



Externalizing behavior problems, including oppositionality, hyperactivity and impulsivity, emotion dysregulation, conduct problems, and aggression, are among the most prevalent forms of psychopathology exhibited by children (Costello et al., Reference Costello, Mustillo, Erkanli, Keeler and Angold2003). Such behavior problems are particularly important to assess and treat early because their emergence early in life is strongly associated with a multitude of maladaptive consequences across several domains of functioning later in life (Beauchaine et al., Reference Beauchaine, Shader, Hinshaw, Beauchaine and Hinshaw2016). For example, young children who exhibit externalizing behavior problems are more likely to experience signficant challenges as they get older, including academic struggles, delinquency, antisocial behavior, and involvement in the criminal justice system, as well as greater levels of family dysfunction, interpersonal and work environment problems, and increased risk for comorbid psychopathology, such as depression, anxiety, and self-harm (Hechtman et al., Reference Hechtman, Swanson, Sibley, Stehli, Owens, Mitchell, Arnold, Molina, Hinshaw, Jensen, Abikoff, Perez Algorta, Howard, Hoza, Etcovitch, Houssais, Lakes, Nichols, Vitiello, Severe, Jensen, Arnold, Hoagwood, Richters, Vereen, Hinshaw, Elliott, Wells, Epstein, Murray, Conners, March, Swanson, Wigal, Cantwell, Abikoff, Hechtman, Greenhill, Newcorn, Molina, Hoza, Pelham, Gibbons, Marcus, Hur, Kraemer, Hanley and Stern2016; Odgers et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington, Poulton, Sears, Thomson and Moffitt2007; Pinderhughes et al., Reference Pinderhughes, Dodge and Greenberg2005; Sourander et al., Reference Sourander, Jensen, Davies, Niemelä, Elonheimo, Ristkari, Helenius, Sillanmäki, Piha, Kumpulainen, Tamminen, Moilanen and Almqvist2007).
Parenting behavior is a key factor that influences the development of children’s self-regulation skills and can mitigate or exacerbate the manifestation of early externalizing psychopathology (Davies & Cicchetti, Reference Davies and Cicchetti2004; Dodge & Pettit, Reference Dodge and Pettit2003; Kiff et al., Reference Kiff, Lengua and Zalewski2011; Klein et al., Reference Klein, Lengua, Thompson, Moran, Ruberry, Kiff and Zalewski2018; Lengua et al., Reference Lengua, Honorado and Bush2007; Pardini et al., Reference Pardini, Fite and Burke2008). Parents and caregivers play a key role in child development, as children learn from and respond to parental and caregiver behaviors (Calkins et al., Reference Calkins, Propper and Mills-Koonce2013; Cummings et al., Reference Cummings, Davies and Campbell2002). The impact of parenting is particularly strong during early childhood, before the school environment and peers become powerful influences (Dora & Baydar, Reference Dora and Baydar2020; Patterson, Reference Patterson, Reid, Patterson and Snyder2002). Just as parenting behaviors influence early childhood development, young children’s behaviors also influence parents and caregivers. Indeed, a longstanding body of research in developmental psychopathology has considered the transactional nature of the parent-child relationship, referring to the bidirectional, interdependent effects between between parenting behaviors and children’s behavior problems (Cicchetti, Reference Cicchetti1993; Eisenberg et al., Reference Eisenberg, Taylor, Widaman and Spinrad2015; Pettit & Arsiwalla, Reference Pettit and Arsiwalla2008; Sameroff, Reference Sameroff and Sameroff2009; Serbin et al., Reference Serbin, Kingdon, Ruttle and Stack2015).
Few studies have examined this bidirectional relationship across early childhood when problems typically first emerge and intervention might be most potent; even fewer use large, longitudinal samples with repeated measures for both parenting and child behaviors. In addition, prior examinations often do not consider the role of other important, time-varying family factors that can affect this bidirectional relationship (for example, parental stress and psychopathology, social support, family conflict), which obscures the full picture of the multi-system influences on the changing parent-child relationship (Campbell et al., Reference Campbell, Shaw and Gilliom2000; Carneiro et al., Reference Carneiro, Dias and Soares2016; Deater-Deckard et al., Reference Deater-Deckard, Dodge, Bates and Pettit1998; Shaw et al., Reference Shaw, Owens, Giovannelli and Winslow2001). The main aim of the present study was to leverage a large, well-characterized, sociodemographically diverse prospective pregnancy cohort to examine the bidirectional nature of parenting behaviors and child externalizing behavior problems during early childhood – a key period for the development of later psychopathology– using a robust, repeated-measures model that also considered the potential role of family risk factors.
The importance of bidirectional processes in parenting and child externalizing behavior
The relations between parenting behaviors and child externalizing behaviors are complex and change over time. Patterson’s coercion theory highlights how child externalizing behavior, combined with ineffective parenting behaviors (i.e., increasingly harsh, threatening, and coercive behaviors), mutually reinforce each other and can set the stage for later, more serious behavioral problems, such as aggression, delinquency, substance use, and criminality (Besemer et al., Reference Besemer, Ahmad, Hinshaw and Farrington2017; Loeber & Stouthamer-Loeber, Reference Loeber and Stouthamer-Loeber1998; Patterson, Reference Patterson1982, Reference Patterson, Reid, Patterson and Snyder2002). Using longitudinal, repeated measures designs, studies have provided evidence that both “parent-driven” processes (where parenting behaviors have an impact on child behavior) as well as “child-driven” processes (where the opposite occurs) are likely at play and are mutually influential (Lansford et al., Reference Lansford, Criss, Laird, Shaw, Pettit, Bates and Dodge2011; Pardini et al., Reference Pardini, Fite and Burke2008; Yan et al., Reference Yan, Ansari and Peng2021). However, most of the extant research has focused on parent-driven processes. For example, numerous studies have documented that a range of parenting behaviors – both “positive” and “negative” aspects of parenting – are predictive of child externalizing behaviors. Among these parent-driven processes, positive aspects of parenting, such as warmth, responsiveness, monitoring, and sensitivity have all been associated with reductions in child externalizing behaviors (Harvey & Metcalfe, Reference Harvey and Metcalfe2012; Merz et al., Reference Merz, Landry, Montroy and Williams2017; Pearl et al., Reference Pearl, French, Dumas, Moreland and Prinz2014; Pinquart, Reference Pinquart2017; Willoughby & Hamza, Reference Willoughby and Hamza2011), suggesting the importance of focusing on those domains in externalizing research. Notably, these studies have primarily focused on later childhood and adolescence, with fewer studies examining early childhood, limiting our understanding of the early origins of these reciprocal relations.
