



According to the European Risk Observatory, psychosocial risks can be defined as those aspects from work design and management, as well as their social and organizational context, susceptible to affect physical, psychological, and social health and wellbeing of individuals (Brun & Milczarek, Reference Brun and Milczarek2007). Recent publications show that psychosocial risk factors are the main contributors to health issues such as depression, stress, and anxiety (Tomaschek et al., Reference Tomaschek, Lanfer, Melzer, Debitz and Buruck2018). The occupational stress, violence and workplace harassment or mobbing are the aspects with the highest impact on people’s mental health (European Agency for Safety and Health at Work, 2008). Other studies have demonstrated that psychosocial risk management is an efficient way to increase job satisfaction and to minimize conflict at work (Sureda et al., Reference Sureda, Mancho and Sesé2019). Positive personal and organizational aspects (e.g., autonomy, work climate, leadership, social support climate) are also related to productivity, creativity and quality of work performed with healthy organizational results (Garrosa Hernández & Carmona Cobo, Reference Garrosa Hernández and Carmona Cobo2011).
It is interesting to note that psychosocial risks have an uneven impact on people, as risks are interfered by sex and age differences, not only due to biological, but also sociocultural differences (Benavides et al., Reference Benavides, Declós, García and Ruíz2007). Moreover, when working in a specific occupational sector, such as the sanitary sector, professionals are affected in a transversal way due to both psychosocial risk factors of the sector as well as inequalities, generated by gender and age. For that reason, it has been a topic of interest in the investigation to identify the levels of mental health and their antecedents, in professions that include dealing with people, as in the case of the sanitary field (Wieclaw et al., Reference Wieclaw, Agerbo, Mortensen and Bonde2006).
Thus, the aim of this study is to analyze the differences in the perception of psychosocial risk in healthcare workers, according to age and sex, by identifying the impact these have on people’s work engagement and performance. The Job Demands-Resources Model (Demerouti et al., Reference Demerouti, Bakker, Nachreiner and Schaufeli2001; Schaufeli & Bakker, Reference Schaufeli and Bakker2004) framework is used as theoretical basis for this study. This model assumes a motivational process where work engagement can be predicted through the combination of both job demands and resources. The model predicts that high job resources (e.g., autonomy or social support climate), increase work engagement and counteract the negative effect of demands (e.g., quantitative overload). The model also predicts that high levels of work engagement lead to high levels of job performance. Therefore, a virtuous cycle is produced where high levels of job resources increase engagement and this, in turn, increases performance.
This is the first study to separately analyze the impact of psychosocial risk on different demographic groups (i.e., gender and age) among healthcare workers. Therefore, the prior knowledge provided by other similar studies in other sectors of activity is expanded. This analysis makes it possible to find out which labor demands and resources are most relevant, according to each sex and age group, with the aim of establishing guidelines for psychosocial intervention and tailored training plans. It must be taken into account that the health sector has been one of the activity sectors that were affected the most by the COVID–19 pandemic (Buselli et al., Reference Buselli, Baldanzi, Corsi, Chiumiento, Del Lupo, Carmassi, Dell’Osso and Cristaudo2020; Chen et al., Reference Chen, Liang, Li, Guo, Fei, Wang, He, Sheng, Cai, Li, Wang and Zhang2020; Iob et al., Reference Iob, Frank, Steptoe and Fancourt2020; Moreno Martínez et al., Reference Moreno Martínez, Fernández-Cano, Feijoo-Cid, Llorens Serrano and Navarro2022), so it can be very useful to know which resources and demands have the highest influence on each demographic group to develop intervention strategies that can improve wellbeing and performance.
Differences between Sexes
Job insecurity in women on the labor market has decreased towards more egalitarian positions between sexes. However, there are still sex differences within the working environment, with women occupying the most precarious job positions, which has a negative impact on their mental health (Messing & Mager Stellman, Reference Messing and Mager Stellman2006). Moreover, recent data show that women present a significant probability of having worse employment conditions and a higher exposure to psychosocial risks than men (Artazcoz et al., Reference Artazcoz, Escribà-Agüir and Cortès2006; Payá & Beneyto, Reference Payá and Beneyto2019; Cifre & Vera, Reference Cifre and Vera2019). Although there is still no evidence that women suffer higher work-related stress than men, different studies report that female workers experience a higher exposure to psychosocial risks than men (Benavides et al., Reference Benavides, Declós, García and Ruíz2007).
