



Introduction
Depressive disorders are one of the leading causes of morbidity globally [Global Burden of Disease (GBD) 2017 Disease and Injury Incidence and Prevalence Collaborators, 2018; World Health Organization, 2017]. This pattern is clear in Europe (Andlin-Sobocki, Jonsson, Wittchen, & Olesen, Reference Andlin-Sobocki, Jonsson, Wittchen and Olesen2005), and in Sweden, the incidence and indirect costs of depressive disorders have increased over the last decades (Tiainen & Rehnberg, Reference Tiainen and Rehnberg2009). Depression represents not only a large cost to individuals, but also the people around them and society as a whole.
For this reason, a better understanding of potentially modifiable risk factors is crucial in order to devise strategies for the prevention and improvement of depression. One such factor is the working environment, where most adults spend much of their time. Psychosocial characteristics of the work environment may be important for the development of depressive symptoms, as has been concluded in several systematic reviews (Bonde, Reference Bonde2008; Madsen et al., Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola, Alfredsson and Kivimäki2017; Netterstrom et al., Reference Netterstrom, Conrad, Bech, Fink, Olsen, Rugulies and Stansfeld2008; Siegrist, Reference Siegrist2008; Theorell et al., Reference Theorell, Hammarstrom, Aronsson, Traskman Bendz, Grape, Hogstedt and Hall2015).
One of the most important and widely used theoretical models for understanding psychosocial working conditions in relation to stress and health is the job demand–control or job strain model (Karasek, Reference Karasek1979). Job demands refer to the amount of work and time pressure that is experienced, while job control refers to how much influence a person has over the organization and pace of their work. Jobs that have high demands in combination with low control are known as high strain jobs, and this has been found to be associated with adverse health outcomes (Kivimäki et al., Reference Kivimäki, Nyberg, Batty, Fransson, Heikkilä, Alfredsson and Theorell2012).
While previous systematic reviews and meta-analyses have concluded that poor work environments regarding these psychological components are related to an increased risk of depression (Bonde, Reference Bonde2008; Madsen et al., Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola, Alfredsson and Kivimäki2017; Netterstrom et al., Reference Netterstrom, Conrad, Bech, Fink, Olsen, Rugulies and Stansfeld2008; Siegrist, Reference Siegrist2008; Theorell et al., Reference Theorell, Hammarstrom, Aronsson, Traskman Bendz, Grape, Hogstedt and Hall2015), the studies included in these reviews have some important methodological limitations. These limitations include inadequate control for confounding, relying on self-report of workplace exposures and/or depression and sometimes using the same informant for measuring both, and small sample sizes or sampling limited to a single branch or firm. These reviews conclude the need for independent measures of exposure and outcome and more objective measures of depression such as clinical diagnosis. Controlling for confounding is particularly important because there are several factors that may influence entrance and position in the labor market and risk for developing depression. Some such factors are disadvantages during childhood, immigrant status, education, family situation, and previous psychiatric health. One approach to independently measuring the psychosocial workplace conditions is the use of a Job Exposure Matrix (JEM). This approach surveys individuals within different occupations and aggregates their answers about exposures on an occupational level. These JEM scores can then be connected to individuals based on their occupations and have the potential to be used in population-level studies using more objective diagnostic healthcare data.
Some experts have argued that job control may be the more important factor in the job strain model in predicting health outcomes (Ingre, Reference Ingre2015; Knardahl et al., Reference Knardahl, Johannessen, Sterud, Harma, Rugulies, Seitsamo and Borg2017; Mikkelsen et al., Reference Mikkelsen, Andersen, Bonde, Hansen, Kolstad and Thomsen2018), and that job control may actually be the reason for observing significant associations for the combined job strain variable. This, however, is not agreed upon by all (Kivimäki, Nyberg, & Kawachi, Reference Kivimäki, Nyberg and Kawachi2015). Possibly for this reason, some researchers choose to focus only on job control (Svane-Petersen et al., Reference Svane-Petersen, Holm, Burr, Framke, Melchior, Rod and Madsen2020). The different aspects of the model and their combination are most often expressed as a single dichotomous measure, which can make interpretation difficult. It is important to closely investigate a more extensive range of the different components of this model as well as their combination in order to better understand the relationship between job strain and depression and investigate possible dose–response relationships.
