

Nearly 40 years ago, Brown and his colleagues believed that ordinary aspects of family life were crucial to an understanding of how families interact with patients in their midst (Reference Brown, Leff and VaughnBrown, 1985). The concept and measurement of the ‘expressed emotion’ within families were developed in the 1960s, initially for use in schizophrenia. They were subsequently used for a number of physical and psychiatric conditions, ranging from dementia to diabetes and Parkinson's disease. They have been a major impetus for the development and evaluation of social treatments of schizophrenia (Reference Kuipers and BebbingtonKuipers & Bebbington, 1990). The family's expressed emotion has been shown to be predictive of outcome in mental and physical illnesses in a variety of cultural settings.
The first research instrument to record the range of feelings and emotions found in ordinary families was the Camberwell Family Interview, developed by Brown. This is conducted with the key carers of the patient, and from it the interviewer tries to create a picture of how things have been in the household in the months leading to the onset of illness. In the first phase of development of the interview, Brown and colleagues (Reference BrownBrown, 1959; Reference Brown, Carstairs and ToppingBrown et al, 1958, Reference Brown, Monck and Carstairs1962, Reference Brown, Birley and Wing1972) reported that theoretical constructs were being developed at the same time as the interviews were being conducted. In a historical account of the process, Reference Brown, Leff and VaughnBrown (1985) suggested that the term ‘expressed emotion’ emerged only after several studies had been carried out.
After the instrument had been in use for a while, the researchers developed a semi-standardised interview, distinguishing between critical comments and dissatisfaction (although they clearly go together). The original interview was very long and it has now been shortened so that it can be completed in 2–2½ hours. In current usage, the interview is taped and its transcript is rated on a number of parameters. Two types of information are elicited: objective information about events and circumstances in the home in the months before the admission and subjective information concerning the relative's feelings and attitudes towards the patient when talking about the illness. Reference Leff and VaughnLeff & Vaughn (1985) point out that the interview is in a ‘mental conversational style … rather than a clinical one’. All judgements on the relative's expressed emotion are based on this interview.
The components of expressed emotion
In his original interview, Brown described five components of expressed emotion (Reference Brown, Leff and VaughnBrown, 1985): emotional overinvolvement, critical comments, hostility, positive remarks and warmth. Critical comments are simply counted over the period of the interview, and hostility is rated as being absent or present and as generalisation and rejection. Warmth is rated on a 6-point scale. Emotional overinvolvement is an extremely complex construct and it often causes difficulties for both researchers and clinicians. It is also the most likely of the five components to vary across cultures. Many attitudes and behaviours relevant to this rating may be evident during the interview, for example exaggerated emotional response, excessive self-sacrifice or devoted behaviour, and marked over-protectiveness. The index of expressed emotion therefore can be seen as an indicator of ‘emotional temperature’ in the home – it is a marker of intensity, although it is not necessarily a constant.
The interaction between expressed emotion and patient outcome is complex. Research has demonstrated that patients from households with high expressed emotion do not differ in their pathology from those in households with low. It is the relatives who differ markedly in their response to the patients and their illnesses. Of the five scales, critical comments, hostility and emotional overinvolvement have been shown to be the most predictive of relapse (i.e., of increased symptoms) (Reference KuipersKuipers, 1992).
It should be noted that the interactions between the patient and the family are also important, especially cross-culturally. In some cultures, for example in parts of India, emotional overinvolvement is the norm. If a carer does not show emotional overinvolvement it is seen as lack of care. Interviewers should try to understand and follow cultural norms. Expressed emotion is best measured by a person from the same cultural group: it is difficult for a researcher who is not familiar with the nuances of language and cultural expression of an interviewee to rate any of the components of expressed emotion. If measures of expressed emotion are being applied in cultures where they have not been used before, they must be accompanied by fieldwork to establish the norms and the context. The most important factor for the researcher is to embed emotional overinvolvement, hostility and warmth in the specific cultural context. Measurement is also dependent on an assessment of the interviewee's general style of emotional expression.
