


Numerous indications that adoption of the Mediterranean dietary pattern is associated with decreased all-cause mortality and improvements in levels of cardiovascular risk factors have already been underlined in many studies( Reference Sofi, Abbate and Gensini 1 ). The Mediterranean diet (MD) represents a traditional dietary pattern of people in Greece, Italy, Spain (mostly southern regions) and other Mediterranean countries. This dietary pattern, that successfully combines pleasant taste with positive health effects, does not stand for a homogeneous exclusive model throughout the Mediterranean basin; rather, it represents a set of healthy dietary habits including high consumption of vegetables, fresh fruits, legumes and cereals, and a moderate intake of alcohol, as main sources of fibre and antioxidants, with fish, nuts and olive oil that ensure a high intake of MUFA, associated with a low intake of trans-fatty acids from meat and sweets( Reference Bach-Faig, Berry and Lairon 2 ). Greater adherence to the traditional MD has been associated with a significant reduction in total mortality and improvement in longevity( Reference Sofi, Abbate and Gensini 1 ) as well with lower prevalence and incidence of clustered risk factors( Reference Tzima, Pitsavos and Panagiotakos 3 , Reference Sanchez-Tainta, Estruch and Bullo 4 ) and contrasting findings regarding its effects on obesity( Reference Buckland, Bach and Serra-Majem 5 ). The ongoing trends towards increasing incidence and prevalence of overweight and obesity among populations of the southern European countries may be attributed to a gradual shift from a ‘traditional’ to a ‘Westernized’ diet by the inhabitants of the Mediterranean basin( Reference Moreno, Sarria and Popkin 6 ). The phenomenon of the nutrition transition is connected with the process of urbanization and is usually associated with negative changes in lifestyle habits. Studying nutrition and lifestyle habits in the context of closed environments such islands is interesting in order to assess if the modernization of life influences the habits of island inhabitants and if differences among more rural areas compared with industrialized and urbanized areas still exist. In spite of several epidemiological studies that have evaluated adherence to the MD in Europe( Reference de Lorgeril and Salen 7 , Reference Trichopoulou, Bamia and Norat 8 ), few approaches have tested adherence to the MD specifically in the islands sited in the Mediterranean basin, mainly in Balearic( Reference Tur, Romaguera and Pons 9 , Reference Martínez, Llull and Del Mar Bibiloni 10 ) and Greek islands( Reference Tyrovolas, Polychronopoulos and Bountziouka 11 – Reference Katsarou, Tyrovolas and Psaltopoulou 13 ). Concerning Sicily, the biggest island of the entire Mediterranean basin, there are no data available on dietary habits and the nutrition transition. Thus, the aim of the present study was to assess adherence to the Mediterranean dietary pattern of the general population recruited in both urban and rural areas of Sicily and to evaluate potential associations with sociodemographic, anthropometric and lifestyle characteristics.
Methods
Design and setting
Data were collected through a cross-sectional population-based survey from May 2009 to December 2010 conducted in Sicily, southern Italy. The region includes 6·8 % urban (where most of the population lives) and 83·2 % rural areas( 14 ). The urban and rural areas were chosen through a selection of provinces that are supposed not to be influenced by geomorphologic characteristics (i.e. lowland/mountainous area). Participants from the urban area were recruited in the city of Catania, a metropolitan city of 500 000 inhabitants on the eastern cost of Sicily. The selection was based on a multistage sampling by the main ten districts of the city to obtain a range of varying socio-economic status among the participants. Participants from the rural area were recruited in the village of Lentini, a village of 24 000 inhabitants near the eastern coast of Sicily. The sampling was performed through the selection of a random pool of ten and four general practitioners working in the ten districts of the city and in the village, respectively. The Italian National Health System covers the entire resident population, irrespective of social status or pre-existing health conditions, and provides each citizen with the service of a general practitioner free of charge. Each citizen is required by law to choose one general practitioner from a list at the Local Health Agency. The choice of general practitioner is influenced mainly by the proximity of the general practitioner's office to the citizen's place of residence rather than by the citizen's health status. Only severe impairment and mental illness were considered exclusion criteria. A total number of 3250 inhabitants were randomly selected through the lists of the general practitioners to enrol in the study. Adults were asked to join the survey when attending a visit at the general practitioner's ambulatory clinic. Interviews and measurements (height and weight) were performed during the visit. Participation was not mandatory. Of these, 3190 (2035 urban and 1155 rural) agreed to participate (98 % participation rate) and a final number of 3090 participants were considered suitable to be included in the survey (sixty-four questionnaires were excluded due to incomplete or inconsistent data). Power analysis showed that the number of participants was adequate to evaluate two-sided standardized differences between subgroups of the study and that the investigated parameters greater than 0.5 achieved statistical power greater than 0·90 at the 5 % probability level (P value).