The present study aims to investigate the relationship between the psychosocial work environment exposures of job control, job demands, and job strain and the risk of developing depression during a 10-year follow-up period using aggregated job exposure data and patient registry information on the Swedish working population age 30–60 in 2005, taking into account previous psychiatric diagnoses, family situation, birth country, socioeconomic position (SEP) during childhood, and parents' mental health. Because of Sweden's relatively gender-segregated labor market (Hansen & Wahlberg, Reference Hansen, Wahlberg, Solomon and Konstantinos2008) and important differences in potential workplace exposures, associations are considered separately for men and women.
Based on Karasek's job strain model (1979), we hypothesize that low job control and high job demands will independently relate to an increased risk of depression in a dose–response pattern, and that their combination (job strain) will also be associated with an increased risk of depression. We expect these associations to be partially explained by the above-mentioned background factors and for the pattern to be similar for men and women, though the strength of associations may vary.
Methods
Study population
The present study is based on the linkage between the Swedish total population register, the Longitudinal Integrated Database for Health Insurance and Labor Market Studies register (LISA), the Swedish National Patient Register, as well as census information from 1960, 1970, and 1980.
The total population register includes information on births, deaths, civil status, and migration and the LISA register includes mandatory reported information on occupation for everyone 16 years of age or older as well as their obtained education (Ludvigsson, Svedberg, Olen, Bruze, & Neovius, Reference Ludvigsson, Svedberg, Olen, Bruze and Neovius2019). The national in-patient register has existed since the 1960s and has included psychiatric hospitalizations since 1973, while the out-patient register includes less severe public and private psychiatric visits and has been in use since 2001 (Socialstyrelsen, 2019). These Swedish registers have been commended for their accuracy and completeness in reporting (Ludvigsson et al., Reference Ludvigsson, Andersson, Ekbom, Feychting, Kim, Reuterwall and Olausson2011, Reference Ludvigsson, Almqvist, Bonamy, Ljung, Michaelsson, Neovius and Ye2016, Reference Ludvigsson, Svedberg, Olen, Bruze and Neovius2019).
The initial cohort resulting from these linkages, which has recently been named the Swedish Work, Illness, and labor-market Participation (SWIP) cohort, consists of around 5.4 million individuals. The present study is restricted to those born between 1945 and 1975 (i.e. between the ages of 30 and 60 at the baseline year, 2005). This restriction was made because it is assumed that those in this age group would have been both established and remaining in the labor market. We assume that those over the age of 30 are more likely to be stable in their occupations during the follow-up period compared to those under 30. The resulting population consists of around 3.8 million individuals of which around 3 million had complete information on occupation in 2005.
Ethical approval was obtained from the Stockholm ethics review board, reference number 2017/1224-31 and 2018/1675-32.
Measures
Exposures
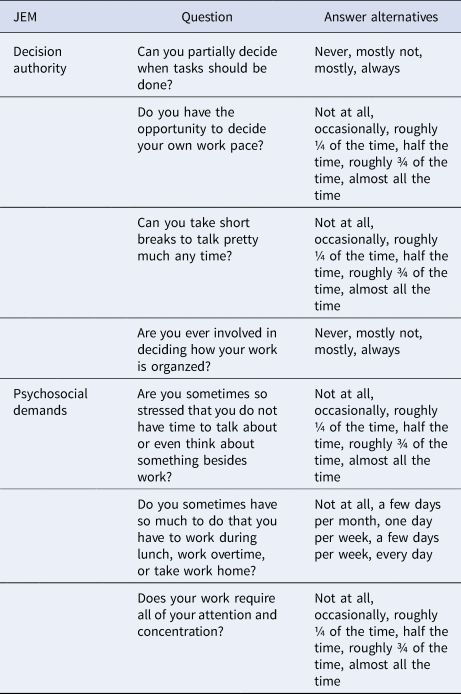
Job control and job demands were measured using the Swedish JEM measuring psychosocial workload based on information from the Swedish Work Environment Surveys (1997–2013). This JEM measures the aggregated experience of aspects of the work environment in different occupations separately for men and women. These scores are based on around 75 000 respondents and linked to a person's occupation based on the Swedish ISCO-88 four-digit classification of occupations obtained from the LISA register in 2005 (SCB statistics Sweden, 2001). Job control is measured based on four questions measuring decision authority, which is related to the amount of influence people have over the way their work is done. These questions focus on the aspects of the ability to determine which tasks to do, the pace of work, when to take breaks, and the structure of the work. Job demands are measured using three questions focused on the stress, time, and level of concentration of the job. The translated items are shown in Table 1, and extensive information on the construction of these JEMs is described in detail elsewhere (Fredlund, Hallqvist, & Diderichsen, Reference Fredlund, Hallqvist and Diderichsen2000). These measures were initially scored as a mean for each occupation. We categorized these mean scores according to their quintile distribution separately for men and women, resulting in five categories ranging from low to high.
