



Background
Consistent and appropriate use of research findings to inform policy and practice has been shown to improve health outcomes (Graham et al., Reference Graham, Logan, Harrison, Straus, Tetroe and Caswell2006; Grol, Reference Grol2001; Hanney & González-Block, Reference Hanney and González-Block2015; McGlynn et al., Reference McGlynn, Asch, Adams, Keesey, Hicks and DeCristofaro2003). Unfortunately, this does not happen often, and a gap exists between research and the actual use of research findings (Bero et al., Reference Bero, Grilli, Grimshaw, Harvey, Oxman and Thomson1998; Lewis et al., Reference Lewis, Jewell, Turpie, Patterson, McCoy and Baxter2005; Mallonee, Fowler, & Istre, Reference Mallonee, Fowler and Istre2006). Factors that contribute to this research-to-practice gap include: lack of communication between researchers and intended users of research (who may include policy makers and decision makers, patients, and frontline health care providers) findings; a too general, or too narrow research focus; lack of effective promotion of research findings and their relevance to users; and lack of support from health care policy and decision makers at various levels in the health care system (Mallonee et al., Reference Mallonee, Fowler and Istre2006; Sussman, Valente, Rohrbach, Skara, & Ann-Pentz, Reference Sussman, Valente, Rohrbach, Skara and Ann-Pentz2006). These factors can be addressed in part by knowledge translation or implementation science (Graham et al., Reference Graham, Logan, Harrison, Straus, Tetroe and Caswell2006; Nilsen, Reference Nilsen2015). Knowledge translation is defined as “a dynamic and iterative process that includes synthesis, dissemination, exchange and ethically sound application of knowledge to improve the health…, provide more effective health services and products and strengthen the health care system” (Canadian Institutes of Health Research, 2015).
In this article, we consider knowledge translation in the context of older adults. A focus on older adults is timely because of Canada’s aging population, and the related expected increases in the demand for health programs and services (Canadian Institute for Health Information, 2011; Chatterji et al., Reference Chatterji, Kowal, Mathers, Naidoo, Verdes, Smith and Suzman2008; Ries, Reference Ries2010; Statistics Canada, 2021). One way of meeting this demand is to improve the health care system’s ability to generate, share, and use knowledge and innovations in the field of health and aging. Researchers have examined the ways in which evidence derived from research, as well as practice-based knowledge, is shared and translated into policy and practice. One mechanism to promote knowledge-to-action (KTA) that has garnered considerable interest is the community of practice (CoP) (Brown & Duguid, Reference Brown and Duguid1991; Snyder & Briggs, Reference Snyder and Briggs2003; Kothari, Boyko, Conklin, Stolee, & Sibbald, Reference Kothari, Boyko, Conklin, Stolee and Sibbald2015).
There are several explanations of CoPs with a common theme that they are made up of individuals with a common interest. Wenger (Reference Wenger2016) defines CoPs as “…groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly” (p. 2). Wheatley (Reference Wheatley2005) introduces the idea of “advancing the field of practice” and “sharing” knowledge, which moves the focus from the groups’ interacting and learning as an end in itself to making the knowledge available for the benefit of others outside the immediate group.
CoPs are not restricted to any particular area; they can be found in business, academia, and the health care sector (Lesser & Everest, Reference Lesser and Everest2001; Lesser & Storck, Reference Lesser and Storck2001; Li et al., Reference Li, Grimshaw, Nielsen, Judd, Coyte and Graham2009b; Kothari et al., Reference Kothari, Boyko, Conklin, Stolee and Sibbald2015). According to Wenger (Reference Wenger2016), CoPs have three characteristics: the domain, the community, and the practice. Domain refers to the common interest that the members share. Related to the common interest are the unique competencies and skills that differentiate members of a CoP from people outside the group. “Community” refers to relationships resulting from the group interactions that enable learning and functioning. “Practice” refers to shared experiences, resources, and ways of doing things. A CoP “is like a virtual center of excellence, where all the partners are experts” (Snyder & Briggs, Reference Snyder and Briggs2003, p. 4). CoPs have been described as mobilizers of KTA; they are composed of members from diverse backgrounds and experiences who otherwise might not interact but for their common vision and passion. The members bring with them external connections and networks, which widen the CoP reach with regard to sources of knowledge. The connections also expand the CoP’s reach with regard to disseminating and promoting use of knowledge. The diversity of CoP members is a reservoir of explicit knowledge (such as published research) and tacit knowledge (such as expertise and experience-based knowledge).
According to Collins (Reference Collins2010), tacit knowledge is knowledge that cannot be explicated; it resides in individuals, and comprises three distinct phenomena: weak (relational tacit knowledge referring to knowledge that guides interpersonal interactions), medium (somatic tacit knowledge, which refers to aspects of knowledge that are connected to the physical body, for example knowing when one is not feeling well), and strong tacit knowledge or collective tacit knowledge, which is the knowledge that differentiates human beings from other living things. In contrast, explicit knowledge can be accessed, packaged in different forms, explicated, and disseminated for use (Wyatt, Reference Wyatt2001). Although tacit and explicit knowledge differ, the two relate in a dynamic way (Adler, Reference Adler, Pogorel and Allouche1996). This relationship can be observed in a CoP, for example, in the process of identifying and deciding on the specific area of focus, or knowing where to get the information (tacit), and in synthesizing knowledge and developing the recommendations for use to address an issue (explicit knowledge).
The members of CoPs take on different roles. Benne and Sheats’ (Reference Benne and Sheats2007) framework places group roles in three categories: (1) group task roles related to the issue and the task at hand, which enable the group to successfully accomplish a task, and address the issue of concern to the group; (2) group building and maintenance roles that guide how the group functions as a team; and (3) individual roles that are concerned more with the individual member’s needs not relevant to the successful accomplishment of the task or the cohesive and productive functioning of the group. This last category can potentially have a negative effect on the group (Snyder & Briggs, Reference Snyder and Briggs2003).
CoPs exemplify collective and social learning, in which bodies of knowledge are cultivated through involvement of a variety of voices and opinions. This is especially important because knowledge is fluid and ever changing, which makes it difficult for any one individual to master knowledge in one particular field on their own (Wenger, McDermott, & Snyder, Reference Wenger, McDermott and Snyder2002). CoPs are increasingly being used to translate knowledge into practice and there has been research and discussions on CoPs’ KTA processes (for example Handley, Sturdy, Fincham, & Clark, Reference Handley, Sturdy, Fincham and Clark2006; Li et al., Reference Li, Grimshaw, Nielsen, Judd, Coyte and Graham2009a; Roberts, Reference Roberts2006). More research is needed to further understand how CoPs contribute to KTA processes in specific contexts. In the study reported here, we were interested in gaining a deeper understanding of the KTA processes of a CoP that was focused on synthesizing and sharing knowledge related to environmental design changes to improve wayfinding for persons with dementia living in long-term care (LTC) environments.
