywords among all respondents. As shown in Fig. 1, whereas respondents in Canada and the USA were most likely to make generic references to healthy eating or dietary habits, the most common keywords mentioned in valid responses in the UK and Australia were sugar (35·6 %) and sugary drinks (27·1 %), respectively. Indeed, sugar, sugary drinks and/or sugar taxes were common campaign topics overall and were mentioned in at least 6 % of valid responses in each country. FV were also commonly mentioned in all countries, ranging from 8·6 % of responses in Mexico to 17·8 % in the UK. Many respondents also mentioned physical activity: it was by far the most commonly used keyword in Mexico (35·1 %), the third-most common in Australia (13·7 %) and was mentioned in 8·9–10·6 % of responses in the remaining countries.
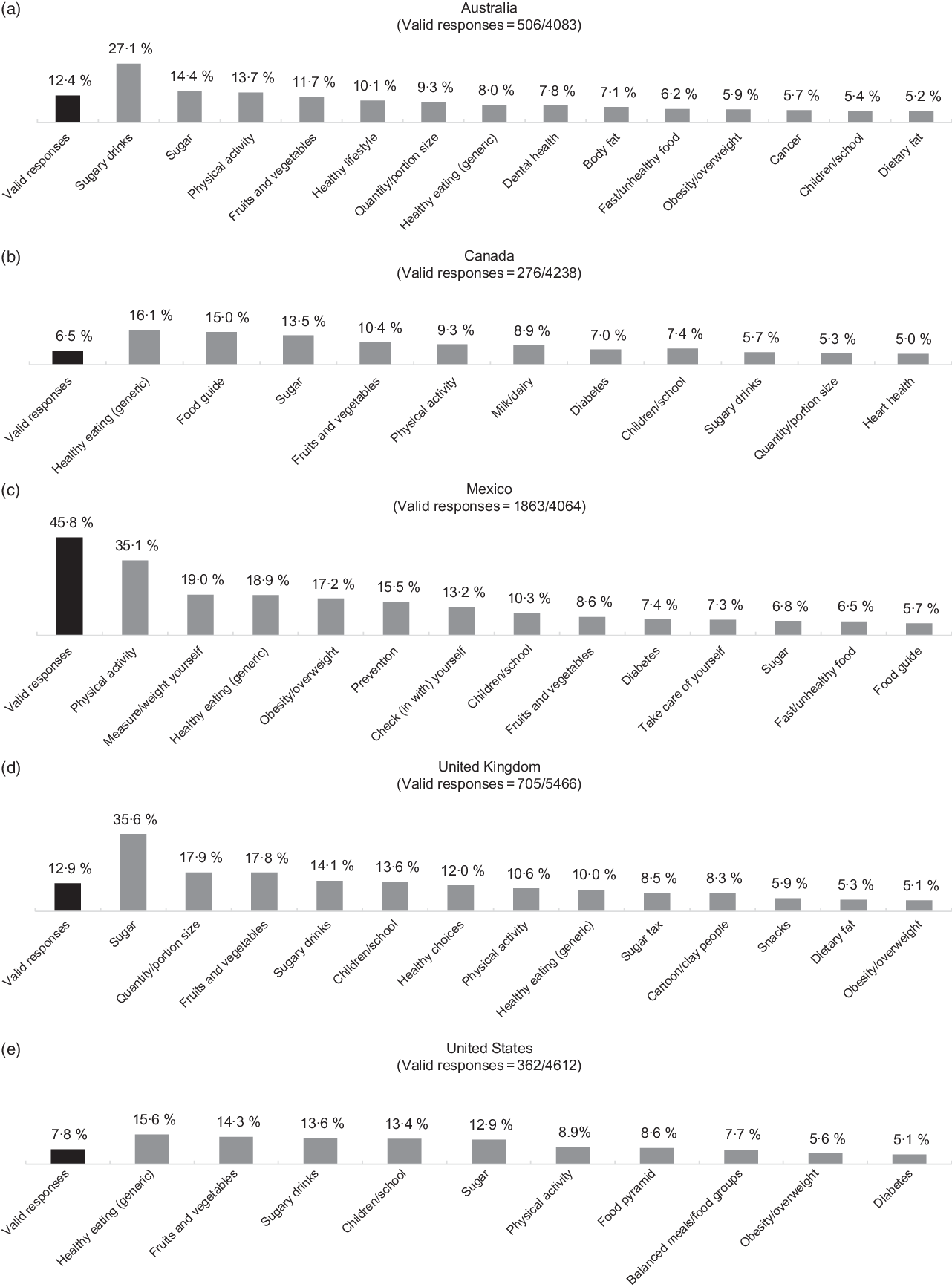
Fig. 1 Keywords mentioned by at least 5 % of respondents in each country who provided valid answers to the question, ‘Do you remember seeing any educational messages or campaigns on healthy eating from the government or health authorities in the past 12 months?’ (n 3711)*. *Of the 4824 respondents who reported seeing a campaign, 3711 provided valid responses. The remaining responses were nonsensical (n 106), irrelevant comments or qualitative campaign feedback (e.g., ‘Great’) (n 319), did not specify the message in the campaign (n 473) or described the source but not content of the message (n 215). Values shown for keywords are proportions of the total valid responses in each country
Specific campaigns recalled
Across countries, three of the top five ‘campaigns’ freely recalled were from Mexico, and two were from the UK and Australia: (1) Chécate, mídete, muévete (Mexico;n 451); (2) PrevenIMSS (Mexico;n 280); (3) Change4Life (UK;n 171); (4) LiveLighter® (Australia;n 104) and (5) Actívate, Vive Mejor (Mexico;n 86). As shown in Table 4, national FBDG were among the top 10 ‘campaigns’ mentioned in all countries except Mexico, where La jarra del buen beber – a more widely known pictorial guide to healthy beverage intake developed by the government(49) – was among the top 10.
Table 4 Top 10* education campaigns mentioned in unaided recall task, among all respondents in each country (n 22 463)

* Campaigns with the same proportion of responses are separated by semi-colons.
Discussion
Study results showed that across countries, respondents in Mexico were substantially more likely to report seeing a healthy eating campaign. This higher campaign awareness appears to be largely associated with Chécate, Mídete, Muévete, which was implemented from 2013 to 2019 and was one of the few campaigns in the country with continued social media presence in 2018. The campaign’s ongoing nature and salient advertisements, which included a catchy