



The opioid epidemic in the United States (US) has surged in recent years, with 67,367 Americans dying from an opioid overdose in just 2018 (Center for Disease Control and Prevention 2019). Since 1999, it has claimed over 750,000 deaths and wreaked havoc in families and communities across the US (Center for Disease Control and Prevention 2019). As the opioid epidemic has worsened in the US in recent years, federal and state governments have sought policy solutions to combat the epidemic. Most notably, former President Trump declared the opioid epidemic a public health emergency, unlocking federal funds for states and local governments to reduce the supply and demand of illicit drugs and thus reduce inappropriate opioid use in the US (White House 2018).Footnote 1 More recently, efforts to fight the opioid epidemic have confronted a new set of challenges as the coronavirus pandemic has increased stressors for many Americans while negatively impacting access to substance use disorder (SUD) treatment, further increasing opioid mortality rates (American Medical Association 2020).
One common narrative surrounding the opioid epidemic has emphasised those experiencing SUD and blaming individuals for their circumstances and the epidemic’s growth. This is, of course, in line with past narratives surrounding SUDs, and Nancy Reagan’s famous argument that users could have just said no to drugs vividly comes to mind (Quenqua Reference Quenqua2016). Similarly, President Trump has argued that “If they [users] don’t start, they won’t have a problem” (White House 2017). This narrative has also been used by street-level bureaucrats within local communities like the tough law-and-order sheriff in Butler County, OH, who refused to let his deputies carry Narcan (Wootson Reference Wootson2017).
As the scope of the opioid epidemic has grown in recent years, other narratives explaining opioid use disorder (OUD) have gained prominence as well. For example, one emerging narrative has been to place blame at the feet of health professionals and, in particular, pharmaceutical companies such as Purdue Pharma, the maker of the narcotic OxyContin. The prescription drug has been prominently featured in media reports detailing how the company sought to expand the use of prescription opioids by incentivizing sales staff to push OxyContin to “pill mills” (Lopez Reference Lopez2017; Taddonio Reference Taddonio2019). More recently, this narrative has been amplified by dozens of state attorneys general seeking restitution from opioid manufacturers and their owners for the damage the crisis has done to their states (Lopez Reference Lopez2019).
Given these conflicting narratives alternatively blaming individuals who use substances themselves or the healthcare industry, it is not surprising that while most Americans see OUD as a severe health and social issue facing the US, there is less consensus on the policies that are needed to combat the epidemic (see Kaiser Family Foundation 2016). We posit that the disparity between the widespread acceptance of OUD as a problem and variation in support for strategies to fight the opioid epidemic is partially due to disagreements over the root causes of the opioid crisis among the public and policymakers. We thus argue that the attribution of blame for the epidemic has important, albeit understudied, policy consequences. Most importantly, by influencing support for and opposition to policies designed to address the opioid epidemic, it may make policymakers hesitant to push for certain types of policy solutions like supervised injection facilities (SIFS) even though they have been found to be effective (Beletsky et al. Reference Beletsky, Davis, Anderson and Burris2008). The dialogue about the causes of the opioid epidemic thus provides an intriguing context for the study of attribution and its influence on policy attitudes and, ultimately, policymaking and implementation.
To explore the role of blame attribution in the opioid epidemic, our study utilises attribution theory as a theoretical framework to help explain policy preferences about the opioid epidemic. We posit that the way individuals view the causes of the opioid epidemic will influence their preferences towards policies designed to combat it. Specifically, we anticipate that to whom individuals’ attribute the causes of the epidemic, that is, either to personal choices (factors controlled by the individual) or situational factors (factors outside the control of the individual), will exert a substantial effect on what type of policies they support to mitigate the epidemic. Simultaneously, other factors are also likely to influence attitudes towards policies to combat the opioid epidemic. We argue that attitudes may be influenced by a personal connection to someone coping with SUD or having personal experience with SUD. The first-hand knowledge these individuals gain about the struggles those suffering from SUD face daily could inform their preferences for policy. Furthermore, we hypothesise that ideology and racial resentment will exert a substantive effect on policy attitudes.
In the discussion below, we begin by briefly describing attribution theory and its potential role in explaining attitudes toward policies to combat the opioid epidemic. We then lay out expectations for determinants of policy preferences towards solutions for the opioid epidemic, focusing on attributions of blame, personal connections, political ideology and racial resentment. Our analysis suggests that attributions of blame influence policy preferences related to combatting the opioid epidemic. We show that individuals who attribute OUD to personal choices are consistently more likely to support policies designed to punish individuals and are less likely to favour policies designed to aid individuals overcoming SUD/OUD. We also find consistent effects for the impact of ideology and racial resentment on attitudes. However, while the findings for personal connection and experience align with our expectations for supportive policies, they are more nuanced for punitive ones. We conclude by discussing the implication of our findings for health policy and combatting the epidemic by noting directions for future research.
Factors influencing attitudes toward opioid policies
As described above, we rely on attribution theory as the theoretical framework that informs our expectations about public opinion related to the opioid epidemic. In his seminal work on attributions, Fritz Heider (Reference Heider1944, Reference Heider1958) examined how individuals assess the causes and consequences of human behaviour. These inferences arise from interactions with the environment throughout the lifetime of an individual. For example, an individual may encounter a homeless person and attribute the cause of their homelessness to the personal choices of that specific individual, or instead to situational factors like the economy, employment opportunities, systemic biases or family dynamics. Footnote 2 The inferences we make about SUD can be similar to the inferences an individual could make about homelessness. Numerous studies using attribution theory have confirmed and significantly extended Heider’s original theory to various policy fields, including obesity (Cozzarelli et al. Reference Cozzarelli, Tagler and Wilkinson2002; Haider-Markel and Joslyn Reference Haider-Markel and Joslyn2018), gay rights (Haider-Markel and Joslyn Reference Haider-Markel and Joslyn2008), gun violence (Joslyn and Haider-Markel Reference Joslyn and Haider-Markel2017), poverty (Zucker and Weiner Reference Zucker and Weiner1993) and smartphone addiction (Jeong et al. Reference Jeong, Yum and Hwang2018).
Attributions of blame and opioid addiction
We theorise that individuals make inferences toward the underlying causes of SUD/OUD, which affect how individuals attribute blame for an individual becoming addicted to opioids. Specifically, individuals’ explanations can be grouped into two categories. Internal attributions focus on the individual (i.e. personal choices), while external attributions focus more on the environment (i.e. situational factors outside the control of the individual). A critical third dimension of how blame is assigned is the notion of controllability. Weiner’s (Reference Weiner1995, Reference Weiner2006) controllability dimension proposed that individuals are less willing to support (and more willing to punish) when they perceive that the cause of a problem is due to an individual’s own decisions and less willing to punish when they perceive the cause of the problem is beyond the control of the individual. The emphasis on controllability is beneficial when trying to explain public attitudes towards stigmatised topics. Drug addiction falls into this category as it is one of the most stigmatised conditions in society (Corrigan et al. Reference Corrigan, Kuwabara and O’Shaughnessy2009; Barry et al. Reference Barry, McGinty, Pescosolido and Goldman2014).