All participants were informed about the aims of the study, agreed to give the requested information and gave an informed consent. The study was approved by the Medical Research Ethics Committee of the University of Catania and was carried out in accordance with the Declaration of Helsinki (1989) of the World Medical Association.
Data collection
The interviews were conducted by one lead investigator and one public health specialist (or attending to the specialization) with a standard approach to data collection by using a questionnaire and standard procedures to perform the dietary recall. The field investigators had previous experience of dietary data collection and underwent 1 d of training by F.G. in order to standardize the methodology of collection among interviewers. The questionnaire included questions about demographics, dietary and lifestyle habits of the participants. Demographic information included age, gender, area of living, marital status, and educational and occupational category. Lifestyle information regarded smoking and physical activity habits. Marital status included (i) engaged/married and (ii) unmarried/widowed. Education was measured by years of schooling and categorized into three groups: (i) low =none/primary/secondary (<9 years); (ii) medium = high school (9–13 years); and (iii) high = university (>13 years). Employment was categorized into four groups which were generated from several professions and specifies the character of the most important employment during the year before the investigation. Since most people aged above 65 years were retired, last employment before retirement was considered for the study. The variable was categorized into: (i) low (unemployed or unskilled professions); (ii) medium (partially skilled professions); and (iii) high (skilled professions) socio-economic status( Reference Miller, Trieman and Cain 15 ). Smoking habits included questions about smoking status, with answers categorized into (i) never smoker, (ii) current smoker and (iii) former smoker (i.e. stopped smoking for >3 months), as well as quantity of cigarettes or tobacco used, duration of the habit and time since stopping. Physical activity status was categorized into: (i) low active (expended energy <16·7 kJ (<4 kcal)/min, i.e. walking slowly, cycling stationary, light stretching, etc.); (ii) moderately active (expended energy 16·7–29·3 kJ (4–7 kcal)/min, i.e. walking briskly, cycling outdoors, swimming moderate effort, etc.); and (iii) highly active (expended energy >29·3 kJ (7 kcal)/min, i.e. walking briskly uphill, long-distance running, cycling fast or racing, swimming fast crawl, etc.). BMI (kg/m2) was calculated as the ratio of weight to height squared by measuring participants’ height to the nearest 0·5 cm (without shoes, with the back square against the wall tape, eyes looking straight ahead, with a right-angle triangle resting on the scalp and against the wall) and weight with a lever balance to the nearest 100 g (without shoes and with light undergarments).
Dietary data
The dietary questionnaire included a slightly modified version of a semi-quantitative FFQ previously designed and validated to capture eating behaviours in Sicily( Reference Pisani, Faggiano and Krogh 16 ). Food intake was assessed through the 24 h recall of the previous day's dietary intake. On a group basis and considering the group size as adequate, the 24 h reported intake can provide a reasonably accurate estimate of mean energy and macronutrient intakes( Reference Kontogianni, Vidra and Farmaki 17 ). Participants were accordingly asked to report in detail the type of food consumed (i.e. brand name for pre-packaged foods or constituents of mixed dishes) as well as the quantity or volume using common household or other measures (i.e. glasses, spoons, or fractions of a plate). Special attention was paid to the day of the recall so that weekend days were not considered and the recall was carried out twice during the study period, both in the temperate and cold seasons to avoid the influence of seasonal variations. Each 24 h recall lasted from 30 min to 1 h, strongly depending on the respondent. Energy density and nutrient intakes were derived from the 24 h dietary recall by a web program containing the food composition tables of the European Institute of Oncology database( Reference Salvini, Parpinel and Gnagnarella 18 ). Food intakes were converted by S.M. and G. Grosso and checked for intra- and inter-individual variability by CV. Despite the seasonal variation, no significant difference was found between the two recalls, probably due to the constantly temperate climate in the region. However, inconsistent results (those exceeding more than 2 sd) were excluded from the analysis (n 38).