jingle(Reference Sánchez-Reina and Fuentes50) and paid dissemination through TV, radio, print media and the internet, among other avenues, may have contributed to its wide reach and shaping of public opinion. In fact, the presidential administration drastically overspent its social communication budget in 2018, with the Ministry of Health reporting the largest spending on social communication(51). Overall, the campaign was recalled by 24·2 % of Mexicans who provided a valid open-text response – or 11 % of all Mexican respondents – consistent with the 11 % of Mexican survey respondents who were aware of the campaign in a 2016 study(Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29), but substantially lower than the 57 % reported by the Ministry of Health(30). The latter study may have used a recognition task, which generally leads to higher awareness (see below). Both the 2016 study and the current study found higher campaign awareness among those with higher education levels(Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29); however, unlike previous studies which found significantly higher campaign awareness among women(Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29,30) , the current study found similar campaign awareness across the sexes, with males slightly more likely to recall the campaign than females.
As expected, respondents in the UK and Australia also had higher overall awareness of healthy eating campaigns compared with Canada and the USA, although they followed Mexico by a wide margin (<20 % awareness in both countriesv. 51 % in Mexico). Several of the major mass media campaigns described earlier, including Change4Life in the UK and LiveLighter® in Australia, were among the top campaigns described by respondents, indicating their wide reach (see Table 3). Free recall is generally lower than recognition(Reference Niederdeppe48), which may explain the lower levels of campaign awareness found in the presentv. previous studies which asked participants about specific campaigns(Reference Morley, Niven and Dixon22,Reference Morley, Niven and Dixon24,Reference Croker, Lucas and Wardle33) . Numerous campaigns on healthy eating occurred in both Australia and the UK during the study period, and there may be several reasons for the lower level of awareness compared with Mexico. For one, many campaigns identified were implemented only in specific states/regions rather than nationally, were targeted at specific settings or subgroups and may be better described as social marketing campaigns, which utilise marketing concepts to encourage socially responsible behaviours(1,Reference Carins and Rundle-Thiele2) . Additionally, campaigns launched in the months preceding the study may not yet have garnered sufficient exposure to be freely recalled.