Individuals with SUD are often perceived to be personally blamed for their addiction, with many supporting the narrative that individuals suffering from SUD lack the self-discipline to properly use drugs – particularly prescription opioids – without becoming a person with SUD (Kennedy-Hendricks et al. Reference Kennedy-Hendricks, Barry, Gollust, Ensminger, Chisolm and McGinty2017). Existing research has examined the influence of attributions on the way individuals view policies to combat the opioid epidemic (Barry et al. Reference Barry, Kennedy-Hendricks, Gollust, Niederdeppe, Bachhuber, Webster and McGinty2016; Kennedy-Hendricks et al. Reference Kennedy-Hendricks, Barry, Gollust, Ensminger, Chisolm and McGinty2017; Goodyear et al. Reference Goodyear, Haass-Koffler and Chavanne2018; Haeder et al. Reference Haeder, Sylvester and Callaghan2021). However, the literature has yet to fully incorporate psychological dispositions, social variables and political variables into studies of attribution related to the epidemic and consider their impact on punitive and supportive policies. We posit that accounting for these specific factors, the way individuals view the causes of the opioid epidemic, as either internally or externally driven, will shape how they view policies to battle the opioid epidemic. That is, those individuals who feel addiction to opioids is a personal choice will be less likely to support policies designed to support those suffering from OUD, and they will prefer policies that are designed to punish (Hypothesis #1).
Personal connection
While the notions of attribution and controllability are important to consider when evaluating public attitudes toward opioid policies, just as important may be a personal connection to an individual who suffers from OUD. The influence of personal connections on individual policy preferences is an important predictor in other areas of health policy, most notably with policy preferences towards Medicaid. For example, Grogan and Park (Reference Grogan and Park2017, Reference Grogan and Park2018) found that individuals with any connection to the Medicaid program were more likely to view the program as an important federal policy than those who had no connection to the program.
Some research suggests that being familiar with SUD/OUD (i.e. having contact with someone dealing with OUD/SUD) can play an important role in determining attitudes (see Addison and Thorpe Reference Addison and Thorpe2004; Corrigan et al. Reference Corrigan, Kuwabara and O’Shaughnessy2009; Sattler et al. Reference Sattler, Escande, Racine and Göritz2017). However, research on whether having a personal connection to someone with OUD/SUD influences attitudes and preferences has produced mixed results. For example, Barry et al. (Reference Barry, Kennedy-Hendricks, Gollust, Niederdeppe, Bachhuber, Webster and McGinty2016) found that those with a personal experience with the opioid crisis, through either themselves, a family member or a close friend, were more likely to gravitate towards individual-orientated causes of OUD, which includes self-discipline. Other research, however, has found no significant difference between the attitudes of those with a personal connection to OUD and those without a personal connection to OUD (Kennedy-Hendricks et al. Reference Kennedy-Hendricks, Barry, Gollust, Ensminger, Chisolm and McGinty2017; Haeder et al. Reference Haeder, Sylvester and Callaghan2021). Because of the mixed findings in the extant literature, it is important to investigate how personal connections influence individual policy preferences about potential solutions to the opioid epidemic. We expect that individuals who connect to an individual suffering from OUD will be more likely to support policies designed to help overcome the disorder and will be less likely to support policies meant to punish individuals suffering from OUD (Hypothesis #2a). We expect that the same effect to be present for individuals who personally suffer from OUD (Hypothesis #2b).
Political ideology
Highlighting the importance of political measures on individual attitudes towards policy, a growing body of research shows that an individual’s perception of blame can influence policy preferences. For example, evidence suggests that liberals are more likely to perceive the structural causes of poverty, which are beyond an individual’s control, as important (Furnham Reference Furnham1982; Pandey et al. Reference Pandey, Sinha, Prakash and Tripathi1982; S. Williams Reference Williams1984; Bullock Reference Bullock1999; Skitka Reference Skitka1999; Cozzarelli et al. Reference Cozzarelli, Tagler and Wilkinson2002; Bullock et al. Reference Bullock, Williams and Limbert2003; Haeder et al. Reference Haeder, Sylvester and Callaghan2020). That is, liberals attribute the root causes of poverty to situational factors like discriminatory governmental policies, a lack of educational opportunity and outright racism. This leads liberals to be more likely to support policies meant to aid individuals out of poverty through social programs like Medicaid and unemployment benefits.
On the other hand, conservatives are more likely to point to individuals as being responsible for their circumstances. In the case of poverty, some conservatives believe that economic circumstances are at least partially attributable to individuals themselves and feel individuals can and should pull themselves up out of poverty through hard work; a failure to do so can be ascribed to laziness and poor personal choices like SUD (Pandey et al. Reference Pandey, Sinha, Prakash and Tripathi1982; Griffin and Oheneba-Sakyi Reference Griffin and Oheneba-Sakyi1993; Bullock Reference Bullock1999; Bullock et al. Reference Bullock, Williams and Limbert2003; Hopkins Reference Hopkins2009). Conservatives are hence much less likely to support extending unemployment benefits and have actively worked to make it harder to access many social safety net programs designed to assist individuals out of poverty. These causal attributions and subsequent policy preferences often extend beyond poverty and welfare policy (Haider-Markel and Joslyn Reference Haider-Markel and Joslyn2008). We expect conservatives to be more likely to support policies that criminalise the use of opioids. At the same time, liberals will be more likely to support policies designed to aid individuals overcoming OUD (Hypothesis #3).
Racial resentment
Finally, the last key factor to consider, especially when studying stigmatised issues like drug use and addiction, is racial resentment. Research has demonstrated that for many people of colour, and Black Americans in particular, their direct interactions with the government comes in the form of punishment (Weaver Reference Weaver2007). Elected officials have regularly used race as a mechanism to appeal to Whites, most notably with the presidential campaigns of Nixon and recently with former President Trump, tapping into the rising rates of racial resentment among Whites in recent years (Baker et al. Reference Baker, Grynbaum, Haberman, Karni and Buettner2019; Jardina Reference Jardina2019).
However, the extent to which racial attitudes shape White Americans’ attitudes toward public policy depends on the policy domain. One area where race has been a primary focus of rhetoric and discourse is criminal justice policy. For example, Enns and Ramirez (Reference Enns and Ramirez2018) found that support for privatising prisons and immigration detention facilities was influenced by racial resentment. Similarly, Morris and LeCount (Reference Morris and LeCount2020) found that racial resentment predicts support for increased spending on law enforcement. Scholars have long argued that criminal justice changes in the US have been used as a mechanism to reassert control over Black Americans (Bobo and Johnson Reference Bobo and Johnson2004; Weaver Reference Weaver2007).
Racial attitudes have also been found to influence policy preferences within social welfare policy. Research has shown that many Whites believe redistributive programs primarily benefit people of colour, although most redistributive programs primarily benefit Whites (Tesler Reference Tesler2016; Callaghan and Olson Reference Callaghan and Olson2017; Wetts and Willer Reference Wetts and Willer2018). This includes assistance for low-income seniors, unemployment insurance and parental leave benefits (Harell et al. Reference Harell, Soroka and Iyengar2016). Some scholars have even found that racial resentment influences attitudes towards projects that could benefit their state (Krimmel and Rader Reference Krimmel and Rader2017). Finally, recent public health policy issues, particularly the Affordable Care Act, are significantly affected by racial resentment (Tesler Reference Tesler2012; Haeder Reference Haeder2020).
