



Background
Mental health disorders and cardiovascular disease (CVD) affect more than 600 and 400 million people worldwide, respectively [1, Reference Roth, Johnson, Abajobir, Abd-Allah, Abera and Abyu2]. One of the most common mental health disorders is anxiety disorder. Over the past 20 years, annual incident cases of anxiety disorder have increased globally by almost 50%, from 31 to 45 million [Reference Xiong, Liu, Liu and Hall3]. Those with anxiety disorder are more likely to have CVD risk factors, such as hypertension and diabetes [Reference Lim, Solmi and Cortese4, Reference Mersha, Tollosa, Bagade and Eftekhari5]. A meta-analysis found a 40% excess risk of hypertension among those with anxiety disorder [Reference Lim, Solmi and Cortese4]. Further evidence has suggested an association between anxiety disorder and CVD. A meta-analysis reported 29 and 42% higher risk of incident CVD among women and men with anxiety disorder, respectively [Reference Smaardijk, Lodder, Kop, van Gennep, Maas and Mommersteeg6]. Single prospective cohort studies also showed associations between anxiety disorder and myocardial infarction (MI) (hazard ratio [HR] 2.51; 95% confidence interval [CI] 1.38–4.55) [Reference Janszky, Ahnve, Lundberg and Hemmingsson7], and stroke (HR 1.14; 95% CI 1.03–1.25) [Reference Lambiase, Kubzansky and Thurston8] specifically.
However, these studies did not assess the association of anxiety disorder with CVDs independently of and jointly with depression. Existing evidence has shown both that depression is associated with CVD [Reference Van der Kooy, van Hout, Marwijk, Marten, Stehouwer and Beekman9–Reference Wei, Hou, Zhang, Xu, Xie and Chandrasekar11] and that, based on Mendelian randomization studies, the association is likely to be causal [Reference Li, Cheung, Chung, Cheung, Wong and Fok12, Reference Tang, Yuan, Xiong, He and Larsson13]. Since anxiety disorder and depression often co-exist and may have shared or overlapping etiology [Reference Lamers, van Oppen, Comijs, Smit, Spinhoven and van Balkom14–Reference McTeague, Huemer, Carreon, Jiang, Eickhoff and Etkin17], the mechanism by which they are associated with CVD may be common to both conditions.
To that end, our study aimed to examine the individual and joint associations of anxiety disorder and co-existing depression with a range of incident CVD (MI, stroke/transient ischemic attack [TIA], or heart failure) using the UK Biobank population cohort.
Methods
Study design and participants
We conducted a prospective cohort study using data from UK Biobank. UK Biobank recruited over 500,000 participants between 2007 and 2010 from the general population, aged 40 to 69 years. Participants visited one of the 22 assessment centers across England, Scotland, and Wales to provide their information and biological samples. We excluded participants who had experienced CVD, MI, stroke/TIA, or heart failure before the baseline assessment ascertained through either self-report or linkage to medical records and who were first admitted for anxiety disorder or depression after the baseline assessment.
Measurements
The exposures of interest were anxiety disorder and depression diagnosed before the baseline assessment and were obtained through record linkage to hospital admission data: Health Episode Statistics (England and Wales) and Scottish Morbidity Records (Scotland). We defined anxiety disorder as F40–43 and depression as F32–33, using the International Classification of Diseases, 10th revision (ICD-10).
The outcomes of interest were incident (fatal or non-fatal) CVD, MI, stroke/TIA, and heart failure. The death certificate data were obtained from the National Health Service Information Centre (England and Wales) and the National Health Service Central Register Scotland (Scotland) and were available up to September 2021 in England and Wales, and October 2021 in Scotland. The hospital admission data were available up to September 2021 in England, July 2021 in Scotland, and February 2018 in Wales. Follow-up was censored at the date of relevant hospitalization or date of death, whichever occurred first. We defined CVD as an ICD-code of I20–25, I42.0, I42.6, I42.7, I42.9, I50, I60–64, and I110; MI as I21; stroke/TIA as I60–64 or G45, and heart failure as I42.0, I42.6, I42.7, I42.9, I50, or I110.