Child-driven processes have received less empirical attention, but evaluations generally find that children’s externalizing behaviors predict decreases in positive parenting behaviors and increases in negative parenting behaviors (Dieleman et al., Reference Dieleman, De Pauw, Soenens, Beyers and Prinzie2017; Lansford et al., Reference Lansford, Criss, Laird, Shaw, Pettit, Bates and Dodge2011; Serbin et al., Reference Serbin, Kingdon, Ruttle and Stack2015). Few studies examining these reciprocal transactional relations have done so during early childhood using large, mixed-sex samples and prior work has often been limited to studies with only two time points of data (Paschall & Mastergeorge, Reference Paschall and Mastergeorge2016). Of related studies that focus on very young children, there is evidence for the bidirectional associations between parenting behavior and early temperament (see, e.g., Klein et al., Reference Klein, Lengua, Thompson, Moran, Ruberry, Kiff and Zalewski2018; Krieger & Stringaris, Reference Krieger, Stringaris, Beauchaine and Hinshaw2016; Lengua & Kovacs, Reference Lengua and Kovacs2005; Wittig & Rodriguez, Reference Wittig and Rodriguez2019). Although temperatment is distinct from psychopathology, such empirical research suggest that reciprocal relations between parenting and child behaviors begin very early (Mesman et al., Reference Mesman, Stoel, Bakermans-Kranenburg, Van Ijzendoorn, Juffer, Koot and Alink2009; Muris & Ollendick, Reference Muris and Ollendick2005; Smith & Day, Reference Smith and Day2018). We also know little about how these processes (either parent-driven or child-driven) might change across early childhood – which could inform intervention strategies by identifying optimal windows for intervening to either sustain positive or redirect problematic pathways.
Another important benefit of utilizing such bidirectional repeated-measure, longitudinal designs is that they can advance insights into the complexities of emerging psychopathology by partially accounting for the stability of individual factors over time. This is accomplished by assessing changes in behavior over time while holding effects of initial levels of parenting and child behavior constant (Beauchaine et al., Reference Beauchaine, Shader, Hinshaw, Beauchaine and Hinshaw2016). Importantly, most studies have been conducted with predominantly White or middle-to-upper income samples, with less representation from sociodemographically diverse populations (see, however, Pearl et al., Reference Pearl, French, Dumas, Moreland and Prinz2014). These relationships are important to explore across samples with greater diversity, to improve representation in research, ensure generalizability of findings across populations, and reduce biases in healthcare and healthcare decision making that contribute to health disparities (e.g., across race/ethnicity and socioeconomic position; Dovidio & Fiske, Reference Dovidio and Fiske2012; Fitzgerald & Hurst, Reference Fitzgerald and Hurst2017; Pedersen et al., Reference Pedersen, Lindstrom, Powe, Louie and Escobar-Viera2022; Roberts et al., Reference Roberts, Bareket-Shavit, Dollins, Goldie and Mortenson2020). In particular, this can disproportionately impact youth of color with regard to diagnoses for externalizing disorders (Fadus et al., Reference Fadus, Ginsburg, Sobowale, Halliday-Boykins, Bryant, Gray and Squeglia2020).
Measuring parenting in transactional parent-child research
There is a robust, informative literature examining the transactional nature of parenting behaviors and externalizing behaviors in middle-late childhood and adolescence. Most of these studies share two noteworthy limitations regarding the operationalization of parenting. First, few studies utilize comprehensive, multi-faceted measures of parenting behaviors or include aspects of parenting that might be particularly salient for younger children – such as scaffolding and responsive behaviors. These behaviors – showing warmth, empathy and support, establishing structure, and importantly, providing encouragement (such as when faced with a novel/challenging task) – are especially important to assess with young children, as these developing self-regulation skills are important for later executive functioning and behavioral outcomes (Blair & Diamond, Reference Blair and Diamond2008; Bornstein et al., Reference Bornstein, Putnick and Suwalsky2018; Morawska et al., Reference Morawska, Dittman and Rusby2019; Sulik, Reference Sulik2017). Many bidirectional parent-child studies are also limited by utilizing only one or two aspects of parenting, focus on specific subscales within a given parenting measure, or instead focus on negative aspects of parenting (see, e.g., Ciciolla et al., Reference Ciciolla, Gerstein and Crnic2014; Dora & Baydar, Reference Dora and Baydar2020; Harris et al., Reference Harris, Vazsonyi and Bolland2017; Lewis et al., Reference Lewis, Collishaw, Thapar and Harold2014; Taraban et al., Reference Taraban, Shaw, Leve, Natsuaki, Ganiban, Reiss and Neiderhiser2019; Wang & Liu, Reference Wang and Liu2018). Given that many aspects of parenting behavior influence child behavior over time, this focus on specific aspects of parenting limits capture of the broad dynamics of the parent-child relationship and, might miss key aspects of parenting that are especially important for young children.
A second limitation in extant bidirectional studies regarding measures of parenting behavior relates to informants. Very few studies examining the bidirectional nature of parenting and child externalizing behavior utilize observational measures of parenting, most often relying on self-reported instruments, which are subject to potential informant biases and do not correlate strongly with observational data (Hendriks et al., Reference Hendriks, Van der Giessen, Stams and Overbeek2018; Korelitz & Garber, Reference Korelitz and Garber2016; Morsbach & Prinz, Reference Morsbach and Prinz2006). The utilization of more objective measures of parenting behavior, including direct observation and coding of parenting behaviors in the laboratory or in the home environment, is often considered the “gold standard” for assessing parenting behavior and can minimize potential biases regarding parent self-reports, (see Ciciolla et al., Reference Ciciolla, Gerstein and Crnic2014; Coe et al., Reference Coe, Davies, Hentges and Sturge-Apple2020; Merz et al., Reference Merz, Landry, Montroy and Williams2017).
Additional factors affecting parenting and child externalizing behavior
Other factors within the family environment – particularly parental psychopathology and parenting stress – are rarely accounted for when examining the transactional nature of parenting behaviors and child externalizing behaviors (Bayer et al., Reference Bayer, Hiscock, Ukoumunne, Price and Wake2008; Coe et al., Reference Coe, Davies, Hentges and Sturge-Apple2020; Dix & Meunier, Reference Dix and Meunier2009; Dora & Baydar, Reference Dora and Baydar2020; Schleider et al., Reference Schleider, Patel, Krumholz, Chorpita and Weisz2015; Taraban et al., Reference Taraban, Shaw, Leve, Natsuaki, Ganiban, Reiss and Neiderhiser2019). A large body of literature shows that maternal mental health (such as depression or anxiety), as well as parenting-related stress, are associated with offspring psychopathology, including child externalizing problems (Ashman et al., Reference Ashman, Dawson and Panagiotides2008; Goodman et al., Reference Goodman, Rouse, Connell, Broth, Hall and Heyward2011; Roubinov et al., Reference Roubinov, Epel, Adler, Laraia and Bush2022; Taraban et al., Reference Taraban, Shaw, Leve, Natsuaki, Ganiban, Reiss and Neiderhiser2019; Yan et al., Reference Yan, Ansari and Peng2021). Parental psychopathology has been associated with negative parenting behaviors, such as negativity and ineffective discipline practicies (Berg-Nielsen et al., Reference Berg-Nielsen, Vikan and Dahl2002), which in turn is associated with child behavior problems. Parenting stress has also been associated with parenting behavior and child behavior problems (Abidin, Reference Abidin1992; Crnic et al., Reference Crnic, Gaze and Hoffman2005). For example, Williford et al. (Reference Williford, Calkins and Keane2007) found that both parental psychopathology and child emotion dysregulation, among other factors, were longitudinally associated with parenting stress, and stability of parenting stress was predicted by child externalizing problems. Although some studies account for such factors in their models, this is most often as a covariate, mediator, or moderator at a single point in time, without accounting for how these factors change over time. Very few studies have accounted for these dynamic factors in longitudinal models utilizing a repeated-measure design (for an exception, see Wei et al., Reference Wei, Eisenberg, Ramos-Olazagasti, Wall, Chen, Bird and Duarte2017). The exclusion of these factors from bidirectional parenting-child externalizing studies overlooks the possibility that such factors may contribute to either parenting behaviors or child behaviors across time and their omission might bias the estimated effects of parenting behaviors on child behavior, or vice versa (Barroso et al., Reference Barroso, Mendez, Graziano and Bagner2018; Yan et al., Reference Yan, Ansari and Peng2021).