Much like criminal justice policy, the connection between punitive policies and racial resentment has been used to explain individual attitudes towards drug use. Racial bias has long been associated with drug policy, most notably, with how crack cocaine use was punished more severely than powdered cocaine use, disproportionately affecting Blacks (Bobo and Johnson Reference Bobo and Johnson2004). Other research has found, for example, that white respondents who hold prejudicial attitudes toward African Americans and Latinos are less likely to say that too little money is spent on drug rehabilitation (Nielsen Bonn, and Wilson (Reference Nielsen, Bonn and Wilson2010). Based on this body of literature demonstrating the impact of racial resentment on policy attitudes and drug use, we expect individual attitudes toward policies designed to combat the opioid epidemic to be influenced by racial resentment, much like attitudes towards criminal justice, social welfare, health and other drug policy. Specifically, we expect that individuals who hold higher levels of racial resentment will be more likely to support policies meant to punish individuals suffering from OUD and less likely to support policies meant to assist individuals to overcome OUD (Hypothesis #4).
Data and methods
To test our hypotheses, we fielded a demographically representative online survey in December 2018 administered through Qualtrics (Sylvester et al. Reference Sylvester, Haeder and Callaghan2021). Qualtrics relies on large, online opt-in panels to recruit respondents to take surveys, an approach suitable for our analyses here. Footnote 3 We received 2,131 responses, including an oversample of 754 LGBTQ individuals (whose data was collected for a separate project also included in the survey). Footnote 4 We weighted the data to reflect national population benchmarks on gender, race, income and education, which we drew from the US. Census 2017 Current Population Survey. Footnote 5 Although the unweighted survey data are close to Census benchmarks, Table A1 in the supplemental material shows that the weights improve representativeness. Footnote 6
Dependent variables
Our primary interest in this study is to examine the correlates of attitudes towards policies designed to combat the opioid epidemic. For our dependent variables, we asked respondents their opinions about various policies associated with the opioid epidemic. We categorised these policies into two themes: (1) policies designed to aid individuals to overcome OUD and (2) policies designed to punish individuals suffering from OUD. Respondents were asked to state whether they favoured or opposed the various policies on a five-point scale ranging from “strongly favor” to “strongly oppose.” The full wording of the survey questions used in our analysis can be found in the supplemental materials.
Explanatory measures
In order to gauge whom Americans hold responsible for the current opioid epidemic, we asked respondents to think about why people become addicted to prescription opioids. In order to measure attributions of blame (Personal Choice), respondents were asked to choose between two possible answers: whether OUD is caused by the personal choices of the users themselves or due to some other factor. Footnote 7
Our analysis also included a measure to gauge how having a personal connection to the opioid epidemic influences policy preferences. To measure this, we asked respondents if they personally knew anyone who has ever been addicted to prescription opioids or heroin to create our measure of Personal Connection. Respondents were coded with a 1 if they personally knew someone who was addicted to opioids and 0 if they did not personally know anyone. Footnote 8 Simultaneously, we also accounted for whether the respondent has suffered from OUD.
Recall that we also are interested in how political ideology and racial resentment influence policy preferences toward opioids. Our measure of Ideology was created by using the standard approach of asking respondents to describe their political views on a seven-point scale ranging from “extremely liberal” to “extremely conservative.” Racial Resentment was measured using a four-question scale developed in previous work by Kinder and Sanders (Reference Kinder and Sanders1996) meant to tap into racial predispositions of individuals. Footnote 9
Finally, we also control for a variety of other demographics in our models. These include gender (a dichotomous measure with female coded as 1); race (using separate indicators for whether participants are Black or Hispanic); age and its squared term; educational attainment (we include indicator variables for high school degree, high school plus college and bachelor degree or higher with less than high school as the reference category); household income (on a seven-point scale included as indicators with the lowest income category as reference); indicators for rural and urban residence (with suburban as reference); insurance coverage type (indicators for employer-sponsored coverage and Medicare); political knowledge (on a seven-point scale) and religiosity (a measure to assess respondents level of church attendance on a five-point scale).
Results
The effect of causal attributions on policy preferences
Policies designed to support treatment efforts for opioid addiction
As described above, we asked respondents about their preferences for several policies that were either supportive of individuals suffering from OUD or more punitive policies. We selected policy options based on those policies currently discussed among policymakers as potential solutions to mitigate the opioid epidemic. Policy options designed to aid those addicted to opioids include implementing Good Samaritan protections (Table 1: Model 1), allowing for SIFS (Table 1: Model 2), Footnote 10 expanding access to drug testing kits (Table 1: Model 3), Footnote 11 creating diversion programs like drug courts (Table 1: Model 4), allowing Medicaid to pay for rehabilitation services (Table 1: Model 5), mandating private insurance to pay for SUD treatment (Table 1: Model 6) and legalising marijuana (Table 1: Model 7). Footnote 12
Table 1a. Estimates for supportive policies, all respondents
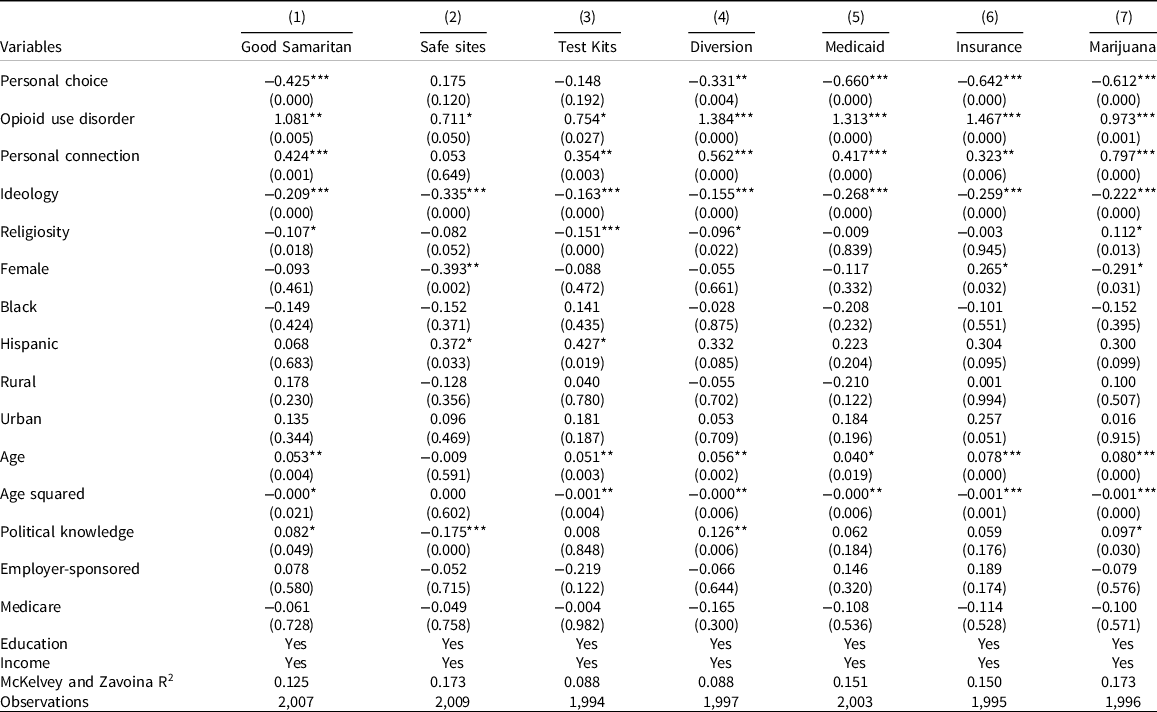
Robust p-values in parentheses *** p < 0.001, ** p < 0.01, * p < 0.05.