Covariates included sociodemographic (age, sex, ethnicity, and deprivation level) and lifestyle (alcohol intake, smoking status, sleep duration, TV viewing duration, physical activity, and body mass index [BMI]) factors. Age, sex, and ethnic group were self-reported by participants using a touchscreen questionnaire at baseline. Deprivation level was based on tertiles of the Townsend area deprivation index, which was derived from the postcode of residence using aggregated data on unemployment, car and home ownership, and household overcrowding [Reference Townsend, Phillimore and Beattie18]. Alcohol intake, smoking status, sleep, and TV viewing duration were self-reported using the touchscreen questionnaire at baseline. Physical activity was based on tertiles of metabolic equivalent minutes per week, which were derived from the self-completed, validated International Physical Activity Questionnaire [Reference Craig, Marshall, Sjöström, Bauman, Booth and Ainsworth19]. BMI was calculated as weight/height2; height was measured to the nearest centimeter, using a Seca 202 stadiometer, and body weight was measured to the nearest 0.1 kg, using a Tanita BC-418 body composition analyzer by trained staff.
Statistical analyses
Cox proportional hazard models were used to estimate the associations between anxiety disorder and depression and CVD outcomes, and the results expressed as HR and 95% CIs. Proportional hazard assumptions were checked by statistical tests based on Schoenfeld residuals. Separate models were run for each CVD outcome: overall CVD, MI, stroke/TIA, and heart failure. The main analyses comprised two stages. Firstly, the associations of each anxiety disorder and depression with CVD outcomes were analyzed by (1) univariable models, (2) multivariable models adjusted for sociodemographic confounders (age, sex, ethnic group, and deprivation level), and (3) multivariable models adjusted for both sociodemographic confounders and lifestyle factors (alcohol intake, smoking status, sleep duration, TV viewing duration, physical activity, and BMI). Because we could not establish the temporality between exposures and lifestyle factors, which could follow the exposure onset, we used models adjusted for sociodemographic confounders in the following analyses. Secondly, the individual and joint associations of anxiety disorder and depression with each of CVD, MI, stroke/TIA, and heart failure were determined, and multiplicative and additive interactions were tested. CVD outcomes were regressed on anxiety disorder, depression, their product term, and sociodemographic confounders. The HRs of anxiety disorders, depression, and their product term were used to estimate the individual and joint associations. The product term, and the relative excess risk due to interaction (RERI), were used to investigate the presence of multiplicative and additive interactions respectively. Missing values were < 5% and all analyses were complete case analyses.
Two different sensitivity analyses were performed to assess whether the additional use of self-reported exposures or primary care-diagnosed exposures and outcomes (available for 45% of the participants) affected the results. The case ascertainment in primary care settings was based on the UK Biobank Read codes mapping (https://biobank.ndph.ox.ac.uk/showcase/refer.cgi?id=592) (Supplementary Table S1). All analyses were conducted using R (version 3.5.3) with packages survival (version 3.2-7) and interactionR (version 0.1.5).
Ethical considerations
UK Biobank was approved by the North-West Multi-Centre Research Ethics Committee (Ref: 11/NW/0382). The investigation conforms to the principles outlined in the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study. This work was conducted under the UK Biobank application number 7155.
Results
Of the 502,413 UK Biobank participants who had not withdrawn from the study and could be linked to hospital admission/death data, 35,058 were excluded because they had CVD before the baseline assessment and 35,382 were excluded because they developed depression or anxiety disorder after the baseline assessment. Consequently, 431,973 participants were included in the analyses (Figure 1).

Figure 1. Flowchart of the participant selection process.
Overall, 428,296 (99%) had no anxiety disorder or depression, 911 (0.2%) had anxiety disorder only, 2,427 (0.6%) had depression only and 399 (0.1%) had both anxiety disorder and depression (Table 1). Participants with either anxiety disorder or depression or both were more likely to be female and deprived than participants without either condition. They were also more likely to be a current smoker, inactive, and obese and to have longer sleep and TV viewing hours, but less likely to drink more alcohol than recommended. Those with both anxiety disorder and depression were more likely to have unhealthy lifestyles and develop CVDs than those with only anxiety disorder or depression (Table 1 and Supplementary Table S2).
Table 1. Characteristics of subjects by anxiety disorder and depression

Abbreviations: BMI, body mass index; N, number; SD, standard deviation; TV, television.
When adjusted for sociodemographic factors, both anxiety disorder and depression were associated with increased risk of CVD, MI, stroke/TIA, and heart failure (Table 2). Additional adjustments for lifestyle factors attenuated most of the estimates but anxiety disorder remained associated with overall CVD and stroke/TIA and depression remained associated with both of these and heart failure (Table 2).