In Canada and the USA, where there were few major mass media campaigns on healthy eating in the years preceding the study, FBDG were the most commonly recalled message about healthy eating. This suggests an overall awareness of the existence of FBDG in both countries, perhaps at least partially attributed to dissemination by schools and medical practices, resulting in established knowledge of the FBDG among adults. Additionally, in Canada, many respondents may have heard about the upcoming revisions to the national FBDG(44). In the USA, FBDG were the top two messages listed, with more respondents mentioning the food pyramid than the plate model, despite the fact that MyPlate was released more recently (2011) than MyPyramid (2005)(52). Interestingly, the food pyramid was mentioned in all countries, despite the USA being the only country examined that had a pyramid model in 2018. In Australia, this may be attributed to the fact that the NGO Nutrition Australia has used a food pyramid since the 1980s and continues to update it (in line with the Australian Dietary Guidelines), despite the Australian Government’s introduction of a plate model in 1998(27,28) . Similarly, Mexico utilised a pyramid model before the Plato del buen comer (plate model), which was introduced in 2006(53). Respondents in other countries may have been exposed to the pyramid model via sharing of online resources.
Memory biases may have been at play in the current study, such as forward telescoping, in which more distant events feel more recent, or the spacing effect, in which memory is enhanced with repeated exposures spread out over time(Reference Lavrakas54). Indeed, several of the top 10 campaigns listed in each country were either ongoing (e.g., Australia: LiveLighter®, Healthier Happier, Rethink Sugary Drink, Make Healthy Normal, Try for 5; Canada: ParticipACTION; Mexico: PrevenIMSS, PrevenISSSTE; UK: Change4Life, 5 A Day, Eatwell Guide, Sugar Swaps, One You; the USA: Let’s Move) or no longer in effect at the time of the study (e.g., Australia: Go for 2&5; Mexico: Actívate, Vive Mejor; the USA: Pouring on the Pounds). As in Mexico, the major campaigns recalled in Australia and the UK – including LiveLighter®, Healthier Happier, Change4Life and 5 A Day – were conducted over multiple years and still actively promoted (in some cases, since the early 2000s), which likely contributed to their recall.
In addition, although participants were asked about healthy eating campaigns run by governments or health authorities, several commercially sponsored and/or physical activity-related campaigns were recalled. This may have stemmed from the public’s lack of awareness regarding the agency responsible for producing each campaign (e.g., government, NGOv. Commercially sponsored campaigns). Indeed, the top four campaigns recalled across countries included elements of both healthy eating and physical activity, and the fifth focused exclusively on physical activity. Commercially sponsored and/or physical activity campaigns were recalled especially in Canada and the USA, where there were few government-run campaigns about healthy eating. For example, the well-known physical activity programmes ParticipACTION and Body Break were among the top 10 campaigns recalled in Canada, as was Carrot Rewards, an industry-sponsored mobile application that allowed consumers to earn rewards points by increasing their step count. In the USA, after the FBDG, the next most commonly cited programme was the Obama administration’s Let’s Move campaign, which encouraged both healthy eating and physical activity(35). The Got Milk? campaign, which promotes milk consumption and is sponsored by the dairy industry, was also among the top 10 in the USA(55). In Mexico, the most frequently mentioned keyword was physical activity, in line with previous reports indicating that the ‘Move’ component of the Chécate, Mídete, Muévete campaign was the most understood(30). In addition, the Mexican National Commission of Physical Culture’s Actívate, Vive Mejor campaign promoted physical activity.
While the majority of responses could not be linked to specific campaigns, the keywords mentioned by respondents provide insight into public awareness of the specific campaign themes or concepts. Sugar and/or sugary drinks were among the top five keywords mentioned in four countries and among the top 10 in Mexico. This aligns with the media campaigns and policy measures in place at the time of the study. For example, in the UK, campaigns focusing on sugar – including Sugar Smart and Sugar Swaps, a Change4Life sub-campaign – were ongoing at the time of the study, and the Soft Drinks Industry Levy (‘sugar tax’) was implemented in April 2018(56–58). Correspondingly, sugar, sugary drinks or sugar taxes were collectively mentioned in close to 60 % of UK responses. In Australia, ongoing campaigns related to reducing consumption of sugar and sugary drinks included Rethink Sugary Drinks (including Don’t be Sucked In) and Kids are Sweet Enough(59–63). Rethink Sugary Drink was the fourth most commonly recalled campaign, and sugar, sugary drinks or sugar tax were collectively mentioned in over 40 % of responses. In addition, 4 % mentioned the ‘toxic fat’ that accumulates around internal organs – a central message of the LiveLighter® campaigns. Moreover, mainstream discourse regarding the health consequences of sugar may have influenced recall of messages related to sugar. For example, the popular 2014 documentary That Sugar Film spawned That Sugar Movement in Australia(64), and may have contributed to the salience of messages about sugar. Similar diet and health-related documentaries were released around the same time in Canada and the USA(65,66) . In Mexico, the 2016 campaign No dañes su corazón (‘Don’t harm your child’s heart’) focused on reducing children’s sugary drink consumption to prevent obesity, CVD and diabetes(67). In Canada and the USA, where there were no widespread campaigns about sugar at the time of the study, references to sugar may have stemmed from knowledge of the FBDG, which discourage eating foods high in sugar, salt or saturated fats(36,68) , or from a widespread trend towards reducing sugar(69), which is supported by WHO recommendations(70). FV were also commonly mentioned by respondents in every country, which is perhaps unsurprising given that FV intake is a key component of national FBDG in all countries(27,36,53,68,71) . Adequate FV intake was also the focus of several major campaigns, including Go for 2&5 and Try for 5 in Australia, 5 al Día in Mexico and 5 A Day in the UK.