A specific assessment was conducted on coffee and alcohol consumption. Caffeine intake included usual weekly frequency, the type of coffee (i.e. ‘espresso’, American, instant coffee), tea, soft and energy drinks, and chocolate intake, as well as quantity (i.e. in 35 ml or 150 ml cups of coffee or tea consumed daily), and the median amount of daily caffeine was computed. Consumption of alcohol included usual weekly frequency, the type of alcohol usually consumed (i.e. red or white wine, beer, other high-alcohol beverages) and the estimated quantity of each type of alcohol (as the number of 100 ml glasses they drank), and the amount of alcohol was converted to grams of ethanol.
Mediterranean diet adherence
The Mediterranean dietary pattern was defined according to the MedDietScore( Reference Panagiotakos, Pitsavos and Arvaniti 19 ), a previously defined score indicating the degree of adherence to the traditional MD. This score assigned each participant a rating (from 0 to 5, or the reverse) for each of the food groups mainly inherent with the characteristics of the Mediterranean dietary pattern depending on his/her weekly consumption. An increasing score (i.e. from 0 to 5) was assigned according to participants’ increased weekly consumption of items presumed to be close to this pattern: (i) non-refined cereals (wholegrain bread and pasta, brown rice, etc.), (ii) potatoes, (iii) fruit, (vi) vegetables, (v) legumes, (vi) fish and (vii) olive oil use in daily cooking; whereas the scores on a reverse scale (i.e. from 5 to 0) were assigned for consumption of those items presumed to be away from this dietary pattern: (viii) meat and meat products, (ix) poultry and (x) full-fat dairy products (such as cheese, yoghurt, milk). Since an association of alcohol drinking with cardiovascular risk has been observed( Reference Ronksley, Brien and Turner 20 ), usual alcohol intake was evaluated with a non-monotonic scoring system (i.e. assigning a score of 5 for consumption of <300 ml/d, a score of 0 for no consumption or for consumption of >700 ml/d, and a score of 4 to 1 for consumption of 600–700, 500–600, 400–500 and 300–400 ml/d, respectively). The final score ranged from 0 to 55 and higher values of this diet score indicate greater adherence to the MD. Adherence rates were plotted by dividing the score in ranges of four points for a better graphical presentation of the data.
Statistical analysis
Continuous variables were presented as means and standard deviations; Student's t test for independent samples was used to evaluate mean differences between normally distributed variables whereas the Mann–Whitney U test was used for non-normally distributed continuous variables. Accordingly, one-way ANOVA using Bonferroni correction and the Kruskal–Wallis test were used for multiple comparisons. Normality was evaluated by use of the Kolmogorov–Smirnov test.
Within- (intra-) and between- (inter-) individual components were estimated for the two data collections. The within- (CVw = S w/mean of each nutrient) and between-individual (CVb = S b/mean of each nutrient) CV were calculated using a formula provided by Beaton, where S w and S b are the square roots of the estimated intra- and inter-individual variance, respectively( Reference Beaton, Milner and Corey 21 ).
In order to evaluate the association between demographic and behavioural data and adherence to the Mediterranean dietary pattern, multiple regression models adjusted by age and gender were performed considering the tertiles of MedDietScore values as dependent variables; the results are presented as odds ratios with the corresponding 95 % confidence intervals.
All reported P values were based on two-sided tests and compared with a significance level of 5 %. The statistical software package SPSS version 17 was used for all statistical calculations.