Table 1. Translated items used for the decision authority and demands Job Exposure Matrices (JEM)
Job strain is defined as the combination of job control and job demands split at their medians and was initially categorized into four categories: high strain jobs (low control/high demands); low strain jobs (high control/low demands); passive jobs (low control/low demands); and active jobs (high control/high demands). To make our results more comparable to some of the more influential studies on job strain (Kivimäki et al., Reference Kivimäki, Nyberg, Batty, Fransson, Heikkilä, Alfredsson and Theorell2012; Madsen et al., Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola, Alfredsson and Kivimäki2017), we further dichotomized this variable in order to compare high strain jobs to all other categories.
Outcome
Diagnosis of depression is taken from both in-patient and out-patient registers. The in-patient register includes hospitalizations while the outpatient register includes specialist psychiatric care. Visits to primary care are not included in these registers. Cases of depression are defined as those with any diagnosis of depression whether primary or contributing during the follow-up period between 2006 and 2016 using the ICD 10 definition of depression diagnosis (F32 and F33).
Covariates
Highest obtained education was reported in the LISA register from the year 2005. From seven original categories, we categorized this variable as (1) primary and lower secondary school or less (⩽9 years); (2) secondary (10–11 years); (3) upper-secondary (12 years); (4) post-secondary/university, 2 years or less (13–15 years); and (5) more than 3 years of post-secondary/university (>15 years).
Information on birth country and civil status is taken from the LISA register from 2005. The former was dichotomized to reflect whether the individual was born in Sweden or not. The latter was categorized as married/registered partner, divorced/separated partner, and widowed/surviving partner where partner refers to same-sex partners before marriage was legally recognized. Number of children was also taken from the LISA register in 2005 and was categorized as no children, one to two children, three to four children, and more than four children between the ages of 0 and 19. Age is derived from the index person's birth year. Gender was obtained from the individual's current personal registration number.
Previous psychiatric diagnosis was obtained from the in-patient register and was defined as having any psychiatric diagnosis with the ICD codes F00 to F99 before the baseline year of 2005.
Parents' SEP during the index person's childhood was obtained by linking the index person to their parents' census information from 1960, 1970, or 1980 when the index person was between the ages of 5 and 15. Occupational information was taken primarily from the father, but when this information was missing, the mother's occupation was used. The parents' SEP was classified as non-manual employees at a higher level, non-manual employees at an intermediate level, assistant non-manual employees, skilled manual workers, non-skilled manual workers, farmers, or those with no parental occupation reported.
Parents' psychiatric diagnoses were obtained by linking the index person to their parents' inpatient records from 1973 onward. This variable indicates whether either parent had a first-time psychiatric diagnosis prior to age 65.
Statistical analysis
Baseline characteristics of the study population were explored according to gender and depression diagnosis during follow-up and according to the quintile categories of job control and demands.
Cox proportional hazard regression models with age as the underlying timescale were built for men and women separately to estimate hazard ratios and 95% confidence intervals for the associations between exposure to different levels of job control, job demands, and job strain in 2005 and diagnosis of depression during the follow-up period. Person-time was counted from 1 January 2006 until diagnosis of depression, emigration, death, or the end of the follow-up period on 31 December 2016, whichever came first.
Model 1 shows the crude associations with no adjustment for covariates, though age is accounted for as the underlying time scale. Model 2 is adjusted for birth year, birth country, civil status, number of children, previous psychiatric diagnosis, parents' SEP during childhood, and parents' previous psychiatric diagnoses. Model 3 is further adjusted for obtained education and mutually adjusted for job demands and control.