Table 2. Associations of anxiety disorder and depression with cardiovascular disease, myocardial infarction, stroke/TIA, and heart failure
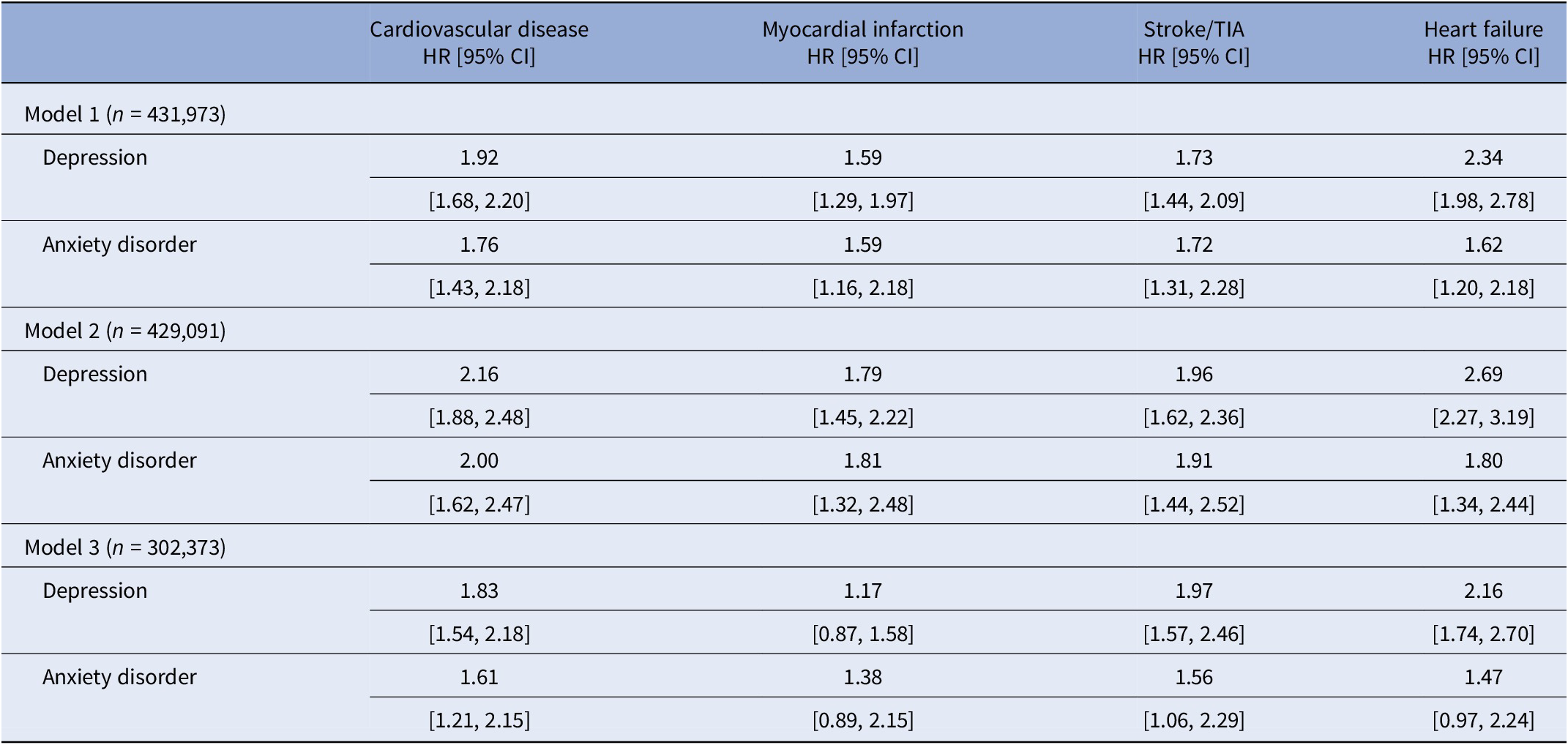
Abbreviations: CI, confidence interval; HR, hazard ratio; n, number; TIA, transient ischemic attack.
Note: Model 1: no adjustment. Model 2: adjusted for age, sex, ethnicity, and deprivation level. Model 3: adjusted for age, sex, ethnicity, deprivation level, alcohol intake, smoking status, sleep duration, television viewing, physical activity, and body mass index.