The CoP examined in this study, hereon in referred to as the CoP1P, was initiated in 2010 as a partnership between the Alzheimer Knowledge Exchange (AKE) now known as the BrainXchange, and the Seniors Health Knowledge Network (SHKN). The AKE is a virtual platform that health care professionals use to share knowledge and best practices, and to build professional partnerships. SHKN, formerly the Seniors Health Research Transfer Network, was launched in 2005 by the Ontario provincial government. It is a network of networks that work together to improve the quality of health care provided to seniors by facilitating knowledge exchange opportunities for formal and informal caregivers, researchers, and policy makers (Conklin, Stolee, Luesby, Sharrat, & Chambers, Reference Conklin, Stolee, Luesby, Sharratt and Chambers2007). The collaboration facilitates knowledge exchange through a library service, knowledge brokers, local implementation teams, collaborative technology, and CoPs whose members work together to identify innovations, translate evidence, and help implement changes in practice (Conklin et al., Reference Conklin, Stolee, Luesby, Sharratt and Chambers2007).
The goal of the CoP1P was to synthesize and translate knowledge into practical tools, and to inform changes in practice, programs, and policy on dementia care. The CoP derives its membership from a pool of the approximately 2,000 members of the AKE who include researchers, educators, health care providers, family caregivers, policy makers, and stakeholder organization representatives working in dementia-related research, policy, or care.
The KTA initiative for the CoP1P that served as the case study for this article was the Wayfinding Initiative, the aim of which was to develop a practice design recommendations toolkit to facilitate individuals with dementia finding their way around the LTC homes. Wayfinding refers to “an integrated system of navigation that enables individuals to find their way quickly and easily within a built environment” (Alzheimer Knowledge Exchange, 2013, p. 1). This initiative arose from CoP members’ recognition of an increasing need to assist persons with dementia, who often experience spatial disorientation, to find their way more easily within their physical environment.
This CoP case study was part of a larger 3-year multiple case study that involved SHKN CoPs working to improve practice and the health of seniors in Ontario, Canada (Conklin, Kothari, Stolee, Chambers, Forbes, & Le Clair, Reference Conklin, Kothari, Stolee, Chambers, Forbes and Le Clair2011). Similar to the other case studies in our program of research (Conklin et al., Reference Conklin, Kothari, Stolee, Chambers, Forbes and Le Clair2011), this case study (Wayfinding Initiative CoP) sought to understand the KTA processes that were initiated through the CoP. Specifically, this project aimed to understand: (1) the extent to which the KTA process involved explicit and tacit knowledge, (2) how active involvement of knowledge users in the CoP influenced knowledge utilization, and (3) the factors that supported or hindered the KTA process.
Methods
A case study methodology allows for in-depth explorations of complex social phenomena within their natural contexts (Anaf, Drummond, & Sheppard, Reference Anaf, Drummond and Sheppard2007; Tellis, Reference Tellis1997) and is therefore an appropriate method for studying processes that occur within CoPs as well as those that extend from CoPs to frontline health care settings (Connell, Lynch, & Waring, Reference Connell, Lynch and Waring2001). Findings from case studies have been used by health services researchers to develop explanatory theories, evaluative conclusions, and recommendations for interventions in health care (Baxter & Jack, Reference Baxter and Jack2008). Different from other types of qualitative methods, case study research involves intensive analyses and descriptions of a single unit or system bounded by space and time and is grounded in multiple sources of information (e.g., interviews, observations, document reviews; Hancock & Algozzine, Reference Hancock and Algozzine2006). A detailed description of the methods used in this study and in the other case studies that make up this program of research, can be found in a study protocol published by the investigators (Conklin et al., Reference Conklin, Kothari, Stolee, Chambers, Forbes and Le Clair2011).
Ethics clearance for the project was obtained from the Health Sciences Research Ethics Board of Western University (#17879E), the Bruyère Continuing Care Research Ethics Committee (#M16-11-004), the Concordia University Human Research Ethics Committee (#HU2010-115), and the University of Waterloo Office of Research Ethics (ORE#16894).
Data Collection
Data collection involved key informant interviews, document reviews, and observations, thus providing methodological triangulation. Members of the CoP who had been actively involved were invited to participate in an interview. Interviewees were purposively selected to include members with leadership, knowledge brokering, and knowledge user roles. Semi-structured interview guides were developed for the multiple case study project; the interview guide is included as an additional file in our published protocol article (Conklin et al., Reference Conklin, Kothari, Stolee, Chambers, Forbes and Le Clair2011). Review of CoP documents provided background information on the CoP, including its membership and its goals. The review also provided information on the sources of knowledge that were used in the KTA process. To gain a closer perspective of interactions, processes, and relationships within the CoP community, a member of the research team (K.M.) recorded observations as field notes after observing the CoP meetings and events (Baker, Reference Baker2006; DeWalt & DeWalt, Reference DeWalt and DeWalt2002).
As a first step in the data-collection process, a teleconference was held with five CoP members (two CoP leads, one SHKN knowledge broker, and two CoP planning members). The purposes of the teleconference were: (1) to introduce the research project, including research activities and outputs, and to review the CoP members’ role in the project; and (2) to learn about the CoP1P and their plan for the Wayfinding Initiative. Data collection then proceeded as follows:
-
1. Interviews: Four semi-structured, 30-minute interviews were conducted with two CoP leads and two CoP planning members at the start of the observation period, to provide contextual data. Additionally, four semi-structured follow-up interviews and four concluding interviews were conducted at the end of the observation period to further understand the behaviours, activities, and environment related to the KTA initiative. The four follow-up and the four concluding interviews involved frontline and non-frontline staff, and took approximately 30 minutes each. Every interviewee was given the opportunity to review their transcript and correct errors or add information; no substantial changes were requested.
-
2. Meeting Observations: A researcher (K.M.) observed all of the meetings (n = 9) held by the CoP over a 12-month period to plan the KTA initiative. These meetings took 60–90 minutes, and were usually facilitated by the same two CoP co-leads. The number of participants in the planning meetings ranged from four to eleven. Topics discussed included updates on CoP membership, literature and resource development, task assignment, future planning, and new issues and opportunities for the CoP.
-
3. Field Notes: After each meeting, rough field notes and audio recordings were used to develop more formal field notes using a standard template. Field notes captured emerging patterns with respect to knowledge types, member roles, and other contextual factors.
-
4. Document Review: Documents about the CoP and the KTA initiative were obtained from the CoP knowledge broker, and relevant information was collected from the documents for analysis.
All interviews and meetings were audio recorded with consent from participants, and were transcribed verbatim. All CoP members who participated in the planning meetings and interviews provided informed consent to take part in the study.
Data Analysis
This article reports on the results of emergent coding that was done following the principles of qualitative description and thematic content analysis (Strauss & Corbin, Reference Strauss and Corbin1990). Emergent coding and analysis of the text allowed new themes to emerge from a thorough review of the data. More than 90 codes were identified from the data analysis. The codes were reviewed, and similar and related codes were grouped together to form a theme. Themes were identified, relationships and connections between themes were assessed, and a summary of findings was drawn (Braun & Clarke, Reference Braun and Clarke2006; Hsieh & Shannon, Reference Hsieh and Shannon2005). The resulting themes were supported by multiple codes and examples from the data; if a theme was not well supported, it was either eliminated or combined with another idea. To assure strength and quality of the analysis (Pope, Ziebland, & Mays, Reference Pope, Ziebland and Mays2000), two researchers conducted the analysis and one of the principal investigators was involved when the two researchers differed in their coding. The research team then synthesized the findings into a detailed case report that highlighted the emerging themes and detailed a description of each theme. The team prepared a thick description of the case study that described the knowledge informing the CoP’s KTA initiative, the knowledge facilitation and translation mechanisms (adaptation, understanding, utilization), and the involvement of users in the KT process.