Covariates were chosen because they have been identified as important potential confounders in previous studies (Grynderup et al., Reference Grynderup, Mors, Hansen, Andersen, Bonde, Kaergaard and Kolstad2012; Harvey et al., Reference Harvey, Sellahewa, Wang, Milligan-Saville, Bryan, Henderson and Mykletun2018; Samuelsson, Ropponen, Alexanderson, & Svedberg, Reference Samuelsson, Ropponen, Alexanderson and Svedberg2013; Svane-Petersen et al., Reference Svane-Petersen, Holm, Burr, Framke, Melchior, Rod and Madsen2020) and may theoretically be related to both the occupation that a person has as well as their likelihood of receiving a depression diagnosis. The covariates in Model 2 are related to background and sociodemographic factors determined early in life, while the additional covariates in Model 3 are those likely to be directly related to the work environment.
In order to further investigate whether adjusting for previous psychiatric diagnoses provided adequate and appropriate control for confounding, we performed the same analyses after excluding those with any psychiatric diagnosis prior to baseline rather than adjusting for previous psychiatric diagnoses.
In order to examine whether associations were stronger based on the severity of the outcome, we also looked only at inpatient diagnoses of depression, which are the more severe diagnoses, rather than combining both inpatient and outpatient depression diagnoses. There may also be important gender differences in these different types of service use because women may be more likely to receive outpatient care before the depression becomes severe enough to require hospitalization.
To investigate whether the relationship between job strain factors and depression differed according to age, models were stratified according to three categorized age groups (30–39, 40–49, and 50–60).
Analyses were done using SAS Enterprise Guide 7.1 (SAS Institute, Cary, NC, USA).
Results
Men and women who, at baseline, were younger, born outside of Sweden, unmarried or divorced, lower educated, had a previous psychiatric diagnosis, had parents without a recorded SEP, or parents with a psychiatric diagnosis were more likely to receive a depression diagnosis during the follow-up period (Table 2). Men without children at baseline were also more likely to develop depression during the follow-up period. Online Supplementary Table S1 shows the distribution of covariates according to job control and demands in their quintile categorization. Most notably, low education and pre-baseline psychiatric diagnoses were more common at lower levels of both job control and demands.
Table 2. Baseline covariates according to diagnosis of depression during the follow-up period for men and women
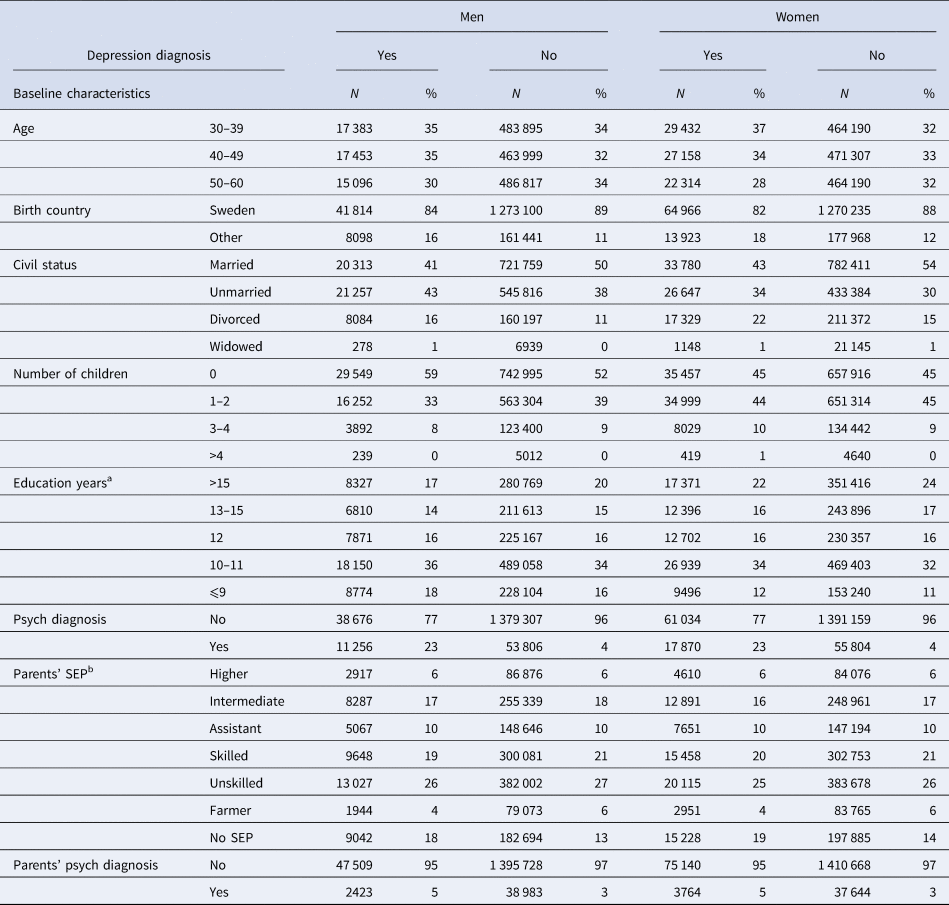
a >15 = more than 3 years of university, 13–15 = less than 3 years of university, 12 = 3 years of upper secondary school, 10–11 = less than 3 years of upper secondary school, ⩽9 = compulsory school or less.