Anxiety disorder was associated with CVD, MI, stroke/TIA, and heart failure independently of and jointly with depression when adjusted for sociodemographic factors (Table 3 and Figure 2). The risk of CVD was higher for those who had been diagnosed with anxiety disorder only (HR 1.72; 95% CI 1.32–2.24), depression only (HR 2.07; 95% CI 1.79–2.40), and both conditions (HR 2.89; 95% CI 2.03–4.11) referent to those without these conditions, respectively (Table 3). There was very little evidence of interaction on the multiplicative scale with the RERI values close to null (Table 3). We found similar results for MI, stroke/TIA, and heart failure.
Table 3. Joint associations and interactions of depression and anxiety disorder with cardiovascular disease, myocardial infarction, stroke/TIA, and heart failure
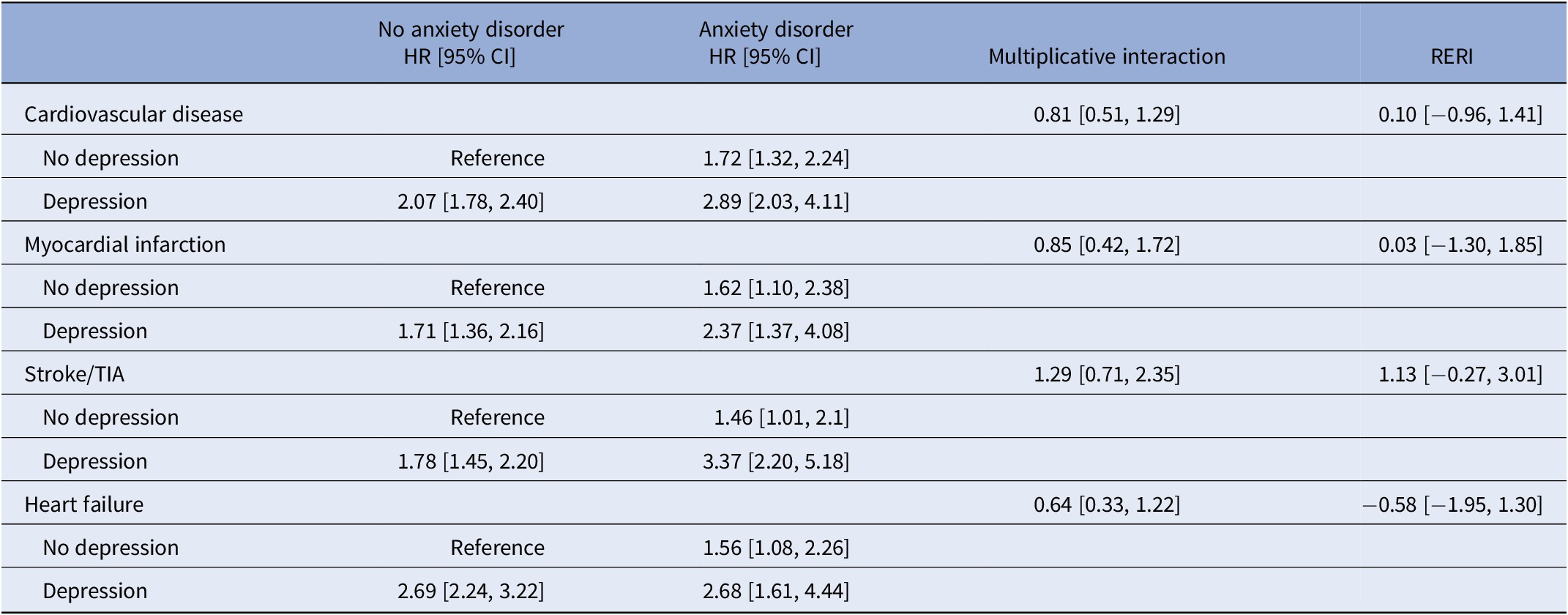
Abbreviations: CI, confidence interval; HR, hazard ratio; RERI, relative risk due to interaction; TIA, transient ischemic attack.
Note: All models were adjusted for anxiety disorder, depression, anxiety disorder × depression, age, sex, ethnicity, and deprivation level.