Developing a Diagram to Represent Results
The next step involved a more detailed analysis to determine interactions and connections among the themes. This involved printing the themes and their descriptions on individual pieces of paper and taping them to a large board. The researchers then examined each theme and description. Connections between themes were noted, allowing researchers to develop a diagram to better display the results.
The results of the analysis and development of the diagram, which were discussed extensively at a team meeting, are discussed in the following section.
Results
The CoP and Case (KTA Initiative)
The KTA initiative for the CoP1P was intended to develop a toolkit with guidelines to assist in wayfinding for people with dementia living in LTC homes (see Table 1 for related acronyms and meaning). The intended recipients of the Wayfinding Toolkit included frontline caregivers (nurses, nursing assistants, physiotherapists, occupational therapists, and other allied health professionals), and administrators within LTC. The toolkit was considered to be of particular interest to those working in LTC, as they deal with issues of responsive behaviours and wayfinding with residents on a daily basis.
Table 1. Acronyms and meaning
The Wayfinding Initiative of the CoP1P included a knowledge broker, two co-leads, and five to nine participants. Team members were selected based on an invitation from the knowledge broker sent to the larger AKE membership to see who might be interested in joining the initiative. The CoP1P planning team was composed of researchers, health care providers (predominantly psychogeriatric resource consultants who provide consulting support to LTC homes), students, and stakeholder organization representatives involved in dementia care (see Table 2 for participant roles/perspectives). The CoP held planning meetings once a month. These were chaired by the CoP co-leads and co-facilitated by the SHKN knowledge broker. The initiative included an information specialist’s initial literature search on wayfinding to identify potential design topics and considerations for persons with dementia. The SHKN knowledge broker amalgamated this information into a document and separated the information into initial sub-categories related to specific design features and brought this to the planning team. Subsequent literature searches filled information gaps, and members collaborated on further development of the document through a number of in-person and virtual planning meetings. The final version of the Wayfinding Toolkit was shared with the larger AKE membership via a webinar on January 21, 2013; a total of 15 individuals outside of the core planning team attended the webinar.
Table 2. Participant roles
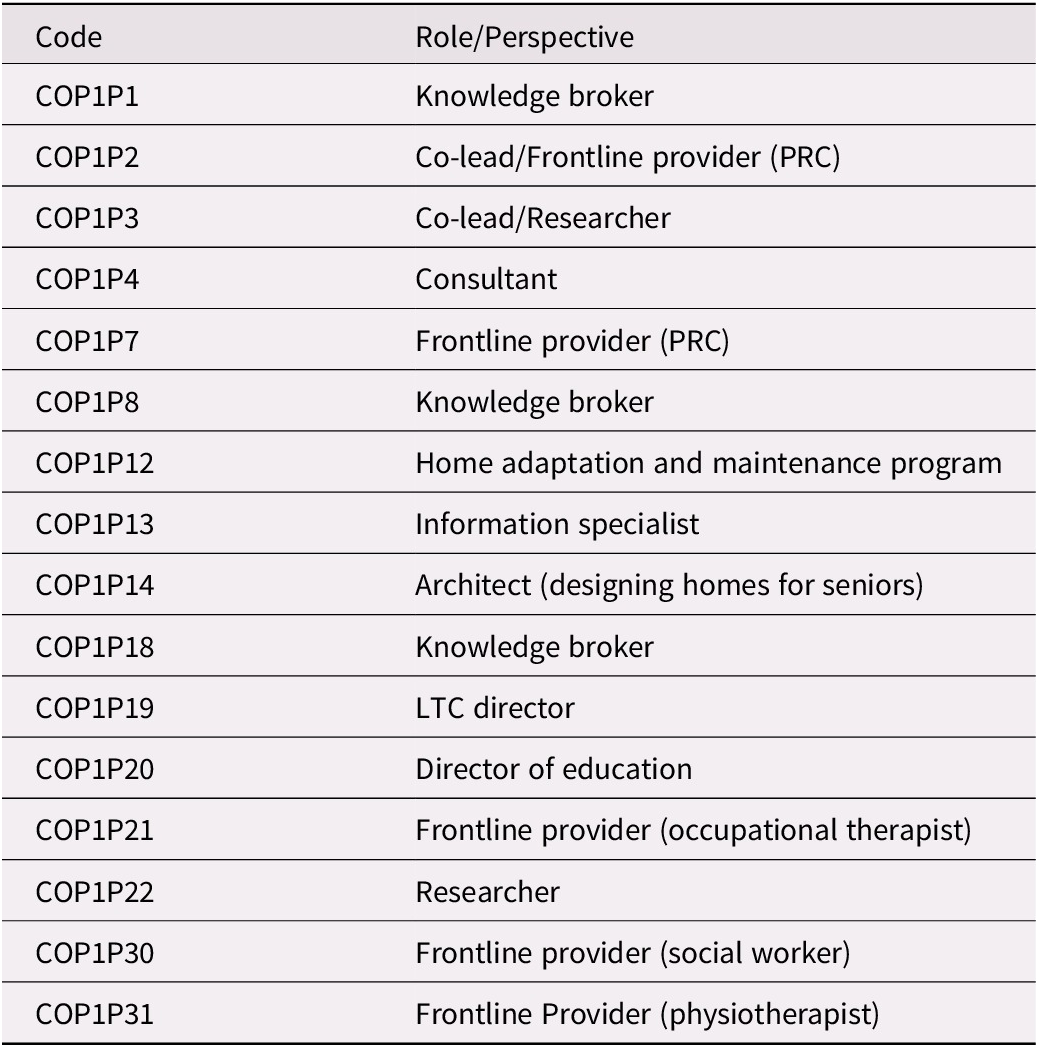
Note. PRC = psychogeriatric resource consultant; LTC = long-term care.
The purpose of the webinar was to share the recommendations with the larger AKE audience who expressed interest in CoP1P, particularly wayfinding. The CoP also used the webinar to gather feedback on the recommendations before broader dissemination took place. The planning team hoped to use the webinars to reach not only frontline care providers and long-term care administrators, but also representatives of important stakeholder organizations such as the Alzheimer Society. The planners were particularly interested in reaching policy and decision makers through the webinar; however, this proved to be a challenge as reflected in the following field note from a planning meeting:
In terms of the target population for the webinar, the group was pleased with the diversity of attendance. However, they did mention that they would like to see more representation from legislative or regulatory bodies (e.g., fire marshals) –they want to attract people that can make a “regulatory” or political difference as well as people that can use the information in a practical way. They mentioned that they have been previously successful in reaching out to the Ministry of Health and the fire marshals to receive input on the development of their previous toolkits. Although they would ideally like to see such representation at the webinar, they are not sure what the best way to get them there would be. They also pointed out that they have been successful in reaching more individuals outside of the field of health, including architecture. (Source: Field Note)
Attendees of the webinar appreciated that the toolkit produced by the CoP included recommendations for simple, manageable, and cost-effective design changes (e.g., signage) that could be made in their facility to assist with wayfinding. Frontline staff felt that they would be able to put into practice small changes that required few resources and minimal or no administrative input. They also expressed that they felt that the recommendations were credible given the support provided through both the academic literature review and the experiential knowledge provided by members of the CoP planning team.