Table 1b. Estimates for supportive policies, White non-Hispanics
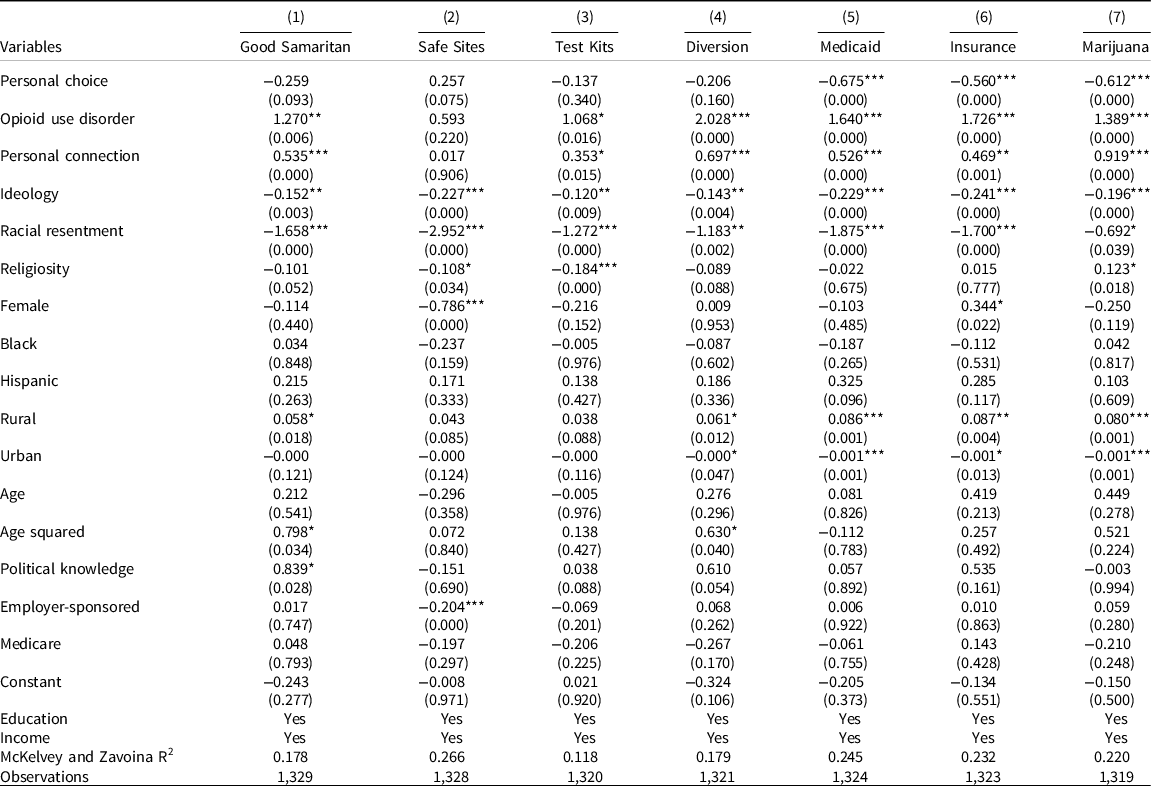
Robust p-values in parentheses *** p < 0.001, ** p < 0.01, * p < 0.05.
To assess support or opposition for the various policy options, we asked respondents whether they strongly favour, somewhat favour, somewhat oppose or strongly oppose adopting the various policies. We also offered respondents a neutral option. Due to the ordinal nature of data, we relied on standard ordered logit models, also known as proportional odds models, for our analyses presented here (R. Williams Reference Williams2016). Footnote 13 Interpretation of ordered logit models is not straightforward. To facilitate interpretation, we rely on average marginal effects (AMEs) as well as predicted probabilities (Cameron and Trivedi Reference Cameron and Trivedi2010; Long and Freese Reference Long and Freese2014). For both, we utilise graphical displays. Finally, we also estimated standard ordinary least squares (OLS) regression models as a robustness check of our findings. Footnote 14
Results for policies designed to aid those suffering from OUD are shown in Tables 1a and 1b, with the former displaying the results for all respondents and the latter displaying the results for non-Hispanic White respondents only. Footnote 15 Across the two tables, we found that coefficient signs and significance were in line with our expectations. Coefficients for Personal Choice (with two exceptions) and Ideology were negatively signed and significant, indicating that those who saw addiction as a personal choice and conservatives were more strongly opposed to policies assisting those struggling with OUD. The opposite holds for those who have suffered from OUD (Addiction) and for those with Personal Connections to someone with an OUD (with one exception).
AMEs offer additional help in interpreting the results, particularly for policy-relevant research, because they illustrate how substantively and statistically significant effects are (Cameron and Trivedi Reference Cameron and Trivedi2010). To provide context, we present the average predictions for all models from Table 1a and 1b in Figure 1. The figure displays the distribution of respondents along with the five-point scales of the dependent variables. Focusing on the results for all respondents first, we note that for six of the seven policies, probabilities of falling in the two favourable categories (somewhat and strong favour) exceed 0.5, and in four of the seven cases, 0.6. Notably, in six of seven cases, the oppositional categories do not exceed 0.2. The policy that stands out among the seven choices is the creation of SIFS. Here, support and opposition both have probabilities of roughly 0.4, with the remainder falling in the neutral category. When we compare the average predictions for all respondents to those for non-Hispanic Whites only, the results indicate general congruence, with some differences in support for SIFS and drug test kits (more opposition among non-Hispanic Whites). However, it is perhaps unsurprising that the public is more likely to oppose implementing SIFS. First, there are no SIFS located in the US to serve as a successful example for respondents to consider, and only a few exist in North America, in Canada. Second, the stigmatisation of individuals who use injection drugs influences support for SIFS (McGinty et al. Reference McGinty, Barry, Stone, Niederdeppe, Kennedy-Hendricks, Linden and Sherman2018). Some individuals might simply be uncomfortable providing a space for individuals to use drugs in violation of the law. In sum, Americans appear quite favourable of policies supporting individuals suffering from OUD with the exceptions of SIFS and, to a lesser degree, drug test kits.

Next, we present the AMEs for the five explanatory variables of interest we hypothesised about (Figure 2). We hold all variables constant for the three indicator variables (personal choice, personal connection and addiction) while varying the respective explanatory variable between the two choices. We only display results for those changes in AMEs that were statistically significant, at least at the 0.1 level.
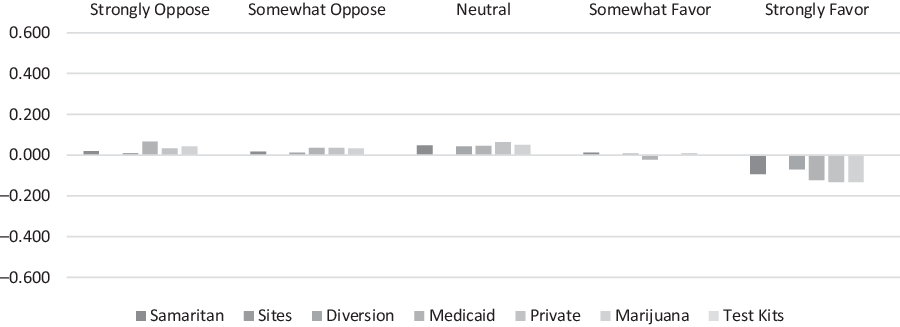
Figure 2a. Average marginal effects for personal choice.