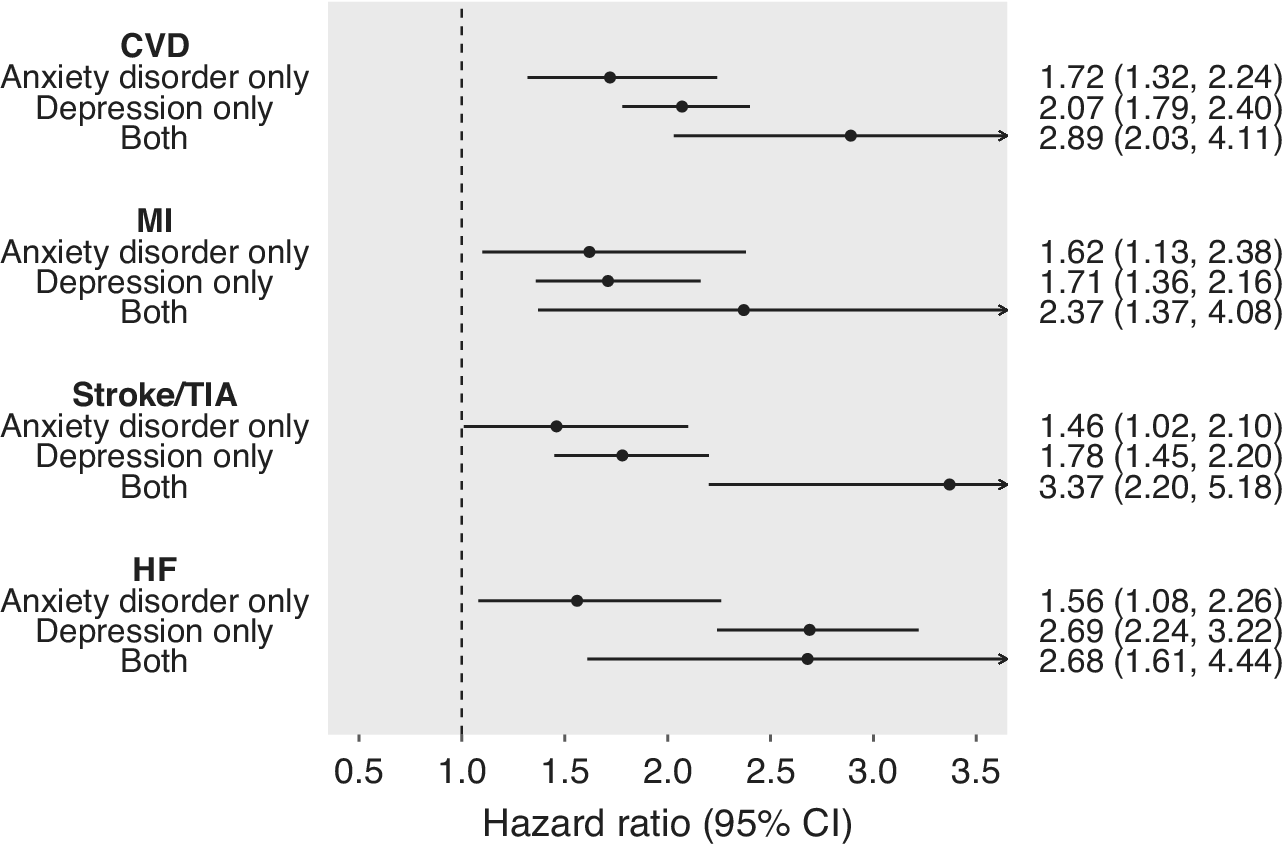
Figure 2. Individual and joint associations of anxiety disorder and depression with cardiovascular disease, myocardial infarction, stroke/TIA, and heart failure.
CI, confidence interval; CVD, cardiovascular diseases; HF, heart failure; MI, myocardial infarction; TIA, transient ischemic attack. All models were adjusted for age, sex, ethnicity, and deprivation level.
In the sensitivity analysis, the addition of self-reported anxiety disorder and depression attenuated overall associations but there were individual and joint associations of both conditions with overall CVD (Supplementary Table S3). Similarly, the addition of primary care data showed individual and joint associations with MI (Supplementary Table S4).
Discussion
Primary findings
Our study examined the individual and joint associations of anxiety disorder and depression with incident CVD and its subtypes (MI, stroke/TIA, and heart failure) using the UK Biobank population cohort. Anxiety disorder and depression were associated with incident CVD independently of each other and their co-existence was associated with a higher risk than either condition in isolation. However, there was no evidence of interaction implying that the sum of their individual associations with CVD was almost identical to their joint association based on RERI. Therefore, having anxiety contributes to the same relative excess risk of CVD regardless of whether depression is also present.