Results from Emergent Coding
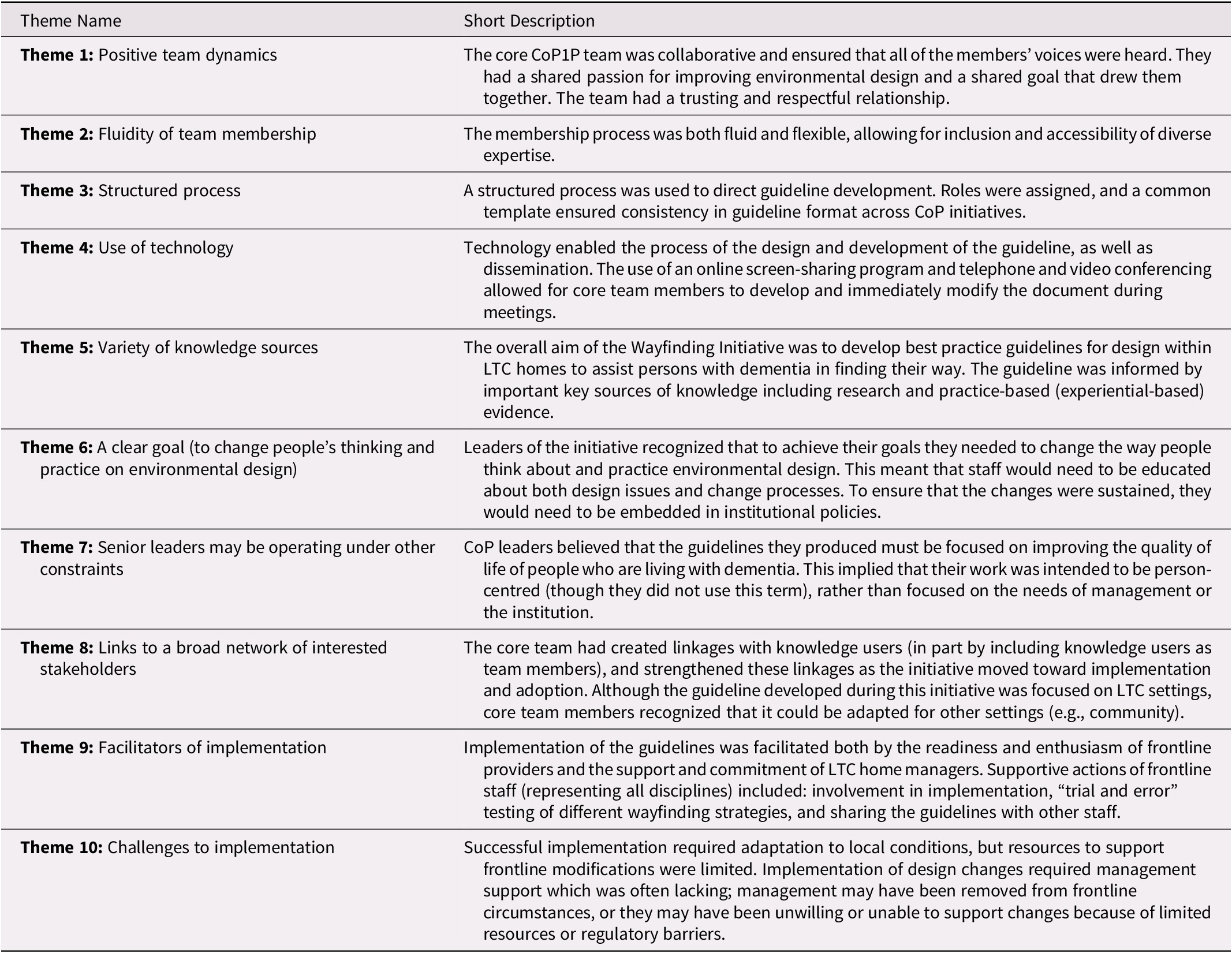
Ten themes emerged from the data analysis; these are summarized in Table 3 and considered in the following paragraphs.
Table 3. Emerging themes
Theme 1: Positive Team Dynamics
The formation of the CoP1P was facilitated by the SHKN and composed of members committed to developing practice design recommendations to facilitate wayfinding for individuals with dementia, in particular those living in LTC homes. The members included individuals with diverse perspectives and expertise who represented a variety of professions such as: psychogeriatric resource consultants (PRCs), architects, academics, Alzheimer-related organizations, and students. During one of the planning meetings, the researcher observed that some CoP members were experts in environmental design. They also had access to resources such as research articles that they shared with the group. One member had extensive knowledge on wayfinding and had conducted considerable research on the topic.
The CoP members were collaborative, organized, and supportive of one another. The CoP created a good environment for the members to contribute to a cause they cared about, as CoP1P3 (to protect the identity of research participants, they are identified by codes beginning with the letters CoP1P) expresses in the following quote:
…this community of practice seems very well suited in terms of personalities and strengths and we are able to really count on one another… to trust one another with information, and I think it is a very nice blend of folks to work with and we don’t push ourselves hard because this is not our full time job, but when we do create something, we’re pretty proud of it. It’s a very collaborative group effort in anything we do (COP1P3).
Clear expectations of members were necessary to ensure proper group functioning. For example, to remain in the group, members were expected to attend all meetings, and they would be dropped if they failed to attend three consecutive meetings. They were also expected to read documents and to provide input in the development of the guidelines.
Another factor that contributed to the functioning of the group was the freedom they had to contribute whatever knowledge they had regarding the guidelines. Their suggestions on additions, changes, and improvements were well received and incorporated in the initiative. For example, COP1P2 suggested that the group could later work on signage, either as an addition to the document that they were working on, or as a separate companion document. Other members were keen on details, and they identified gaps in knowledge and brought questions regarding literature and research that were discussed in meetings.
Although all members of this CoP shared roles, a member of the team always stepped up to guide discussions and generation of ideas during meetings. When people got off track (although the group did not seem to mind) a member (often CoP1P2 or CoP1P3) would pull them back.
At times the meeting got off course…. This got confusing at times as several ideas were being floated around at once – this did not seem to faze the group however, as they continued to engage in conversation as if the change in focus had not occurred (Source: Field Notes).
COP1P18 took the important role of organizing meetings and activities (including assembling academic literature and editing the document), being the liaison between the general (peripheral) membership and core team, and seeking new partnerships to facilitate broader dissemination.