To understand why gender could be a cause of differences in psychosocial health, social inequalities must be understood. On one hand, the uneven distribution of productive work, on the other hand, the double working day, since women are forced to reconcile paid and unpaid work due to lack of conciliation and co-responsibility, which leads to an emotional division between job demands and family needs. There is evidence that many women suffer from role conflict as they must juggle work and family life with all that entails. Childcare is still a task mainly performed by women, since they devote more time to child, elder and dependent care (Ruiz-Frutos et al., Reference Ruiz-Frutos, García, Delclós and Benavides2007).
In this sense, both job and family demands may suppose a difference between men and women, and therefore have an impact on their psychological wellbeing scale (Ansoleaga et al., Reference Ansoleaga, Díaz and Mauro2016). However, many of the studies that have analyzed the impact of psychosocial risks between men and women are based on horizontal segregation (women usually occupy nursing positions, compared to more men in medical positions) (Ibáñez Pascual, Reference Ibáñez Pascual2008), so that they identify the main cause of the differences in the fact that women are more likely to assume precarious job positions, rather than in other gender-related inequalities. However, there is a total vertical gender segregation in the sanitary sector (i.e., more women in lower-ranking occupations and an unequal distribution of women in the hierarchical scale), so it is expected to observe differences with respect to psychosocial risks, considering the effect of both types of segregation (Moscato et al., Reference Moscato, Apfelbacher, Brockow, Eberle, Genuneit, Mortz, Quecchia, Quirce, Siracusa, Tarlo, van Kampen, Walusiak-Skorupa and Raulf2020).
Differences between Age Groups
Age acts as a moderating variable in the relationship between work engagement and job satisfaction: As age increases, the work engagement-job satisfaction relationship weakens, “This means that highly engaged workers will not only be more satisfied, but also tend to increase their resources over time, becoming more resilient to stress and adverse working conditions.” (Guglielmi et al., Reference Guglielmi, Avanzi, Chiesa, Mariani, Bruni and Depolo2016). Therefore, the motivational engagement-satisfaction pattern plays a prominent role for younger people, which suggests that stressors (such as job demands) could have a significant impact on them. However, other results indicate that older people are more likely to have higher levels of performance than younger people, partially due to the aging process (e.g., maturity, transformation of personality, etc.) rather than to high levels of effort (Beier et al., Reference Beier, Kanfer, Kooij and Truxillo2022; Kanfer & Ackerman, Reference Kanfer and Ackerman2004). A recent analysis from multiple meta-analytic studies shows no significant relationship between age and core task performance, this may seem somewhat surprising given the significant relationship between abilities and job performance and the negative relationship between fluid abilities and age. Despite multiple studies on the relationship between job performance and age, there is still much to be learned about how fluid and crystallized abilities mediate the relationship between age and job. However, differences have been found between older and younger workers on most job attitude measures, including psychosocial well-being measures such as job satisfaction, role conflict, role ambiguity, and commitment, with older workers having more positive well-being outcomes than their younger counterparts Beier et al., Reference Beier, Kanfer, Kooij and Truxillo2022).
Other studies relate both physical and mental toughness to aging (Prieto Albino et al., Reference Prieto Albino, Robles Agüero, Salazar Martínez and Daniel Vega2002; Sapolsky, Reference Sapolsky2013). There are also studies that indicate a significant activation of the sympathetic nervous system, caused by stress in older people Prieto Albino et al., Reference Prieto Albino, Robles Agüero, Salazar Martínez and Daniel Vega2002; as well as a poorer adaptation to shift works (McMichael, Reference McMichael, Payne and Cooper1978). Job stress seems to decrease with age (Buendía, Reference Buendía1998), because the greater experience of older people seems to provide them with more capacity and resources to face job demands (Garnés Ros, Reference Garnés Ros2001).
Objectives
The objective of this study is twofold. Firstly, it aims to identify the differences in the perception of psychosocial risk (i.e., job demands, job resources, wellbeing, and organizational outcomes) in each demographic group (i.e., women/men and younger/older) in the healthcare sector. Secondly, it aims to identify how to replicate the motivational process proposed by the Job-Demands–Resources (JD-R) model in the healthcare sector, and thus identify those job demands and resources that have a higher impact on work engagement and performance for each demographic group (i.e., women/men and younger/older). Designing ad hoc intervention strategies for each demographic group will be allowed by these findings, so that sanitary organizations can intervene in the improvement of their employees’ psychosocial health.
Starting from this theoretical basis, five hypotheses are raised.
According to the literature analyzed, it seems that women have higher exposure to psychosocial risks and therefore higher levels of job demand. For this reason, it (Aparicio García et al., Reference Aparicio García, Sánchez López, Dresch and Díaz Morales2008; Catalina Romero et al., Reference Catalina Romero, Corrales Romeo, Cortés Arcas and Gelpi Méndez2008; Ruiz-Frutos et al., Reference Ruiz-Frutos, García, Delclós and Benavides2007), is expected that our results go in the same direction. We will also be able to analyze the differences in relation to job resources which, according to the JD-R model, could compensate for the high demands perceived. Thus, we propose:
H 1: There are differences in the perception of psychosocial risk according to sex, with women having higher job demands and more resources than men.