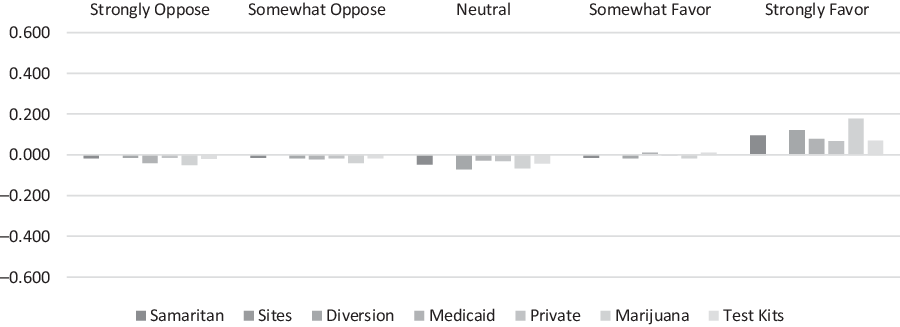
Figure 2b. Average marginal effects for personal connection.
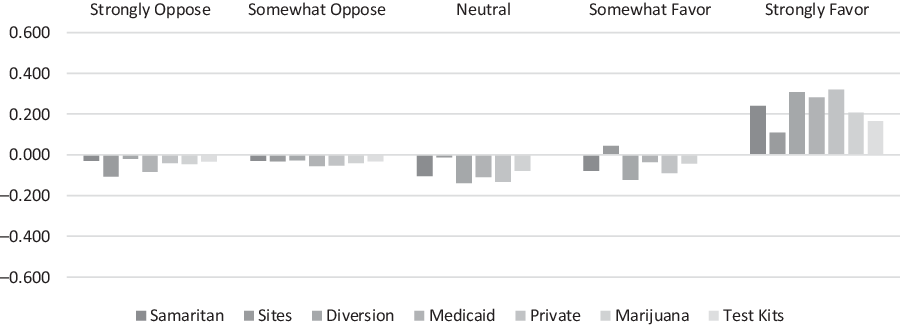
Figure 2c. Average marginal effects for opioid use disorder.
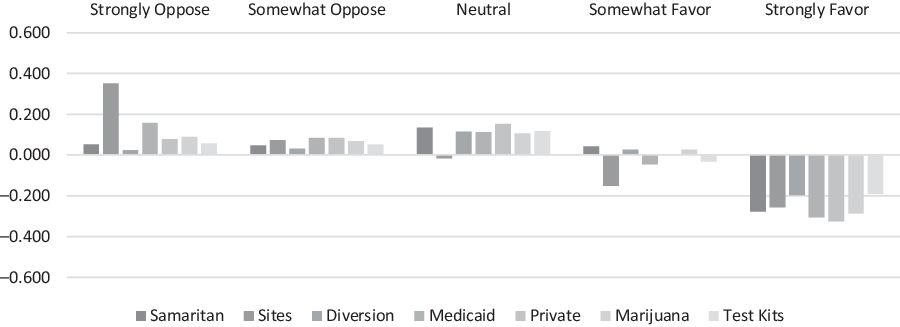
Figure 2d. Average marginal effects for ideology.
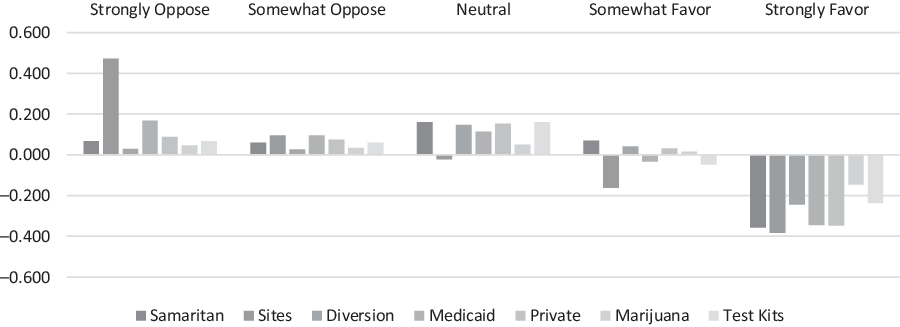
Figure 2e. Average marginal effects for racial resentment.
Comparing those who think that OUD is a personal choice to those who think it is due to factors beyond the individual’s control shows consistently significant effects. For five policies (all except SIFS and drug testing kits), we see increases in the strongly and somewhat oppose categories as well as the neutral category. In contrast, the strongly favourable category is markedly reduced for those who consider addiction a Personal Choice. Personal Connections, on the other hand, appear to have the opposite effect. That is, there appears to be a significant decrease in the oppositional and neutral categories paired with a significant increase in the strongly favourable bin for those with personal connections as compared to those without. While we see no effect on the SIFS policy option, we see some limited effects for the drug testing kit option. The most pronounced effect can be found comparing those suffering from OUD to those who do not. Here, increases in the strongly favourable category exceed 0.300 in two of the seven cases and 0.200 in five of the seven cases. Notably, we also see an effect for SIFS (0.108), albeit the smallest effect among the policy choices.
For the remaining two key explanatory variables, Ideology and Racial Resentment, we vary the variables from their minimum to their maximum value while holding all other variables constant. Again, we only display results for those changes in AMEs that were statistically significant, at least at the 0.1 level. Varying the Ideology of respondents from extremely liberal to extremely conservative has a ubiquitous effect on all policy options and all answer categories. Comparing the most liberal to the most conservative respondents illustrates a significant reduction in the most favourable category for all seven policy options with increases in both oppositional and the neutral category. For SIFS, substantial reductions are also visible in the somewhat favourable category, and the increase in the strongly opposed category approaches 0.400. Finally, when varying Racial Resentment from high to low, the effects are even more pronounced, approaching 0.500.
Policies designed to punish individuals for OUD
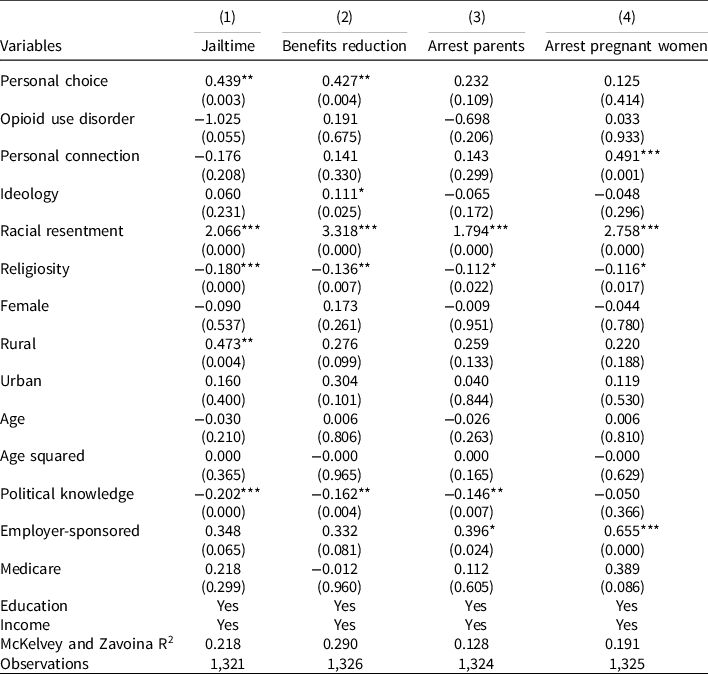
We also asked respondents their preferences about policies designed to punish those suffering from OUD. These include jail time for those who misuse opioids (Table 2: Model 1), denying social welfare benefits to those who test positive for drugs (Table 2: Model 2), charging parents addicted to drugs with child abuse (Table 2: Model 3) and charging pregnant mothers suffering from OUD with child abuse (Table 2: Model 4). Again, we estimate all models for all respondents (Table 2a) and non-Hispanic Whites (Table 2b), respectively.