b Socioeconomic position: higher = non-manual employees at higher level, intermediate = non-manual employees at intermediate level, assistant = assistant non-manual employees, skilled = skilled manual workers, unskilled = unskilled manual workers, no SEP = no parental occupation reported.
Around 3% of men and 5% of women received a depression diagnosis during the follow-up period. For men around 22% of these diagnoses came from the inpatient register and for women around 19% were diagnosed in the inpatient register. The rest, 78% and 81%, respectively, came from the outpatient register.
Lower job control was associated with an increased risk of depression among men, and this showed a dose–response relationship, where decreasing job control was associated with a greater risk of receiving a depression diagnosis during the follow-up period (Table 3). Higher demands compared to the lowest category were associated with a slight decrease in the risk of depression. Having a passive or high strain job, compared to having a low strain job, was also associated with an increased risk of depression (HR 1.23, 95% CI 1.20–1.26 for passive jobs and HR 1.26, 95% CI 1.23–1.30 for high strain jobs), while having an active job was associated with a decrease in the risk of developing depression (HR 0.94). High strain jobs compared to all other jobs were associated with an increased risk of depression (HR 1.17, 95% CI 1.15–1.20).
Table 3. Hazard ratios and 95% confidence intervals for risk of depression diagnosis according to job control, job demands, and job strain for men
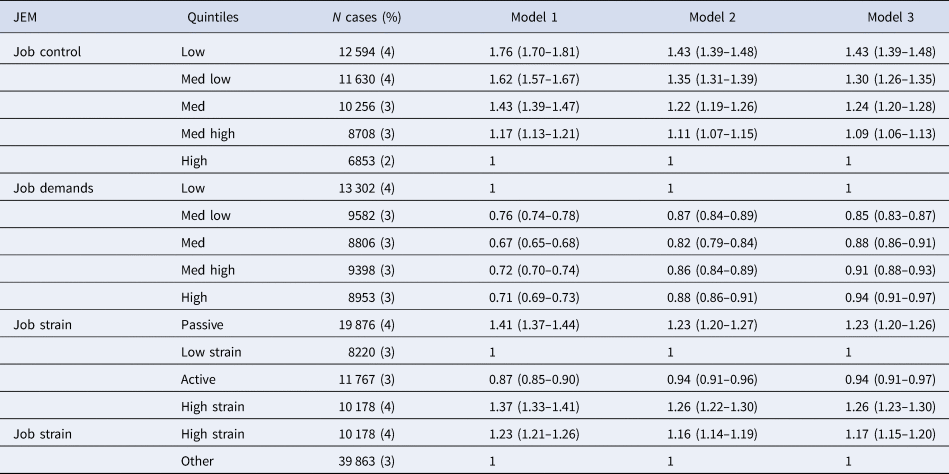
Model 1 is adjusted for age.
Model 2 is adjusted for age, birth year, previous psychiatric diagnosis, civil status, number of children, immigrant status, parents' socioeconomic position, and parents' psychiatric diagnoses.
Model 3 is adjusted for age, birth year, previous psychiatric diagnosis, civil status, number of children, immigrant status, parents' socioeconomic position, parents' psychiatric diagnoses, obtained education, and job control and demands are mutually adjusted.