In relation to age, research obtained contradictory results. While some authors claim that younger people have higher levels of engagement and job satisfaction (Guglielmi et al., Reference Guglielmi, Avanzi, Chiesa, Mariani, Bruni and Depolo2016) others state that it is more common in older people, due to maturity (Atance Martínez, Reference Atance Martínez1997; Hadjiolova et al., Reference Hadjiolova, Mincheva and Deyanov1994; Prieto Albino et al., Reference Prieto Albino, Robles Agüero, Salazar Martínez and Daniel Vega2002) While some authors report that older people have greater physical and mental strength, and therefore greater job resources due to experience (Garnés Ros, Reference Garnés Ros2001; Olmedo Montes et al., Reference Olmedo Montes, Santed Germán, Jiménez Tornero and Gómez Castillo2001), others report just the opposite (Atance Martínez, Reference Atance Martínez1997; Prieto Albino et al., Reference Prieto Albino, Robles Agüero, Salazar Martínez and Daniel Vega2002; Sapolsky, Reference Sapolsky2013). Considering that more literature has been found in favor of greater resources in older people, the following hypothesis is proposed:
H 2: There are differences in the perception of psychosocial risk according to age, with older people perceiving more job resources and wellbeing and less job demands than younger persons.
As observed in the bibliography, older people have greater well-being, commitment, and satisfaction, as well as a lower burden due to conflict and role ambiguity, than their younger counterparts. Therefore, a greater resistance to psychosocial risks could be expected in this group (Beier et al., 2022).
H 3: Job resources will be positively related to work engagement, regardless of sex and age.
Following the rationale of the previous hypothesis, the JD-R model also predicts that an increase in job demands will have a negative impact on work engagement and therefore on performance. This study intends to prove that the model is fulfilled in this same sense, regardless of age and sex. In this case, it will also be possible to know which demands have the greatest impact on work engagement, which will allow us to establish specific psychosocial intervention plans for each demographic group. Thus, the following hypothesis is proposed:
H 4: Job demands will be negatively related to work engagement, regardless of sex and age.
Finally, the mediating role of work engagement in relation between job resources and demands with performance is verified with the last hypothesis. According to the proposed hypothesis, this mediating role will be independent of sex and age.
H 5: Work engagement mediates the relationship between demands and resources with performance, regardless of sex and age.
Method
Sample and Procedures
The sample was collected between 2017 and 2018 through the project Hospital Optimista (Peláez Zuberbühler et al., Reference Peláez Zuberbühler, Salanova Soria and Martínez2017). It includes a total of 4,451 employees from 75 Spanish hospitals. 74.5% were women with an average age of 43.5 (SD = 10.0), divided into job positions including Nurse (33.6%); Nursing Assistant (17.4%); Administrative Assistant (13.0%); Ward Staff (4.0%), Medical Practitioner (24.8%) and other occupations (6.9%).
The sample was divided into two age groups: The group with younger age ≤ 39 (37.5%) and the group with older age ≥ 40 (62.5%). This division has been selected since it falls in the middle of the working age interval, considering that there is a later incorporation into the labor market. Moreover, this division at the age of 39 coincides with the recommendations of other authors (Martín Ruiz, Reference Martín Ruiz2005).
Before collecting data, we contacted the hospital’s leading executives (i.e., Human Resources and Management) to explain the purpose and requirements of the study. In addition, it was explained to everyone that participation was voluntary, that the presentation of the data would be added, and that any identifying information would be eliminated. The surveys were completely confidential, since the questionnaire did not ask for any personal information that could identify the author. Each person received access to the questionnaire in their email, through which they could access the online form. Data were collected over a three-month period.
Materials and Methods
The variables were measured with previously validated scales and grouped in dimensions, using a questionnaire, specifically developed for healthcare workers (Salanova & Llorens, Reference Salanova and Llorens2010; Salanova et al., Reference Salanova, Llorens, Cifre and Martínez2012). In general, internal consistency (Cronbach α) for the scales reached the cut-off point of 0.70 (Nunnally & Bernstein, Reference Nunnally and Bernstein1994). All items have a 7 points Likert scale, from 0 (never, strongly disagree) to 6 (always, strongly agree).