Findings from Western countries
Meta-analyses
There have been more than 30 studies of outcome in schizophrenia for a total of over 1500 patients. The most recent meta-analysis of the relationship between expressed emotion and outcome examined the predictive validity of the construct in relapse of schizophrenia, mood disorders and eating disorders (Reference Butzlaff and HooleyButzlaff & Hooley, 1998). Using 27 of the studies that focused on outcome in schizophrenia, the authors concluded that expressed emotion is a significant and robust predictor of relapse in schizophrenia. Additional analyses demonstrated that the relationship between expressed emotion and relapse was strongest for patients with more chronic schizophrenic illness. Interestingly, although the expressed emotion construct is most closely associated with research in schizophrenia, the mean effect sizes for expressed emotion for both mood disorders and eating disorders were significantly higher than the mean effect size for schizophrenia.
Butzlaff & Hooley's study agrees with Reference Bebbington and KuipersBebbington & Kuipers’ (1994) aggregate analysis of 25 studies with 1346 patients. This found that for patients living in situations rated as showing high expressed emotion (the ‘high expressed emotion group’; n = 705) the relapse rate was 50%, whereas in the ‘low expressed emotion group’ (n = 641) the rate was 21%. In the majority of the studies, high expressed emotion was predictive of relapse in symptoms of schizophrenia 9 months later for both genders. A large amount of face-to-face contact (more than 35 hours per week) with a relative with a high expressed emotion score increased the risk of relapse, but in households with a low expressed emotion score, high levels of contact appeared to be protective. Both warmth and positive comments were predictive of good outcome. Interestingly, medication had an independent effect on relapse rate, suggesting that medication is useful for patients irrespective of the expressed emotion status in the family. One of the criticisms of the applications of this construct, therefore, is that it can ‘pathologise’ the family or specific relatives who might in reality be struggling hard to cope with a difficult home situation.
The UK
Reference Vaughn and LeffVaughn & Leff (1976) studied 43 patients with schizophrenia and 32 patients with ‘depressive neurosis’, and were able to follow up 37 and 30 patients respectively in the two groups. Most of the patients with depression came from marital homes. The relapse rate for the patients from homes that showed high expressed emotion was 50%, compared with 12% for those from homes with low expressed emotion. The authors used seven or more critical comments and/or an emotional overinvolvement rating of 4 or 5 to rate expressed emotion as high. They found that the amount of face-to-face contact also reflected the status of expressed emotion. They reported that more than 35 hours of face-to-face contact was the crucial cut-off. Those whose exposure was more than 35 hours had higher relapse rates (89% v. 57%). When they explored the use of medication they found that high expressed emotion subjects who were not on medication were more likely to relapse (78%) than those who were on medication (25%). They argue that low expressed emotion and regular medication act as additive factors in reducing the risk of relapse. Of the patients with depression, 67% of those who had a relative with a critical comments score of more than 2 relapsed, compared with 22% if the score was 0 or 1.
The USA
Using similar methods in California, Vaughn and her colleagues observed that 33% of Californian families had been rated low expressed emotion compared with 52% in the British sample (Reference Leff and VaughnLeff & Vaughn, 1985). The Californian families were significantly less likely to make no critical comments than the London families, and ratings of hostility were more common in the Californian sample, but there were no cultural differences in emotional overinvolvement. Once again, patients in high expressed emotion settings were more likely to relapse (56% compared with 17% for low expressed emotion). Also, there was a high relapse rate (68%) among those in the non-medicated high expressed emotion group, whereas there were no relapses at all in the medicated low expressed emotion group.
Australia
In Australia, Reference Vaughan, Doyle and McConaghyVaughan et al(1992) recruited 91 suitable patients with schizophrenia and found that 59% in the high expressed emotion group relapsed compared with 36% in the low expressed emotion group. High contact (more than 35 hours per week) was more likely to increase relapse (68%) compared with only 12% in low expressed emotion groups. There was no gender difference and those from high expressed emotion households were still more likely to relapse even when on medication (42%), confirming the previous findings from London and California.