For women, lower job control was also associated with an increased risk of depression compared to the highest category, but this did not show a dose–response pattern, as the lowest job control category showed a weaker association than the medium-low category (HR 1.27, 95% CI 1.24–1.30 and HR 1.47, 95% CI 1.44–1.51, respectively) (Table 4). Higher job demands compared to the lowest job demands category tended to be associated with a slight decrease in risk for depression, except in the medium-low category. Passive jobs compared to low strain jobs were associated with a slight increase in the risk of depression (HR 1.12, 95% CI 1.10–1.14), while active jobs were associated with a slight decrease in risk (HR 0.84, 95% CI 0.82–0.86), and high strain jobs showed no association. When comparing high strain jobs to all other types of jobs for women, there was a very slight increase in the risk of depression (HR 1.04, 95% CI 1.02–1.06).
Table 4. Hazard ratios and 95% confidence intervals for risk of depression diagnosis according to job control, job demands, and job strain for women

Model 1 is adjusted for age.
Model 2 is adjusted for age, birth year, previous psychiatric diagnosis, civil status, number of children, immigrant status, parents' socioeconomic position, and parents' psychiatric diagnoses.
Model 3 is adjusted for age, birth year, previous psychiatric diagnosis, civil status, number of children, immigrant status, parents' socioeconomic position, parents' psychiatric diagnoses, obtained education, and job control and demands are mutually adjusted.
For both men and women, crude associations were attenuated after adjusting for birth year, previous psychiatric diagnosis, civil status, number of children, immigrant status, parents SEP during childhood, and parents' psychiatric diagnoses, and were generally very slightly further attenuated after additionally adjusting for education, and mutually adjusting for job control and demands.
When analyses were repeated after excluding those with a psychiatric diagnosis prior to baseline, estimates in the adjusted models were similar with only slight variation (online Supplementary Tables S2 and S3).
Using only inpatient diagnosis of depression rather than the combination of both inpatient and outpatient diagnoses resulted in similar associations for men and slightly stronger associations for women for the relationship between job control and depression diagnosis (online Supplementary Tables S4 and S5). The associations for higher demands showed a very slight reduction in risk for men and little change for women. The different categories of job strain were quite similar for both men and women when using only inpatient depression diagnoses compared to both inpatient and outpatient diagnoses.
Stratifying by age group showed virtually no change in the associations (data not shown).
Discussion
In this register-based study of approximately 3 million Swedish workers, we found that for both men and women, lower job control, measured by decision authority at work, was associated with an increased risk of depression during the follow-up period, even after adjusting for pre-baseline psychiatric diagnoses, background sociodemographic factors, and other factors related to the working environment. These associations, however, only showed a dose–response relationship among men. Additionally, having high job demands was associated with a slight decrease in the risk of developing depression during the follow-up period for both men and women. High strain and passive jobs, that is, jobs with low control were associated with an increased risk of developing depression for men, and passive jobs were associated with an increased risk of developing depression for women.
Several previous studies have found a similar relationship between lower job control and a greater risk of depression or common mental disorders (Harvey et al., Reference Harvey, Sellahewa, Wang, Milligan-Saville, Bryan, Henderson and Mykletun2018; Samuelsson et al., Reference Samuelsson, Ropponen, Alexanderson and Svedberg2013; Svane-Petersen et al., Reference Svane-Petersen, Holm, Burr, Framke, Melchior, Rod and Madsen2020). For example, one Danish study reported findings in the same direction when using a JEM measuring job control and registered diagnoses of depression (Svane-Petersen et al., Reference Svane-Petersen, Holm, Burr, Framke, Melchior, Rod and Madsen2020). That study, however, does not allow comparisons of dose–response patterns.
Previous studies have also found consistently different patterns between men and women in terms of the relationship between job strain factors and depression or other common mental health disorders (Cohidon, Santin, Chastang, Imbernon, & Niedhammer, Reference Cohidon, Santin, Chastang, Imbernon and Niedhammer2012; Virtanen et al., Reference Virtanen, Honkonen, Kivimäki, Ahola, Vahtera, Aromaa and Lonnqvist2007; Wieclaw et al., Reference Wieclaw, Agerbo, Mortensen, Burr, Tuchsen and Bonde2008). These associations tend to be weaker among women. That women in the lowest job control category had a lower risk of developing depression than women in the medium-low category is a somewhat puzzling result, though most previous studies do not allow for dose–response comparisons. The lowest job control category for both men and women tended to have a higher proportion of highly educated individuals compared to all other categories besides the highest (online Supplementary Table S1). A closer investigation into the occupations included in the different categories of job control revealed that the lowest category of job control included physicians and a large group of primary school teachers among women, that is, individuals with higher education and perhaps a more prestigious position in society. Women in the medium-low category were almost exclusively lower-level healthcare workers, while men in the equivalent group had a large range of different occupations. Thus, one possible explanation could be that women in the lowest job control category may have a lower risk of depression due to having higher status jobs that require higher education and career planning and women in the medium-low category may have an increased risk of depression due to unmeasured factors related to working in lower-level healthcare jobs. One such factor may be emotional demands (Vammen et al., Reference Vammen, Mikkelsen, Hansen Å, Bonde, Grynderup, Kolstad and Thomsen2016). However, excluding doctors and primary school teachers did not result in a different pattern of association.