Job Demands. 8 job demands were measured, all of them evaluated through 3 items: Quantitative overload (α = .92) (e.g., “The work we do requires us to work against the clock”), role ambiguity (α = .89), role conflict (α = .89) (e.g., “The work we do requires us to do tasks that are disorganized”), routine (α = .82) (e.g., “The work we do requires us to do routine tasks”), mental overload (α = .74), emotional overload (α = .55) (e.g., “The work we do requires us to deal with difficult or peculiar people”), mobbing (α = .86) (e.g., “We have experienced situations where the work of a colleague has been systematically evaluated negatively”) and emotional dissonance (α = .90) (e.g., “How often do you need to express emotions in your work that do not correspond with what you feel at that time”).
Job Resources. 8 job resources were measured, all of them evaluated by 3 items: Autonomy (α = .62) (e.g., “Within my work team, we do our tasks in the way that we think is most convenient”), feedback (α = .75) (e.g., “In my work team, colleagues exchange information about how we do the work”), social support climate (α = .85) (e.g., “Within my work team, the supervisor shows his / her concern for our personal issues”), coordination (α = .81) (e.g., “Within my work team, we effectively handle unexpected events”), empathy (α = .97) (e.g., “During interpersonal relationships that we have with other colleagues and supervisors, we try to know how they feel”), mental competence (α = .80) and emotional competence (α = .68) (e.g., “In general, I think we are capable of being aware and remembering many things at the same time”). Transformational leadership (α = .98) was measured through 15 items, according to its dimensions (3 items per dimension): Vision, communication, stimulation, support, and recognition (e.g., “My immediate supervisor understands perfectly what the team’s goals are”).
Wellbeing. 5 indicators were measured: Efficacy beliefs (α = .90, 3 items, e.g., “We can do the job well even if we run into many obstacles”), engagement (α = .91, 9 items) (e.g., “Within my work team, we enjoy doing the work”), resilience (α = .92, 9 items) (e.g., “In situations of uncertainty and crisis, we try to find the positive side to difficult situations”), vertical trust (α = .93) and horizontal trust (α = .89) (4 items each) (e.g., “Workers from our team can share their ideas, emotions and hopes with each other”).
Organizational outcomes. 3 organizational outcomes were measured, all composed of 3 items: Intra-role performance (α = .96) (e.g., “Within my work team, we achieve the work objectives”), extra-role performance (α = .95) (e.g., “We perform roles that are not formally required but which improve the organizational reputation”), and organizational commitment (α = .93) (e.g., “Within my work team, the problems of this organization are “our” problems”).
Data Analysis
To test Hypotheses 1 and 2, mean comparison analyses were performed by ANOVA, with the aim of identifying differences between age groups and sex groups in the analyzed variables of demands, job resources, wellbeing, and organizational results.
To address Hypothesis 3 to 5, structural equation modelling (SEM) was carried out to identify which demands and job resources have a more significative impact on engagement and performance, (i) between men and women and (ii) by age groups. To analyze the hypotheses raised, SEM has been carried out by using AMOS 21.0 (Arbuckle, Reference Arbuckle2012) with the multi-group method. The maximum likelihood estimation method was used for analyses, using absolute and relative indices from the goodness-of-fit index (Marsh et al., Reference Marsh, Balla, Hau, Marcoulides and Schumacker1996). Besides the goodness-of-fit statistic of χ² and the Root Mean Square Error of Approximation (SEM), the Normed Fit Index (NFI), the Incremental Fit Index (IFI), the Tucker-Lewis Index (TLI) and the Comparative fix index (CFI) are included. An SEM under .06 indicates a good fit. For most indices, values higher than .90 indicate a good fit, and even higher values such as .95 indicate an excellent fit (Hu & Bentler, Reference Hu and Bentler1999). Modification indices were used to improve the fit model, for which previously missing values (N = 4.12%) were substituted by the average value of each variable. These missing values correspond to the blank questions of the questionnaires.
Results
Descriptive Analysis
Descriptive results for different demographic groups are displayed in Table 1. The internal consistency (α by Cronbach) of the scales used exceeded the cut-off point of .70 (Nunnally & Bernstein, Reference Nunnally and Bernstein1994), except for the emotional overload scales (.55), autonomy (.62) and emotional competence (.68).
Table 1. Mean, Standard Deviation (SD) and ANOVA results for different sex and age groups

Note: variables with statistically significant differences: p < .05 and p < .0001 are shown in boldface type.