Finally, campaign recall differed somewhat across socio-demographic groups. We did not observe differences in campaign recall by age (except in the UK), income adequacy or BMI classification (except for a difference between those who didv. did not provide their height and weight/provided implausible values). In contrast, those with higher education were more likely to report seeing healthy eating campaigns than those with lower education levels in all countries except Canada, as were males compared with females in Canada, Mexico and the USA. Previous studies examining healthy eating campaigns have shown mixed results with regard to socio-demographic differences: some reported no differences in campaign awareness by sex, BMI or SES(Reference Morley, Niven and Dixon22,Reference Morley, Niven and Dixon24) , whereas others have found higher awareness among higher socio-economic groups(Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29,Reference Erinosho, Moser and Oh41) , and differences in campaign awareness by ethnicity(Reference Erinosho, Moser and Oh41), sex and/or age(Reference Morley, Niven and Dixon23,Reference Kite, Gale and Grunseit25,Reference Salazar-Coronel, Martinez-Tapia and Mundo-Rosas29,Reference Erinosho, Moser and Oh41) . Similarly, a review examining differences in the impact of physical activity campaigns by SES found mixed results with regard to differences by SES(Reference Thomas, Phongsavan and McGill72). Qualitative research suggests that campaign effectiveness can be improved among individuals of lower SES by drawing their attention towards specific health issues (e.g., current weight or consumption levels)(Reference Bukman, Teuscher and Feskens73). Research should further examine the factors influencing recall of public health campaigns and/or how to ensure broad reach across diverse socio-economic groups, especially given the need to address nutrition-related health disparities.
Strengths and limitations
The current study benefited from a large sample size and findings from five countries with diverse populations and different levels of government-initiated healthy eating education campaigns. However, other than in Mexico, specific campaign recall was low, with many campaigns reported by < 1 % of respondents in a given country. Although this likely reflects true differences in campaign reach, it may also reflect measurement issues. Specifically, the use of an open-text question in a larger survey likely resulted in lower engagement with the question compared with other possible formats (such as measures of aided recall or ‘recognition’), which tend to produce higher estimates of exposure due to the lower level of cognitive effort required(Reference Niederdeppe48), or compared with in-person or telephone surveys, which are more likely to encourage responses to open-ended questions. In addition, many respondents did not mention campaigns by name; in such cases, campaigns were identified based on keywords and descriptions. While all efforts were made to link participant responses to specific campaigns, considering these limitations, the proportion mentioning each campaign should be considered an underestimate, and between-group differences in overall campaign recall should be the central focus of study findings. Several campaigns identified were also targeted at specific subgroups or settings, which may not have been adequately represented in the sample. Ensuring that campaign messages and/or delivery channels are tailored to target audiences based on culture or socio-demographic characteristics such as age, sex or ethnicity may be an important factor in campaign engagement(Reference Snyder5). The current study did not assess campaigns for this type of message content; however, this is a direction for future research. Moreover, previous research indicates that campaigns are more likely to be recalled by those who are interested in the topic and/or who consume a lot of media; further research should examine these factors as covariates(Reference Niederdeppe48). Given inconsistencies in the terminology used to describe mass media campaigns, the search strategy used to identify health eating campaigns may have failed to distinguish public health-related initiatives from broader ‘social advertising’ or ‘social marketing’ efforts that may have been funded by industry. Future research should distinguish between these initiatives when examining campaign awareness(Reference Carins and Rundle-Thiele2). Finally, respondents were recruited for an online panel using non-probability-based sampling; therefore, the findings do not provide nationally representative estimates. For example, although the data were weighted by age group, sex, region, ethnicity (except in Canada) and education (except in Mexico), the Mexico sample had notably higher levels of education than census estimates, while BMI was similar or somewhat lower than national estimates across the five countries. In addition, there were notably higher levels of missing data for BMI in the UK.