Gender differences in depression are persistent and universal with depression being more common in women (Steel et al., Reference Steel, Marnane, Iranpour, Chey, Jackson, Patel and Silove2014). Women may be disproportionately exposed to additional risk factors for depression that are unrelated to the characteristics of the working environment. Thus, depression cases are more evenly spread across different levels of education and different occupations among women compared to men. If these additional depressions are in fact related to something other than the psychosocial work environment, then we would indeed expect weaker associations among women. Though no single factor has been found to explain the gender difference in depression, it has been suggested that this may be partially explained by women more often being exposed to stressful life events and important differences in physiological as well as emotional reactions to stress (Nolen-Hoeksema, Reference Nolen-Hoeksema, Gotlib and Hammen2002).
That higher job demands were not associated with an increased risk of developing depression deviates from the expectation based on the theoretical model of job strain (Karasek, Reference Karasek1979). However, several previous studies which also use JEM or other aggregated measures of job demands show null results (Cohidon et al., Reference Cohidon, Santin, Chastang, Imbernon and Niedhammer2012; Grynderup et al., Reference Grynderup, Mors, Hansen, Andersen, Bonde, Kaergaard and Kolstad2012) or results similar to our own, suggesting a decrease in the risk of depression when job demands are higher (Samuelsson et al., Reference Samuelsson, Ropponen, Alexanderson and Svedberg2013; Wieclaw et al., Reference Wieclaw, Agerbo, Mortensen, Burr, Tuchsen and Bonde2008). Podsakoff, LePine, and LePine (Reference Podsakoff, LePine and LePine2007) also make a distinction between challenge stressors and hindrance stressors in the workplace, where the former gives an opportunity for development and the latter relates to issues such as role conflict and employment insecurity. It may be that jobs classified as having high demands in our study benefit individuals through challenges and opportunities, and thus may be related to a decreased risk of depression. Two high-quality population-based cohort studies reported opposite findings. That is, higher demands were associated with a greater risk of depression (Harvey et al., Reference Harvey, Sellahewa, Wang, Milligan-Saville, Bryan, Henderson and Mykletun2018; Virtanen et al., Reference Virtanen, Honkonen, Kivimäki, Ahola, Vahtera, Aromaa and Lonnqvist2007). These studies, however, relied on individuals to report their own experience of job demands. The individual experience of job demands has been found to be strongly affected by reporter bias and to overestimate associations (Kolstad et al., Reference Kolstad, Hansen, Kaergaard, Thomsen, Kaerlev, Mikkelsen and Bonde2011). Thus, what is captured on an individual level may reflect differences in personality, working style, and depressive disposition.
Two important meta-analyses have reported overall associations between job strain and depression which were higher than what we found in the present study (Madsen et al., Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola, Alfredsson and Kivimäki2017; Theorell et al., Reference Theorell, Hammarstrom, Aronsson, Traskman Bendz, Grape, Hogstedt and Hall2015). The summary odds ratio in a meta-analysis conducted by Theorell et al. (Reference Theorell, Hammarstrom, Aronsson, Traskman Bendz, Grape, Hogstedt and Hall2015) was 1.74 (95% CI 1.53–1.96). In a meta-analysis by Madsen et al. (Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola, Alfredsson and Kivimäki2017), the summary risk ratio was 1.77 (95% CI 1.47–2.13). However, when the latter included only unpublished datasets using hospital diagnosis of depression rather than diagnostic interviews, the summary risk ratio was lower (RR 1.27, 95% CI 1.04–1.55). That job control is the more important and driving force of the job strain model has been postulated in relation to coronary heart disease as well as depression (Ingre, Reference Ingre2015; Mikkelsen et al., Reference Mikkelsen, Andersen, Bonde, Hansen, Kolstad and Thomsen2018) and has been debated among experts (Kivimäki et al., Reference Kivimäki, Nyberg and Kawachi2015). Specifically, using quadrants or a dichotomous measure to represent job strain has been criticized as being uninformative as these associations can be driven by only one of the factors in these combined categories. Furthermore, there is evidence supporting job control alone as a more important predictor of depression and little evidence for an interaction between control and demand (Mikkelsen et al., Reference Mikkelsen, Andersen, Bonde, Hansen, Kolstad and Thomsen2018; Theorell et al., Reference Theorell, Hammarstrom, Aronsson, Traskman Bendz, Grape, Hogstedt and Hall2015). Our separate analysis of job control and job demands, as well as the more extensive four-category job strain categorization including passive jobs, also reveals that on the aggregated level, job control appears to be the more important predictor of depression.