The results of Harman’s single factor test Confirmatory Factor Analysis showed a poor fit of the single-factor test model for job resources: χ2(1,260) = 1,540.890; SEM = .17; NFI < .001; IFI = .00; TLI = –.06; CFI < .001; and for job demands: χ2(276) = 71.298; SEM = .24; NFI < .001; IFI < .001; TLI = –.09; CFI < .001. To confirm these results, additional analyses were performed (Podsakoff et al., Reference Podsakoff, MacKenzie, Lee and Podsakoff2003). This approach means to add a first-order factor to the investigator’s theoretical model with all measurements as indicators. Results showed that the model fit improved, even though none of the trajectory coefficients, corresponding to the relationships between the indicators and the general factor method, were significative. This finding suggested that, even though the method bias may be present, it does not significantly affect the results or the conclusions (Conger et al., Reference Conger, Kanungo and Menon2000).
Demographic Group Comparison
In Table 1, results of ANOVA are also presented. From the comparison of sex groups, statistically significant differences were observed in the following dimensions. In job demands, it is observed that the female group has significantly higher values than the male group in quantitative overload F(1, 4,363) = 4.64, p < .05, routine F(1, 4,347) = 40.70, p < .001 and mental overload F(1, 4,342) = 19.80, p < .001. In job resources, the female group has significantly higher values in autonomy F(1, 4,305) = 19.92, p < .001, empathy F(1, 4,271) = 28.93, p < .001, mental competence F(1, 4,267) = 16.59, p < .001 and leadership- vision F(1, 4,242) = 4.65, p < .05. Regarding the results of psychosocial health, it is observed that the female group has significantly higher values in work engagement F(1, 4,191) = 9.78, p < .01 than the male group. Finally, regarding organizational outcomes, the organizational commitment F(1, 4,137) = 4.40, p < .05, is significantly lower in the female group.
From the comparison of age groups, statistically significant differences were observed in the following dimensions. The older age group (≥ 40 years) has significantly higher values for all job demands, except for mental overload, where the value is higher for the younger group F(1, 4,184) = 16.39, p < .001. Moreover, it is observed that the older group (> 40 years) has significantly lower values for practically all the job resource dimensions analyzed: Feedback F(1, 4314) = 102.50, p < .001; social support climate F(1, 