The present study
In the present study, our primary aim was to employ a repeated measures, longitudinal design to examine the transactional nature of parenting behavior and child externalizing symptoms in a large, well-characterized, socioeconomically diverse, predominantly Black sample of mothers and their offspring across early childhood (ages 1–6). To advance the rigor of evidence in this domain, we utilized a high-quality, observed measure of overall parenting quality that included aspects of parenting that are particularly relevant for younger children (i.e., scaffolding activities that support a young child’s socioemotional and cognitive growth – such as teaching them a new skill). Additionally, we incorporated repeated measures of two important maternal psychosocial factors (i.e., parenting stress and psychopathology) known to be associated with both parenting behaviors as well as child externalizing psychopathology into our longitudinal design. Finally, given the mixed findings regarding sex differences for these associations during childhood, and a particular lack of evidence for very young children (Rothbaum & Weisz, Reference Rothbaum and Weisz1994; Yan et al., Reference Yan, Ansari and Peng2021), we explored whether the developmental associations within this transactional model varied by child sex within this large community sample. Based on prior research, we predicted: (Hypothesis 1) that higher levels of developmentally-appropriate measures of parenting quality would be longitudinally associated with lower levels of child externalizing behaviors at an early age, and higher levels of child externalizing behaviors would subsequently be associated with lower levels of parenting quality; and (Hypothesis 2) these associations would be maintained even after accounting for other maternal psychosocial risk factors over time. Regarding potential moderation by child sex (Hypothesis 3), given the mixed findings to date and limited evidence in mixed-sex samples of young children, we made no specific prediction regarding whether these longitudinal associations would differ by child sex.
Method
Participants and procedure
The present study used data from the Conditions Affecting Neurocognitive Development and Learning in Early Childhood (CANDLE) study (Sontag-Padilla et al., Reference Sontag-Padilla, Burns, Shih, Griffin, Martin, Chandra and Tylavsky2015), part of the ECHO PATHWAYS consortium (Lewinn et al., Reference LeWinn, Karr, Hazlehurst, Carroll, Loftus, Nguyen, Barrett, Swan, Szpiro, Paquette, Moore, Spalt, Younglove, Sullivan, Colburn, Byington, Sims Taylor, Moe, Wang, Cordeiro, Mattias, Powell, Johnson, Norona-Zhou, Mason, Bush and Sathyanarayana2022). CANDLE is a longitudinal pregnancy cohort study that was designed to assess the pre- and postnatal factors that impact neurocognitive development using a robust, longitudinal design. The study enrolled 1503 pregnant women within the greater Memphis, Tennessee area between 2006 and 2011. Women were enrolled in their second trimester, were between ages 16 and 40, did not have chronic preexisting conditions that required medication, and were considered low-risk pregnancies. See Table 1 for participant demographic information. The sample was racially (64% self-identified as Black, 31% as White, 5% as Mixed Race or Other) and socioeconomically diverse, although more than half of families were considered lower-income (median family-size-adjusted annual household income of $15,151; 59% reported being on federal or state-supplemented health insurance and almost 41% had private/employer health insurance). Approximately 2% of participants self-identified as Hispanic/Latino. Participants were fairly representative, based on US census bureau statistics, of the greater Memphis metropolitan area in terms of race, education, income, and health insurance status (Sontag-Padilla et al., Reference Sontag-Padilla, Burns, Shih, Griffin, Martin, Chandra and Tylavsky2015). The study was approved by the Institutional Review Board at the University of Tennessee Health Science Center.
Table 1. Demographic information and model variables (N = 1287)

Baseline data were collected at study enrollment during pregnancy. Perinatal data were additionally collected during a third trimester visit and then again at childbirth. Following childbirth, families were followed prospectively, with data collected at four clinic visits occurring at approximately child ages one-year (Wave 1; N = 1106), two-years (Wave 2; N = 1074), three-years (Wave 3; N = 1023), and four-to-six years (Wave 4; N = 1099). Families were compensated for their time after each assessment they completed. The following information was obtained during clinic visits: demographic information, mother-reports of both mother and child psychosocial functioning (maternal psychopathology, parenting stress, child externalizing behavior), and clinical observations of parent-child interactions. The analytic sample (N = 1287) comprised all mother-child dyads for which there was at least one measure of child behavior and one measure of parent-child interactions across the four in-person follow-up visits (Waves 1–4). Approximately 8% of the sample contributed only one timepoint of parent-child data; most dyads (92%) contributed two or more waves of parent-child data. For the postnatally-retained sample, mothers tended to be older at study enrollment (M age = 26.3 years vs. 24.2 years, t = 3.94, p < .001), and had slightly higher adjusted household incomes (M = $20.4k years vs. $16.4k, t = 2.33, p = .011) compared to mothers who were lost to attrition, but otherwise did not significantly differ on study variables.
Measures
Repeated measures
Three constructs were utilized for the cross-lagged panel model design: parenting quality (Waves 1–3), child externalizing behaviors (Waves 1–4), and a maternal risk composite (Waves 1–4).
Parenting quality
Parenting behavior was assessed during clinic visits at Waves 1–3 using the Nursing Child Assessment Satellite Training Parent-Child Interaction Teaching Scale (NCAST; Huber, Reference Huber1991; Oxford & Findlay, Reference Oxford and Findlay2013). The NCAST comprises 73 items, each endorsed yes/no, and was completed by study staff (psychologists or psychology interns) who received rigorous training in the NCAST coding system. All examiners maintained 85% interrater reliability during the initial training and all subsequent training that occurred every six months during the data collection period. During this task, the examiner asked the mother to review a list of possible activities and select one that her child had not yet mastered. The mother then teaches her child the activity while the examiner observes, which can place some stress on the parent-child interaction, thus allowing observation of adaptive patterns of behavior between mother and child outside of their usual interactive routines (Graff et al., Reference Graff, Bush, Palmer, Murphy, Whitaker and Tylavsky2017). The NCAST was completed by a single, trained, examiner immediately after observing the mother-child interaction for approximately five minutes. We use the term “parenting quality” moving forward to capture the overall measure of parenting behavior, which was assessed using the Total Caregiver score (with higher scores indicating more positive responses from the parent). This score consists of 50 items that comprise the following four subscales that assess a range of social, nurturant, and didactic caregiving behaviors: (1) sensitivity to cues (e.g., “caregiver gives instruction only when child is attentive” and “caregiver praises child’s success or partial successes”), (2) response to child’s distress (e.g., “caregiver makes positive, sympathetic, or soothing verbalization” and “caregiver avoids making negative comments to the child”), (3) social-emotional growth-fostering (e.g., “caregiver laughs or smiles at child during the teaching interaction” and “caregiver makes cheerleading style statements to the child during the teaching interaction”), and (4) cognitive growth-fostering (e.g., “caregiver focuses attention and child’s attention on the task during most of the teaching (60% of the time)” and “caregiver uses both verbal description and modeling simultaneously in teaching any part of the task”). The NCAST has been used with diverse populations and has been associated with infant cognitive and socioemotional development (Britton et al., Reference Britton, Gronwaldt and Britton2001; Letourneau et al., Reference Letourneau, Tryphonopoulos, Novick, Hart, Giesbrecht and Oxford2018; Lugo-Gil & Tamis-LeMonda, Reference Lugo-Gil and Tamis-LeMonda2008; Page et al., Reference Page, Wilhelm, Gamble and Card2010; Ransone et al., Reference Ransone, Graff, Bush, Oxford and Wicks2018). This measure has shown good internal consistency and test-retest reliability; Cronbach’s alpha for the present sample was also good (α = .83; Graff et al., Reference Graff, Bush, Palmer, Murphy, Whitaker and Tylavsky2017).
