

Introduction
Within Astley Cooper’s archive at the Royal College of Surgeons of England is a file collated by his nephew, Bransby Cooper.Footnote 1 After Astley’s death in 1841, Bransby assumed responsibility for preparing his uncle’s biography and, in the course of his research, wrote to a number of Astley’s friends and associates, particularly those who had known him in his youth, in order to solicit anecdotes and reminiscences illustrative of the great man’s character. One of the responses he received was from Samuel Sherrington (1776–1845), who had attended school in Brooke, the small village just to the south of Norwich where Astley’s father, the Rev. Samuel Cooper (bap. 1739, d. 1800), then occupied the manor house. In Bransby’s two-volume biography of his uncle, published in 1843, he quotes at length from Sherrington’s letter, including his account of first meeting Astley. According to Sherrington, one of his schoolmates had seized the hat of another pupil and thrown it into a nearby pond: ‘The boy, lamenting the loss of his hat, and fearing he should be punished for his absence from school, was crying very bitterly’ when along came the young Astley, dressed in a ‘scarlet coat, a three-cocked hat […] and white silk stockings – his hair hanging in ringlets down his back’. Seeing the boy’s tears, Astley strode into the pond and fetched his hat, emerging with his fashionable attire soaking wet and caked in mud ‘much above his knees’. As Sherrington writes, he and Astley fell into conversation and ‘from that period he seemed to have taken a fancy to me, and selected me as his companion. We were both of us frolicsome, mischievous boys and played many pranks together in the village’.Footnote 2
If Bransby was happy to relate this story of the dashing young Astley, suggesting as it did his inherent sympathy with the distresses and misfortunes of others, he was somewhat more circumspect with another of Sherrington’s anecdotes. In fact, he passed over this story, which saw the two friends ‘engaged against a tailor in the village, to whom Astley owed a slight grudge’, in some haste, claiming that ‘in the detail […] of the principal event, – an attack upon the poor man’s windows, – there is nothing worthy of publication, nor characteristic of my uncle, excepting proof of the natural kindness of his disposition, from his having subsequently […] remunerated him for the fright and injury to which he had been subjected’.Footnote 3
Clearly, Bransby Cooper was keen to manage his uncle’s posthumous reputation: to ensure that his narrative of Astley’s transformation from, in his father’s words, a ‘sad rogue’ into a ‘shining character’ accorded with the morally edifying ideal of Romantic Bildung, and that any account of Astley’s youthful misbehaviour was balanced by a clear demonstration of his heartfelt sensibility.Footnote 4 To that end, it might seem peculiar that Bransby chose to quote quite as extensively as he did from another letter in the archive, this one sent by Peter Holland (1766–1855), an ‘intimate associate’ of Astley during his time as a surgical apprentice, when both boys lived in the house of Henry Cline. According to Holland:
During this time Astley, who was always eager to add to his physiological and anatomical knowledge, made a variety of Experiments on living animals. I recollect one day walking out with him when a dog followed us […] home, little perceiving the fate that awaited him. He was confined for a few days till [Astley] had ascertained that no owner would come to claim him – He was then brought up to be the subject of various operations. The first of these was the tying one of the femoral arteries. When poor Chance – for so we named the dog, was sufficiently recovered from this, one of the humeral arteries was subject to a similar process. After the lapse of a few weeks the ill-fated animal was shot, the vessels injected and preparations were made from each of the limbs.Footnote 5
Aside from substituting the word ‘killed’ for the specific (and perhaps more brutal) ‘shot’ in his description of the poor dog’s fate, Bransby reproduced this anecdote almost verbatim in his published biography.Footnote 6 And yet this brief reference to the young Astley’s practice of vivisection necessitated a two-page apologia, lest its inclusion ‘lead those, who are unconscious of its necessity, to attribute a disposition devoid of feeling to my uncle and his friend’. ‘In order to remove such an impression’, Bransby continued, ‘it becomes incumbent on me to say a few words on the advantages which this source of knowledge alone offers, and the consequently necessary sacrifice of our feelings in embracing them’.Footnote 7
Vivisection was not the only unsavoury activity that Bransby chose to address in his biography. Another anecdote, also taken from Holland, involved the dissection of cadavers in Cline’s house, away from the ‘common dissecting room’ of St Thomas’ Hospital. One day, Holland claims, he and Astley were ‘busily engaged with a subject on the table’ when they noticed several men, who had been replacing some tiles on the building opposite, ‘eagerly watching our operations’ through the window. ‘At that time’, he notes, ‘a mob was readily collected in the streets’ and so they ‘thought it prudent to convey our subject into a more private part of the house’.Footnote 8 Holland makes no specific mention of the fact that these bodies were illicitly acquired, but the implication is clear enough. Indeed, the last three chapters of the first volume of Bransby’s biography are entirely dedicated to those ‘Resurrection Men’ who supplied Astley, and others like him, with the disinterred corpses of the poor.Footnote 9
Both vivisection and anatomical dissection were highly contentious issues at the height of Astley Cooper’s career in the 1820s. In June 1825, for example, the recently founded Society for the Prevention of Cruelty to Animals held a meeting at the Crown and Anchor on the Strand to consider the issue of animal experimentation. Several testimonies from leading London surgeons were read out and, while all acknowledged what John Abernethy called ‘the unwarrantableness of such experiments, unless to determine some important question’, opinion varied from Everard Home’s conviction that ‘the Lord has blessed his creatures for our use’ to Charles Bell’s incredulity that ‘Providence should intend that the secrets of nature are [to] be discovered by means of cruelty’. Others were even less equivocal. Bell’s fellow Paleyite, the Oxford professor John Kidd (1776–1851), questioned ‘whether anyone can habitually inflict pain on even a brute, without impairing that sensibility, for the possession of which we ought to be most thankful’. Philip Crampton (1777–1858) likewise argued that ‘The natural feelings of commiseration which we entertain for the sufferings of a helpless and inoffensive animal, are entwined with the best and tenderest sympathies of our nature’ and ‘we cannot part with the one without tearing up the others by the very roots’.Footnote 10 As Rob Boddice has demonstrated, the moral and emotional politics of vivisection were vociferously contested throughout the century, and for Bransby Cooper, writing in the early 1840s, the use of animals in physiological experiment clearly remained a highly sensitive topic, requiring extensive justification.Footnote 11 By contrast, the issue of anatomical dissection was, by this time, seemingly settled. ‘When the dead can be rendered subservient to the most important interests of the living, however much humanity may shudder at the idea of a beloved relative being disturbed from the stillness of the tomb’, Bransby asked, ‘who is there that would not sacrifice those feelings of repugnance, which, though so common, in truth can […] be traced only to selfish motives?’Footnote 12
That Bransby Cooper was willing to address issues such as vivisection and grave-robbing in a biography ostensibly concerned to present his uncle as a gentleman of exquisite feeling suggests something about the contours and boundaries of sentiment and sensibility in relation to surgery, the shifting delineations of which are the subject of this chapter. The first half of this book has been concerned to demonstrate the extent to which the emotional regime of early nineteenth-century surgery was shaped by the cultures of Romantic sensibility and defined by an idealised emotional intersubjectivity between surgeons and their patients. In Chapter 4, we considered how those cultures of sensibility and sentiment were ‘weaponised’ by radical reformers in an effort to undermine the political hegemony of the metropolitan surgical elites. In this chapter, we shall continue our exploration of the ambiguities of surgical emotion by charting the beginnings of a shift, whereby the appropriateness of feelings such as sympathy and pity, as well as their imagined objects, came to be questioned and, ultimately, reconfigured. We shall do this by focusing on two key moments in surgical history, separated by some twenty years. They are, firstly, the debates surrounding the practice of anatomical dissection that came to the fore in the 1820s and culminated in the passage of the Anatomy Act in 1832, and, secondly, the introduction and early use of inhalation anaesthesia in the later 1840s. Both have extensive historiographies of their own, but they have rarely been examined together, let alone treated as cognate phenomena. Indeed, they could hardly be viewed more differently. One is regarded, generally speaking, as a political assault upon the dignity and rights of the poorest in society, while the other, despite waves of more nuanced scholarship, retains its status as a triumphant moment of scientific discovery: a deliverance from pain and suffering that marks the birth of modern surgery.Footnote 13 However, what connects these two episodes is the process by which the ‘emotional object’ at the heart of the Romantic surgical encounter, namely the body, either as the writhing, anguished agent of an agonised consciousness or as the object of professional pity, sympathy, and emotional self-reflection, came to be silenced: rendered quiescent and subservient to a more abstract emotional logic.Footnote 14 More specifically, what also unites them (and, indeed, the period as a whole) is the powerful political, cultural, and ideological influence of utilitarianism, the consequentialist moral philosophy propounded by Jeremy Bentham (1747–1832) and his acolytes, whose ideas about the social good allowed early nineteenth-century medical practitioners to reimagine the relations between ‘knowledge, expertise and civil and state governance’.Footnote 15