The group members encouraged and supported one another throughout the process. For example, CoP1P1, CoP1P2, and CoP1P3 regularly praised other members for their contributions. CoP1P2 was particularly passionate about the Wayfinding Initiative and expressed her feelings several times during meetings. CoP1P3 made many positive comments about the team in interviews and planning meetings:
She’s brilliant. Oh, everybody is, honestly. We’ve got this librarian goddess who keeps us all on track and we’ve got these inspired passionate people that really enjoy coming together and CoP1P1… we’ve had a number of knowledge brokers, COP1P1 and then COP1P18… and in particular, the last couple of knowledge brokers had dedicated time to our group, and we’ve accomplished a lot by having that kind of dedicated time, our tools look great and we’re always looking forward to our meetings on the third Friday of every month, it’s been a really good ride for this Community of Practice (COP1P3).
…At the conclusion of the meeting, COP1P19 specifically singled out COP1P13 so that praise could be given for her work done with the group. This led COP1P3 to thank COP1P18 for her work, following which COP1P18 acknowledged that the group had been very welcoming. The group was clearly supportive of one another as they moved towards a common goal, and recognized the importance of the role specific members played and the contributions they made to the CoP. (Source: Field Notes).
Theme 2: Fluidity of Team Membership
The fluidity of the CoP membership allowed for flexibility and resilience in its composition; changes in the teams did not seem to affect task roles. Instead, these changes benefited the CoP with expertise and perspectives from multiple members. COP1P3 and COP1P14 capture this fluidity in the following example:
We normally have a wonderful engineer (COP1P10) that participates and he’s been a very, very steady member in our group. Way-finding is not his area of expertise and he opted out…. So we do have people that come in and out of the group (COP1P3).
… the more people who are involved, the more likely we are to find the people we need (COP1P14).
Participants appreciated the flexibility of the CoP, as it allowed for people to come in and out of the group depending on their interest in the topic and their availability. Although this fluidity may have introduced confusion into the group’s work, they mitigated this by developing a structured process (discussed in theme 3) that balanced their flexibility with suitable management controls.
Theme 3: Structured Process
The development of the Wayfinding Guidelines had a structured process. For example, there was a schedule for meetings, although not all members adhered to it, which is be expected in any group. In addition, the Wayfinding Initiative was one of the many initiatives that the CoP had undertaken over time, and the CoP had developed a common template to ensure consistency in the format of the guidelines across all the initiatives.
We have a template for the document…so all of the documents look the same…(COP1P2).
The structured process was also evident in the assignment of tasks. For example, the knowledge broker assigned tasks to each core team member, while a librarian obtained the research articles and assisted the core team in filling the emerging knowledge gaps. Having a librarian on the team to pull together materials from different sources was an important contribution to the initiative.
However, there were no set timelines for the completion of tasks, and there was no clear reason for the flexibility with regard to time schedules. In response to a question about time schedules, COP1P2 and COP1P3 had the following to say:
We don’t really have one. When we’re finished then we are finished and that’s by mutual consent usually…. Usually each time we meet we identify gaps in what we have or whether we’re lacking accreditation and all of that stuff, and so then we carry on until we feel the document is complete (COP1P2).
…probably we could finish it (the task) in about four more visits if we all were diligent and read our articles (COP1P3).
This flexibility in timelines may have been because the CoP members were volunteers who had other commitments in their professional roles and had little room for additional tasks.
Theme 4: Use of Technology
Technology was a key component of the initiative. Web and telephone-based conferencing helped coordinate members of the team. Screen-sharing was an efficient means of making live modifications to the document, and allowed for simultaneous discussions on the process.
…technology… teleconferencing and videoconferencing, that’s certainly been an important aspect of what makes this work (COP1P14).
Some knowledge users could not take time away from their work, and some may not have had the time to read the document containing the recommendations. Webinars were a convenient means of reaching these knowledge users. They attended the webinars during lunch breaks, and participated in two-way communications that took place between the core team and other participants.
I used to do more of that than I do now and that is mostly because of a time factor. I have almost 150 residents on my caseload and I am just flying around like a crazy woman. If I had a half a day a week or something where I could actually sit down and read, that would be great. But that’s another reason why I like these webinars because they – you know, I can sit. I can have my lunch. It is my lunch break that I’m taking but I can just listen and I’m still learning. No, I don’t have a lot of time for reading (COP1P30).
Apart from being useful in the development of the guidelines, webinars were used to disseminate the guidelines to, and get feedback from, stakeholders. In addition to webinars, the AKE Web site was an important resource for the target audience to access the guidelines.
Theme 5: Variety of Knowledge Sources
The aim of the Wayfinding Initiative was to develop best design practice guidelines to assist persons with dementia in finding their way in an LTC home. The initiative drew from both explicit and tacit knowledge. The sources of information for the guidelines were research and best practices (explicit knowledge), and personal and experience-based knowledge (tacit knowledge). Explicit knowledge was in the form of academic literature and documented best practices. Some CoP members had solid research backgrounds and expertise that they contributed to the initiative. COP1P3 was a good example of a member who was a source of explicit knowledge. As an academic working on her doctorate, she came across a lot of literature that she shared with the group. Another member, the knowledge broker, accessed and distributed research information to the CoP members for analysis.
The members also brought in personal and experience-based, or tacit, knowledge. They shared their knowledge on design in the form of ideas and viewpoints based on their lived experiences and professional backgrounds. For example, COP1P2 provided information and examples on design from her work, which supported the information found in the literature, and in one instance, she knew that specific recommendations such as use of cartoons, would not work in the context of the dementia community. Tacit knowledge was often included when no academic or research evidence was available. The inclusion of this experience-based knowledge made the guidelines both useful and practical to the context and to the target audience.
I think wherever we can we try to back up the tacit knowledge with the academic literature…. We rely a lot on people’s tacit knowledge, and in particular, I’ve really benefited myself from COP1P21’s Occupational Therapy (OT) experience and COP1P14’s architecture experience…. They’ve brought a dimension that is very, very necessary for grounding in terms of actual applied knowledge, being out there and working in the field (COP1P3).
Theme 6: Goal to Change People’s Thinking and Practice
One way of achieving the CoP’s goal was by transforming people’s thinking about practice and environmental design in dementia care. The main target of the Wayfinding Guidelines (Wayfinding Toolkit) were the frontline caregivers (nurses, nursing assistants, physiotherapists, occupational therapists, and other allied health professionals) and administrators in LTC. These health care providers and administrators deal with issues of responsive behaviors and wayfinding among LTC residents on a daily basis. The guidelines could also be used to influence development of policy in LTC.
The development of the guidelines was not an end in itself; they needed to be disseminated and promoted to key audiences including health care providers, organizations such as The Alzheimer Society, and importantly, to policy and decision makers. CoP leaders’ intention was for appropriate design changes to be embedded into the health system and into institutional pLolicies. CoP leaders recognized that administration, not the frontline staff, of LTC homes was responsible for making decisions on design. They were also aware that staff needed education on both design issues and change processes. At the system level, policy makers needed to buy in for the recommendations to be entrenched into policy. The CoP used webinars to disseminate and to get feedback on the recommendations. The webinars attracted participants from diverse backgrounds.
