In recent years, the twin birth rate has been increasing in Iran (Yazdekhasti et al., Reference Yazdekhasti, Firouzfar, Hajheidari, Havaei, Tavakol and Karbasian2018). Similarly, this increasing trend is shown in the USA, Spain and Beijing (Derks et al., Reference Derks, Dolan and Boomsma2006; Sahu & Prasuna, Reference Sahu and Prasuna2016; Wood & Neale, Reference Wood and Neale2010). Identical or monozygotic (MZ) twins share 100% and fraternal or dizygotic (DZ) twins share, on average, 50% of their genome (Yu et al., Reference Yu, Cozen and Hwang2019). A comparison of disease concordance between MZ and DZ twin pairs can crudely estimate heritability. The additional concordance for disease among MZ twins compared to DZ twins suggests a role for genetic factors in disease etiology (McNamara et al., Reference McNamara, Alzubaidi and Jackson2019). For the first time in the 1920s, twins were used to study the heritability of characteristics (Mishra, Reference Mishra2019) and then the idea of twin registries developed. Various twin registries are available worldwide in countries such as Sweden, Denmark, Norway, Finland, Australia and the UK (Ferlay et al., Reference Ferlay, Colombet, Soerjomataram, Mathers, Parkin, Piñeros and Bray2019). Twin registries are a good database of information about both MZ twins and DZ twins, which is often conserved country-wide or by research institutes and considered as epidemiological tools aimed to investigate the contribution of genetics as opposed to the environment, to specific phenotypes (Bray et al., Reference Bray, Ferlay, Soerjomataram, Siegel, Torre and Jemal2018).
Nowadays, noncommunicable diseases (NCDs) such as cardiovascular disease (CVD), cancer and diabetes are considered as the main cause of death around the world (Siegel et al., Reference Siegel, Miller and Jemal2019). The behavioral risk factors and lifestyle indicators for these NCDs, such as smoking, unhealthy diet, and low physical activity, are also well known (Lacombe et al., Reference Lacombe, Armstrong, Wright and Foster2019).
Twins registries provide information about genetic factors and lifestyle habits and can be considered as a powerful instrument to study the complex mechanism of NCDs.
To the best of our knowledge, there is no other twin registry in Iran, and perhaps few in the Eastern Mediterranean region; therefore, the Isfahan Twin Registry (ITR) aims not only to register all twins and multiples in Isfahan, Iran, but also to provide a valid and standard biobank of their biomaterials for future studies.
Methods
Study Population Recruitments
In Isfahan, ITR was launched in late 2017 and started in August 2018. Isfahan is one of the larger provinces in the central part of Iran, with a population of more than 4 million. Details of the ITR was approved by the ethical committee of the Isfahan University of Medical Sciences. After the description of the study protocol for subjects, they signed a written consent and were entered in the study. Twins living in Isfahan province are invited from welfare agencies, public health homes, public and private maternity hospitals and the Persian Twins Association, which is a nongovernmental organization. The details of the registry were announced in broadcast programs as well as in social media, which led to more recruitment of twins and multiples. We organized the participants of the ITR into six categories: infants (1–24 months), early childhood group (2–6 years), late childhood group (7–12 years), adolescents (13–18 years) adults (19 years and older) and parents of children aged under 6 years and developed data collection protocols for each group. Health professionals who were trained for two days to be able to complete the registry questionnaires. A questionnaire method was used to assess twins’ zygosity (Reed et al., Reference Reed, Plassman, Tanner, Dick, Rinehart and Nichols2005).
Information on demographics and socioeconomic situation was collected using validated questionnaires. Lifestyle behaviors such as food consumption were assessed with food frequency questionnaires. Participants were considered to be a smoker if they were currently smoking and/or had a history of smoking more than 1 pack/day. Data related to physical activity were collected based on the International Physical Activity Questionnaires. The Hospital Anxiety and Depression Scale was used in order to measure psychological health. A validated women’s questionnaire was designed for women who are experiencing menstrual, menopausal or gynecological health concerns. Parents of children aged under 6 years completed questionnaires for their children and a brief one for themselves.