Results
Of the 3190 participants included in the study, nearly 60 % were female, the mean age was 51.8 (sd 16·2) years and the mean BMI was 25·4 (sd 4·03) kg/m2, with 35·4 % of participants being overweight and 13·9 % obese. The distribution of MedDietScore roughly followed a normal distribution both in the rural and urban areas (Kolmogorov–Smirnov P < 0·001) with a significant difference between the two environments (Fig. 1). Indeed, the overall mean MedDietScore was 27·5 (sd 6·5), whereas comparing the two areas, rural participants were barely more significantly adherent than their urban counterparts (27·8 v. 27·2, respectively, P = 0·037). Table 1 reports mean MedDietScore values for variables of major interest. Higher adherence was found in older participants with higher educational level. On the contrary, obese participants younger than 35 years old reported having low mean MedDietScore values demonstrating a scarce adherence to the MD. High mean MedDietScore values were also reported among participants consuming a moderate (12–35 g/d) quantity of alcohol derived from red wine (P < 0·001).
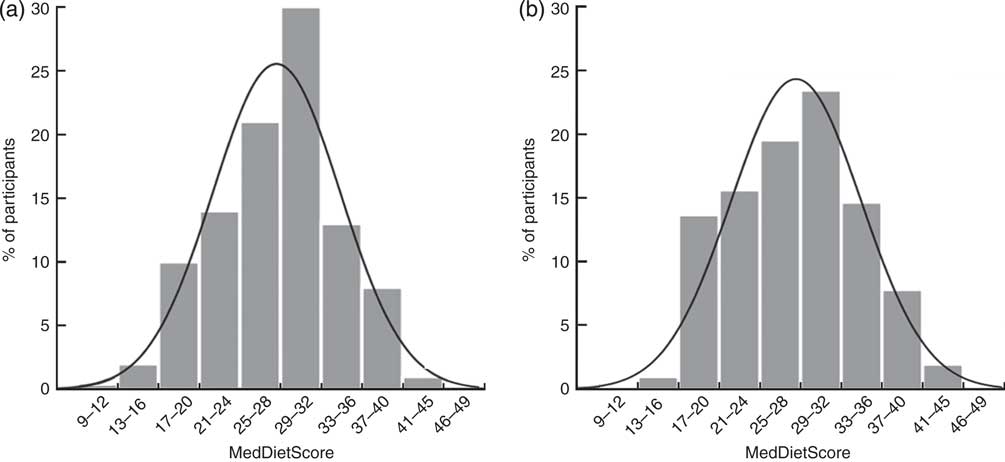
Fig. 1 Distribution of percentage adherence to the Mediterranean dietary pattern (as measured by the MedDietScore) by place of living: (a) rural areas and (b) urban areas; Sicily, southern Italy, May 2009–December 2010 (n 3090)
Table 1 Demographic characteristics of the study population by Mediterranean diet adherence score; Sicily, southern Italy, May 2009–December 2010 (n 3090)
Ratios of intra- to inter-individual variations in energy and nutrient intakes ranged from 0.7 for alcohol to 1.5 for vitamin C (Table 2). Examination of within- and between-individual CV (CVw and CVb, respectively) showed that high ratios resulted from low CVb for some macronutrients such as protein and carbohydrate, and from high CVw for micronutrients such as vitamin C. Some foods, such as cereals and dairy products, had both high CVw and low CVb, giving them the highest ratios (Table 2).
Table 2 Intra-individual and inter-individual CV in the study population; Sicily, southern Italy, May 2009–December 2010 (n 3090)

CVw, intra-individual coefficient of variation; CVb, inter-individual coefficient of variation.
In the total sample, the MedDietScore was correlated (Pearson or Spearman) with intakes of MUFA (r = 0·049; P < 0·05), fibre (r = 0·138; P < 0·001) and vitamin C (r = 0·039; P < 0·05), whereas no association was found for the other nutrients calculated (Table 3). Regarding foods, non-refined cereals (r = 0·056; P < 0·05), vegetables (r = 0·200; P < 0·001), fruit (r = 0·330; P < 0·001), meat (r = −0·073; P < 0·001), dairy products (r = 0·039; P < 0·05), alcohol (r = 0·106; P < 0·001) and nuts (r = 0·051; P < 0·05) consumption were correlated with the MedDietScore.
