



A 5-year-old asymptomatic male patient was referred for outpatient echocardiography secondary to a heart murmur.
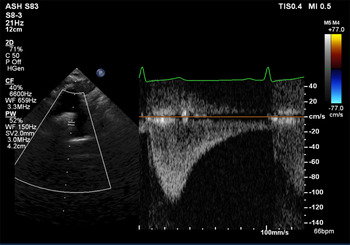
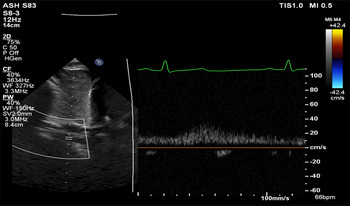
Aortic arch contour was abnormal and appeared to taper at the isthmus. Doppler velocity at the isthmus was within normal limits (1.1 m/s), but a pathologic flow profile with continuation through diastole was noted (Fig 1). Lack of pulsatility and low-velocity continuous flow was found on abdominal descending aorta interrogation (Fig 2). Exam revealed the absence of distal pulses and upper extremity hypertension (139/87 mmHg) with a significant gradient to the lower extremity (72/48 mmHg). CT angiogram confirmed the suspected diagnosis of coarctation of the aorta (Fig 3) and showed extensive vertebral collateralisation supplying the descending aorta. He underwent successful surgical coarctectomy with a lumenal diameter of the excised aortic isthmus found to be less than 1 mm diameter (Fig 4).

Figure 1. Pathologic Doppler profile in the distal aortic arch showing a “diastolic tail” – flow continuation through diastole. Peak velocity (1.1 m/s) is within the normal range.
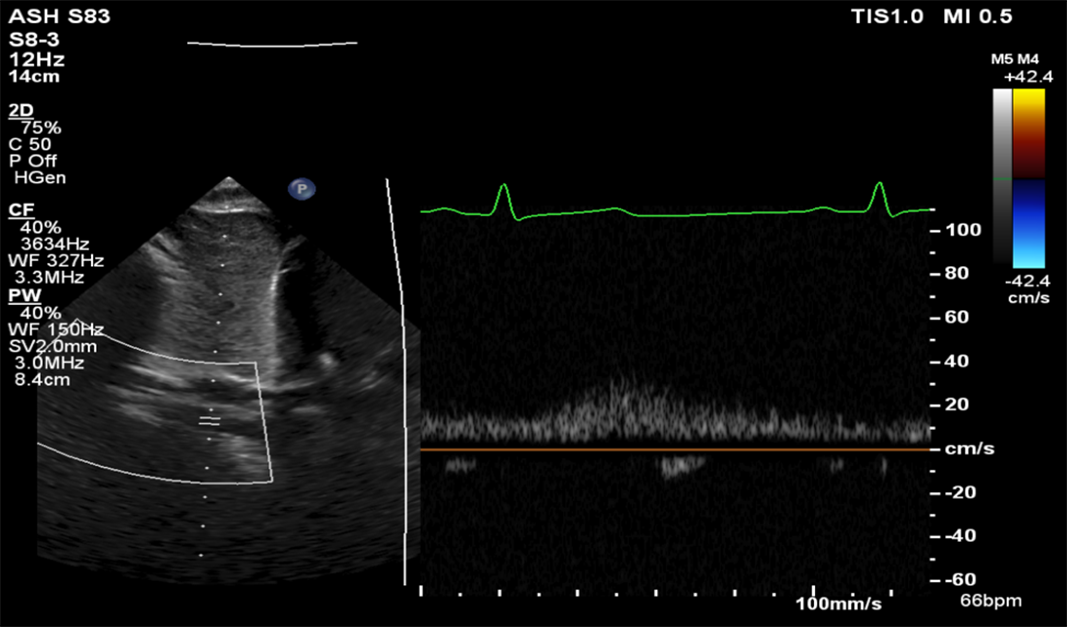
Figure 2. Subcostal duplex Doppler showing lack of pulsatility in the abdominal descending aorta. Low-velocity continuous flow is similar to a venous flow profile.

Figure 3. CT angiogram showing severe short segment juxtaductal coarctation of the aorta with the luminal diameter measuring 1 × 1 mm with well-formed collateral circulation supplying the descending thoracic aorta through the paravertebral arteries.

Figure 4. Excised aortic isthmus with a lumenal diameter of less than 1 mm.
Transthoracic echocardiography is the principal imaging modality for suspected coarctation of the aorta as it is readily available, safe, and offers measurement of coarctation gradient using Doppler, and can assess for associated functional or structural intracardiac abnormalities. CT and cardiac MRI have emerged as second-line advanced imaging modalities, by providing high spatial resolution imaging for intracardiac and extracardiac structures and allows multidimensional reconstruction of vascular anatomy.Reference Dijkema, Leiner and Grotenhuis1,2
We often grade the severity of obstruction by reporting Doppler-derived pressure gradients, and high-velocity flow through the isthmus is expected in severe coarctation. But, a basic tenet of echocardiography is that flow is required to produce a high gradient. When the coarctation has been longstanding and severe, the presence of collateral flow through the vertebral arteries may diminish flow across the coarctation and the Doppler-derived gradient may be less severe than expected for the degree of obstruction.Reference Houston, Simpson, Pollock, Jamieson, Doig and Coleman3 This case elegantly highlights the significance of Doppler flow profile in making the diagnosis – tracings with continuous antegrade diastolic flow in the arch and low amplitude continuous undulating flow in the abdominal descending aorta are pathologic, and provide important indirect evidence for aortic coarctation.Reference Dijkema, Leiner and Grotenhuis1,2,Reference Shaddy, Snider, Silverman and Lutin4–Reference Doshi and Chikkabyrappa6
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflict of interest
None.
Ethical statement
The authors assert that all procedures contributing to this work comply with the ethical standards.



 Open access
Open access