4,310) = 78.91, p < .001; coordination F(1, 4,305) = 96.55, p < .001; empathy F(1, 4,286) = 111.06, p < .001; mental competence F(1, 4,281) = 53,46, p < .001; transformational leadership F(1, 4,256) = 119.31, p < .001. Regarding wellbeing, it is observed that the group of older people has significantly lower values in all wellbeing dimensions, with a p < .001 in all cases. Finally, it is observed that the older group has significantly lower values across all dimensions of organizational outcomes, with a p < .001 in all cases.
SEM Analysis
Multi-group SEM were raised between job demands, resources, work engagement and performance, following the motivational process proposed by the JD-R Model. First, multi-group analysis was performed across sex groups, simultaneously using samples with men and women. The model fits the data well, with all fit indexes satisfying their criteria: χ² = 5,539; df = 342; RMSEA = .059; NFI = .908; IFI = .913; TLI = .894; CFI = .913. For both sexes, job resources are positively related with work engagement which, in turn, is positively related with performance. Moreover, as expected, job demands are negatively related with work engagement. Coefficients are shown in Figures 1 and 2 for men and women, respectively. In all cases, the regression coefficients were significant p < .001.

Figure 1. CFA analyses JD-R Model Concerning organizational outcomes: engagement and performance in men group. (n=1137). Note: only the significant coefficients are displayed. X2 = 5539; df = 342; RMSEA = .059; NFI = .908; IFI = .913; TLI = .894; CFI = .913
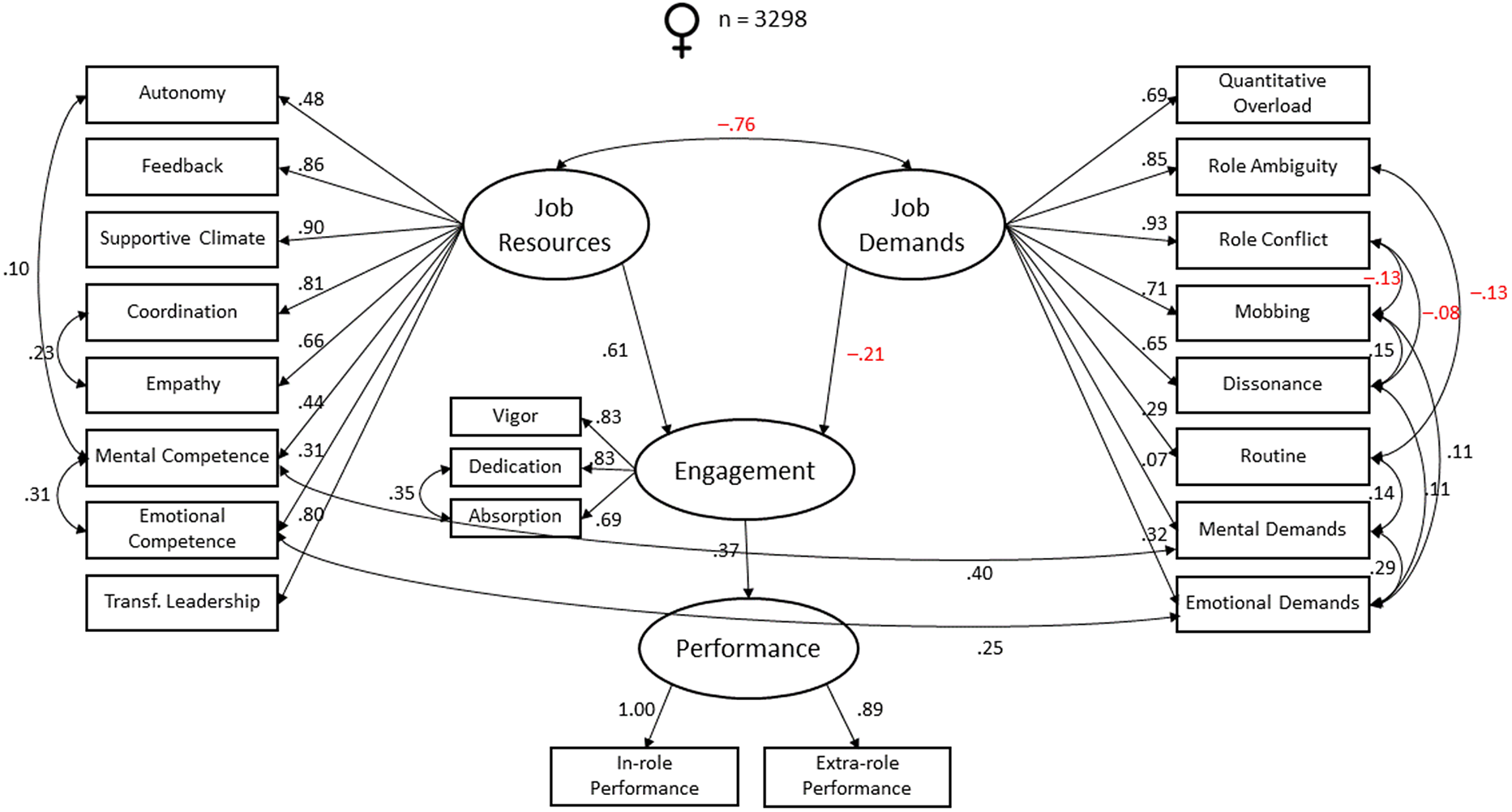
Figure 2. CFA analyses JD-R Model Concerning organizational outcomes: engagement and performance in women group. (n=3298). Note: only the significant coefficients are displayed. X2 = 5539; df = 342; RMSEA = .059; NFI = .908; IFI = .913; TLI = .894; CFI = .913
Second, multi-group analysis was performed across age groups, simultaneously using younger and older samples. The model fits the data well, with all fit indexes satisfying their criteria: χ² = 5,645; df = 342; RMSEA = .059; NFI = .906; IFI = .911; TLI = .891; CFI = .911. For both age groups, job resources are positively related with work engagement which, in turn, is positively related with performance. Moreover, as expected, job demands are negatively related with work engagement. Coefficients are shown in Figures 3 and 4 for younger and older people, respectively. In all cases, the regression coefficients were significant p < .001.