Table 3 Energy, nutrient and food intakes of the participants and correlation coefficients (r) with the MedDietScore; Sicily, southern Italy, May 2009–December 2010 (n 3090)

*P < 0·05, ***P < 0·001.
†Significance tested by Pearson's or Spearman's correlation coefficient, as appropriate.
The variables associated with high adherence to the MD (i.e. high v. low tertile of MedDietScore) with odds ratios and respective 95 % confidence intervals are presented in Table 4. Participants scoring low on the MedDietScore had lower educational level and were younger compared with those scoring medium or high. Regression analysis revealed that older and more educated people were more likely to be in the highest tertile of MedDietScore (OR = 1·90; 95 % CI 1·39, 2·59 and OR = 1·29; 95 % CI 1·05, 1·58, respectively). Moreover, the percentage of obese people among low-adherent participants was higher than that in the other two groups. Total consumption of alcohol was generally low in the whole sample (67·9 % reported not drinking alcohol), but a significant difference in quantity (moderate, OR = 2·01; 95 % CI 1·46, 2·77) and quality (red wine, OR = 2·07; 95 % CI 1·45, 2·94 and beer, OR = 1·65; 95 % CI 1·02, 2·67) of alcohol was found according to adherence to the MD. Finally, more active participants were 1·5 times more likely to form part of the high adherence group.
Table 4 Demographic characteristics of the study population by tertile of MedDietScore and multiple logistic regression analysis of factors associated with high adherence to the Mediterranean diet, adjusted for age and sex; Sicily, southern Italy, May 2009–December 2010 (n 3090)

*P < 0·05, ***P < 0·001.
†Low v. medium/high tertile.
Discussion
Studies examining adherence to the MD among people living in Mediterranean islands are scarce. We studied population-based nutritional data from 3090 individuals in Sicily and evaluated their adherence to the MD. We assessed relatively good adherence to the MD, with 40·2 % of men and 59·8 % of women reporting to follow the principles of the MD (high adherence group). Hence, our results agree with findings of previous studies assessing low to moderate adherence to the traditional dietary patterns among the inhabitants of Mediterranean islands( Reference Tur, Romaguera and Pons 9 , Reference Tyrovolas, Polychronopoulos and Bountziouka 11 , Reference Katsarou, Tyrovolas and Psaltopoulou 13 ). When analysing adherence by demographic characteristics such age, our findings supported previous evidence of lower adherence to the MD among younger generations compared with older people( Reference Moreno, Sarria and Popkin 6 , Reference Kontogianni, Vidra and Farmaki 17 , Reference di Giuseppe, Bonanni and Olivieri 22 ). Another noteworthy finding was similar adherence to the MD among people living in the different environments (urban/rural) after adjusting for potential confounders. Data from studies point out that diets of Mediterranean populations are gradually moving away from the traditional patterns( Reference León-Muñoz, Guallar-Castillón and Graciani 23 , Reference Trichopoulos and Lagiou 24 ). Although several factors contribute to the corroborated phenomenon of the nutrition transition, it seems that the change to modern lifestyles, especially in the younger generation, plays a major role independently of the place of living. Some evidence has demonstrated a relatively good stability of traditional dietary habits over time irrespectively of urbanization of life( Reference Pelucchi, Galeone and Negri 25 ). Regarding our sample, rural participants had a higher average MedDietScore compared with their urban counterparts maybe due the mediating effect of age, since the mean age of people living in the rural areas was higher than that of people living in the urban areas. Another factor found to influence adherence to the MD in the present study was educational level, which was higher among the urban participants compared with the rural. Indeed, it has been documented in many previous studies that different educational groups have healthier food choices (i.e. more adherent to the MD) probably due to increased nutrition knowledge and increased motivation to follow healthy lifestyles( Reference Moreno, Sarria and Popkin 6 , Reference Katsarou, Tyrovolas and Psaltopoulou 13 , Reference Pelucchi, Galeone and Negri 25 – Reference Bibiloni Mdel, Martínez and Llull 28 ). We confirmed the aforementioned trend, since participants in the medium educational category, mostly representative in the urban sample, were more likely to adhere to the MD compared with participants in the lower educational category. On the contrary, we did not find the same association between the higher educational category and the MedDietScore, probably due to the low percentage of participants recruited in this category. Another possible reason explaining the good adherence in both environments may be the close proximity of the rural and urban areas in the context of a relatively small island that may allow the urban centres to offer a wide availability of foods, even those more popular in the rural areas such as fresh fruit and vegetables. Thus the urban areas of Sicily may not be representative of modern urban centres but, on the contrary, may offer the same food quality as the rural environments.