Studies of home and residential settings
In an interesting development, Reference Moore, Kuipers and BallMoore et al(1992) studied expressed emotion in group homes and long-term care settings in the UK and found that high expressed emotion settings were characterised by less tolerance, inappropriate expectations of patient progress and frustration in the keyworker. Criticisms focused on embarrassing behaviours and negative symptoms. In a follow-up UK study, Reference Ball, Moore and KuipersBall et al(1992) found that higher discharge rates were possible for patients who were ready to return to low expressed emotion hostels.
The study and identification of expressed emotion in the relatives of patients with schizophrenia in different settings have led to the development of intervention strategies with families and carers. The aim of such work is to reduce expressed emotion by education and also to reduce the patients’ faceto-face contact with high expressed emotion individuals to less than 35 hours per week. Most studies have shown that this is possible. Lowering of the expressed emotion can be achieved through relatives’ groups and individual and family work. Another innovation is the use of the ‘5-minute speech’, during which a relative is asked to talk about the patient (Reference Magana, Goldstein and KarnoMagana et al, 1986). This has been shown to be a useful practical measure of levels of expressed emotion. However, the authors point out that this method may misclassify a proportion of high expressed emotion individuals as low.
Findings from non-Western countries
India
Levels of expressed emotion in families in developing countries have been assessed in several studies. The levels as well as the prevalence of the various components of the rating scale vary. For example, the tone of the voice can play a role in the identification of high expressed emotion, but in several cultures speaking loudly is the norm. In a Chandigarh-based sub-study of the World Health Organization's study of first-onset schizophrenia, 104 relatives were interviewed for the purposes of assessing expressed emotion (Reference Wig, Menon and BediWig et al, 1987b ). Of the three centres studied (Chandigarh, Aarhus and London) the Chandigarh sample reported the lowest ratings on all of the following: mean number of critical comments; proportion of relatives showing hostility; positive remarks; mean score on warmth; and level of parental overinvolvement. Compared with the 54% of relatives classified as showing high expressed emotion in the two European centres, the Chandigarh sample had only 23% of relatives classed as showing high expressed emotion. More than a quarter (29%) of the Chandigarh sample showed hostility but low criticism. The authors concluded that the Chandigarh relatives commonly express both high criticism and high warmth at the same time. One-year follow-up suggested that the better outcome in cases of schizophrenia in Chandigarh may be related to the high proportion of relatives with low expressed emotion. In a further report, the authors suggest that expression of anger in the form of hostility is relatively unmodified by cultural factors (Reference Leff, Wig and GhoshLeff et al, 1987).
Egypt
In a study from Egypt, Reference KamalKamal (1995) observed that high expressed emotion was present in 55% of the families of patients with schizophrenia. They reported that Egyptian patients tolerated higher levels of criticism before relapse than have been reported in Western studies. They suggested that these levels were inclusive of benign criticism. A similar observation was reported by Reference Okasha, El-Akabawi and SnyderOkasha et al(1994), who found that criticism is an accepted and acceptable component of interpersonal relations in Egyptian culture and that it might well reflect an element of care. It is also possible that criticism and overinvolvement are intertwined and that warmth might act as a key protective factor. Emotional overinvolvement is seen in the West as pathological because it crosses the boundaries of individuals (i.e. it acts against the individual, egocentric position), whereas in other cultures such an approach may be the norm. In sociocentric societies emotional overinvolvement is to be expected because the individual is part of the larger kinship group. (Egocentric or individualistic societies are those in which the individual is seen as predominant, whereas in sociocentric or collectivist societies individuals are an integral part of kinship and it is kinship that takes precedence over individuals.)
Israel
Similarly, it has been demonstrated that anger is more openly and more immediately expressed in Israel than in Western countries and a failure to express one's anger is perceived as a weakness (Reference Heresco-Levy, Greenberg and DasbergHeresco-Levy et al, 1990). Thus, it is likely that both hostility and critical comments seen in the context of anger may result in false-positive rates of high expressed emotion. Heresco-Levy et al emphasise that expressed emotion ratings must be adjusted in relation to the normative levels of overt expression of emotions, which vary across cultures. However, changes in levels may be influenced by processes of acculturation if cultural groups move across national and cultural boundaries.