At one level, the influence of utilitarianism could hardly be more widely acknowledged than in the literature on the Anatomy Act. Ruth Richardson’s pioneering account, Death, Dissection and the Destitute (1987), presents the utilitarians and their Parliamentary advocates, particularly Henry Warburton (1784–1858), as the prime movers behind the Act. And yet, while Richardson acknowledges the vital role played by surgical interests in pushing for legislation, she does not explore the ideological dimensions of early nineteenth-century surgery in especially close detail, nor does she consider the influence of utilitarianism on surgical culture more generally. Indeed, within her analysis, surgery is, to borrow the Latourian concept, ‘black-boxed’, its internal dynamics reduced to broad characterisation (even caricature).Footnote 16 This is a corollary of Richardson’s underlying belief that, for all surgeons stood to gain from the Act, it was not fundamentally a piece of surgical legislation but rather ‘a class reprisal against the poor’, which only ‘incidentally […] endorse[d] the respectability of scientific medicine’.Footnote 17 Without seeking to contest the general point about the social, political, and humanitarian implications of utilitarian thought, it is clear that Richardson’s approach mirrors that of E. P. Thompson, especially his ‘rationalist’ conception of social relations, wherein the ‘emotional’ appeal of charismatic preachers like Joanna Southcott is rendered ‘delusional’ in the very same sentence as his celebrated rejection of historical ‘condescension’.Footnote 18 Such tendencies are similarly evident in Richardson’s treatment of emotion, which features prominently, yet obliquely, in her book. She acknowledges that ‘The Anatomy Act was an emotive issue’ and she regularly situates the cold rationalism of utilitarianism in opposition to ‘popular sentiment’ surrounding the corpse.Footnote 19 However, she regards all discussion of ‘feeling’, especially when deployed by Parliamentary proponents of the Act, as a mere cover for ‘real’ economic and political motives.Footnote 20 Pitting callous liberals against the persecuted poor in a morally unambiguous class war, she views emotions as ‘valid’ or ‘authentic’ only when deployed by (or, more commonly, on behalf of) the potential ‘victims’ of the Act. Hence surgeons, who are as much the villains of the piece as their political allies, are, in emotional terms, entirely defined by the idea of clinical detachment, and their appeals to feeling either ignored or dismissed as inherently cynical and disingenuous.Footnote 21
As we have seen, the monolithic and transhistorical concept of clinical detachment does little to explain the emotional cultures of Romantic surgery. And, as we shall see in this chapter, it likewise does nothing to capture those shifts in the emotional regime of surgery that were underway in the 1820s and that were exacerbated by the debates around anatomical dissection. In Chapter 4, we saw that the 1820s and early 1830s witnessed what we might call the crescendo of surgical sentiment when, in pursuit of specific political ends, surgical reformers invested the bodies of surgical patients with heightened emotional significance, publicising their sufferings and deaths in order to provoke pity, outrage, and anger. And yet, at precisely the same moment, many of those self-same reformers were seeking to divest other bodies, namely dead bodies and, more especially, the dead bodies of the poor, of much of their emotional significance, presenting them as a corporeal terra nullius that might be appropriated for the education and edification of surgeons and their pupils. There was no inherent contradiction in this position. Indeed, sympathy for the patient’s sufferings, and a desire to alleviate their plight, was not infrequently invoked as the very reason why that same patient’s body might cease to have any emotional meaning at the moment of their death. However, what was of profound and lasting significance for the emotional cultures of surgery was the way in which the feelings of the individual, once the principal nexus of the surgical ideal, were subordinated to an abstract conception of the social good. This act of sublimation is clearly evident in Bransby Cooper’s appeal to emotional sacrifice, as are its utilitarian roots. But what is instructive about this example is that Cooper was no utilitarian and neither were many of those surgeons who advocated for the appropriation of ‘unclaimed’ bodies from hospitals and workhouses. Indeed, one of the great ironies of the Anatomy Act is how pervasive such rhetoric was even among the most conservative of surgical commentators, while those who were more closely aligned with the utilitarian political agenda often found it hardest to reconcile themselves. Hence, while the Anatomy Act was hugely important in shifting the emotional focus of surgery away from the individual and towards the social, it was by no means a straightforward process, not only, as we shall see, because utilitarians often made appeals to emotion themselves, but also because those contortions of logic that sought to render the dead bodies of the poor uniquely free of emotional association only served to enhance their pathos.
By contrast with the practice of surgical anatomy, the role of utilitarianism is somewhat less well acknowledged in the scholarship on anaesthesia. To be sure, in his ground-breaking revisionist history of anaesthesia in the United States, Martin S. Pernick frequently uses the term ‘utilitarianism’ and invokes a form of reasoning reminiscent of Bentham’s famous ‘felicific calculus’. However, Pernick’s conception of utilitarianism is more akin to a pragmatic process of clinical decision-making than to an historically contingent and contextually specific moral philosophy or cultural ideology.Footnote 22 Stephanie Snow, meanwhile, has notably less time for utilitarianism in her account of the development of anaesthesia in the United Kingdom, and the same is true for Bourke and Moscoso in their respective histories of pain.Footnote 23 This is perhaps surprising, given Bentham’s explicit identification of pain as ‘in itself an evil; and, indeed, without exception, the only evil’.Footnote 24 One of the few historians to make a firm connection between utilitarianism and the advent of anaesthesia is Christopher Lawrence, in a relatively obscure article from 1997.Footnote 25 This chapter takes up Lawrence’s suggestive reasoning, arguing that utilitarianism was as implicit in the making of anaesthesia as it was explicit in the making of the Anatomy Act. I say implicit, because few commentators of the period necessarily identified Bentham or his philosophy by name in decrying the pain of operative surgery or imagining its abolition. But that, I contend, is because, from around the time of the debates surrounding anatomical dissection, utilitarian values had become so deeply embedded in medical and surgical thinking, as well as in much social and political thought more generally, that they hardly required identification. Having said this, the place of pain in surgical culture was not necessarily a straightforward or clear-cut one, as historians of anaesthesia have recognised.Footnote 26 The same, as we shall see, was true of the emotional and intersubjective qualities of surgery in the years immediately before and after the advent of anaesthesia. Indeed, while this chapter seeks to demonstrate the ways in which the operative subject was culturally and emotionally silenced by the practice of anaesthesia, rendered a quiescent pseudo-presence in the operating theatre, it is important to recognise that this process was, in common with the debates surrounding anatomical dissection, replete with complexity and ambivalence. Indeed, one of the principal purposes of my argument is to demonstrate how, as with anatomical dissection, the figure of the anaesthetised patient as a de-emotionalised object, akin to a corpse or, more palatably perhaps, a person asleep, had to be made, forged from a set of messy, complex, and culturally problematic associations with other ‘altered states’. Moreover, as well as considering how the patient was emotionally and culturally reconfigured by the advent of anaesthesia, the chapter also explores its implications for surgical identity and self-presentation, ultimately demonstrating how anaesthesia paved the way for a techno-scientific conception of surgery in which the thoughts, feelings, and experiences of the individual patient were subordinated to a more abstract ideological rationale as the emotional regime of Romantic sensibility gave way to one of scientific modernity.
This argument about the switch of emotional focus from the individual to the broader social good has clear parallels with Boddice’s arguments about later nineteenth-century vivisection, vaccination, and eugenics. Indeed, at one point in The Science of Sympathy (2016), Boddice digresses into a brief discussion of anaesthetics and surgery, although he posits an opposition between the surgeon caring for the individual patient and the vivisecting physiologist ‘whose operations were for the good of everybody’.Footnote 27 As we shall see in this chapter and, more especially, Chapter 6, such observations could increasingly be made of surgeons too. This chapter therefore bears out Boddice’s argument about the shifting terrain of scientific sympathy. However, whereas Boddice is concerned to locate this shift within a post-Darwinian discourse, and presents a somewhat two-dimensional characterisation of the emotional cultures of the Romantic era, this chapter demonstrates the importance of the period from the 1820s to the 1850s, at least as concerns the practice of surgery, and argues for the ideological significance of utilitarianism, of which Boddice is generally dismissive.Footnote 28
There are also parallels, albeit somewhat slighter, between my argument and that of William Reddy, who suggests that the displacement of sentimentalism by ‘liberal reason’ and ‘Romantic passions’ in Restoration France provided for a more ‘stable’ emotional regime.Footnote 29 I make no such claims for the stability or otherwise of the two emotional regimes at work here, namely those of Romantic sensibility and scientific modernity. For one thing, there was evidently a greater continuity between sentimentalism and Romanticism in Britain than in France, where the former became so closely intertwined with the fervid political cultures of the Revolution. Nor do I completely share Reddy’s opinion that Romanticism relegated sentiment to ‘a private realm of personal reflection, artistic endeavour, and interior, noncivic spaces’.Footnote 30 After all, we have already seen the extent to which sentiment shaped interpersonal relations and political discourse within Romantic surgical culture. Most importantly of all, however, while Reddy is inclined to downplay the persistence of sentiment within his own schema, I think it is important to acknowledge the inconsistencies and incompleteness of the transition from one emotional regime to another.Footnote 31 As we shall see, neither utilitarian rationalism nor anaesthetic oblivion entirely eliminated emotional intersubjectivity between surgeon and patient. Nor did they end the discourse of sentiment in surgery. What they did do was lay the groundwork for a surgical identity whose social and moral authority derived less from emotional authenticity than from techno-scientific rationality.