Child externalizing behaviors
Two measures were used to assess child externalizing behaviors across Waves 1–4, based on what was appropriate for their age and developmental stage (see also Roubinov et al., Reference Roubinov, Browne, LeWinn, Lisha, Mason and Bush2022 for a previous example). At Waves 1 and 2, mothers reported on their child’s externalizing symptoms via the Brief Infant Toddler Social Emotional Assessment (BITSEA; Briggs-Gowan et al., Reference Briggs-Gowan, Carter, Irwin, Wachtel and Cicchetti2004). This measure has demonstrated good test-retest reliability and interrater agreement between parents, as well as good criterion and predictive validity to the Child Behavior Checklist CBCL (Briggs-Gowan et al., Reference Briggs-Gowan, Carter, Irwin, Wachtel and Cicchetti2004, Reference Briggs-Gowan, Carter, McCarthy, Augustyn, Caronna and Clark2013). We utilized the externalizing subscale, which consists of six items measured on a 3-point scale (“not really true/rarely,” somewhat true/sometimes,” and “very true/often”). Example items include: “is restless and can't sit still,” “often gets very upset,” and “hits, bites, or kicks you (and other parent).” At Waves 3 and 4, mothers reported on their child’s externalizing symptoms using the externalizing subscale from the CBCL/1.5–5 (Achenbach & Rescorla, Reference Achenbach and Rescorla2000). The CBCL evaluates some of the same externalizing behaviors as the BITSEA (e.g., “hits others”) and also includes other developmentally-appropriate items for children aged 3–5. The CBCL is widely used and has strong psychometric properties, including reliability and validity (Achenbach & Rescorla, Reference Achenbach and Rescorla2000).
Maternal risk composite
Following an approach similar to Wei et al. (Reference Wei, Eisenberg, Ramos-Olazagasti, Wall, Chen, Bird and Duarte2017), maternal risk was assessed at all four study timepoints (Waves 1–4) using a composite of two measures. Maternal self-reported psychopathology symptoms were measured by the Global Severity Index from the Brief Symptom Inventory (BSI; Derogatis, Reference Derogatis1983; Urbán et al., Reference Urbán, Kun, Farkas, Paksi, Kökönyei, Unoka, Felvinczi, Oláh and Demetrovics2014). The BSI is a widely used measure of overall psychiatric symptoms that is based on the longer Symptom Checklist-90. Parenting stress was measured by the total score from the Parenting Stress Index – Short Form version (PSI; Abidin, Reference Abidin1990). A maternal risk composite was utilized for analytic purposes to reduce the complexity of the cross-lagged panel model (correlations between the BSI and PSI across Waves 1–4 ranged from .48 to .53; all p’s < .001; refer to Supplemental Figure 1). Both measures were standardized at each time point, then averaged to create the composite, with higher scores indicating more risk (i.e., higher psychopathology and parenting stress) and lower scores indicating less risk.
Covariates
All models included the following covariates: maternal age at study enrollment and marital status at time of child’s birth; household income adjusted for family size; and child gestational age at birth and sex.
Analytic plan
All analyses were performed in MPLUS version 8. Bivariate correlations evaluated the associations among all study variables. To test Hypotheses 1-3, the current study used cross-lagged panel model (CLPM) analyses to examine the between-family differences for the associations among maternal parenting quality, child externalizing behaviors, and the maternal risk composite across Waves 1–4 (see Figure 1).Footnote 1 CLPM simultaneously examines both autoregressive paths within variables as well as cross-lagged paths between two different variables (Selig & Little, Reference Selig, Little, Laursen, Little and Card2012). The autoregressive paths estimate directional associations within a variable across time (i.e., stability; e.g., child externalizing from Wave 1 to Wave 2). The cross-lagged paths then estimate the direction of influence of one variable on subsequent changes in the other variables (e.g., parenting practices at Wave 1 to child externalizing at Wave 2, controlling for child externalizing at Wave 1). We also included paths from the maternal risk composite to child externalizing behaviors and t-2 autocorrelations among the residuals of the maternal parenting and, separately, the child externalizing measures to account for the high stability in our repeated measures. Our analyses utilized 3 main models, with each subsequent model built on the prior model. For Model 1, model fit evaluations examined all directional paths between parenting and child behavior (see Figure 2). Model 2 builds on Model 1 by adding the maternal risk composite into the model to predict parenting and child externalizing behavior – both concurrently and at the subsequent wave (see Figure 3). To determine the best-fitting model, we utilized the root mean squared error of the approximation (RMSEA) with 90% confidence intervals, comparative fit index (CFI), Tucker-Lewis index (TLI), and chi-square with degrees of freedom and p-value (Hu & Bentler, Reference Hu and Bentler1999; Xia & Yang, Reference Xia and Yang2019). The covariates – maternal age, marital status, adjusted household income, gestational age, as well as child sex – were included as correlated exogenous variables at Wave 1, with the exception of child age at Wave 4, which was included as a correlated exogenous variable at Wave 4. This method was used in all adjusted models. Prior to model estimation, all externalizing scores were standardized for comparability (BITSEA at Waves 1 and 2, and CBCL at Waves 3 and 4). Missing data was handled using maximum likelihood estimation with robust standard errors (MLR).