The CoP leaders recognized the need to target large LTC homes because these homes had financial and other resources to redesign their facilities. Decision makers in the targeted institutions needed to be shown the link between design changes and practical concerns, such as reducing incidents of responsive behaviours, and financial benefits (e.g., cost reductions). However, the design guidelines were not restricted to LTC homes; they were applicable to other settings.
… it may appear that… [focus] is long-term care homes, but they could be supportive housing, it could be adult day programs, and even worth looking at in the person’s own home and we’re going to start inviting other members of the Alzheimer’s Society for example…(COP1P3)
There was therefore a need for continued engagement with key stakeholders in dementia care to create awareness of the issues, to promote the guidelines, to change policy on design, and ultimately, to change individuals’ and organizations’ knowledge, attitude, and practice regarding design.
Theme 7: Senior Leaders May Be Operating Under Other Constraints
CoP leaders wanted the guidelines to focus on improving the quality of life of persons living with dementia. Participants suggested that frontline providers in particular needed guidelines when dealing with a population whose behaviour could be unpredictable.
Dementia is an incredibly challenging disease to work with, and …. So we need to have the biggest toolkit we possibly can have to try and manage the behaviours and keep things going relatively smooth inside the institutions. And you know to be very respectful of the people who have dementia, to be very supportive of the people who are trying to work frontline with these challenging behaviours (COP1P30).
People with dementia respond in a variety of ways to different interventions. The guidelines (or toolkit) needed to cover many areas relevant to the complexities of dementia care. Frontline staff interacted with, and knew the appropriate care for, people with dementia. COP1P31 reported that it was common practice for practitioners like her to share information and knowledge with others involved in dementia care. However, she also reported that it was not easy to share the same information with, and get buy-in from, managers in the institutions. This could be because managers and administrators sometimes set priorities based on circumstances such as regulatory expectations and financial constraints in their institutions. It was also pointed out that management is usually disconnected from frontline activities, and implementation of Wayfinding Guidelines may not be a priority.
Theme 8: Links to a Broad Network of Interested Stakeholders
This theme is related to the first theme regarding membership composition, the resources membersbring with them, and the functioning of the CoP. The members had linkages and networks with other stakeholders (including other CoPs) and knowledge users outside the immediate group. Although the guidelines focused on LTC home settings, they could be adapted and used in other settings, and therefore the CoP leveraged these connections and networks in the development of the guidelines.
We tend to focus on physical design and it is easiest to look at this in settings such as long term care homes. However, the work may be applicable to other design settings such as supportive housing, adult day programs and personal homes. We are working with people from different agencies, like personal education coordinators, to make [the guidelines] applicable to other settings (COP1P3)
The CoP tapped into the different viewpoints, experiences, and expertise in diverse areas of practice relevant to design. The CoP also obtained feedback from a broader network of existing and potential stakeholders, potentially making the guidelines applicable in diverse settings.
COP1P2 explained that the general membership tends to be our core group. We then asked for clarification, “Do you have a larger group that you seek clarification from, outside of your core group?” COP1P2 stated that they have sought feedback from a group of PRC’s (psychogeriatric consultants) in Ontario. She mentioned having collaborated with the other CoPs a couple of times, presenting the guidelines and receiving feedback. COP1P2 and COP1P3 also talked about surveys they had done in the past to gather feedback from a larger group of people. (Source: Field Notes)
In addition, the expanded networks and connections enabled the CoPs to disseminate and promote use of the guidelines to audiences beyond the immediate knowledge users.
Theme 9: Facilitators of Implementation
The CoP1P had a number of frontline staff members involved with the Wayfinding Initiative. Frontline staff are key knowledge users and their involvement in the initiative provided information and perspectives on LTC issues of which the CoP may not have been aware. Participation of frontline staff was helpful in presenting the guidelines in a language consistent with the language used in LTC settings, and ensured that the recommendations were practical and appropriate for use in that context. A member who was familiar with the context suggested use of appropriate content and illustrations for the document. Moreover, frontline staff (for example, COP1P30, a social worker) promoted the initiative by inviting their colleagues to the webinars, and by sharing the Wayfinding Guidelines with them.
We also have a weekly meeting here with all the nurse managers and both social workers and part of that meeting is to talk about challenges we’re having with different responsive behaviours and that’s when I’m able to share a lot of my knowledge [COP1P30].
Participants reported that LTC homes and hospitals had expressed interest in the guidelines, and that there were plans to translate them into French for wider dissemination and use. It was also reported that frontline staff were enthusiastic about using the guidelines, and some had applied the guidelines in their places of work, albeit on a small scale, and on a trial-and error-basis, as COP1P30 reported:
They [unit staff] don’t really have time to sit and read things. It’s more, you know, talking on the fly and trying to get, you know, let’s try this one intervention today and then I’ll come up tomorrow and see if it helped and if not, we’ll try something else and so it’s just more trial and error… (COP1P30).
Some of the guidelines being put into practice included camouflaging exits by setting up a mural of bookcases over the door to minimize exit-seeking for some of the patients. Another practical application was the use of room identifiers such as pictures in a patient’s room. The patients might not be able to read their names but they could identify the pictures and be able to locate their rooms more easily. Although it was too early to assess the full uptake of these guidelines, COP1P31 (a physiotherapist) provides an example of a positive impact from the use of the guidelines.
It is a little [thing] and certainly the simple ones as far as putting the pictures up outside the rooms has helped me. A lot of our luminescence is taupe on blue so everything is quite similar so I have had a couple of patients say “Where’s my room, oh, I have to go towards the flowers” and then they have been able to find their room which has been great but a very simple, simple change [COP1P31].
This happened with the support of LTC home managers, which included providing staff time for education and providing some resources for the changes.
Theme 10: Challenges to Implementation
Barriers to practical application
Dementia is a complex disease, and people with dementia have particular challenges in terms of behaviour and the type of care they need. The guidelines were required to address specific needs of different residents, and to be aligned with the needs of different organizations so as to be applicable in specific LTC homes. At the local level, frontline staff needed to see the guidelines as an important tool in their work. It was reported that some frontline staff were more reactive than proactive with regard to dementia care. It was also reported that some had negative attitudes towards dementia and that they were not interested in changing the environment for the residents with dementia.
Time constraints prevented frontline staff from passing on knowledge to other colleagues. In addition, consistency was cited as a barrier to the application of the guidelines. Frontline staff worked in shifts, and it was therefore difficult to be consistent in applying the guidelines because of challenges in ensuring continuity.
I would say consistency between front line staff is probably a barrier for us because I can go up and meet with day staff and meet with afternoon staff and really try and say, okay, this is what we’re trying to do and if we could all just be consistent and try to redirect and try to, you know, try all these things that we’re trying, but we really do need to have that consistency so that someone with cognitive issues maybe can catch on if we’re all doing the same thing. It’s very, very, very hard to have that consistency because there’s just so many staff here and it’s, you know, I may meet with two shifts but the next day it’s all new people again [COP1P30].
Lack of financial resources was another barrier to the development and practical application of the guidelines. The CoP did not have enough funds to modify the guidelines for easy reading or to translate them into French for wider reach. According to COP1P31, structural changes to the environment were more desirable, but there was no funding for such changes.