The ‘Struggles of Natural Feeling’: Emotions and the Dead
Of all John Bell’s pupils, John Lizars (1791/2–1860) was perhaps the most closely formed in his master’s image. Born shortly after Bell opened his Edinburgh anatomical school, and three years before he published his Discourses on the Nature and Cure of Wounds (1795), he was only 5 or so when Bell treated the wounded from the Battle of Camperdown (1797).Footnote 32 And yet, such was the duration of the French wars, combined with the youth of contemporary surgical initiates, that he completed his apprenticeship in time to gain his own experience of wartime surgery, serving aboard a frigate off the Iberian Peninsula from 1810 to 1814. Like Bell, Lizars was renowned as a ‘bold and accomplished operator’, the first Scottish surgeon to excise the upper jaw and the first British surgeon to perform an ovariotomy.Footnote 33 Like Bell, he was also a master anatomist and the author of a beautifully illustrated and highly regarded anatomical work in five volumes, published between 1822 and 1826. The second volume of this work opens with Lizars quoting from his former master, who had died only three years before. ‘When I began the First Part of this Work’, he writes, ‘I little thought that I should live to witness the sentiments of my late worthy preceptor Mr John Bell so completely verified’. These sentiments, originally published in 1794, were that Edinburgh had become a place ‘where it is not praise-worthy, but even dangerous to propose dissections’.Footnote 34 ‘When I read this in my early years of study’, Lizars continues, ‘I conceived it to be the sentiment of a disappointed man, and never dreamt that this literary city, and this enlightened age, would endeavour to suppress a study which has been universally allowed to form the basis for all surgical and medical science’.Footnote 35
As Lawrence has shown, anxieties about the declining importance of Edinburgh as a centre for medical and surgical education stretched back to the time when Bell was writing in the 1790s, but they were becoming increasingly pronounced in the 1820s when Lizars could imagine that ‘the City of Edinburgh, which has extended its fame for literature, philosophy, and medicine, to the most distant regions of the earth, is doomed to dwindle into comparative insignificance’.Footnote 36 The reason for this decline, according to Lizars, was the rise of a ‘miserable prejudice’, a tide of ‘ignorance, bigotry and superstition’ by which the authorities, in their ‘zeal, that bodies should remain undisturbed in their progress to decomposition’, had ‘laboured to destroy […] that art, whose province it is to free living bodies from the consequences [of] accident and disease’.Footnote 37 Lizars was one of the earliest surgeons to publicly express his concerns about the increasing practical and legal difficulties of acquiring subjects for anatomical dissection, but he was not quite the first. That distinction is often accorded to John Abernethy who, in his Hunterian Oration of 1819, drew inspiration from continental European practices, most notably those of post-Revolutionary France, to suggest that either ‘the body of any person dying in [public] institutions, unclaimable by immediate relatives’, or, at a push, ‘the body of any person of whatsoever rank or fortune, unclaimable by immediate relatives’, should be subject to dissection.Footnote 38
The history of grave-robbing and anatomical dissection is too well known to warrant extensive repetition here. Suffice it to say that, while the practice of exhuming bodies for the purposes of dissection was of long standing, the marked expansion in anatomical education discussed in Chapter 4, and the move away from anatomical demonstration towards hands-on dissection initiated by the Hunters, Bells, and others, saw an increased demand for cadavers in the later decades of the eighteenth and early decades of the nineteenth century. This was a demand that could not be met by the legal provisions of the Murder Act of 1752, which allowed for the public dissection of hanged felons.Footnote 39 As Lizars’ lament suggests, the shortage of bodies in Edinburgh was particularly acute and encouraged attempts to import cadavers from Ireland, where they were more readily obtainable. But even in London, the situation by the early 1820s had become untenable. As we heard in the previous chapter, in his testimony to the 1828 Select Committee on Anatomy, Astley Cooper estimated that around 700 pupils attended one or more of the anatomy schools in the metropolis and, by Warburton’s calculations, these students required access to at least 2,000 bodies each year.Footnote 40 Various estimates were given by contemporaries as to the number of cadavers available via statutory means, but as records suggest that only 25 people were executed for murder in London between 1800 and 1820 (some 29 per cent of the 87 sentenced to death at the Old Bailey), this provided, on average, just over one body a year.Footnote 41
As a result of this demand, the early nineteenth century saw the rise of a commercial trade in grave-robbing to supply bodies to the anatomy schools. In turn, this encouraged greater vigilance on the part of families and parish authorities, particularly in places like Edinburgh, making bodies harder to obtain and raising their price. According to Cooper, the price per body in London had risen from two guineas at the time of his first entry into practice in the 1790s to eight guineas by 1828 and, in times of especial privation, had reached as much as fourteen.Footnote 42
The legal status of this trade was not entirely clear. As corpses had no monetary value in English law, disinterring them was not technically theft. The case of Rex v. Lynn in 1788 had established that it was a misdemeanour, contra bones mores, to carry away a body from a churchyard for the purposes of dissection, and surgeons could be charged as accessories to that offence. Meanwhile, the case of Rex v. Young had seen the master of a workhouse, a surgeon, and another party convicted of conspiracy for preventing the burial of a former inmate.Footnote 43 However, such prosecutions were rare and most surgeons were unaware that their actions contravened the law in any way, at least until 1828, when a jury at the Lancaster Assizes found two students guilty of a misdemeanour for possessing the body of one Jane Fairclough.Footnote 44
Such were the economic, pedagogical, and legal circumstances of the early 1820s that encouraged practitioners to imagine a new system whereby a regular supply of cadavers might be provided by the state. As has been argued elsewhere, such imaginings were an early expression of the reformist impulse in medicine and surgery, whereby the interests of the profession and those of the state were figured as increasingly congruent, and by which a rhetoric of decline was harnessed to an ideology of progress.Footnote 45 The varied configuration of these imaginings serves to illuminate the emotional regime of surgery and its shifting norms. Hence, what is notable about Lizars’ and Abernethy’s early contributions to the debate is how tentative they seem in comparison to other, later projections. Lizars was perhaps too coy to propose anything concrete in the preface to his second volume of A System of Anatomical Plates (1823).Footnote 46 He even suggested that his work might ‘form some substitute’ for access to real bodies, something that was, in principle, roundly refuted by later commentators.Footnote 47 Meanwhile, Abernethy’s early advocacy for a French-style system of institutional supply was hedged by a desire to give ‘no offence to common decency and humanity’. ‘[B]etter would it seem to me’, he claimed, ‘that medical science should cease, and our bodily sufferings continue, than that the natural rights and best feelings of humanity should not be equally respected in all classes of society’.Footnote 48
And yet, at the same time, these early interventions set the template for much subsequent debate, not least by the way in which they appealed to a higher emotional register, pitting heartfelt professional and patriotic sentiment against vulgar and indulgent popular sentimentality. As a former naval surgeon, Lizars was in a particularly strong position to do this, drawing on his wartime experiences to evoke the frisson produced by imagining the practical consequences of anatomically deficient physicians and surgeons:
Who does not shudder when he thinks of the number of young medical gentlemen who, after a year or two of grinding, obtain a degree or a diploma, and who thus, ignorant of the very elements of their profession, annually go to the East and West Indies, and to the army and navy, where they have the charge of hundreds of their suffering fellow-creatures[?] Little are these individuals aware of the fearful responsibility which awaits them in the hour of sickness, or on the field of battle; and little do the public think that they are the instruments of such cruelty and murder.Footnote 49