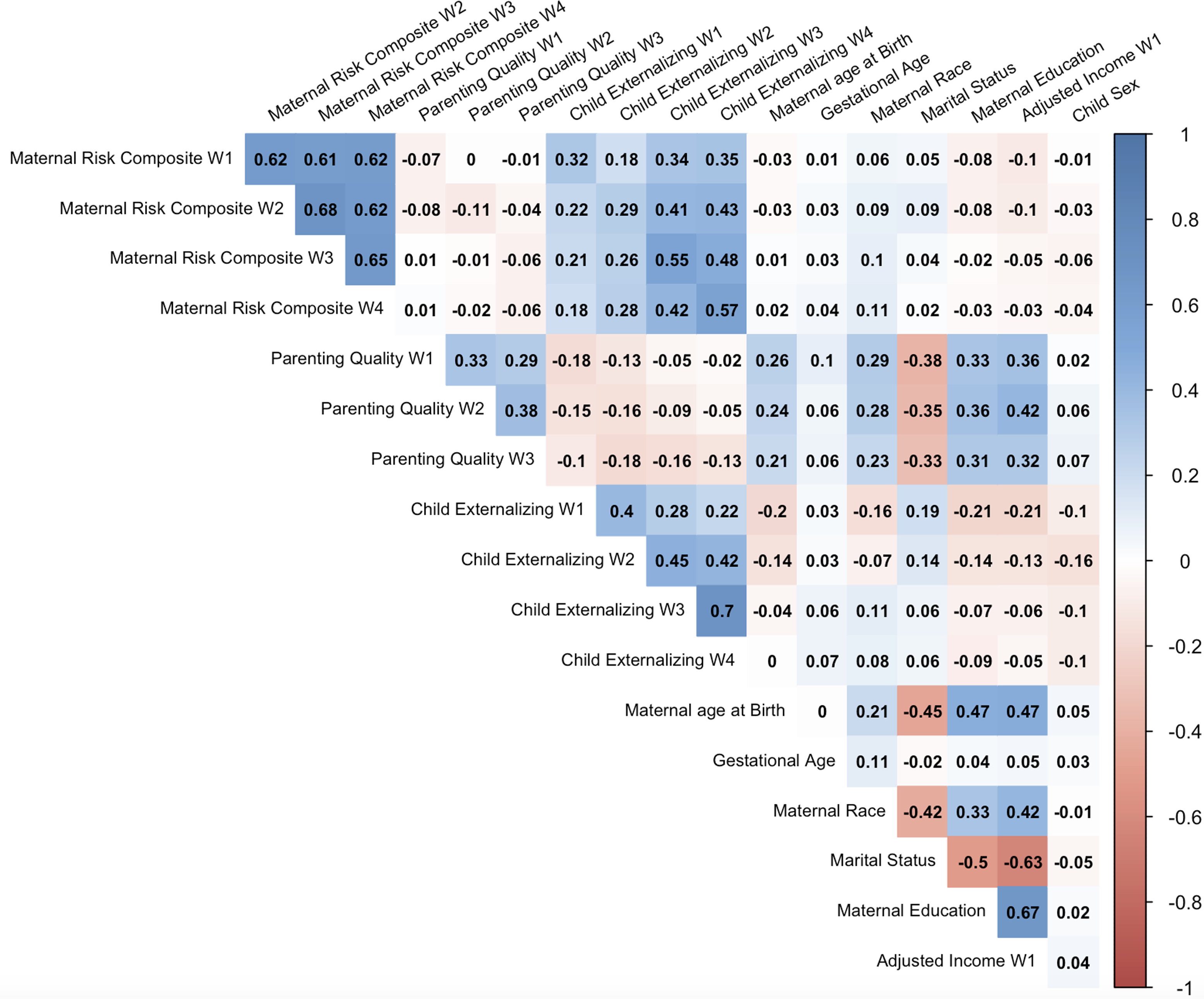
Figure 1. Bivariate correlations among all study variables.
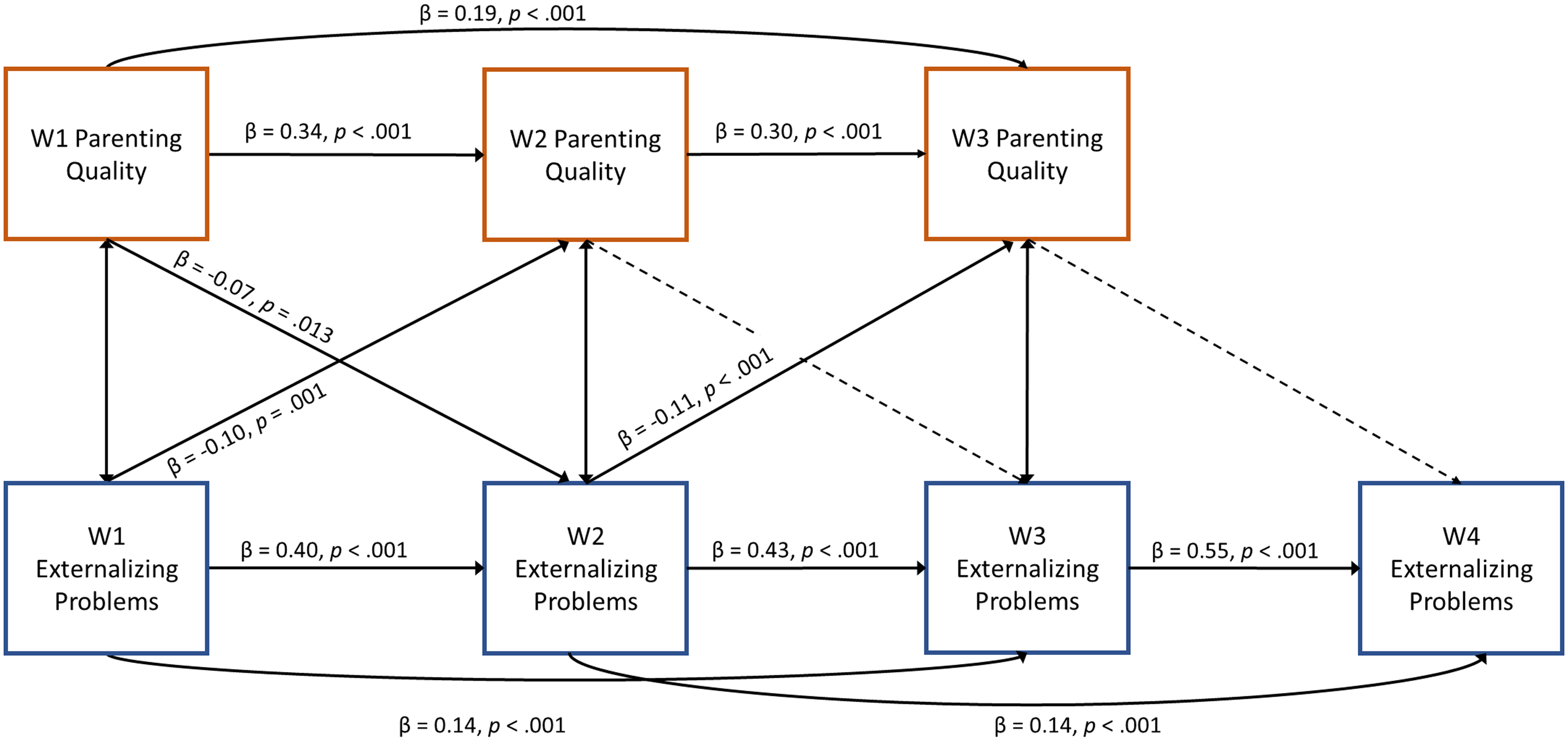
Figure 2. Evaluation of transactions between observed parenting quality and child externalizing problems (Model 1). All cross-sectional paths between parenting quality and child externalizing problems were negative and significant (p’s ranged from < .001 to .014). Model covariates included: adjusted household income, maternal age, marital status, gestational age, child sex, and child age.

Figure 3. Evaluation of transactions between observed parenting quality, maternal risk, and child externalizing problems (Model 2).All cross-sectional paths between parenting quality and child externalizing problems were negative and significant (p’s ranged from .004 to .029). Model covariates included: adjusted household income, maternal age, marital status, gestational age, child sex, and child age.