Barriers to system change
Design changes require management support, which was often lacking. Participants said that management might not be in touch with frontline circumstances, and therefore did not see the need for the changes. Even in cases in which design changes were recognized as desirable, changes were inhibited by more immediate demands and conflicting priorities such as the need to meet government-mandated expectations in other areas. Participants also said that managers may be unwilling or unable to support changes because of limited resources or regulatory barriers.
The CoP recognized the need for KTA processes that engaged policy makers, but their access to this group was limited. Policy makers are important in ensuring that the guidelines are entrenched at the system level and implemented across the board. For example, there were no policy makers in a meeting where suggestions were made regarding modifications within the provincial Long-Term Care Act to support design optimization across the province. In addition, although the CoP had a broad range of connections, they had trouble reaching people at management levels. For example, managers did not attend webinars where the guidelines were disseminated and discussed, although they supported attendance by frontline staff. This denied the initiative important input from those who would spearhead implementation.
When I asked her whether management has been supportive in implementing the knowledge into practice, she explained that she has not yet found a way to increase buy-in at this level. “Management are very far removed from what is happening at the frontline,” she said. (Source: Field Note)
The preceding section highlights the themes that emerged through the CoP’s development of wayfinding guidelines. The themes highlight the importance of team dynamics, the development of guidelines and implementation at both the system and practice levels, the use of technology, and the dissemination plans. The work highlights that system transformation and policy change were not arrived at because of a number of constraints, including lack of involvement by policy makers. However, some changes that required minimal resources (more practical changes) were made. Behaviour change was observed in the residents, implying that more changes are possible with resources and organizational support.
The frontline staff seemed highly receptive and ready to implement small, practical design changes within their homes such as putting pictures up outside of the room. However, they are challenged by the competing priorities of the home to save money. (Source: Field Note)
The impact of the guidelines on environmental design changes was not measured in this case study.
Discussion
The purpose of this case study was to gain a deeper understanding of the KTA processes of the CoP1P. We used the case study of CoP1P’s Wayfinding Initiative to examine the processes that were initiated through the CoP, and the interaction of tacit and explicit knowledge in the process. We also examined how the involvement of knowledge users influenced the utilization of knowledge, and finally, the factors that supported or hindered the effectiveness of the KTA process. The themes that emerged revolved around the group or team (the CoP) functioning, the task (the KTA process of developing the Wayfinding Guidelines), the use of technology, and the implementation of the guidelines. The factors that hindered and those that facilitated the KTA process were also identified.
This initiative had the characteristics of CoPs, which include a common interest (a domain), a practice, and a community (Lave & Wenger, Reference Lave and Wenger1991). The focus of the CoP was to collect, synthesize, package, and share knowledge related to environmental design change to improve wayfinding for persons with dementia living in LTC homes and other environments. The CoP members were committed to the effort, and they provided resources in terms of time and knowledge, which were necessary for its success (Wenger & Snyder, Reference Wenger and Snyder2000). Throughout the KTA process, there was commitment to collective learning and the achievement of the CoP goal. The core members of the CoP collaborated well; they had passion, dedication and strong leadership.
By definition, a CoP has members and relationships at different levels (Lave & Wenger, Reference Lave and Wenger1991). Some members are at the core, whereas others are at the periphery; some are committed to the cause, and others are pursuing their own interests (Benne & Sheats, Reference Benne and Sheats2007). The effectiveness of group existence and functioning depends on members’ support for one another, and on a clear, shared reason for coming together (Smith & McKeen, Reference Smith, McKeen and Holsapple2004; Wageman, Hackman, & Lehman, Reference Wageman, Hackman and Lehman2005). The members of the CoP1P were committed to and supportive of one another. They had the common goal of changing people’s beliefs and practices with regard to environmental design. However, membership in the CoP was not static, and there were changes over time for various reasons. Whereas some members left the CoP because the topic was not relevant to them, others joined because they possessed skills and knowledge that they wanted to contribute to the initiative. This is consistent with fluid teams; changes occur in fluid teams because they are structured around interests and roles depending on members’ skills, experiences, and personalities (Bechky, Reference Bechky2006; Huckman & Staats, Reference Huckman and Staats2010). Some authors (Feldman, Reference Feldman1994; Kane, Argote, & Levine, Reference Kane, Argote and Levine2005) argue that fluidity benefits teams by bringing in fresh ideas and perspectives. Other authors (Summers, Humphrey, & Ferris, Reference Summers, Humphrey and Ferris2012) argue that changes disrupt the balance and relationships among team members, and that these changes leave gaps that often take time to fill, therefore affecting the team’s performance. With regard to the CoP1P, the fluidity of its members provided different levels of expertise and experience to the group, and the external networks that the new members brought expanded the CoP’s reach.
The development of the Wayfinding Guidelines followed a structured process based on available best practices (Jacobson, Butterill, & Goering, Reference Jacobson, Butterill and Goering2003; Phillipson, Lowe, Proctor, & Ruto, Reference Phillipson, Lowe, Proctor and Ruto2012). Members took on roles and a core group coordinated the process. In addition, the CoP had developed tools, including a template for use in all the initiatives that the CoP undertook. This is consistent with proper functioning of self-organized groups (Stempfle, Hübner, & Badke-Schaub, Reference Stempfle, Hübner and Badke-Schaub2001). These groups establish certain structures, processes, and tools to guide their work, which include standards to govern procedures, the quality of work, methods of doing things, clarity of roles, guidelines on what needs to be achieved, and the timing of the activities. However, these elements can be changed or modified at any time depending on the stage of the task, the prevailing needs, and the context (Kane et al., Reference Kane, Argote and Levine2005; Summers et al., Reference Summers, Humphrey and Ferris2012). This was evident in the development of the Wayfinding Guidelines, where, for example, the document was said to be “live” in that it could be changed at any time depending on new evidence from research or practice. In another example, the timing of activities could be extended to accommodate the schedule of members.
Our work has highlighted the role of CoPs as knowledge translation mechanisms that link both tacit and explicit knowledge, consistent with the view of Wenger and Snyder (Reference Wenger and Snyder2000) that CoPs are groups of people who share both knowledge and experiences. According to Smith (Reference Smith1997), members’ diverse tacit and explicit knowledge provides a CoP with a variety of knowledge, perspectives, and ways of doing things. Members of the CoP1P used tacit and explicit knowledge to develop the Wayfinding Guidelines. The development of the design guidelines was supported by a variety of knowledge sources including academic literature and experience-based knowledge. They also tapped into their relational and collective tacit knowledge (Collins, Reference Collins2010) to ensure group functioning and cohesion.
Technology is another key resource that can play an important part in CoPs (Hemmasi & Csanda, Reference Hemmasi and Csanda2009). The CoP1P used technology for its internal and external processes to not only collaborate and create the toolkit, but also to facilitate wider dissemination of the recommendations to knowledge users. The CoP’s use of Web and telephone-based communication during their planning meetings provided such a forum, where evidence was shared, discussed, and modified. This collective exchange and interpretation of knowledge through the use of technology helped facilitate the uptake of new knowledge and the collection of a more comprehensive range of information (Mohrman, Gibson, & Mohrman, Reference Mohrman, Gibson and Mohrman2001).