All participants were asked to bring their medical records, including hospitalization or records of any disease or pharmacological treatment, surgeries, or any para-clinical tests. Family history of disease was considered positive if subjects’ father or mother, sister and brother had been diagnosed with CVD, cancer or diabetes at or before the age of 55 years in men and 65 years in women. Weight, height and waist circumference was measured. Body mass index was calculated using the formula: weight(kg)/(height(m)2 (Gharipour et al., Reference Gharipour, Sarrafzadegan, Sadeghi, Andalib, Talaie, Shafie and Aghababaie2013). Waist and hip circumference (in centimeters) was measured in the standing position. Waist circumference was measured midway between the lowest rib and the iliac crest, and hip circumference was measured over the widest part of the gluteal region (Winham & Biernacka, Reference Winham and Biernacka2013). Blood pressure was measured using a random zero sphygmomanometer in supine position from the right arm after fasting for 12 h. The average of three measurements was used in the analyses. A 10-ml blood sample was collected from the antecubital vein of all participants aged more than 6 years. For newborns, which usually refer to babies from birth to about 18 months, only three spots of fresh blood were collected on the Guttery papers.
Laboratory measurements were done in the central laboratory of the Isfahan Cardiovascular Research Institute. Fasting blood sugar, total cholesterol, triglyceride and high-density lipoprotein cholesterol were measured by using a Hitachi 902 Analyzer and the standard enzymatic method; low-density lipoprotein (LDL) cholesterol level was calculated using the Friedewald formula. Aspartate aminotransferase, alanine aminotransferase and quantitative C-reactive protein were measured using a standard enzymatic method. Whole blood, serum, plasma, buffy coat, stool, guttery papers, nail, hair, and urine samples were collected. All bio-samples were stored for future studies either in a freezer at −70°C or at room temperature. For early and late childhood groups, a brief questionnaire and whole blood was given to parents.
Preliminary Results
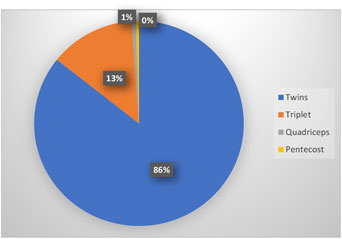
Until November 2019, a total of 378 twins, 62 triples, 3 quadruple and 2 more were registered. Table 1 displays the demographic, anthropometric and biochemical measurements of participants based on the age of participants. The number of registered participants based on age category till November 2019 were 82 infants ((1–24 month), 365 early childhoods (2–7 years), 294 late childhoods (7–12 years), 102 adolescences (13–18 years) and 155 adults (≥19). The number of registered participants based on age categories is presented in Table 1. Females consists 40.2%, 55.4%, 50.7%, 66.7% and 58.6%% in infants, early and late childhood, adolescents and adults, respectively. Table 2 shows the difference between anthropometric and biochemical measurements of participants by age groups and based on sex. Our preliminary findings show no significant difference between sexes on weight, height, waist and hip circumference in early childhood. The mean of fasting blood sugar was 83.45±8.57 vs 85.33±7.87 in females and males, respectively (P=0.046). We found that in late childhood, female twins have higher LDL, triglyceride, cholesterol than male twins. The mean level of triglyceride and total cholesterol in female and male, were 96.22±48.46 vs. 81.42±29.86 (P=0.002), 159.99±26.08 vs. 148.42±23.85 (P<0.001), respectively. In adolescents, the mean of fasting blood sugar in females and males 84.98±7.5 vs. 89.71±6.76 (P = 0.004), respectively. In adults, mean weight, height and waist circumference are lower in females than males. In addition, the mean value of aspartate aminotransferase and alanine aminotransferase are lower in females than in males 17.97±5.92, 27.17±13.96 (P<0.001), 14.27±9.72, 13.7±27.07(P<0.001).
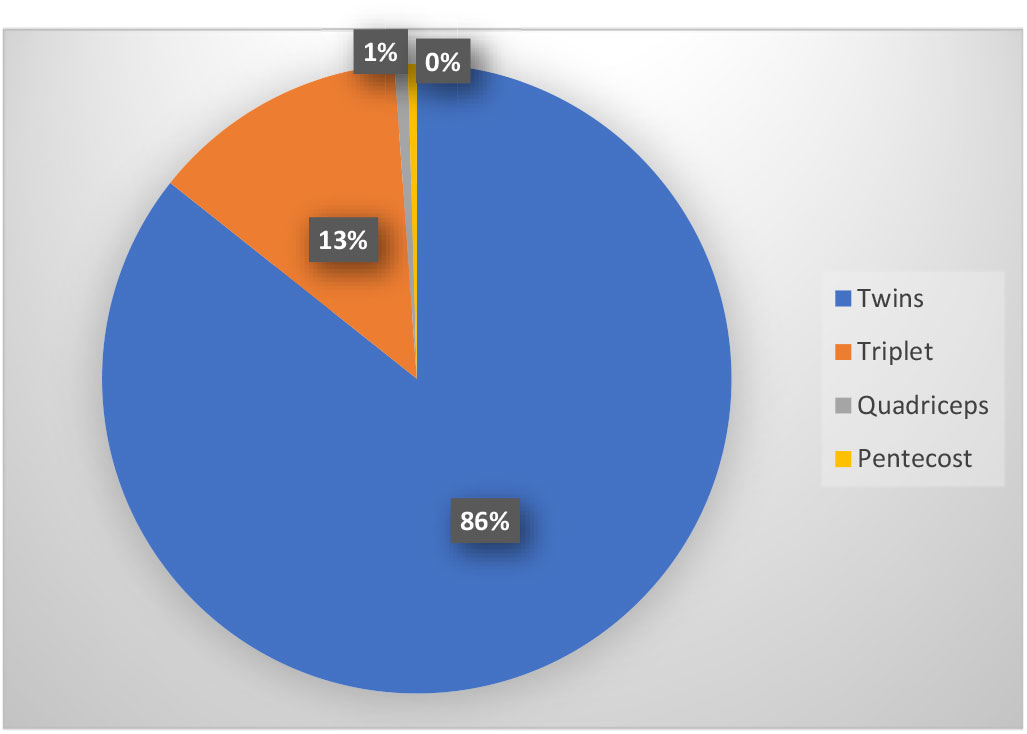
Fig. 1. Prevalence of multiple births at Isfahan Twin Registry.