Table 2a. Punitive policies, all respondents
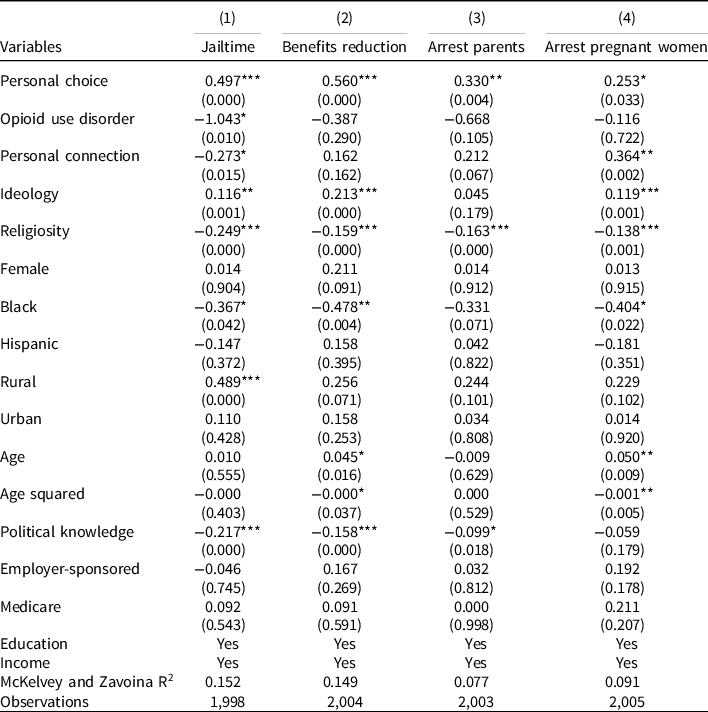
Robust p-values in parentheses *** p < 0.001, ** p < 0.01, * p < 0.05.
Table 2b. Punitive policies, White non-Hispanics only
Robust p-values in parentheses *** p < 0.001, ** p < 0.01, * p < 0.05.
Again, as coefficients from ordered logit models are limited in their interpretative value we hence rely once more on graphical displays to illustrate our findings. Figure 3 shows the average predictions for the estimates presented in Tables 2a and 2b. For three of the four policy options, the somewhat and strongly favourable categories exceed 0.500, with the remaining policy option requiring jail time for individuals who misuse opioids, almost approaching that mark. On the other end of the spectrum, the two oppositional categories generally combine for 0.150–0.200, with the jail category again serving as an exception with almost 0.300. Figures 4a-e corresponds to Figure 2a-e and display the AMEs for the punitive policy options.

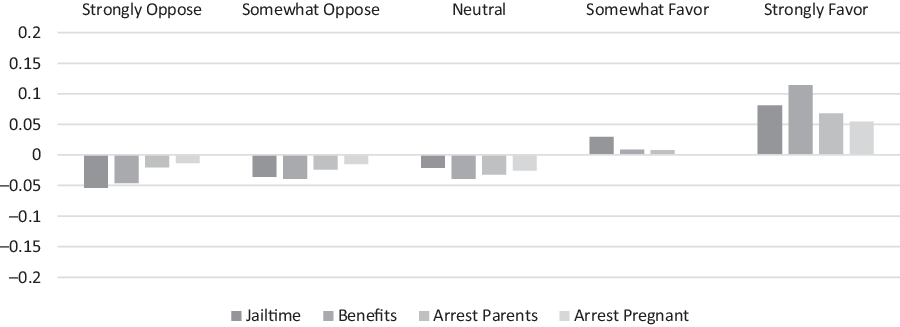
Figure 4a. Average marginal effects for personal choice.

Figure 4b. Average marginal effects for personal connection.
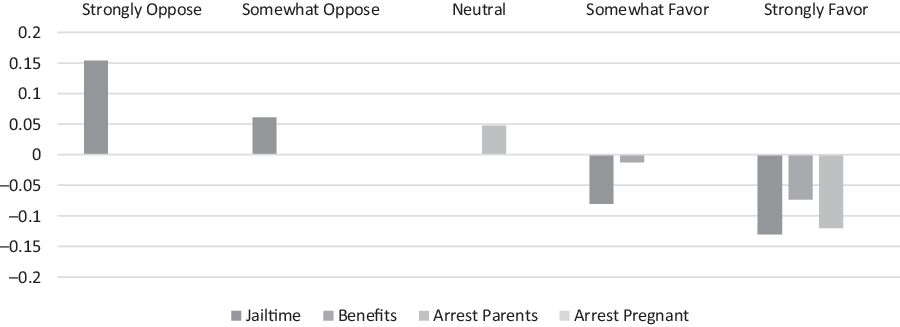
Figure 4c. Average marginal effects for opioid use disorder.
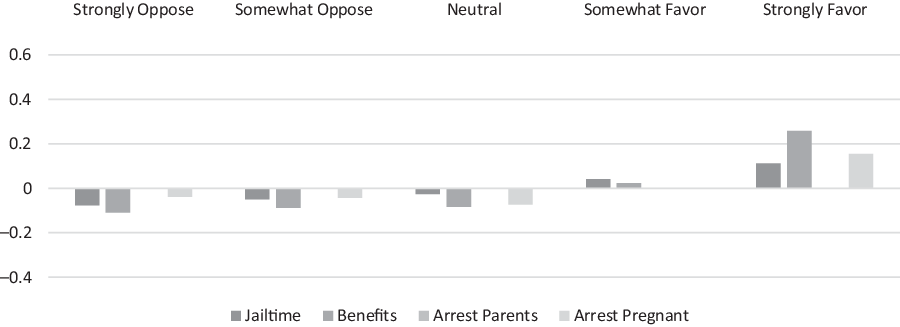
Figure 4d. Average marginal effects for ideology.
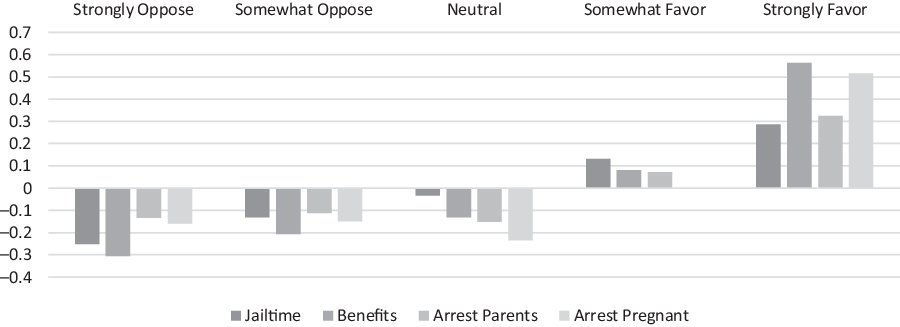
Figure 4e. Average marginal effects for racial resentment.