Effective knowledge translation requires not only the ability and skill to navigate the complexities of identifying the problem and the sources of knowledge and synthesizing, disseminating, and promoting use of knowledge; it also requires the ability to address the needs of multiple stakeholders (Graham et al., Reference Graham, Logan, Harrison, Straus, Tetroe and Caswell2006; Ward, House, & Hamer, Reference Ward, House and Hamer2009). Frieden (Reference Frieden2014) suggests involving many stakeholders (including public-and private-sector organizations, the health care community, decision makers, the general public, and the political establishments) to enhance the implementation of health initiatives. This provides more information and different perspectives, and builds private and public support for initiatives. The CoP1P involved researchers, frontline staff, architects, students, and stakeholder organization representatives involved in dementia care in the KTA initiative. The frontline staff were aware of the end-use context and provided information that made the recommendations practical and appropriate for use in LTC homes. The CoP, however, had limited success in involving policy makers and administrators in its KTA process. One reason for their lack of involvement could be that the CoP did not understand the complex environment of policy making and the intricacies of getting policy makers to participate in the KTA process (Lavis, Reference Lavis2006). Additionally, administrators and policy makers linked to long-term care homes are often forced to follow government mandates that may have competing priorities. We note that whereas front-line staff attending webinars on their lunch hours reflects the ability of the CoP to accommodate their educational efforts to their schedules, this may also reflect that administrators do not see these activities as a priority. Future research should investigate how to engage key stakeholders, such as policy makers, in KTA processes to achieve positive policy outcomes (McWilliam, Reference McWilliam1997). The CoP also did not involve residents and family caregivers in the development of the Wayfinding Guidelines. In more recent years, there has been an emphasis on engaging patients, residents, and family caregivers in co-creating health system change including care processes, tools, and resources. At the time that this study took place, engagement of patients, residents, and family caregivers was suggested; however, it was not well known how to do this (McNeil et al., Reference McNeil, Elliott, Huson, Ashbourne, Heckman and Walker2016). Involving patients, residents, and family caregivers takes time: to build relationships, make sure they are well supported to participate in meetings, and ensure they feel meaningfully involved in the process (McNeil et al., Reference McNeil, Elliott, Huson, Ashbourne, Heckman and Walker2016). The involvement of residents and family caregivers in CoPs should be explored in future research initiatives.
Despite the successes of the CoP in synthesizing and disseminating the design recommendations, there were barriers to their utilization. These barriers highlight the need to consider the many factors in the dissemination and use of research knowledge. Many studies (for example Amara, Ouimet, & Landry, Reference Amara, Ouimet and Landry2004; Grimshaw et al., Reference Grimshaw, Thomas, MacLennan, Fraser, Ramsa and Vale2004) show that synthesizing and packaging knowledge may be the easier part in the KTA process, whereas dissemination and the eventual use of the knowledge is more challenging. Bero et al. (Reference Bero, Grilli, Grimshaw, Harvey, Oxman and Thomson1998) examined 18 systematic reviews for evidence of the effectiveness of different strategies used to disseminate and implement research findings. They found that the mode of disseminating knowledge determined how it was received and used. They also discovered that passive dissemination of knowledge was ineffective, and that multiple strategies including interactive educational meetings were more effective in ensuring use of knowledge. The least effective strategies were using educational materials and holding educational meetings. Sudsawad (Reference Sudsawad2007) suggests making decisions earlier in the KTA process regarding the intended users of the knowledge and how the users will use it. However, there is no way to guarantee the effective implementation or use of knowledge even with such early decisions, because of the many factors that affect the implementation process (Al Ghabeesh, Reference Al Ghabeesh2015).
Our findings highlight the fact that CoPs operate in the same environments as other knowledge translators and that they face equivalent challenges. This particular CoP was flexible and adaptive, and used a variety of techniques to make the design recommendations available to knowledge users. However, it was unable to create a mechanism to facilitate change at a policy level.
This project aimed to observe the KTA process. We were not responsible for developing the process in which the Wayfinding Guidelines were created, who was involved, or how the product was disseminated. This case study shares the limitations that arise in this type of qualitative inquiry: subjectivity and reflexivity in collecting and analysing data. However, this limitation was mitigated in a number of ways. First, data were collected using a standard template that was applied to all of the other case studies, to allow for consistency in data collection and later cross-study analysis. Second, the researchers were not active participants; they merely observed the KTA process. Third, more than one researcher analysed the data and a larger team of researchers was involved in verifying and interpreting the findings, thus providing added objectivity to the research. Finally, the final data were collected and analysed in 2013. Although the data may therefore seem dated, we believe that they are still very relevant given the continued recognition of the need for efforts to apply best practices in dementia care in the design of LTC homes (Seetharaman et al., Reference Seetharaman, Chaudhury, Kary, Stewart, Lindsay and Hudson2020).
Conclusion
Overall, many factors were evident in the KTA process for the CoP1P. Consistent with Wenger, the structural elements of a CoP (domain, community, and practice) were in place for successful accomplishment of the CoP’s task. The CoP benefited from the extensive tacit and explicit knowledge of its members, who also had extensive networks and linkages. The diverse and proactive nature of the group allowed for broad perspectives and active dissemination strategies at a practical level. Additionally, technology created a forum to access, interpret, and package knowledge. Deeper understanding of the themes that came out of this CoP case study could be used to build stronger CoPs that are effective at both knowledge synthesis and knowledge application. High level management and policy maker buy-in of the recommended design changes, which was a barrier for this CoP, could be considered more explicitly during the planning stages in an effort to secure earlier involvement and commitment of these decision makers.
Findings from this study can inform future KTA processes of CoPs including how these processes can best be improved and supported in their efforts to improve health system capacity and functioning.
Ethics Approval and Consent to Participate
Ethics clearance for the project was obtained from the Health Sciences Research Ethics Board of Western University (#17879E), the Bruyère Continuing Care Research Ethics Committee (#M16-11-004), the Concordia University Human Research Ethics Committee (#HU2010-115), and the University of Waterloo Office of Research Ethics (ORE#16894).
Consent to Publish
Participants consented to having information shared as per the ethics consent process indicated previously. Signed consent forms have been obtained.
Availability of Data and Materials
Data are not publicly available, as our ethics clearance did not allow for this.
Acknowledgments
We thank Heather Drouin and Sospeter Gatobu for their assistance in the preparation of this manuscript. We also acknowledge the help and support of the leaders of the Seniors Health Knowledge Network and the Alzheimer Knowledge Exchange, who helped us find an appropriate site for this investigation. Finally, we thank the participants of the CoP1P who shared their work and insights as the basis of this case study.
Author Contributions
J.E. analysed the data and drafted the manuscript. K.M. collected data and assisted with analysis. P.S., J.C., and A.K. conceived of the study, reviewed findings, and edited manuscript drafts. All authors have approved the final draft of this manuscript.
Funding
The “Knowledge-to-Action Processes in SHRTN Collaborative Communities of Practice” research program was supported by a grant from the Canadian Institutes of Health Research (FRN#106696). A.K. was partially supported by a CIHR New Investigator Award.