To test Hypothesis 3 (Model 3) – we build on Model 2 by examining child sex as a moderator of the associations between parenting quality and child externalizing behaviors across time by evaluating multigroup comparisons within the best-fitting transactional model. First, we constrained all bidirectional paths to be equivalent across males and females (fully constrained model). Next, we allowed all bidirectional paths to be estimated freely across males and females (fully unconstrained model). Chi-squared difference tests compared the fit of these two models to determine if allowing the paths to vary among child sex would result in better model fit (i.e., support examining moderation by child sex).
Results
The analytic sample included 1,287 mother-child dyads who had at least one measurement of observed parenting and one measure of child externalizing behavior. Full sample demographics are presented in Table 1. Bivariate correlations are presented in Figure 1. Coded parenting quality demonstrated appropriate levels of variability in the total caregiver score across the sample and was moderately and positively correlated across time (r’s = 0.29–0.38). Child externalizing symptomatology was also positively correlated across time, though the strength of the association varied (r’s = 0.22–0.70) with weaker associations for the most distant assessments (i.e., between Wave 1 and Wave 4). There were also small negative correlations between parenting and child externalizing across time (r’s = −0.02 – −0.18).
Transactions between parenting and child externalizing behaviors
Fit indices identified a good fitting model for Model 1 (χ 2 (70) = 1846.9, p = 0.00, RMSEA = 0.062 [90% CI = 0.055, 0.069], CFI = 0.873, TLI = 0.826, SRMR = 0.077; see Figure 2). Autoregressive paths for observed parenting were significant across age 1–2 (β = 0.34, SE = 0.03, p < 0.001) and age 2–age 3 (β = 0.30, SE = 0.03, p < 0.001). Similarly, autoregressive paths for child externalizing were also significant from age 1–2 (β = 0.40, SE = 0.03, p < 0.001), age 2–age 3 (β = 0.43, SE = 0.03, p < 0.001) and age 3–age 4–6 (β = 0.55, SE = 0.03, p < 0.001). Evaluating Hypothesis 1, evidence of transactional associations between observed parenting and child externalizing behaviors emerged at three timepoints. First, higher observed parenting quality at 1-year predicted decreased child externalizing behaviors at 2-years (β = −0.07, SE = 0.03, p = 0.013). Additionally, higher child externalizing behaviors at 1-year predicted lower observed parenting quality at 2-years (β = −0.010, SE = 0.03, p = 0.001). Subsequently, higher child externalizing behaviors at 2-years predicted decreased observed parenting quality scores at 3-years (β = −0.11, SE = 0.03, p < 0.001). The maternal-directed paths from parenting at ages 2-years and 3-years were not statistically significant.
Maternal risk in the transactions between parenting and child externalizing behaviors
Next, for Model 2 we included the directional paths from the maternal risk composite variable predicting concurrent parenting quality as well as concurrent and future child externalizing behaviors to examine Hypothesis 2 (see Figure 3). Fit indices identified a good fitting model and improved model fit over Model 1 (χ 2 (115) = 4564.67, p = 0.00, RMSEA = 0.054 [90% CI = 0.049, 0.060], CFI = 0.926, TLI = 0.899, SRMR = 0.058). Like Model 1, autoregressive paths for both observed parenting quality and child externalizing behaviors were significant (all ps < 0.001) and identified stability across time for both constructs. The transactional associations between parenting and child externalizing behaviors were consistent with Model 1. First, higher observed parenting quality at 1-year predicted decreased child externalizing behaviors at 2-years (β = −0.06, SE = 0.03, p = 0.047). Additionally, higher child externalizing behaviors at 1-year predicted lower observed parenting quality at 2-years years (β = −0.09, SE = 0.03, p = 0.003). Subsequently, higher child externalizing behaviors at 2-years predicted lower observed parenting quality at 3-years (β = −0.10, SE = 0.03, p = 0.001). The maternal-directed paths from parenting at ages 2-years to child externalizing behaviors at 3-years, and from parenting at age 3-years to child externalizing behaviors at 4-years, were not statistically significant.
Of note, none of the cross-sectional paths between the maternal risk composite and observed parenting quality were significant across early childhood. In contrast, all of the cross-sectional paths between the maternal risk composite and child externalizing behaviors at all four time points were significant, with higher maternal risk associated with higher child externalizing behaviors at the same timepoint (β’s ranged from 0.32 to 0.44, p’s < .001). Finally, after adjusting for all other associations in the model, two unexpected findings emerged: longitudinal associations between the maternal risk composite at 1-year predicted decreased child externalizing behaviors at 2-years (β = −0.10, p = .007) and maternal risk at 3-years predicted decreased externalizing behaviors at 4-years (β = −0.08, p = .009), although these coefficients were small compared to the (expected) positive associations between maternal risk and concurrent child externalizing behaviors.
Evaluation of moderation by child sex
Hypothesis 3 examined whether these patterns varied by child sex. We evaluated model fit indices of a fully constrained model where all paths were constrained to be equal for boys and girls and an unconstrained model where all paths were free to vary by sex. In comparing these fit indices, we found that the fully constrained (χ 2 (174) = 550.79, p = 0.00, BIC = 104188.70, RMSEA = 0.058 [90% CI = 0.053, 0.063], CFI = 0.915, TLI = 0.897, SRMR = 0.070) had similar fit to the unconstrained model (χ 2 (144) = 510.345, p = 0.00, BIC = 104604.75, RMSEA = 0.062 [90% CI = 0.057, 0.068], CFI = 0.918, TLI = 0.881, SRMR = 0.060) and was not statistically different in a chi-squared difference test (χ 2 Δ(30) = 10, p = 0.104). Therefore, there was no evidence to support moderation by child sex.
Discussion
Early childhood is a sensitive period during which developmental changes, combined with evolving family dynamics and parenting, contribute significantly to the development of children’s self-regulation abilities and behavior more broadly. Theories and research in developmental psychopathology have highlighted the importance of the bidirectional relations between parenting behaviors and child externalizing psychopathology (Burke et al., Reference Burke, Pardini and Loeber2008; Calkins et al., Reference Calkins, Propper and Mills-Koonce2013; Pettit & Arsiwalla, Reference Pettit and Arsiwalla2008; Sameroff, Reference Sameroff and Sameroff2009), yet few studies have examined how these patterns might develop and change during early childhood or have taken into account other salient family factors. The present study utilized a large, socioeconomically diverse, well-characterized sample of Black and White families in the South to examine these transactional relations during early childhood – a key period for the initial development of externalizing psychopathology. Our repeated-measures longitudinal design allowed us to examine these relationships across multiple time points, from age one to age 4–6. Moreover, our bidirectional models incorporated repeated measures of objectively-coded parenting during a series of teaching tasks as well as a multi-domain measure of maternal risk factors that have rarely been incorporated into extant bidirectional parent-child developmental psychopathology research.