Comparison with the literature
Our findings would be consistent with different mechanisms by which anxiety disorder and depression potentially increase CVD risk. This would be biologically plausible based on previous studies suggesting different brain structures between these conditions [Reference Serra-Blasco, Radua, Soriano-Mas, Gómez-Benlloch, Porta-Casteràs and Carulla-Roig20–Reference Lai and Wu22]. For example, a recent meta-analysis found lower gray matter volume in the superior temporal gyrus of people with anxiety disorder, compared with those with depression. This structural difference could affect reactions to stimuli, which could lead to distinctive behaviors associated with anxiety disorder [Reference Serra-Blasco, Radua, Soriano-Mas, Gómez-Benlloch, Porta-Casteràs and Carulla-Roig20].
Our findings are consistent with previous evidence that has suggested similar individual and joint associations of anxiety disorder and depression with CVD risks [Reference Walters, Rait, Petersen, Williams and Nazareth23, Reference Seldenrijk, Vogelzangs, Batelaan, Wieman, van Schaik and Penninx24] but a few studies reported conflicting findings. A US prospective cohort study did not find an association between anxiety disorder and CVD, ascertained through self-reported symptoms, independent of depression (HR 1.06; 95% CI 0.80–1.39) [Reference Karlsen, Saksvik-Lehouillier, Stone, Schernhammer, Yaffe and Langvik25]. Their conflicting results may be explained by reporting bias or the inclusion of milder cases of anxiety disorder. Similarly, a German prospective cohort study did not show individual or joint associations for depression and sub-types of anxiety disorder (e.g., generalized anxiety disorder) [Reference Tully and Baune26]. This finding might be explained by sub-types of anxiety disorders operating differently from composite anxiety disorder and highlights the need for future research powered to investigate sub-group differences.
Limitations
There are some limitations to our study. First, ascertainment of anxiety disorder and depression using hospital admission may be incomplete and less likely to include people with less severe conditions since they are often treated in primary care settings [Reference Ansseau, Dierick, Buntinkx, Cnockaert, De Smedt and Van Den Haute27]. However, we investigated how the additional use of self-reports or primary care data affected our findings in sensitivity analyses and still found individual and joint associations with CVD and MI. Second, we only ascertained whether anxiety disorder and depression had ever occurred over a time period. We could not record varying anxiety severity or remitting–relapsing fluctuations, and therefore could not investigate the impact these may have on the relationship between anxiety and CVD [Reference Peter, Meyer, Mons, Schöttker, Keller and Schmucker28]. Third, our findings may not be generalizable to the whole UK population because UK Biobank participants are more likely to be white, affluent, and healthy than the national survey data [Reference Fry, Littlejohns, Sudlow, Doherty, Adamska and Sprosen29].
Implications
Our findings suggest that anxiety disorder and depression may increase the risk of CVD independently of each other. As we are facing an increasing number of people living with anxiety disorder, their higher risk of CVD should be noted. In recent years, some CVD risk prediction algorithms (e.g., QRISK3) have included depression [Reference Hippisley-Cox, Coupland and Brindle30]. Given the findings of our study, the added value of including anxiety disorder in risk prediction and stratification should be explored.
Conclusions
We examined the individual and joint associations of anxiety disorder and depression with incident CVD, MI, stroke/TIA, and heart failure among the middle- and old-aged UK population using the linkage of UK Biobank to hospital admission and mortality data. We found a higher risk of CVD among those with anxiety disorder only and depression only and the highest risk among those with both conditions, but no evidence of interaction on multiplicative or additive scales. This implies that the sum of their individual associations with CVD was almost identical to their joint association and therefore having anxiety contributes the same relative excess risk of CVD regardless of the presence of depression. One explanation is the existence of different mechanisms by which anxiety disorder and depression increase the CVD risk and this requires further research. Meanwhile, as has happened with depression, anxiety should be considered for inclusion in CVD risk prediction and stratification.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2023.2425.
Data availability statement
The data that support the findings of this study are available from the UK Biobank, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission from the UK Biobank.
Acknowledgments
We are grateful to the UK Biobank participants. This research has been conducted using the UK Biobank Resource under application number 7155. We are also grateful to the Medical Research Council and the University of Edinburgh/University of Glasgow. This work was supported by the Medical Research Council (MR/N013166/1-LGH/MS/MED2525).
Financial support
S.N. is supported by a Ph.D. studentship award from the Medical Research Council (MR/N013166/1-LGH/MS/MED2525).
Competing interest
The authors declare that there is no competing interest regarding the publication of this article.








 Open access
Open access
Comments
No Comments have been published for this article.