China
In China, Phillips & Xiang (1995) found that, using conventional criteria for rating expressed emotion, over 42% of Chinese family members of patients with schizophrenia were rated as showing high expressed emotion. They also observed a non-significant increase in the relative risk of relapse for Chinese patients from high expressed emotion households when compared with low expressed emotion households. They attribute this to a number of factors. First, the impact on the patient of a high expressed emotion relative may be less significant in Chinese culture than in other cultures. Second, the fact that the role of families (especially small families) in the context of a political system in which an individual's role is as seen by the state may well act as a protective factor. Third, it might also reflect the diverging attitudes of the community and the individual regarding the individual's autonomy.
Japan
From Japan, Reference Mino, Tanaka and InoueMino et al(1995) reported that, contrary to their expectations of low expressed emotion (as Japanese tend not to display emotions readily), 48% of Japanese households were classified as high expressed emotion, with criticism being the most common item (39% of households made six or more critical comments).
This brief overview of expressed emotion across cultures suggests that different components of expressed emotion (Box 1) have varying prevalence across different cultures.
Box 1 Indicators of high expressed emotion
Critical comments: six or more
Emotional overinvolvement: a score of 3 or higher
Hostility: present
Warmth: absent
Positive regard: absent
Ethnic minority groups
It is inevitable that different cultures will place differing emphasis on the various components of expressed emotion. For example, in the Indian context, mothers are over-involved with their sons and this overinvolvement is not necessarily pathological. Similarly, in Jewish settings, critical comments and overinvolvement on part of the mother are culture-related and should not be perceived as pathological.
Mexican American families
In the study of expressed emotion in ethnic minority groups, Jenkins’ work, especially that dealing with Mexican American families, has been ground-breaking. Highlighting the anthropological and clinical dimensions of individually variable (and sometimes deviant) constructions of family worlds within particular cultural contexts, she argues that emotional overinvolvement is clinically rated on the basis of affective and behavioural features (that may include self-sacrificing and extremely overprotective behaviours) but that it should not be (Reference Jenkins and GainesJenkins, 1992). In her study of Mexican Americans she suggests that Mexican culture encourages relatives to display a high degree of involvement in kin affairs.
After studying 70 Mexican American families and 109 key relatives, Reference Karno, Jenkins and DelaselvaKarno et al(1987) found that only 11% of the relatives were rated as showing high expressed emotion. Nearly all of the 11% were female and almost all of the patients were male. The authors had adapted the expressed emotion rating scales for the Mexican American cultural context and found that the outcome of schizophrenia in their sample was indeed related to expressed emotion in the family, but they caution that the cross-cultural validity of concepts such as overinvolvement must be taken into account.
Asian families in the UK
In Birmingham, UK, Reference Hashemi and CochraneHashemi & Cochrane (1999) reported on expressed emotion in 60 families (20 British Pakistanis, 20 British Sikhs and 20 matched Whites), all of which included a relative with a diagnosis of schizophrenia. They observed that 80% of the British Pakistani, 45% of the White and 30% of the British Sikh families exhibited high levels of expressed emotion. Emotional overinvolvement was significantly higher among the British Pakistani group (55% v. 10% for the British Sikh group). They observed that the modal score for White and Sikh relatives on emotional overinvolvement was 1, whereas for British Pakistanis it was 4. Using the conventional rating criteria the authors found that White patients with high expressed emotion relatives were significantly more likely to relapse than those from low expressed emotion families, whereas for both Asian groups, high expressed emotion did not predict relapse. However, raising the cut-off of emotional overinvolvement for Pakistani families led to significantly better prediction of relapse. Although the numbers are small in this study, these differences indicate that using conventional measures of expressed emotion across different ethnic groups is fraught with difficulties. The authors draw our attention to similarities between the UK Asian and North Indian groups. Hashemi & Cochrane subsequently carried out a population-based normative study for expressed emotion and found that Pakistani families in the UK were more likely to be rated as high expressed emotion than White families, indicating that components such as emotional overinvolvement may be cultural rather than pathogenic traits (Reference Hashemi and CochraneHashemi & Cochrane, 1999).