We found evidence for transactional associations (both parent-driven and child-driven effects) between parenting quality and child externalizing behavior during early childhood. First, higher levels of parenting quality at child age 1 were associated with decreases in child externalizing behavior problems at age 2. Although such positive parenting behaviors (involving scaffolding and teaching tasks) have been associated with language and cognitive development in very young children, to our knowledge, no previous studies have identified associations with child behavior. Our observed associations between these scaffolding/teaching parenting behaviors and reductions in early child externalizing behavior are a particularly novel contribution to the literature and suggest additional targets for prevention and intervention. Later parenting quality (e.g., at Wave 2 or Wave 3), however, was not associated with subsequent child externalizing problems in our cross-lagged model. One possible explanation for this pattern is that parents are a key factor in the development of self-regulation in very young children, but as children get older, additional factors – especially factors outside of the home – become increasingly influential (Eisenberg et al., Reference Eisenberg, Taylor, Widaman and Spinrad2015; Karreman et al., Reference Karreman, Van Tuijl, Van Aken and Deković2006; Sulik et al., Reference Sulik, Blair, Mills-Koonce, Berry and Greenberg2015). Augmenting prior research with older children, we found significant associations between concurrent parenting quality and child externalizing behaviors at all time points, as well as stability in both child externalizing behaviors and parenting quality across time in early childhood. Although not tested in the present study, a more direct examination of the potential associations between parenting behaviors, child self-regulation, and externalizing behavior problems would be informative.
Additionally, we found that higher levels of child externalizing behavior problems were longitudinally associated with decreases in parenting quality at two time points. Although evidence for such child-driven effects has gained more prominence in recent years (Roubinov et al., Reference Roubinov, Browne, LeWinn, Lisha, Mason and Bush2022; Yan et al., Reference Yan, Ansari and Peng2021), our findings are novel in that they show that such patterns can manifest at very early ages when externalizing behavior problems may first begin to emerge. Importantly, these effects were present after accounting for the stability of child externalizing behaviors and parenting behaviors over time and after incorporating repeated measures of a maternal risk composite into the models. These findings are consistent with Patterson’s coercion theory, whereby children’s externalizing behaviors have a negative effect on subsequent parenting behaviors (Patterson, Reference Patterson1982, Patterson, Reference Patterson, Reid, Patterson and Snyder2002), and also suggest the potential importance of sustained interventions to ensure that any early improvements in child behavior are not lost over time. It is compelling to note that this pattern of child-driven findings is consistent with some prior transactional parent-child research among older offspring (Dieleman et al., Reference Dieleman, De Pauw, Soenens, Beyers and Prinzie2017; Serbin et al., Reference Serbin, Kingdon, Ruttle and Stack2015; Wang & Liu, Reference Wang and Liu2018). For example, Serbin et al. (Reference Serbin, Kingdon, Ruttle and Stack2015) found that, in a 3-wave design of school-aged children and adolescents (ages 7–13), higher levels of positive parenting at Wave 1 was associated with lower levels of externalizing behavior at Wave 2, whereas higher levels of externalizing behavior at Wave 2 was associated with lower levels of positive parenting at Wave 3. Our findings extend the evidence for this process to young children, beginning as early as toddlerhood.
Study findings highlight the dynamic interplay of parenting behaviors and child externalizing psychopathology beginning in toddlerhood. Whereas most longitudinal studies tend to utilize longer inter-wave intervals (e.g., 2–4 years between study visits), one strength of the present study is the evaluation of how changes in parenting behaviors predict changes in externalizing psychopathology over a 1-year period of time and vice versa. Shorter intervals are particularly important to capture rapid developmental changes that occur during infancy and toddlerhood that require changes in parenting to support safety vs. exploration in early years while responding to the development of self-regulation skills (Lengua et al., Reference Lengua, Honorado and Bush2007). Our findings indicate that younger children may be particularly sensitive to caregiving behaviors, consistent with the known powerful influence of parenting and caregiving behaviors on child behavior during this developmental period. Consequently, aligned with developmental theories of psychopathology (e.g., Calkins et al., Reference Calkins, Propper and Mills-Koonce2013; Cummings et al., Reference Cummings, Davies and Campbell2002; Patterson, Reference Patterson, Reid, Patterson and Snyder2002), early screening and dyadic prevention and intervention programs that occur early in childhood may be particularly impactful – especially for children at higher risk for later behavior problems. Of note, parenting quality at later waves (e.g., Wave 2 or Wave 3) was not associated with subsequent child externalizing behavior problems in our sample after accounting for prior effects, despite the study’s large sample size and robust measurement of positive parenting behaviors (for a similar finding, see, Dora & Baydar, Reference Dora and Baydar2020), suggesting the particular importance of early life parenting for the behaviors assessed here. Our findings regarding child-driven effects point to toddlerhood as a particularly important period for the influence of child externalizing behaviors’ on positive parenting. After adjusting for this period of behavior, subsequent preschool behavior problems may be less powerful – at least for this domain of parenting. As children get older, they might be more likely to have a subsequent influence on other aspects of parenting behaviors (e.g., Serbin et al, Reference Serbin, Kingdon, Ruttle and Stack2015), just as their behaviors are more influenced by factors outside of the home.
Consistent with prior research, we found marked continuity for all three key constructs in our models – maternal parenting quality, child externalizing behaviors, and a maternal risk composite variable. In other words, earlier parenting behaviors predicted later parenting behaviors, which was similarly the case for child externalizing behaviors and other maternal psychosocial risk factors. We also found significant cross-sectional associations between several key study variables, including between a maternal risk composite and child externalizing problems, which aligns with the broader evidence base cited earlier. More notably, however, we did not find an association between concurrent maternal self-reported psychosocial risk (i.e., psychopathology and parenting stress) and observed parenting quality. Despite empirical associations between maternal psychopathology and parenting, literature also suggests that mothers who experience stress and related mental health problems can enjoy secure attachments with their offspring and be responsive and supportive parents (Daryanani et al., Reference Daryanani, Hamilton, Abramson and Alloy2016; Davis & Narayan, Reference Davis and Narayan2020; Greene et al., Reference Greene, McCarthy, Estabrook, Wakschlag and Briggs-Gowan2020; Jones-Mason et al., Reference Jones-Mason, Coccia, Alkon, Melanie Thomas, Laraia, Adler, Epel and Bush2023). Our pattern of findings may also be related to differences in how parenting quality and maternal risk were measured. In the current study, parenting quality measure was derived from a standardized observational assessments of mothers engaging with children in a novel task in-clinic, while the parenting stress measure reflects a mother’s perception of both herself as a parent and of her child. Some research indicates that mothers – especially mothers who experience psychopathology – might have more biased, negative self-perceptions of their own parenting behaviors as well as the behaviors of their child (e.g., Muzik et al., Reference Muzik, Morelen, Hruschak, Rosenblum, Bocknek and Beeghly2017), when, in fact, their observed parenting behaviors are more positive and supportive.
After accounting for the multitude of other associations in the model, our composite measure of maternal risk was negatively associated with later child externalizing behavior problems at ages two and four. We would have expected the association to be in the opposite direction – given that the maternal risk composite was positively associated with child externalizing behavior problems across all waves at the bivariate level (for similar cross-sectional findings, see Kochanova et al., Reference Kochanova, Pittman and McNeela2022). It is possible that this association is substantively meaningful and would be mediated by other omitted psychosocial/family factors for the current sample. It is also possible that these counterintuitive results are a statistical artifact of the complex multivariate models (e.g., due to statistical suppression). We are therefore hesitant to interpret these findings, especially within the context of such a robust model, where the remaining variance to be explained is quite reduced.