We find consistent effects for our Personal Choice variable. That is, those who think that OUD is a personal choice are much more likely to be supportive of all four punitive policies compared to those who think OUD is related to factors outside an individual’s control. We note that the size of the effect is smaller than for supportive policies. Our findings for personal connections are more complex. While those with a personal connection are generally less favourable of requiring jail time for those with OUD, we also note significant increases in support for pursuing criminal charges against parents and pregnant women. Generally, we find only limited effects for punitive policies for those suffering from OUD themselves: they are significantly less supportive of requiring jail sentences and other criminal persecutions of all types. With the exceptions of requiring jail time, the effects are only significant for the strongly favourable category, and they are generally substantively small.
We find more consistent and substantively large effects for Ideology and Racial Resentment. As conservatism increases, so does support for punitive policies. Notably, this effect is largest for reducing welfare benefits followed by punishment for pregnant women with OUD issues and requiring jail time. We do not find statistically significant effects for the prosecution of parents’ policy option. However, the most pronounced effects are apparent comparing those with low levels of racial resentment to those with high levels. The order of effect sizes mirrors that of ideology and ranges from almost 0.600 for eliminating welfare benefits and 0.500 for arresting pregnant women to about 0.300 for jail time and arresting of parents.
Overall support for supportive and punitive policies
Finally, we created several indices that combine all seven supportive policy options and all four punitive policy options, respectively. The first index provides a count of the number of policies (supportive or punitive) that each individual is somewhat or strongly favourable towards, while the second for each type of policy is an additive index that adds the ordinal value of the responses (from strongly oppose coded as 1 to strong favour coded as 5). All indices have Cronbach’s alpha values of around 0.800, indicating appropriate levels of reliability. We then utilised the index values as dependent variables and estimated both Poisson and standard OLS models utilising the same independent variables as in previous models. For both supportive and punitive indices, our findings are analogous for the respective indices, and we thus focus on the first set of indices described above. We focus on the OLS models (Table 3) to present our findings below (Poisson models omitted) for ease of interpretation.
Table 3. Results for analyses of indices of supportive and punitive policies
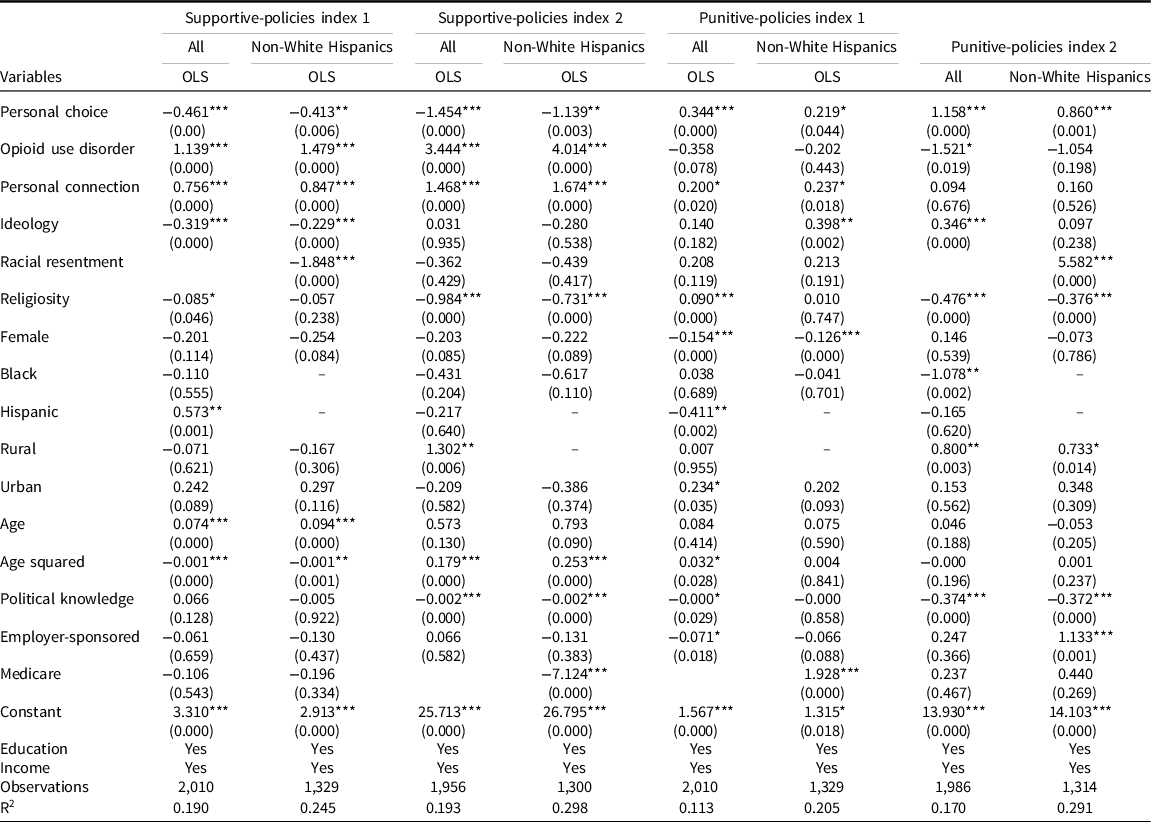
Robust p-values in parentheses *** p < 0.001, ** p < 0.01, * p < 0.05.
The findings for the supportive-policies indices are presented in Table 3 above for OLS models. Looking at Supportive Index 1 for all respondents, respondents who viewed OUD as a Personal Choice supported 0.5 fewer policies (out of 7). Similarly, each increase in the level of conservatism was associated with a decrease in support by 0.3 policies. Support for more policies was related to having a Personal Connection (0.8 more policies) and personal experience with OUD (1.1 more policies). Findings for non-Hispanic White respondents are analogous. That is, those who consider OUD a Personal Choice and conservatives support fewer policies (0.4 for the former and 0.2 for each increase in the level of the latter) while those with Personal Connections (0.8) and those with personal experiences with OUD (1.5) support more policies. However, the effect of Racial Resentment once more stands out: respondents with high levels of Racial Resentment support almost two fewer policies compared to those with low levels of resentment.
For Punitive-Policies Index 1, also presented in Table 3, we find that considering OUD a Personal Choice is associated with support for an additional 0.3 policies (out of four). In comparison, each increasing level of conservatism is associated with support for an additional 0.1 policies supported among all respondents. We also find effects for Personal Connection. Individuals who know someone suffering from OUD support 0.2 more punitive policies. We do not find any effects for personal experience with OUD, which is just above our cut-off p-value of 0.05. These findings are robust when only analysing non-Hispanic Whites for the Personal Connection, personal experience with OUD, and Personal Choice variables while we find no effect for Ideology. However, we note the again strong effect for Racial Resentment: those with high levels of resentment support 2 more punitive policies compared to those with low levels.
Discussion
Our research applies Weiner’s attribution theory of controllability to individuals’ attitudes about the causes of OUD. According to attribution theory, the causes of addiction are perceived to be either controllable (driven by personal choice) or not controllable (driven by situational factors). We posited that attributions and other factors like personal connection, personal experience with addiction, ideology and racial resentment would influence how individuals view policies designed to combat the opioid epidemic.
Consistent with our theoretical expectations, we find significant, and at times substantial, differences in support for policies to combat the opioid epidemic across our variables of interest. Whereas a personal connection and personal experience with OUD are related to higher support for supportive policy options, the opposite holds for conservatives, those with high racial resentment and those who blame individual’s personal choices for their OUD issues. Notably, there appears to be relatively broad support for these supportive policy options except for SIFS.