Clinical implications
Studies of different national and ethnic minority groups show that it is essential that normative data on expressed emotion in the population are available before clinicians can assess the prevalence and effects of high expressed emotion among the families of patients with psychiatric or physical disorders. Expressed emotion is not a simple unidirectional concept and it should not be seen in isolation of intermediary factors such as the role of kinship, attitudes of the family to mental illness and family and cultural dynamics.
Implications for management
There is some evidence that outcome in schizophrenia is better in developing countries and this has been attributed to low expressed emotion (Reference Wig, Menon and BediWig et al, 1987a ,Reference Wig, Menon and Bedi b ). However, although outcome has been shown to be variable for different ethnic groups in the UK, data on expressed emotion and its relationship to outcome in minority ethnic groups are sparse. Out of the five constructs of expressed emotion (critical comments, emotional overinvolvement, hostility, warmth and positive remarks) it is the first three that have been shown to predict outcome for patients with schizophrenia. Our conjecture is that these three components are helpful, but that they must be seen in the context of culture and kinship and, more important, they must be considered in the context of warmth and positive regard. Most studies neglect to place warmth and positive regard in the protective light that they should be seen in. In some cultures, positive regard is related not to the individual but to his or her social status and background. These social factors may then interact with hostility and emotional overinvolvement, blunting their edge in a more significant way.
For the clinician, several significant factors affect the way prognosis or outcome of schizophrenia can be seen in the context of expressed emotion. Most importantly, the role of normative cultural data for the general population (who do not have a relative with a mental illness) needs to be understood. If the normative data show high levels of expressed emotion then the significance of these components in mental illness has to be seen in that context. The effects of intermediary factors such as explanation of the illness, attitudes towards the illness, the perceived or real autonomy of the individual, the socio- or egocentric status of the individual in the cultural context, role expectations of the individual and the effect of the illness on these roles must be studied further and related to outcome, compliance and treatment adherence (Fig. 1).
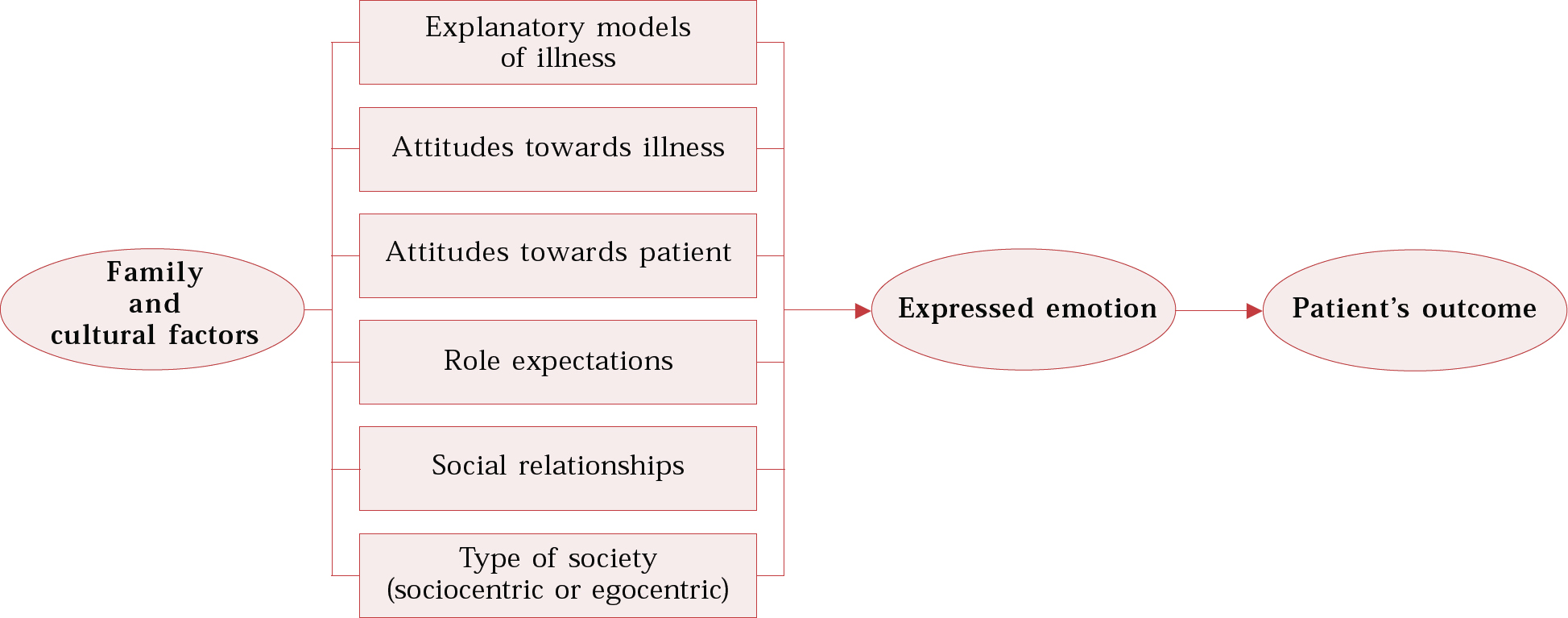
Fig. 1 Family and cultural characteristics that may influence patient outcome through expressed emotion.