Table 1. Mean (SD) of anthropometric and biochemical measurements of participants by age-group (N = 998 individuals)

Note: CRP = quantitative C-reactive protein; LDL = low-density lipoprotein; HDL, high-density lipoprotein.
Table 2. Sex differences in anthropometric and biochemical measurements of participants by age group (N = 998 individuals)
Note: Means is significantly different at p < .05 (*) and p < .01 (**) between two sexes. LDL = low-density lipoprotein; HDL = high-density lipoprotein; CRP = quantitative C-reactive protein.
Discussion
We developed and implemented a twin registry in Isfahan and named it Isfahan Twins Registry (ITR) a demonstration study to be later scaled up at national level. To our knowledge, the ITR is the first twin registry in Iran, and probably in the Eastern Mediterranean Region.
Until November 1st 2019, we recruited 998 persons in this registry. We had less access to adult twins in our community either because it is difficult to find them compared to children, or because of adult twins are unwilling to participate in studies. In late childhood females, twins have higher LDL, triglyceride, cholesterol than males. While in adolescence group, male twins have significantly higher height, waist circumference, fasting blood sugar, triglycerides as well as aspartate aminotransferase. Male adult twins have significantly higher waist circumference, fasting blood sugar, and LDL, aspartate and alanine aminotransferase. In this paper is the first report of the ITR, we tried to focus more on it’s methodology than on preliminary results. The ITR can provide a valuable source of valid data that could be used for future research, especially in epigenetic studies, as a tool for the assessment of the interaction between environment and genetics. By implementing this registry, the infrastructure necessary for conducting prospective cohort study in twins in order to investigate the incidence of of non-communicable diseases (NCD), their risk factors and their mechanisms will be possible. By collecting data on lifestyle, behaviors and environment studies could be helpful to dissect disease mechanisms in humans by using the information on susceptibility and resistance genes to focus on the biological pathways that are most relevant to many diseases, including NCDs, and the environmental factors that are most relevant to these pathways. By integrating epidemiological data with information on biological processes, we may be able to discover biological pathways and design new preventive and therapeutic strategies for diseases.
Limitations and strengths
The strength of this study is including all age groups of Iranian twins with completing data of lifestyle, biochemical and environmental factors as well as a completed bio-bank with gathering DNA, whole blood, plasma, serum, nail, and hair. We also completed lifestyle, behavioral and environmental questionnaires for parents of children under 6 years.
The first limitation is related to older twins and multiples. Although not all twins and multiples may be available, we will endeavor to register as many twins and multiples as possible in Isfahan. Another limitation is related to a lack of financial support to complete whole and whole-genome sequencing that offers the possibility of identifying new molecular targets and improved risk-prediction markers. The third is the lack of financial support for the epigenetic investigation. Epigenome-wide association studies are important because they may elucidate prenatal and postnatal environmental influences on the development of diseases. We hope to organize collaborations to study the changes in gene transcription and translation through environmental influences.
Acknowledgments
This registry is funded by Isfahan University of Medical Sciences and Isfahan Cardiovascular Research Institute. The authors are grateful to the Isfahan Welfare Organization and Persian Twins Society (a non-governmental organization). We thank the laboratory staff of the Cardiovascular Research Institute. The authors also acknowledge volunteers who took part in the study and appreciate their time and involvement in the registry.
Conflict of interest
None.