Strengths of this study include the large sample size encompassing legally working individuals between the ages of 30 and 60 during 2005 in the Swedish population. This substantially reduces bias due to selection and attrition, which some previous studies have been criticized for (Choi et al., Reference Choi, Schnall, Landsbergis, Dobson, Ko, Gómez-Ortiz and Baker2015). That the psychosocial workplace environment was measured independently of the index person using JEM measures is also a strength that provides better evidence for a causal interpretation. Additionally, the use of patient registers for defining depression diagnoses is also a more objective measure than relying on self-report. Furthermore, the patient registers allowed for the possibility to account for those with a previous psychiatric diagnosis prior to baseline. The ability to link the index person to their parents in order to obtain information on SEP during childhood and parents' psychiatric diagnoses was also a strength. Finally, that we found similar associations when only considering the more severe inpatient diagnoses of depression shows that our results were not sensitive to the type and severity of depression diagnosis.
This study is not without its limitations. First, though the use of JEM scores allows for a more independent measure of the workplace psychosocial environment, they do not consider inter-individual variation in exposure levels within particular occupations. In other words, the JEM scores serve as an aggregated experience for people within their occupations, but do not necessarily reflect the work environment that the index person experiences themselves. Second, though patient registers are rather objective measures of depression diagnosis, they only capture more severe cases including those who get hospital or specialized treatment and miss milder untreated cases or cases treated in primary care. It is important to note, however, that this Swedish healthcare system is tax-funded with limited financial barriers for care-seeking. Furthermore, there are no validation studies, to our knowledge, of depression diagnoses in the Swedish patient registers, though these registers have been found to have high coverage of psychiatric diagnoses in general (Ludvigsson et al., Reference Ludvigsson, Andersson, Ekbom, Feychting, Kim, Reuterwall and Olausson2011). Further studies evaluating depression diagnoses in the Swedish patient registers are needed. Third, psychiatric diagnoses for both the index person and their parents were only available after 1973. Thus, pre-baseline psychiatric diagnoses for the index person and parents' diagnoses prior to 1973 would be missed. However, later diagnoses can arguably be used as a proxy for earlier psychiatric problems. Fourth, as with all observational studies, there is a risk for residual confounding. There may be particular differences within psychosocial workplace environments that are also differently related to depression diagnosis that we did not account for. Fifth, Sweden and the other Nordic countries have unique labor market and social welfare policies which may make it difficult to directly generalize the results to other countries or regions. Finally, using one baseline measure of job exposure, while more comparable to previous studies, does not address accumulation or change in occupational exposures over time, which was beyond the scope of the present study.
That lower job control is associated with an increased risk of developing depression is an important finding for future interventions aiming at improving job control or finding other ways to support those with low control jobs with the potential to improve mental health. A synthesis of systematic reviews found that the best evidence indicated that multi-dimensional interventions aimed at decreasing job demands and increasing job control tend to be related to less absenteeism, financial benefits, and increased productivity or performance, but concluded with the need for more research on interventions targeting job control (Williams-Whitt et al., Reference Williams-Whitt, White, Wagner, Schultz, Koehn, Dionne and Wright2015).
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S003329172100060X
Financial support
This research is supported by the Swedish Research Council for Health, Working Life, and Welfare Forte grant number 2019-01249 and 2016-07185.
Conflict of interest
None.







 Open access
Open access