Figure 3. CFA analyses JD-R Model Concerning organizational outcomes: engagement and performance in young group. (n=1667). Note: only the significant coefficients are displayed. X2 = 5645; df = 342; RMSEA = .059; NFI = .906; IFI = .911; TLI = .891; CFI = .911
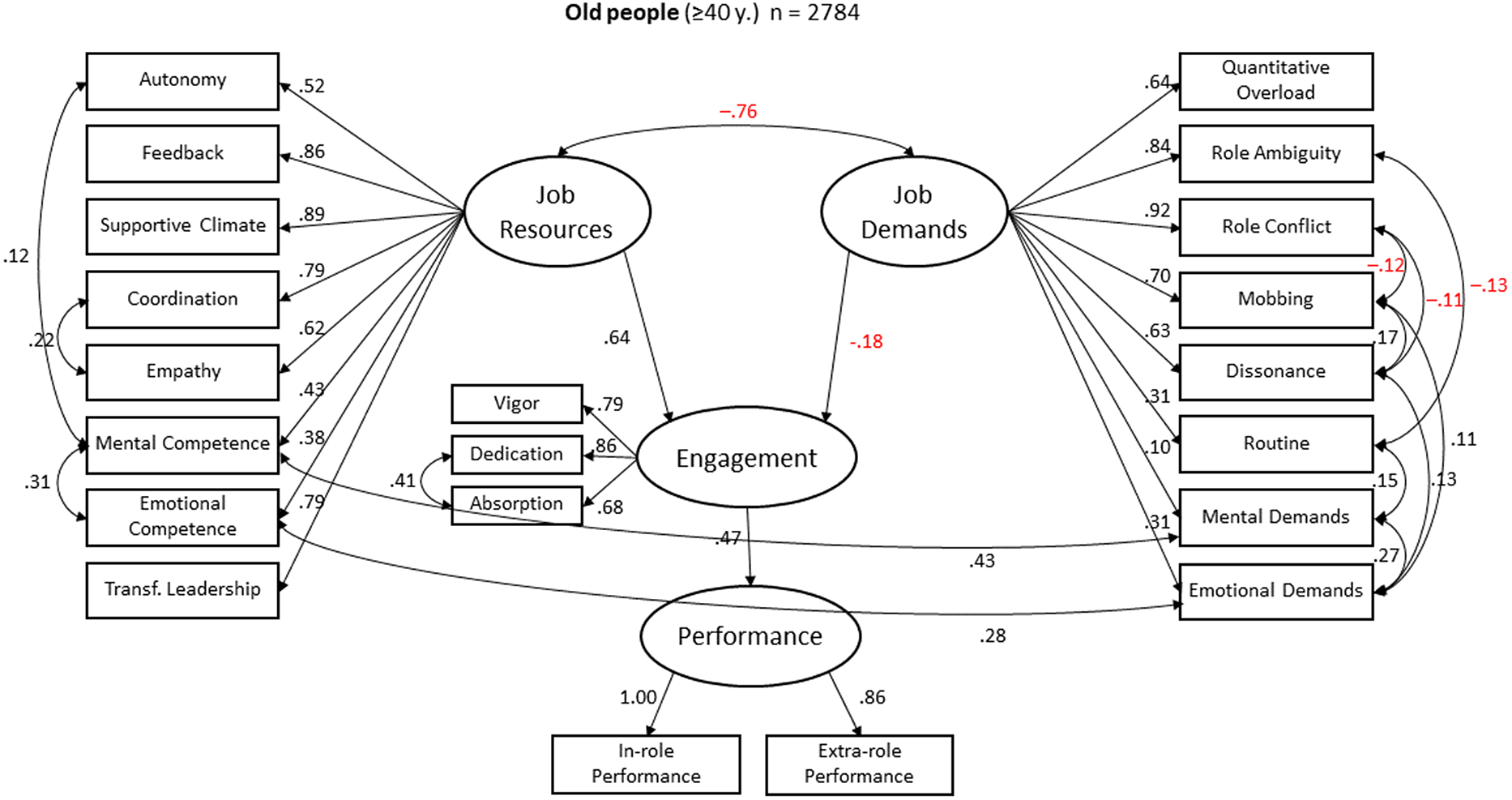
Figure 4. CFA analyses JD-R Model Concerning organizational outcomes: engagement and performance in old group. (n=2784). Note: only the significant coefficients are displayed. X2 = 5645; df = 342; RMSEA = .059; NFI = .906; IFI = .911; TLI = .891; CFI = .911
DISCUSSION
The purpose of this study was twofold: (a) To analyze the difference in perception of psychosocial risk in healthcare workers from the perspective of sex and age; and (b) to investigate the effect of job demands and resources on work engagement and performance in different demographic groups. To fulfill this research objective, we tested several hypotheses.
Hypothesis H 1 can be considered partially accepted, as significative differences in resources and demands are observed between men and women. It is verified that women perceived more job demands than men (i.e., quantitative overload, routine and mental overload), which is in line with previous studies (Julià et al., Reference Julià, Catalina-Romero, Calvo-Bonacho and Benavides2016), but at the same time, women have more job resources (i.e., autonomy, empathy and mental competence) to combat those demands. When analyzing the dimension of wellbeing, it is observed that women show significantly higher values in work engagement. Regarding organizational results, it is observed that the female group is the one which presents significantly lower values in organizational commitment. It should be noted that significant differences in mobbing are not observed between sexes, as some authors suggest (López-Cabarcos et al., Reference López-Cabarcos, Vázquez-Rodríguez and Gieure2017), although it could be due to a non-existence of significant differences in stressors such as role conflict and ambiguity. In fact, these stressors are presented as risk factors and play an important role in explaining mobbing (Bowling & Beehr, Reference Bowling and Beehr2006).