In working with families to reduce expressed emotion, clinicians must take into account the role that family therapy may be seen as having in managing patients. Some families see family therapy as intrusive and prescriptive, whereas others welcome it in order to learn more about managing the patient in their midst and the illness. Gender and gender-role expectations also play an important part in this context (Box 2).
Box 2 Family intervention
In family interventions, clinicians should take the following family characteristics into consideration:
-
• structure, e.g. nuclear or extended
-
• significant members
-
• cultural and social norms
-
• expectations of the patient
-
• knowledge of the illness
-
• acceptance of medical or psychological intervention
-
• gender-role expectations
-
• external support systems
Family structures contingent on economic interdependence and patriarchal norms are protective in some settings. Therefore, the normative prevalence of the components of expressed emotion should be rigorously established across different cultural groups and its constructs may have to be given different emphasis depending on cultural context.
Conclusions
Cultural variation in the degree and type of expressed emotion has to be studied carefully and understood in order to apply the principles of expressed emotion across different cultural groups and settings. The data across cultures have not provided consistent findings, suggesting that different cultural settings have different rates of high expressed emotion normatively. The clinicians and researchers must establish the baseline normative data before accepting these findings and establishing family interventions.
Multiple choice questions
-
1 The following are the components of expressed emotion:
-
a critical comments
-
b hostility
-
c warmth
-
d emotional overinvolvement
-
e heated arguments.
-
-
2 Expressed emotion has been shown to be associated with:
-
a onset of schizophrenia
-
b relapse of schizophrenia
-
c personality disorders
-
d criminal behaviour
-
e relapse in mood disorders.
-
-
3 Cross-cultural studies of expressed emotion have shown:
-
a the same incidence of high expressed emotion in both Western and non-Western cultures
-
b the same incidence of relapse compared in both Western and non-Western cultures
-
c that all five components have equal prominence across cultures
-
d relapse rates are similarly influenced across all nations
-
e that the impact of relatives with high expressed emotion is the same across cultures.
-
-
4 Across ethnic groups:
-
a emotional overinvolvement is higher in some groups
-
b the same cut-off points for rating are valid
-
c emotional overinvolvement may be valued in some groups
-
d it is essential to have normative data for each ethnic group
-
e expressed emotion may be influenced by the gender of the carers.
-
-
5 The following may play an important role in engaging the family for therapeutic work:
-
a family structure
-
b significant family members
-
c the family's expectations of treatment
-
d that all members of the family are involved
-
e the family's knowledge of the illness and treatment.
-
MCQ answers
| 1 | 2 | 3 | 4 | 5 | |||||
| a | T | a | F | a | F | a | T | a | T |
| b | T | b | T | b | F | b | F | b | T |
| c | T | c | F | c | F | c | T | c | T |
| d | T | d | F | d | F | d | T | d | F |
| e | F | e | T | e | F | e | F | e | T |


eLetters
No eLetters have been published for this article.