If neither Lizars nor Abernethy offered a substantive proposal for a system of cadaver supply, it was not long before someone did. That man was William Mackenzie (1781–1868), a Scottish surgeon who had attended Abernethy’s lectures at St Bartholomew’s Hospital in the later 1810s and who, by the mid-1820s, was Professor of Anatomy and Surgery at Anderson College in Glasgow. In 1824, the year after Lizars’ lament, he published An Appeal to the Public and the Legislature on the Necessity of Affording Dead Bodies to the Schools of Anatomy, by Legislative Enactment. This thirty-six-page pamphlet was the first sustained intervention into the emerging debate on the acquisition of anatomical subjects and the first comprehensive proposal for legislative reform. It is notable for many things, not the least of which was the emphasis it placed on surgical anatomy. That surgeons were the professional constituency most directly interested in these matters was implicit in much of the discussion surrounding the practice of anatomical dissection. Even so, anatomy encompassed a range of meanings, including the kinds of demonstrative instruction sufficient for would-be physicians, and it was these forms that allowed opponents to claim that access to bodies might be supplemented, or even supplanted, by illustrated plates, wax models, and other simulacra.Footnote 50 For Mackenzie, however, anatomy was of a different order of importance for surgeons, because in order to operate successfully, and with confidence, on a living patient, it was necessary, as John Bell had argued, to have an intimate, ‘practical acquaintance’ with the human body. ‘No doubt’, Mackenzie wrote, ‘there is a manual address in the performance of surgical operations, which actual practice only can give; but it is evident that practice on the living ought, from the very first, to be under the guidance of a clear and well-understood system of rules, which the surgeon has already put to the test […] on the dead body’.Footnote 51
Needless to say, providing multiple bodies to each and every student would require a far more extensive system of procurement than was necessary for demonstrative purposes only. In order to convince his readers of the necessity for such provision, therefore, Mackenzie drew upon the cultures of Romantic surgical intersubjectivity to evoke sympathy for the prospective plight of both patient and surgeon. Thus, he conjured the spectre of ‘a man tormented with the stone’ whose ‘excruciating sufferings’ and ‘anguish’ could not be ‘adequately’ described, and only alleviated by skilful surgical intervention. Likewise, he imagined the embodied experience of the ill-prepared surgeon as he confronts his operative subject: ‘his hand trembles, and his heart fails, he hears the frightful cries of his victim, and sometimes sees him expire under his hand’.Footnote 52
As we have already seen, such imaginings were typical of Romantic surgical discourse, and owed much to the influence of John Bell. However, rather than simply functioning as a demonstration of the profound sensibility, and hence cultural credibility, of the surgeon, Mackenzie’s appeal to emotion was explicitly intended to counter, and ultimately displace, another set of emotional associations, namely those attached to the bodies of the dead. From the very beginning of his pamphlet, Mackenzie asserted surgery’s status as a social good.Footnote 53 Hence, while he acknowledged the ‘struggles of natural feeling’ that might result from supplying surgeons with ‘unclaimed’ bodies, he maintained that ‘the subject is of the deepest interest to humanity […] almost too deep indeed to admit of personal feelings’.Footnote 54 By figuring the emotional regime of surgery as commensurate with the interests of ‘humanity’, Mackenzie was able to dismiss opponents of anatomical dissection as ‘worshippers of ignorance’ indulging in ‘idolatry of the dead’ who should ‘listen to reason, not to passion’.Footnote 55
Despite Mackenzie’s contrast between ‘reason’ and ‘passion’, he did not seek to exclude emotion from the debate. Rather, he intended to sublimate ‘personal feelings’ into a higher emotional logic. In so doing, however, he figured certain feelings as valid and others as invalid, discriminating between authentic sentiment and what he called the ‘mask of tender-heartedness’.Footnote 56 This concern with inauthentic sentiment, or sentimentality, had its roots in later eighteenth-century debates about the limits of sensibility, but what distinguished Mackenzie’s conception of emotional authenticity was that it was determined not simply, as had been the case before, by the profusion or otherwise of its expression, or, indeed, by the object of its focus, but by the extent to which it accorded with the interests not just of ‘humanity’, but, more specifically, of the state.Footnote 57
By the nineteenth century, the interests of the state were perhaps most obviously manifest in the prosecution of war and imperial conquest and it was these twin endeavours with which medical practitioners increasingly sought to imaginatively align themselves.Footnote 58 For Mackenzie and his contemporaries, the battles of the French wars, most especially Waterloo, were a recent memory. Hence, like Lizars before him, he capitalised on the imaginative and emotional appeal of the military, albeit in a somewhat more ambiguous manner. Addressing those who ‘would reject the present appeal, on the ground that […] this humane and religious nation forbids such cruel butchery of the human body’, he begged leave to ‘in imagination […] convey these persons to the dissecting room, where a single dead body lies under the minute knife of the anatomist, who in his hidden and silent retreat […] is preparing to instruct perhaps a hundred young and ardent minds, in a knowledge of those facts which are to prove, in their hands, the salvation of innumerable lives’. He then proposed
to convey them from a scene which they loathe so much and know so ill, to one which they have heard more of, and have loved better – to the battle-field […] the red and living blood is pouring in torrents, the air is rent with agonizing cries, and […] the ground is covered with weltering corpses. We have seen the day, when Britain, reckoning up the slain, coolly subtracted the number of her own sons whose blood had drenched a foreign soil […] The humane and feeling public received the estimate of slaughter with rapture. It was the estimate of what they had won. The youth, the vigour, and the beauty of the fallen were forgotten. The loud lamentations of the widow, the mother, and the sister, refusing to be comforted, were lost to a deafening cry of victory. The hour was given to madness, and midnight’s darkness could not hide the wantonness of mirth and triumph.Footnote 59
Mackenzie’s intensely melodramatic prose paints a deeply ambivalent picture of ‘victory’ at Waterloo, an ambivalence that, as Philip Shaw and others have shown, was by no means uncommon within Romantic culture.Footnote 60 But in Mackenzie’s hands, this ambivalence served a distinct purpose, highlighting what he perceived to be the emotional hypocrisy of the public (or elements thereof) in celebrating wartime sacrifice while ‘raising their hands in well-affected horror’ at the proposition of anatomical dissection.Footnote 61 Both, he argued, were of equivalent importance to the state, for if ‘the end of war, which is the defence of our country, is sufficient to justify the adoption of a mean[s] so terrible as the destruction of hosts of living men, surely the end of anatomical study, which is the assuagement of human suffering, is ten times sufficient to justify the dissection of the dead!’Footnote 62
There is nothing in Mackenzie’s biography to suggest that he was an avowed utilitarian. However, his claim that in order to ‘discover whether any action […] be right or wrong, we have to inquire into its tendency to promote or diminish the general happiness’, bears the unmistakable stamp of utilitarian thought.Footnote 63 So too does the unflinching rationality of his legislative proposals (he was, as far as I know, the only major commentator who suggested sourcing bodies from foundling hospitals alongside infirmaries, workhouses, and prisons).Footnote 64 Jeremy Bentham had a long-standing interest in the legal status, and potential utility, of the dead and, during the mid-1820s, corresponded with the Home Secretary Robert Peel (1788–1850) about legislative reform on the matter of obtaining subjects for anatomical dissection.Footnote 65 However, rather than Bentham, it was his close associate, the physician and sometime Unitarian minister Thomas Southwood Smith (1788–1861), who would make the single biggest contribution to shaping public and professional discourse on this subject. In 1824, Smith published an anonymous review of Mackenzie’s pamphlet in the Westminster Review under the title ‘Use of the Dead to the Living’. Like Mackenzie, Smith was keen to establish from the outset that medicine and surgery were an inherent social good, claiming that ‘An enlightened physician and a skilful surgeon, are in the daily habit of administering to their fellow men more real and unquestionable good, than is communicated, or communicable by any other class of human beings to another’.Footnote 66 Again, like Mackenzie albeit even more so, Smith was also concerned to reconcile this social good with popular sentiment, elaborating an emotional logic by which the interests of the living were prioritised over their feelings towards the dead. In the published version of his 1832 lecture over Bentham’s corpse, Smith reminded his readers of Bentham’s distinction between the twin fallacies of ‘asceticism’ and ‘sentimentalism’. Whereas asceticism approved of an action ‘in as far as it tends to diminish happiness’, sentimentalism judged actions not by their tendency to enhance or diminish happiness, but according to the subject’s feelings about the act itself. It was as a via media between these two extremes that Bentham proposed his famous principle of ‘felicity’, whereby actions were judged solely by their ‘CONDUCIVENESS TO THE MAXIMUM OF THE AGGREGATE OF HAPPINESS’.Footnote 67
For Smith, Bentham’s principle was to ‘moral science’ what Isaac Newton’s law of universal gravitation was to natural philosophy, and necessitated a thoroughgoing reconfiguration of understandings of emotion and sentiment.Footnote 68 John Stuart Mill (1806–73) maintained that Bentham was both philosophically and personally immune to emotion, stating that ‘In many of the most natural and strongest feelings of human nature he had no sympathy’. Likewise, describing his father, and Bentham’s close friend, James Mill, he claimed: ‘For passionate emotions of all sorts, and for everything which has been said or written in exaltation of them, he professed the greatest contempt’.Footnote 69 Smith, by contrast, was seemingly less averse. Indeed, in the ‘Use of the Dead to the Living’ he acknowledged that one of the most ‘formidable obstacles’ to ‘the prosecution of anatomical investigations’ was a ‘feeling which is natural to the heart of man’, namely an emotional attachment to the bodies, and even material possessions, of our loved ones. We cannot, he alleged, ‘separate the idea of the peculiarities and actions of a friend from the idea of his person’:
everything that has been associated with him acquires a value from that consideration; his ring, his watch, his books, and his habitation. The value of these as having been his is not merely fictitious; they have an empire over my mind; they can make me happy or unhappy; they can torture and they can tranquilize; they can purify my sentiments and make me similar to the man I love; they possess the virtue which the Indian is said to attribute to the spoils of him he kills, and inspire me with the powers, the feelings, and the heart of their preceding master.Footnote 70
These were not Smith’s own words. He was quoting (albeit without attribution) from William Godwin’s (1756–1836) Essay on Sepulchres (1809), a meditation on the dead and a call for a system of national memorialisation that was, in part, shaped by Godwin’s own grief at the loss of his wife Mary Wollstonecraft (1759–97).Footnote 71 As David McAlister has shown, while they shared many of the same utilitarian principles, Godwin and Bentham entertained very different conceptions of the emotions attached to the dead. By quoting as extensively as he did from Godwin, both in his Westminster Review article and in his later lecture, McAlister suggests that Smith was acknowledging ‘what Godwin had got right and Bentham wrong; the importance of emotion and its capacity to stimulate progressive reform’.Footnote 72 There is much truth to this observation, for Smith did indeed appeal to the emotions in making his argument. For example, like Lizars and Mackenzie before him, he sought to conjure feeling through imagination:
We put it to the reader to imagine what the feelings of an ingenious young [surgeon] must be who is aware of what he ought to do, but whose knowledge is not sufficient to authorise him to attempt to perform it, and who sees his patient die before him, when he knows that he might be saved and that it would have been within his own power to save him, had he been properly educated. We put it to the reader to conceive what his own sensations would be, were an ignorant surgeon […] to undertake an important operation […] suppose it were his mother, his wife, his sister, his child, whom he thus saw perish before his eyes, what would the reader then think of the prejudice which withholds from the surgeon that information without which the practice of his profession is murder?Footnote 73
Smith did not valorise emotions for their own sake, however. Rather, like Mackenzie, he valued them only insofar as they were conducive to social utility, to the realisation of a greater good. Thus, he followed up his quotation from Godwin by claiming that ‘It is not the eradication of these feelings that can be desired, but their control: it is not the extinction of these natural and useful emotions that is pleaded for, but that they should give way to higher considerations when these exist’.Footnote 74 And yet, Smith does not follow through on his philosophical premise. He does not invoke the character of the bereaved friend so that he might ask them to sacrifice their tender feelings for the greater good and hand the body of their loved one over to the surgeons. Rather, he proposes to use other people’s bodies, notably, as suggested by Mackenzie and Abernethy, those dying, unclaimed by relatives, in hospitals, workhouses, and other institutions. Richardson has charted the complex and contested meanings of the term ‘unclaimed’ within the debates surrounding the Anatomy Act: whether, for example, it meant those with no living relatives, those whose relatives did not immediately present themselves, or simply those who could not, or would not, pay for a funeral.Footnote 75 What is notable about Smith’s contribution to the debate is that he cast this category in fundamentally emotional terms. To be sure, he made the claim that the bodies of the poor (or rather paupers, though Smith did not admit a distinction) were, in principle, ‘public property’, stating that ‘no maxim can be more indisputable than that those who are supported by the public die in its debt, and that their remains might, without injustice, be converted to the public use’. He also argued that it would be the poor themselves who would benefit from the resulting improvements in surgical standards, as the wealthy could always afford the most experienced and skilled attendants, whereas the poor had little choice about who treated them. However, he maintained that ‘it is not proposed to dispose in this manner of the bodies of all the poor; but only of that portion of the poor who die unclaimed and without friends, and whose appropriation to the public service could, therefore, afford pain to no one’.Footnote 76
The concept of friendlessness has received little consideration within the scholarship on the Anatomy Act, but it is vital to understanding how the Act was justified in emotional terms. More will be said about its ambiguities and contradictions in due course, but for the moment it is important to reiterate that Smith highlighted the ties of friendship not in order to demonstrate the emotional sacrifice demanded of the rational citizen, but, rather, to present a contrast to the emotionless quality of those bodies that would be taken in ‘the public service’. As Smith saw it, the body only possessed emotional meaning within a nexus of interpersonal relationships; it had no intrinsic emotional value and any body that could be said to have fallen outside of this nexus could therefore be appropriated without compunction. Such a measure, he concluded, would ‘tranquilize the public mind. Their dead would rest undisturbed: the sepulchre would be sacred: and all the horrors which the imagination connects with its violation would cease for ever’.Footnote 77
Smith’s essay exerted a huge influence over subsequent debates concerning the procurement of subjects for anatomical dissection. Indeed, while disagreements persisted over issues such as the stigma of juridical dissection, the exact institutions from which bodies might be taken, or the disposal of remains, the maxims established by Smith in 1824 remained remarkably unchallenged throughout the later 1820s and early 1830s, at least among proponents of reform. Thus, the Report from the Select Committee on Anatomy (1828) claimed that ‘If it be an object deeply interesting to the feelings of the community that the remains of friends and relations should rest undisturbed, – that object can only be effected by giving up for dissection a certain portion of the whole, in order to preserve the remainder from disturbance’.Footnote 78 This should perhaps come as little surprise. As Richardson points out, the Select Committee was composed either of ‘first degree Benthamites’ such as Warburton and Joseph Hume (1777–1855), or of ‘keenly sympathetic’ radicals like John Cam Hobhouse (1786–1869).Footnote 79 And, indeed, Smith was one of the witnesses who testified before the Committee. What is notable, however, is the number of other witnesses who would not have been considered utilitarians, but who nonetheless followed Smith’s maxims to the letter. Astley Cooper, for example, who provided some of the most extensive testimony, repeated, among other things, Smith’s claims about the benefits of dissection falling upon the poor and his belief that, when it came to the appropriation of unclaimed bodies, ‘As no person’s feelings would be outraged, there would be no reasonable objection to it’.Footnote 80 Similar sentiments were expressed by Benjamin Brodie, who claimed that ‘the fittest persons in society for dissection, are those who have no friends to care about them’, adding ‘the dead body […] does not feel either injury or disgrace, and where there are no friends to feel it, the mischief to society can be none at all’.Footnote 81
Even more remarkable was the extent to which Smith’s utilitarian ideas permeated sections of the medical press that were otherwise actively hostile to the politics of Bentham and his circle of ‘Philosophical Radicals’. The conservative London Medical Gazette, for example, fell well and truly in behind the reformist party line, railing against ‘popular prejudice’ and advocating a resolutely instrumentalist approach to the dead body. In January 1829, for example, it asked ‘What is the boasted march of intellect good for, if […] the most useful of arts is to be sacrificed to imaginary fears?’, while in May 1828 it struck a resonantly utilitarian tone when it proclaimed that ‘venerate the dead as we may, we should never forget that veneration for the living is a duty of superior obligation: the promotion of human happiness is a duty from which we cannot be exonerated’.Footnote 82 In many ways, the issue of anatomical dissection can be said to have functioned as a kind of conceptual looking glass, through which the usual politics of the Gazette were inverted. Thus, it might find itself advocating a materialist understanding of the body, in which the corpse was merely a ‘residue of molecules’ with ‘no intrinsic value’, or praising the post-Revolutionary French surgical system when it normally deprecated the Francophilia of radical reformers.Footnote 83 The Gazette even attacked the conservative stalwart and Waterloo veteran George Guthrie (1785–1856), for daring to break ranks with surgical orthodoxy and declare his objection to the Anatomy Bill. Referring to one of Guthrie’s lectures in which he expressed ‘his abhorrence of having [dissection] performed on his body after death’, the Gazette queried the emotional sincerity of his remarks, stating:
As an individual confession of undefinable and superstitious horror (for we cannot call it by any other name), it is curious […] But it is only curious. Upon its announcement, in the lecturer’s energetic and fluent tones, it excited in his auditory no feeling but that of surprise – no sympathy; and as it appeared to us, the fact seemed to be communicated rather for the sake of producing effect, than for any other perceptible reason. If this was really Mr G.’s design, he was very successful; but if he intended more – to excite or to encourage a kindred horror and antipathy in the bosom of any of his hearers – he must have been sadly disappointed.Footnote 84
However, while practitioners and the medical press sought to regulate professional opinion, public sentiment could not be so easily disciplined. In the face of attempts to render the ‘friendless’ dead body an emotionless object, Guthrie’s comments were a reminder of the capacity of the imagination to generate intense feelings of dread. Even if some commentators suggested that ‘No man of even ordinary intellect shrinks from the thought of being anatomised himself [for] the senseless man can suffer nothing’, Guthrie’s example suggested otherwise, and affirmed that the living subject (rich or poor, friendless or otherwise) might yet imagine their body being eviscerated after death and feel abhorrence, revulsion, and fear.Footnote 85
Writing shortly before the Anatomy Bill became law in August 1832, a contributor to The Times reflected on Bentham’s decision to have his body dissected and preserved for posterity, stating that ‘it becomes the duty of all those who are interested in the happiness of mankind, to oppose the progress of such injurious opinions’ as expressed by Guthrie and other opponents of the proposed legislation. ‘Mr Bentham’, they continued, ‘impressed with this idea […] determined to devote his own body to the public good’.Footnote 86 Bentham’s ‘Auto-Icon’ was by far the most extravagant expression of mortuary rationalism in this period (Figure 5.1). Even so, many other like-minded individuals sought to do their ‘duty’ in challenging what they believed to be popular superstition and sentimentality. For some, such as the radical Liverpudlian surgeon George Rogerson, public lectures provided an ideal opportunity to preach the rationalist creed. At one of a series of lectures at the Mechanics’ School of Arts in 1830, for example, he castigated the ‘foolish objections against dissections’, exclaiming ‘Begone with such prejudices, with such childish feelings; they are a disgrace to the age we live in’. On receiving a hearty applause from his artisanal audience, he was evidently gratified: ‘Gentlemen’, he proclaimed, ‘I hear this applause with feelings of real pleasure, for it is a proof that the members of this institution have minds enlightened and superior to vulgar prejudices. This is creditable to you’.Footnote 87

Figure 5.1 Jeremy Bentham’s ‘Auto-Icon’, housed in Thomas Southwood Smith’s consulting room before being moved to University College London in 1850.
Others promoted what, to use Richardson’s phrase, we might call an ‘alternative necrology’.Footnote 88 These utopian visions were occasionally so far removed from reality that they might easily have passed for satire. Thus, one commentator imagined a state in which the donation of one’s body for dissection was heralded as a form of civic sacrifice for which the rational citizen would be celebrated in both life and death, their urn ‘distinguished by some mark’ and heralded to the grave by ‘a train of children […] with garlands and songs of thanks’.Footnote 89 The radical proto-socialist Pierre (Peter) Baume (1797–1875), meanwhile, was probably only half joking when, in denouncing the ‘ROMANTICISM OF THE GRAVE’, he decreed that not only should his body be dissected, but ‘even the least particle of my extinguished frame should be rendered subservient to some useful purpose’, his skin tanned and used for furniture and his bones transformed into ‘knife-handles, pin-cases, small boxes [and] buttons’.Footnote 90
Nonetheless, such efforts to ‘tranquilize the public mind’ faced significant challenges, especially after the discovery of William Burke (1792–1829) and William Hare’s (b. 1792/1804) heinous crimes in Edinburgh in late 1828.Footnote 91 The Burke and Hare case transformed the terrain of debate, invoking the spectre of a whole new form of bodily appropriation in which cadavers were not merely disinterred but manufactured through murder. At one level, this merely gave added impetus to legislative efforts to establish a legal supply of anatomical subjects. For large sections of the public, however, it intensified the emotive qualities of the issue and made the rationalist argument harder to sell. For one thing, it raised the possibility that, under any system of bequest or appropriation, the relatives of the dead might sell their bodies for profit, just as Burke and Hare had done their victims. This violation of precisely those emotional ties that the proposed legislation was supposed to protect excited a great consternation that was never fully resolved, not even after the passage of the Act in August 1832.Footnote 92 Thus, the Bill’s most implacable Parliamentary opponent, the radical MP for Preston, Henry Hunt, asked ‘What could be said in favour of a Bill which gave to a father the power of selling the dead body of a child – which gave to a husband the power of selling the dead body of a wife’.Footnote 93 In a similar vein, the conservative MP for Worcester, George Richard Robinson (c.1781–1850), claimed that the Bill held out an ‘inducement to the most poor and miserable class of the community to dispose, by public sale, of the dead bodies of their nearest relatives. A husband, for instance, might sell the body of his wife, the mother of his children’.Footnote 94 Even more significantly, the Burke and Hare murders further amplified the ambivalences surrounding the concept of friendlessness that was so central to the rationalisation of bodily appropriation, for, as many commentators noted, it was precisely these people, itinerant, unknown, unlooked for, who were chief among Burke and Hare’s victims. As Thomas Babington Macaulay (1800–59), an ardent champion of the Bill, put it, ‘What man, in our rank of life runs the smallest risk of being Burked? That a man has property, that he has connections, that he is likely to be missed and sought for, are circumstances which secure him against the Burker […] The more wretched, the more lonely, any human being may be, the more desirable prey is he to these wretches’.Footnote 95
Macaulay’s comments highlight the pitfalls of using friendlessness as the essential category for determining which bodies should be appropriated for surgical use. Friendlessness was not a semantically empty vessel into which the utilitarians might pour their own meaning. It was, on the contrary, a well-established cultural motif. The association of poverty with friendlessness can be traced back to the Bible, specifically Proverbs 14:20, which claimed that ‘The poor is hated even of his own neighbour: but the rich hath many friends’.Footnote 96 Such language found its way, via biblical paraphrase, into hymns such as ‘Rulers of Sodom! Hear the Voice’, which enjoined ‘Do justice to the friendless poor, / and plead the widow’s cause’.Footnote 97 A quick survey suggests that use of the term ‘friendless’ increased markedly over the later eighteenth century, before reaching its peak between 1820 and 1850.Footnote 98 Friendlessness was a concept widely deployed both by the poor themselves, notably in pauper letters, and also by charities, such as the Friendless Poor Society, founded in Newcastle-upon-Tyne in 1797.Footnote 99 The concept of friendlessness therefore served to sharpen political discourse around a Bill that many opponents saw as a calculated attack on the dignity of the poor. As another implacable opponent of the Bill, William Cobbett, noted, ‘It is curious that the WHIG REFORMERS are for this bill, and that TORIES are against it!’; and, indeed, it was true that Parliamentary opposition forged an unlikely alliance between popular radicals like Hunt and ultra Tories like Charles Sibthorp (1783–1855).Footnote 100 The language of friendlessness could thus be deployed in both a defiant and a paternalistic manner. The Earl of Harewood (1767–1841), for example, claimed that he ‘did not see why the bodies of the poor and friendless should be particularly selected for the dissecting-knife’.Footnote 101 Meanwhile, in a neat example of the double meaning that the term had by then acquired, Cobbett’s Weekly Register ran a piece from the Leeds Mercury ahead of the highly contested election of 1832, protesting the ‘DEAD BODY BILL’ and addressed to ‘THE RATE PAYERS OF LEEDS, BUT ESPECIALLY TO THE FRIENDLESS POOR’.Footnote 102
However, the ultimate irony of the utilitarian use of friendlessness was that, in seeking to divest the anatomical body of affective meaning, they only succeeded in investing it with greater emotional significance than might have been the case for the legally more problematic, but culturally less resonant, term ‘unclaimed’. Indeed, far from being the emotive vacuum that men like Smith had imagined, the friendless poor were in actual fact the most pitiable and pathetic of all possible people. By definition, of course, such individuals were largely unknown, if not unknowable, precisely because they lacked social capital, but this only encouraged opponents of what one commentator called the ‘philosophy of the shambles’ to imagine the people they might have been or the lives they might have led.Footnote 103 Due to their powerful association with personal nobility, bodily proficiency, and state service, soldiers and sailors were a favoured subject of such fantasies. Thus, The London Medical Gazette dismissed as a ‘pseudo-pathetic story’ the Morning Herald’s imagined account of a soldier who had ‘fought battles for his country’ only to be ‘brought to the “human shambles” and exposed to the knife of the anatomist, and the “rude gaze of rabble boys”’.Footnote 104 Even more elaborately, in the immediate aftermath of the passage of the Act, Fraser’s Magazine published a story entitled ‘Dialogues of the Dead’, which imagined a reckoning in the afterlife for utilitarians, surgeons, and their Parliamentary allies. Representing the ‘victims’ of the Act was a sailor who had ‘done nothing but served [his] country in three quarters of the globe’. As Charon, the ferryman of Hades, announced:
Well! here’s a fellow come down, who swears that they denied him the common right to his own body, when he died, merely because he was unfortunate! that he led a hard life in their service; by serving them, he was cut off from all connexions of father, husband, friend; and because he was thus cut off, they refused him burial, used his poor remains of a body as they have used their criminals in time out of mind – dissected it! in a word, that because he had no friend on earth, he should neither have mercy nor justice.Footnote 105
It was because of these political and cultural complexities that The Lancet ultimately found itself unable to support the Anatomy Bill. As has been argued elsewhere, Thomas Wakley trod a careful path through the political cultures of the 1820s, balancing the philosophical radicalism of Bentham and his circle against the popular radicalism of Hunt, Cobbett, and their ilk.Footnote 106 In the early days of the debate, The Lancet took a decidedly utilitarian stance on the issue of anatomical dissection. In February 1824, for instance, it decried the existence of a ‘prejudice’ against dissection among the higher orders, by which means it ‘becomes more deeply rooted in the minds of the ignorant and uninformed who are not able to think for themselves’. In order to advance the practice of anatomy and thereby ‘increase the happiness and lessen the misery of mankind’, it called upon the profession to ‘come forward and devise some means by which the present impediments may be removed’. It even recommended Abernethy’s suggestion that bodies should be sourced from ‘those persons who die in London without friends’ as ‘deserving of consideration’.Footnote 107 The Lancet maintained this line throughout the succeeding five or so years. In 1826, for example, it urged surgeons to undertake public demonstrations of anatomy, arguing that it was ‘useless to reason on a circumstance which is purely a matter of feeling. SHOW the people the utility of dissections – SHOW them the benefits which are conferred upon their fellow creatures […] and they will […] consider them the laudable means by which the greatest public good can be accomplished’.Footnote 108 Like other proponents of reform, it also adhered to the idea that the bodies of the ‘friendless’ were emotionally neutral, maintaining that ‘it is the feelings of survivors only, which the legislature is called upon to respect’ and arguing that ‘however averse an individual may be in his life time to the dissection of his body after death, if he has no surviving relatives to respect this prejudice, […] no reason can be urged against the dissection of such a person’s body, nor could public feeling possibly be outraged by it’.Footnote 109
During the later 1820s, however, Wakley’s position began to shift, at first slightly, then completely. When the report of the Select Committee was released in 1828, Wakley declared it to be ‘upon the whole, a satisfactory document’, but objected to Abernethy’s claim that the bodies of the institutionalised poor were, by rights, public property, arguing, somewhat expediently, that ‘though it is obvious that none but the bodies of the poor are likely to be unclaimed’, the law should avoid making dissection ‘inseparable from poverty’.Footnote 110 But with the discovery of Burke and Hare’s crimes, all such nuance was abandoned. In an editorial of January 1829, Wakley stated that ‘It is fearful and humiliating to reflect on the enormities of which wretches wearing the human form are capable’ and called for the immediate closure of all dissecting rooms in Britain. ‘The injury to medical science, [and] the inconvenience to medical teachers’ were, he claimed, ‘all insignificant considerations compared with the overwhelming necessity of protecting the public against assassins, who traffic in the dead bodies of their victims’.Footnote 111 Perhaps unsurprisingly, neither the authorities nor the profession followed Wakley’s lead, and, in a subsequent editorial, he expressed his ‘indignation and disgust’ at ‘the chilling apathy with which the greater number of our teachers of anatomy, have regarded the late unparalleled disclosures’.Footnote 112 As such comments suggest, the crimes of Burke and Hare, together with those of John Bishop and Thomas Williams in the summer of 1831, pushed The Lancet firmly into the camp of popular radicalism and fuelled the kinds of melodramatic outrage explored in Chapter 4. This is not to say that Wakley rejected dissection in principle; indeed, he continued to dismiss opposition to pathological anatomy as an irrational and ‘sentimental’ prejudice.Footnote 113 However, he increasingly came to see the Bill itself as the work of corporate monopoly and political tyranny and professed ‘common feeling’ with the friendless poor.Footnote 114 Hence The Lancet celebrated the failure of the first Anatomy Bill in 1829 and, as the second neared the end of its passage through Parliament, predicted ‘popular fury and violence’.Footnote 115 Moreover, when it finally passed into law, Wakley declared, in characteristic style, that ‘This foul, this disgusting, this anti-humanising, this blood-stained ANATOMY ACT, must be remodelled, or it will bring the profession into everlasting disgrace with the public’.Footnote 116
The Lancet’s response to the Anatomy Act is instructive, and suggests the limits of generalisation. Even so, Wakley was well aware that he was an outlier.Footnote 117 Popular opposition to the Act, which was soon to become intimately bound up with the iniquities of the New Poor Law, continued for some time, but the issues that were debated throughout the 1820s were, by 1832, effectively settled. The vast majority of the profession, from conservatives to radicals, were united in their belief that surgeons should be supplied with the bodies of friendless paupers whose appropriation for the purpose of anatomisation was both socially beneficial and emotionally inoffensive. Of course, it should be noted that surgeons and anatomists had long held a dualistic view of the human body as something to be both healed and used; it was nothing new to view the cadaver as an object. But what was new was that, during the 1820s, surgeons articulated a public discourse that actively positioned itself against popular sentiment, stripping the bodies of the dead of emotional association and rendering them subservient to a surgical project that was figured as congruent with the interests of the state. As their greatest political ally, Henry Warburton, put it to his fellow MPs:
They must recollect […] that there were cases, in which the feelings and wishes of mankind were made to succumb to the service of the state. What could be more savage than war? And yet when the service of the State, the preservation of the nation, and the welfare of the people were at stake, we set aside private feelings, and scenes of bloodshed and suffering were the consequence […] in such instances, the wishes and feelings of individuals were held as nothing, when compared with the interests of the nation at large. Why, then, should they hesitate to make some sacrifice when a question was at issue which so materially affected the welfare of every human being?Footnote 118
This is not to say that the dead body was entirely denuded of all emotional meaning, not even within surgical culture. Two documents in Bransby Cooper’s file, with which we began, indicate the continued emotional complexities of the cadaver. One is a short note sent to Astley Cooper by an unnamed individual who wrote that, having heard ‘you are in the habit of purchasing bodys [sic]’ and ‘knowing a poor woman that is desirous’ of selling hers, ‘I have taken the liberty of calling to know the truth’. Cooper’s curt, incredulous response, written on the back, reads: ‘The truth is that you deserve to be hanged for such an unfeeling offer’.Footnote 119 The second is a far more elaborate bequest sent to Cooper by one William Williams in the aftermath of the Anatomy Act. In lengthy and tortuous legalese, Williams promised his body to Cooper for the sake of the ‘public benefit derived from anatomy’. He states that, should he die a ‘bachelor and unmarried’, his ‘mortal remains may be at your disposal for the aforementioned purposes of dissection’. However, he makes an exception in the event of his marriage, in which case ‘I beg it to be understood […] that […] my said wife’s approbation or disapprobation may be obtained and ascertained and according as she shall or may approve or disapprove of the said dissection the approval or disapproval of and by her […] is to […] be considered as […] my will and earnest desire and pleasure’.Footnote 120 Clearly then, despite all attempts to render the subject one of pure reason, transcending sentiment, the emotional ties of love and marriage could not easily be ‘put asunder’. Even an individual’s stated desire as to the fate of their mortal remains could be countermanded by precisely those emotional attachments that Smith had sought to mitigate through the dictates of a higher duty. In death, as in life, the biblical and legal injunction that the married couple were of ‘one flesh’ was, it seemed, as much literal as figurative. As we shall see in the next section, however, it was not only the dead body that would undergo an uncertain emotional reconfiguration at the hands of surgeons in this period; some fifteen years after the passage of the Anatomy Act, another transformation in practice and perception would render the living body of the operative subject similarly quiescent and, in the eyes of some, uncannily reminiscent of the cadaver on the dissection table.