Conversely, we find that those with high levels of racial resentment, conservatives and those who consider addiction a personal choice are more supportive of punitive policies. The racial resentment findings are particularly noteworthy because they are so substantial. While overdose deaths among individuals of colour have steadily risen since 2000, the opioid epidemic still disproportionately impacts White Americans (Lippold et al. Reference Lippold, Jones, Olsen and Giroir2019; Drake et al. Reference Drake, Charles, Bourgeois, Daniel and Kwende2020). However, given the rising levels of racial resentment among Whites in recent years (Jardina Reference Jardina2019; Bartels Reference Bartels2020), and the research finding that racial resentment negatively influences government spending on drug programs (Nielsen et al. Reference Nielsen, Bonn and Wilson2010), these findings do fit with the existing literature.
In many respects, our findings reinforce how negative stereotypes influence perceptions and subsequent policy preferences toward drug policy. A long history of research shows how racialised stereotypes perpetuated by the media during the crack cocaine epidemic increased support for more punitive policies (Hurwitz and Peffley Reference Hurwitz and Peffley1997; Gilliam Jr. and Iyengar Reference Gilliam and Iyengar2000; Dixon Reference Dixon2006; Wozniak Reference Wozniak2020). While it is true that a focus on treatment-orientated policies regarding opioids has increased, racial inequities and racial stereotypes continue to influence drug policy (Kim et al. Reference Kim, Morgan and Nyhan2020). As reporting on the opioid epidemic shifts to focusing on how the opioid epidemic affects communities of colour, examining how racial attitudes influence public attitudes toward policies becomes increasingly important (Hale Reference Hale2020; Khatri et al. Reference Khatri, Pizzicato, Viner, Bobyock, Sun, Meisel and South2021). Our findings show that racial resentment and attitudes toward opioid policies have real policy implications and could exacerbate the treatment disparities already present within the health system (Hall et al. Reference Hall, Chapman, Lee, Merino, Thomas, Payne, Eng, Day and Coyne-Beasley2015).
The findings for personal connections and personal experience are more nuanced. Those with personal connections are more likely to oppose jail time in general for those suffering from OUD problems. At the same time, they are more supportive of punitive policies against parents and pregnant women. For those who have experienced SUD, support is more subdued for all punitive policies except for arresting pregnant women. The gender findings, in particular, are intriguing. While not being the focus of this article, the findings here show that perceptions of gender, in addition to racial politics, may influence the public’s support for punitive or supportive policies. Importantly, the effects are more pronounced for pregnant women than they are for parents in general. Future research should examine whether or not the different findings across genders can be replicated in other policy areas or are isolated to just OUD. Finally, our analyses of the punitive policies indices indicate consistent substantive effects only for ideology and personal choice.
The findings from our analysis of how Americans think about policies to combat the opioid crisis are remarkably policy-relevant. Some of these policies, most notably SIFS, while legal in the US due to a successful lawsuit in 2019 (Allyn and Winberg Reference Allyn and Winberg2020), continue to face pushback from residents in areas like Philadelphia, San Francisco and New York. With opioid deaths increasing due to the COVID-19 pandemic (Centers for Disease Control and Prevention 2020), the political debate over whether to combat the opioid epidemic through public health and harm reduction mechanisms or punitive policies will continue to be front and centre across the country. By understanding levels of support for policies designed to combat the opioid epidemic, our article can help state and federal policymakers better understand public sentiment while designing future policies and choosing which existing policies to implement. At the very least, policymakers might be encouraged to pass and implement some of the supportive policies we described here that appear to have overwhelming support without having to worry about electoral backlash. Policy advocates and entrepreneurs may also be buoyed to renew their efforts to argue for more comprehensive policy solutions to the opioid epidemic while educating the public of the potential benefits of SIFS (Wood et al. Reference Wood, Tyndall, Zhang, Montaner and Kerr2007; Marshall et al. Reference Marshall, Milloy, Wood, Montaner and Kerr2011).
The consistent importance of personal choice perceptions may reflect what Americans have learned about the epidemic from the media. Particularly, early on, news reports often framed opioid use not as a public health crisis but as a criminal justice issue (McGinty et al. Reference McGinty, Kennedy-Hendricks, Baller, Niederdeppe, Gollust and Barry2016); these effects may be lingering, and it may take time to reframe the issue in the minds of Americans. The persistent influence of racial resentment, while in line with the existing literature, is also concerning. Misperceptions about minorities and African-Americans are persistent in American politics and the media (Santoro and Santoro Reference Santoro and Santoro2018). These perceptions are resistant to change (Haeder et al. Reference Haeder, Sylvester and Callaghan2020) and, as a result, may discourage elected officials from supporting policy proposals that may lead to real or perceived electoral consequences for them. This, of course, bodes ill for the US ability to make headway in reigning in the epidemic.
Despite the importance of these findings, it is necessary to acknowledge several limitations of our study. First, our analysis does not account for differences across states in the severity of the opioid epidemic that could affect how individuals respond to policies designed to combat the epidemic. To the extent that respondents in particularly hard-hit states like West Virginia or Ohio respond differently than respondents in other states, our dataset cannot capture these distinctions, our analyses should thus be considered to focus on the national sentiment on these issues. Second, our analysis is limited in the number of policies explored in our study. While we do analyse public attitudes connected to a wide variety of proposed solutions to combat the opioid epidemic, the number of proposed solutions has been vast. For example, in 2018, the House of Representatives passed 58 bills designed to combat the opioid crisis during a two-week span alone (Killough and Mattingly Reference Killough and Mattingly2018). While we focused on policies frequently mentioned in the public debate, exploring public attitudes about all possible policy options is beyond the scope of our article but expanding our work here to look at topics like attitudes towards treatment-based solutions is an important direction for future research.
Third, it is crucial to recognise that for some survey questions about the epidemic, including personal experiences, our survey explicitly mentions heroin. The distinct cultural politics surrounding heroin versus prescription opioids could affect individual responses, but we are unable to test for the influence of our wording choices here. Future research should examine the public’s policy preferences toward heroin in comparison to prescription opioids. Fourth, our analysis utilised the Kinder and Sanders (Reference Kinder and Sanders1996) racial resentment scale commonly utilised in political science to measure White attitudes towards Blacks. However, the Kinder and Sanders measure has been recently critiqued for being too closely related to conservativism (DeSante and Smith Reference DeSante and Smith2020; Kam and Burge Reference Kam and Burge2018). Future research should examine the robustness of our findings using alternative measures of racial resentment. Finally, our data collection occurred before the COVID-19 pandemic. There is ample evidence that the opioid epidemic might be exacerbated in the wake of the pandemic by both mentally challenging situations and reduced access to treatment options. As such further exploration of our findings here in light of the pandemic is warranted.
Ultimately, even with these limitations, our research represents a significant step forward to understand public opinion about the opioid epidemic and policies to combat it. Our analysis emphasises the importance of considering attributions of blame when studying opioid misuse and highlights the important roles of attribution of blame, political ideology, personal connections, personal experience and racial resentment in influencing public attitudes towards combatting the epidemic.
Data Availability Statement
Replication materials are available at https://doi.org/10.7910/DVN/FOHJ4D
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S0143814X21000155




















 Open access
Open access