Implications for policy and practice
Although participants were asked to recall government healthy eating campaigns, a large proportion freely recalled other messages: campaigns related to other aspects of a healthy lifestyle, such as physical activity, policy measures/initiatives that may or may not have been associated with mass media campaigns (e.g., sugar taxes and/or new FBDG); and marketing campaigns led by NGO. This suggests that when parsing out information from a cluttered information environment, consumers may recall healthy lifestyle messages but not necessarily their source (i.e., government or health authorityv. industry). Industry-sponsored messages may well lead to recall of positive messages about eating(74,Reference Kashty75) . However, industry-sponsored ads are ultimately designed to create positive associations with a specific brand or product, which more often than not involve pre-packaged or processed foods, which tend to be of poorer nutritional quality(Reference Martínez Steele, Popkin and Swinburn76,Reference Forouzanfar, Alexander and Anderson77) . Moreover, some campaigns are implemented by Social Aspects/Public Relations Organisations, that is, industry-funded groups that promote policies favourable to the industry while at the same time promoting an image of social responsibility. Research indicates that campaigns implemented by these organisations rather than public health agencies tend to increase positive associations of unhealthy behaviours (such as alcohol consumption) and may detract from the salience of public health messages(Reference Brennan, Schoenaker and Durkin78). Governments or health authorities therefore should consider increasing the salience of their institutional attributions when developing mass media campaigns in order to distinguish them from industry-sponsored ads. Literature from nutrition labelling suggests that government attributions increase the believability of messages and the likelihood that they will influence consumer choice(Reference Acton, Vanderlee and Roberto79). Secondly, because consumers do not necessarily distinguish between the various aspects of a healthy lifestyle (i.e., nutrition and physical activity) when recalling campaign messages, researchers aiming to evaluate the efficacy of mass media campaigns should consider examining changes in awareness, knowledge, attitudes or behaviours that are broader than the specific campaign objectives. Finally, because higher campaign awareness was documented among those with higher levels of education, it is important that mass media campaigns include strategies to reach particular subsets of the population, including those of lower SES. This could be facilitated by conducting formative work in the form of focus groups and/or pilot testing of campaign materials among target groups to increase engagement(Reference Wakefield, Loken and Hornik3). From a broader perspective, given previous evidence that social marketing campaigns risk increasing existing socio-economic disparities in health outcomes, comprehensive approaches, including policy changes, may be required to broadly address dietary issues in the population(Reference Backholer, Beauchamp and Ball80).
Conclusions
The high levels of campaign recall observed among those who provided responses in Mexico, Australia and the UK demonstrate the potential for public health education campaigns to have wide reach at the population level. Further research is required to examine whether consumers distinguish messages disseminated by public health agenciesv. industry-sponsored organisations.
Acknowledgements
Financial support: This work was supported by a Canadian Institutes of Health Research (CIHR) Project Grant, with additional support from an International Health Grant, the Public Health Agency of Canada (PHAC) and a CIHR – PHAC Applied Public Health Chair (D.H.). Additional funding was provided by the National Institute for Health Research (NIHR) School for Public Health Research (SPHR) (grant number: PD-SPH-2015) (M.K.) and a Heart Foundation Future Leader Fellowship (102035) from the National Heart Foundation of Australia (G.S.).Conflict of interest: There are no conflicts of interest.Authorship: S.G. coded participant responses, conducted statistical analyses and drafted the manuscript. G.C.A. and A.C. performed second coding of participant responses and linked responses to campaigns. G.C.A., L.A., A.J., M.K., J.M., G.S., J.F.T. and L.V. implemented the country-specific search strategies. C.M.W. managed the larger study. D.H. conceived and supervised the larger study and acquired funding. All authors contributed to writing and reviewing the final draft of the manuscript.Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were reviewed by and received ethics clearance through a University of Waterloo Research Ethics Committee (ORE# 21460). Electronic consent was obtained from all subjects.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980021001415