Adherence to the MD was found to be also connected with quantity (moderate) and quality (red wine and beer) of alcohol intake in our study. Such a finding is not surprising, since both variables characterize the traditional Mediterranean dietary pattern( Reference Bach-Faig, Berry and Lairon 2 ). On the contrary, we revealed a curious association between adherence to the MD and moderate caffeine intake. Some previous studies reported that coffee consumption is common in the Mediterranean area and such an association may have a synergistic beneficial effect with the MD on preventing diabetes and hypertension( Reference Sotos-Prieto, Carrasco and Sorli 29 , Reference Panagiotakos, Lionis and Zeimbekis 30 ). However, it is still not clear if such benefits are mediated by caffeine intake or coffee consumption, and further research is needed to assess this issue.
Due to the increasing trends of overweight and obesity in the Mediterranean area, several issues have been pointed out regarding the beneficial effects of the MD on the development of obesity( Reference Buckland, Bach and Serra-Majem 5 ). Although the MD has been considered a high-fat diet, some evidence has demonstrated that adoption of this dietary pattern is associated with favourable effects on weight gain probably due to the high content of MUFA that decreases resistance to the peripheral action of insulin and thus the prevalence of obesity( 31 ). However, a controversy on the role of the MD on body weight and obesity status still exists. In our analysis, we found an inverse correlation between the MedDietScore and BMI status. We speculate that although food habits in the island are particularly well handed down and similar to the old traditional diet characterizing this isolated area of the Mediterranean Sea, a few differences from the old to the new dietary behaviours have developed over time, such as the transition from whole to refined grains, the use of sugary drinks and the higher quantities of bread and pizza, all features that may lead to increased intake of energy and, consequently, contribute to the development of obesity.
Despite our study having the strength of being the only survey exploring adherence to and several characteristics (including nutrient intake) associated with the MD conducted in Sicily, some potential limitations should be reported in order to consider our results. First, the cross-sectional design of the study did not allow us to estimate any causal relationship between lifestyle parameters and adherence to this specific dietary pattern. Moreover, although many variables have been taken into account, the potential for residual confounding by uncontrolled covariates may still exist. Finally, the methodology used to collect dietary data has some limitations related to memory and bias. FFQ and 24 h dietary recalls may lead to under-reporting or over-reporting of the frequency or amount of foods, which in turn are significant contributors to the systematic bias of self-reported dietary assessments. Biomarkers of energy intake have been suggested to play a useful role in dietary assessment, but limitations still exist. Thus, advantages and limitations of such instruments must be taken into account.
Conclusion
Although adherence to the MD is still mostly representative for the adult population living in Sicily, a slow but concrete moving away from the traditional patterns has been observed in younger people. Further analyses are needed to explore other lifestyle factors associated with the abandoning of this dietary pattern, as well as its impact on health and disease.
Acknowledgements
Sources of funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. G. Grosso was supported by the International PhD Program in Neuropharmacology, University of Catania Medical School, Catania, Italy. The contributors had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. Conflicts of interest: There are no conflicts of interest. Authors’ contributions: G. Grosso and A.M. contributed in study design; S.M., D.D., T.R., F.G. and G. Giorgianni contributed in collecting and analysing the data; G. Grosso, A.M. and F.G. contributed in preparation of the manuscript. Acknowledgements: The authors thank the field investigators of the study, namely P. Giorgianni, S. Toscano, L. Bruno, A. Rampulla, S. Grasso, G. Gaeta, S. Siracusano, G. Giorgianni, A. Platania, F. Nolfo, S. Rametta and N. Laudani.