When we analyze the data by age groups, we can observe that, when dividing the sample between younger (< 40 years) and older (≥ 40 years) people, there are statistically significant differences that award the younger group a better position, with more job resources, wellbeing, and organizational outcomes than the older group. And, when analyzing job demands, those resulted significantly lower in the group of younger people. This could be related to the stimulating and motivating effect that the health profession can exert in the first years of practice, given its recognized vocational nature (Herrera Moya et al., Reference Herrera Moya, Alfonso Tejeda, Quintana Uguando, Pérez Ineránty, Navarro Aguirre and Sosa Fleites2018). Thus, hypothesis H 2 is partially accepted, since there are significant differences between age groups. However, younger people perceive more job resources and fewer demands, and not the other way around, as it was initially proposed.
When doing multi-group SEM analysis to test the effect of demands and resources on work engagement and performance, it can be observed that the prediction model of the Motivational Process of the Job-Demands–Resources Model is fulfilled, regardless of sex and age. Then, hypothesis H 3 can be considered as accepted, when verifying that job resources correlate positively with work engagement. In other words, greater job resources have a positive impact on work engagement.
Likewise, hypothesis H 4 can be considered accepted when verifying that job demands correlate negatively with work engagement, regardless of sex and age. That is, higher job demands will have a negative impact on work engagement.
Finally, when the whole model was tested, analysis showed us that the motivational process, proposed by the JD-R model, is fulfilled regardless of sex and age. That is, when employees have more job resources and less job demands, they show higher levels of work engagement which, in turn, is related with higher performance. This means that Hypothesis H5 can be accepted as well.
At a theoretical level, the JD-R model is confirmed in the healthcare sector, segregated for both sex and age. In the analyzed bibliography, discordant results were observed regarding the implication of job demands, resources and wellbeing between older and younger people, and with the results obtained, it can be observed that in the health sector, it is the group of younger people that has significantly higher levels of job resources, work engagement and performance.
The results obtained show us that the perceptions and needs of healthcare workers can be different, depending on their sex and age. This implies that not all groups should be treated in the same way and that psychosocial interventions should be personalized, which means that we can take advantage of these differences in the perception of demands and resources of the different demographic groups to develop specific psychosocial intervention actions, and by confirming the JD-R model, we know that these interventions will have the expected positive effect on work engagement and performance. It is therefore possible to design specific psychosocial intervention programs in the sanitary field, as other authors have successfully developed (Rickard et al., Reference Rickard, Lenthall, Dollard, Opie, Knight, Dunn, Wakerman, MacLeod, Seiler and Brewster-Webb2012).
For instance, for older people, the variables related to feedback, supportive climate and transformational leadership have been more relevant, therefore, interventions to increase their wellbeing and performance should be aimed at promoting these aspects. However, in young people, it has been observed that demands have a greater impact on engagement and performance, and it may be necessary to reduce conflict and role ambiguity.
Regarding the limitations of the study, the most important is the generalization of the results obtained in a single professional collective, which makes it necessary to separate the study into different professional groups (doctors, nurses, etc.) in future studies. To achieve such differentiation, jobs obtained should be categorized in well-defined professional groups.
Another limitation detected is related to a predominant participation of women in the study, although it should be noted that this distribution represents the reality of the analyzed sector.
Regarding the instruments used, although they are self-reported tests (considering the possible bias that these may represent), those ones whose validity and reliability are widely documented were chosen.
Another limitation of the present study is that data have been collected in the same temporal timeslot. Although SEM analysis provides some information about the possible direction of relationships, drawing conclusions about the causal order between variables is not allowed by cross-sectional studies. There is a need for longitudinal studies to strengthen causal inferences over these job demands and resources that have a bigger impact on the wellbeing and performance of employees.
Another limitation of the present study is that the questionnaire used the resources and demands related to the work group and, however, the differences regarding age and sex are an individual variable. However, although the questions refer to the team, we can verify that the answer is determined by the sex and age of the individual, while the results of the study show significant differences for these demographic variables. In this sense, it can be said that the answers that refer to the team are also determined by sex and age and not only by the perception of the situation of their work team.
Lastly, for future research, it would be interesting to study the effect of organizational interventions addressed to reduce the demands and/or to increase the more relevant job resources for the wellbeing and performance of the employees and see if they have a different effect according to sex and different groups of age.
According to the results obtained, we can conclude that there are differences between job demands and resources both for men and women, as well as for younger and older workers in the healthcare sector. This means that resources and demands behave differently, as well as the impact they cause on work engagement and performance of people. Moreover, from the SEM analysis, it can be confirmed that the motivational path from the JD-R model is maintained, regardless of sex and age.






 Open access
Open access