Finally, the present study did not find that any tested associations differed by child sex. Findings regarding sex-specific associations between parenting and child externalizing behaviors have been inconsistent (e.g., Blatt-Eisengart et al., Reference Blatt-Eisengart, Drabick, Monahan and Steinberg2009; Smith & Day, Reference Smith and Day2018; Xing et al., Reference Xing, Wang, Zhang, He and Zhang2011; for an early meta-analysis, see Rothbaum & Weisz, Reference Rothbaum and Weisz1994). This may be due to differences in child age ranges assessed, the type of parenting behaviors measured, and the informants utilized. As our study was well-powered, this might suggest that associations between positive parenting behaviors and child externalizing behaviors may not be unique to boys or girls during the early childhood period, which could indicate that interventions during early childhood may have positive benefits for children (and parents) regardless of the child’s sex. However, we are hesitant to overly interpret our lack of evidence for moderation as more research is necessary during early childhood that utilizes objective measures of parenting and child behaviors to determine whether our null findings replicate.
We note several strengths in the present study. We utilized a large, predominantly Black, socioeconomically diverse sample – both of which are under-represented in extant psychopathology literature. We also leveraged a robust model with multiple repeated measures over time. In addition, the use of trained observers and an established coding paradigm to evaluate parenting behaviors is a noteworthy strength for this study, especially given the large sample size. This measure of parenting assesses behaviors that are very relevant for younger children, such as cognitive and social-emotional growth-fostering behaviors, as well as parental sensitivity, warmth, and responsivity. Another unique strength is the inclusion of other maternal psychosocial factors – which also have the potential to impact parenting and child behavior – within our repeated-measures models. In addition to the fact that their inclusion goes beyond the majority of extant literature, it further increases confidence that the present findings have more to do with parenting than maternal mental health. Our study design also had some limitations. First, we utilized two different measures for child behavior across our four waves of analysis. Although the measures used were age-appropriate and demonstrated some degree of stability across time, we may have been unable to detect some changes over time due to the change in the measure used. Additionally, child behavior was reported by mothers in the present study and mothers also self-reported on their parenting stress and psychopathology indicators, which introduces potential for informant bias. Although parents are a key informant for child behaviors during early childhood, and our use of objectively-rated parenting offsets risk of same-reporter-driven findings, this study would have been strengthened with measures of child externalizing collected from other adults, caregivers, or during laboratory visits. Additionally, although the use of an observational measure to assess parenting quality is a strength, there is still a possibility for rater bias. Also, observed parenting was not assessed at wave 4, which prevented us from evaluating its lagged and cross-sectional associations at that final time point. Although self-regulation is one possible mechanism by which parenting is linked to later externalizing behaviors, it was not assessed in the current study and thus could not be evaluated as a mechanistic link; future work should further elucidate this pathway. Finally, other social determinants of health, such as discrimination and structural racism or childcare quality, certainly have varying affects on family dynamics, including parenting and child behaviors, disproportionately affecting minoritized families or those with fewer resources. Although measures of such constructs were not available for the present study, their roles in the processes studied here are important considerations for future research.
It is important to acknowledge that numerous structural and societal barriers disadvantage some families (particularly lower-income families and families of color), limiting their ability to establish more nurturing home environments with optimal resources for caregiving (Bailey et al., Reference Bailey, Krieger, Agénor, Graves, Linos and Bassett2017; Conradt et al., Reference Conradt, Carter and Crowell2020; O’Brien et al., Reference O’Brien, Neman, Seltzer, Evans and Venkataramani2020; Palmer et al., Reference Palmer, Anand, Graff, Murphy, Qu, Völgyi, Rovnaghi, Moore, Tran and Tylavsky2013; Rowell & Neal-Barnett, Reference Rowell and Neal-Barnett2022). Although we highlight the importance of the mother-child relationship herein, the responsibility for children’s behavioral development certainly does not lie solely with the mother, but also other caregivers, such as fathers (Cardenas et al., Reference Cardenas, Morris, Marshall, Aviv, Martínez García, Sellery and Saxbe2022), and is critically dependent on society providing sufficient resources and supports to children and families (Jones et al., Reference Jones, Simon, Yadeta, Patterson and Anderson2023; McLean et al., Reference McLean, Fish, Rogers and Syed2023; Okuzono et al., Reference Okuzono, Wilson and Slopen2023; Phelan & Link, Reference Phelan and Link2015; Suslovic & Lett, Reference Suslovic and Lett2023; Traub & Boynton-Jarrett, Reference Traub and Boynton-Jarrett2017; Walker et al., Reference Walker, Wachs, Grantham-McGregor, Black, Nelson, Huffman, Baker-Henningham, Chang, Hamadani, Lozoff, Gardner, Powell, Rahman and Richter2011; Winett et al., Reference Winett, Wulf and Wallack2016). Eliminating structural inequities and providing additional supports and resources for parents and families (e.g., parental leave, adequate wages for child care, perinatal interventions, cash transfer programs, family tax credits, increased mental health insurance coverage) that reduce stress and enable positive parenting, in addition to directly supporting the psychosocial interactions among the parent-child dyad early in development, are needed for the prevention of later child psychopathology. Future studies in developmental psychopathology would benefit from including these relevant factors (i.e., examining multiple generations, including family-level factors, as well as structural barriers) when conducting research on parent and child psychopathology and well-being (see, also, McLean et al., Reference McLean, Fish, Rogers and Syed2023).
Conclusion
Overall, the present findings indicate that the transactional nature of the parent-child relationship starts in infancy – with evidence for both parent-driven and child-driven effects across early childhood. Findings underscore the importance of supports for parents, children, and families in order to prevent the development of child externalizing psychopathology. Additionally, given the potential manifestation and stability of early childhood externalizing behaviors, early life interventions provided on an on-going basis seem more likely to sustain improvements in child behaviors over time. With the growing body of literature that highlights the importance of taking a two-generational view on prevention and early intervention strategies for child psychopathology (Ahmad et al., Reference Ahmad, Rudd, LeWinn, Mason, Murphy, Juarez, Karr, Sathyanarayana, Tylavsky and Bush2022; Bush, Reference Bush2024; Roubinov et al., Reference Roubinov, Browne, LeWinn, Lisha, Mason and Bush2022), our findings provide further support for the potential benefits of early screening and intervention for both parenting challenges as well as child externalizing problems (see also Hagan et al., Reference Hagan, Browne, Sulik, Ippen, Bush and Lieberman2017; Piotrowski et al., Reference Piotrowski, Talavera and Mayer2009). Especially for younger children, supportive family- or dyadic-level interventions are likely to be particularly beneficial in the prevention of child psychopathology.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579424001147.
Author contributions
Drs. Roubinov and Bush contributed equally to the conceptualization, supervision, and mentoring on this manuscript as co-senior authors.
Funding statement
The ECHO PATHWAYS consortium is funded by the NIH (grants 1UG3OD023271-01 and 4UH3OD023271-03). The CANDLE study was also funded by the Urban Child Institute and the NIH (R01 HL109977). We are grateful for the participation of families enrolled in the CANDLE cohort, as well as the dedication of CANDLE and PATHWAYS research staff and investigators. Dr Bush is the Lisa and John Pritzker Distinguished Professor of Developmental and Behavioral Health and receives support from the Lisa and John Pritzker Family Foundation and the Tauber Family Foundation.
Competing interests
None.







 Open access
Open access