Constructing the ‘Chamber of Sleep’: Emotions and the Unconscious
In 1900, Frederick Treves (1853–1932), the recently appointed Surgeon Extraordinary to the elderly Queen Victoria, gave a lecture to the annual meeting of the BMA in which he looked back over the preceding century to a time when the surgeon ‘was but a sorry element in social life’. ‘The operator of olden times’, he claimed, ‘stepped into the arena of the operating theatre as a matador strides into the ring’:
Around him was a gaping audience and before him a conscious victim, quivering, terror-stricken, and palsied with expectation. His knife was thrust through living flesh and acutely-feeling tissue, and the sole kindness of his mission was to be quick. In spite of moans for mercy from gagged lips the knife had to move its way steadily and, undeterred by struggles and bursts of haemorrhage, the blade must needs pass without faltering or sign of hesitancy.
‘There is less need for such qualities now’, Treves continued; ‘The operating theatre of the present day has lost its horrors and has changed from a shambles to a chamber of sleep’. For Treves, the advent of anaesthesia in 1846 had not only changed the nature of operative practice, allowing the surgeon to proceed ‘leisurely without fear of being regarded as timorous’, it had transformed the very ‘personality’ and ‘bearing’ of the surgeon, losing, perhaps, some of the ‘dash’ of earlier days, but ‘gain[ing] much in the direction of the sympathetic handling of his patient and in the culture of gentleness’.Footnote 121
By the time of Treves’ talk in 1900, the narrative of surgery’s transformation from an age of filth, disorder, and suffering to one of cleanliness, painlessness, and techno-scientific rationality was firmly established, as was anaesthesia’s pivotal place within it. What is more, and as Treves’ words suggest, this transformation was often couched in terms of emotional deliverance. Pernick observes that ‘anaesthesia made possible a greater range of medical sentiment toward patients – both more routine callousness and more benevolent sensitivity’, but he also suggests that the associated rise of modern bureaucratic medicine ‘limited the expression of sympathy and full concern for the individual’.Footnote 122 In Chapter 6, we shall examine in more detail the emotional ambivalences and complexities of later nineteenth-century techno-scientific surgery. In this chapter, we are concerned with that very specific historical moment in the mid-nineteenth century when the patient, as a conscious, agentive individual, effectively disappeared from the emotional space of the operating theatre, rendered quiescent by anaesthetic oblivion. As we shall see, this process was far from being as simple as Treves’ metaphor of the ‘chamber of sleep’ suggests. Indeed, the phenomena of ether and chloroform were many, potentially far more troubling, things before they were rendered as innocuous as sleep. As Pernick, Snow, and others have demonstrated, though remarkable in its effects, anaesthesia was no magic bullet. Rather, it was a dramatic chemical and technological intervention into well-established practice whose professional, social, and cultural acceptance was conditional and contested. Pernick’s account provides an invaluable insight into the implications of anaesthesia for measuring pain, for rationalising care, and for shaping clinical judgement in the context of the United States.Footnote 123 Snow, meanwhile, tells the story from the British perspective, demonstrating the vital role played by John Snow (1813–58) in making anaesthesia a distinct branch of surgical practice, as well as exploring the varied aspects of its professional and social contestation.Footnote 124 However, although much of this work alludes to the complex emotional dimensions of anaesthesia, few historians have focused specifically on its role in reshaping the cultures of surgical subjectivity and intersubjectivity.Footnote 125 This is precisely what this section seeks to do; but, in order to do so, it is first necessary to address one of the most puzzling and long-standing questions in the history of anaesthesia.
It is virtually impossible to talk about the ‘discovery’ (or invention) of anaesthesia without acknowledging the fact that the chemist Humphry Davy recognised the potential utility of nitrous oxide for pain relief nearly half a century before inhalation anaesthesia became standard practice. In his Researches Chemical and Philosophical (1800), Davy observed that as ‘nitrous oxide in its extensive operation seems capable of destroying physical pain, it may probably be used with advantage during surgical operations in which no great effusion of blood takes place’.Footnote 126 Many early advocates for the use of ether and, later, chloroform felt compelled to note Davy’s abortive discovery, even if they were at a loss to explain why it was not taken up. John Gardner (1804–80), for example, could only opine that ‘Numberless instances might be cited where men have held in their hands, looked at with their bodily eyes, but without perceiving, the elements of great discoveries’.Footnote 127
By contrast with contemporaries, historians have actively sought to understand why the palliative possibilities of nitrous oxide (and other gases) were not fully realised until the later 1840s. Margaret C. Jacob and Michael J. Sauter suggest that Davy and his associates lacked the technical capability to develop nitrous oxide as an effective anaesthetic agent. More importantly, they also contend that these people lacked the conceptual and ideological capacity to perceive nitrous oxide as anything other than a powerful enhancer of sensation, intimately associated with either ‘pleasure or danger’.Footnote 128 Jacob and Sauter situate themselves, in part, against the argument, advanced by E. M. Papper, that anaesthesia was a direct product of Romantic sensibility, which, by giving birth to subjectivity and interiority, made physical suffering inherently insufferable.Footnote 129 In many ways, Papper’s argument runs directly counter to my own. As we have seen in this book, Romantic surgeons were powerfully alive to the sufferings of their patients and were concerned to do what they could to ease them where possible. And yet, as we have also seen, pain was part of a wider cultural sensorium that sustained emotional intersubjectivity and encouraged forms of personal reflection that, though often productive of ‘emotional suffering’, also stimulated ‘good’ emotions such as pity, sympathy, and reverence. For instance, in 1807, Charles Bell wrote to his brother George to share with him a revelation he had experienced during a stay in the rural residence of a patient on whom he was to operate. One day, Charles claimed, he rose at five in the morning and ‘leaped the garden wall, and ran in full chase through the country, making acquaintance with every living thing I met. I found three young horses, an ass, a tame fox, and an owl, particularly conversable’. Driven inside by rain, he ‘enjoyed a waking dream’ in which ‘all was right in the system of the universe – that consistent with our desires and passions was the shortness of our life and our being liable to suffering and disease’ and that, without this, ‘we should have been inanimate, cold, and heartless creatures’. ‘I thought I perceived two great objects of admiration and love’, he continued, the first being ‘the intimate creation’ of life itself, the other being the ‘still higher enjoyment in the contemplation of mind […] strengthened by communication and sympathy’.Footnote 130 For Romantics like Charles Bell, then, sensation was everything, and pleasure and pain so inextricably intertwined in the complexities of sympathy and intersubjectivity that the notion that one specific form of pain might be extinguished from the world was barely conceivable.Footnote 131 This is not to say that Bell or his contemporaries lauded pain and suffering, or would necessarily have rejected anaesthesia had it been offered them. Rather, it is to suggest that, for them, pain was an ineluctable and largely irreducible feature of the human condition that, by necessity perhaps, had its moral and emotional compensations.
Clearly, it would require a far more reductionist understanding of pain in order to imagine the possibility of its abolition and, indeed, this is exactly what would come to pass in the second quarter of the nineteenth century. Stephanie Snow argues that ‘by the 1830s, the radical view that pain was purposeless began to emerge’, and she makes brief reference to Bentham’s conception of pain as an ‘inherent evil’.Footnote 132 However, she does not locate the origins of anaesthesia in these broader social and cultural shifts so much as in the specific conceptual transformations of medicine itself. In particular, she points to the clinical revolution of Parisian medicine at the turn of the nineteenth century and the ascendancy of what, following Owsei Temkin, Erwin Ackerknecht called the ‘surgical point of view’.Footnote 133 There is much to recommend this argument, and there is much truth in Snow’s assertion that the physiological researches of men like Marshall Hall promoted the idea that the vital functions of the body might be uncoupled from conscious volition.Footnote 134 But the clinical revolution does not, in itself, account for changing surgical understandings of pain, for it was perfectly possible for surgeons invested in clinical medicine to believe in the moral or physiological benefits of pain. The only way to fully account for this shift is to acknowledge the ascendancy of a moral and political philosophy that regarded pain as an ‘evil’ to be eradicated. Here we encounter difficulties, for, as I have suggested, it is rare to find surgeons directly invoking utilitarianism in their efforts to eradicate the pain of operative surgery, even if later commentators acknowledged the connection.Footnote 135 Nevertheless, there is enough material to constitute a reasonably robust version of what Dror Wahrman has called the ‘weak collage’ of cultural change.Footnote 136 For example, by 1840, one finds comments such as these from Charles Aston Key who, during a lecture on the ‘Principles and Practice of Surgery’ at Guy’s Hospital, questioned the long-held view that pain was a reliable indicator of the presence of disease:
Do we find that pain is the first impression made in every instance by a morbid cause acting on the whole frame or a part of the human frame? Certainly not. You may have a morbid cause with pain or without it […] Pain is, therefore, merely an accidental concomitant; and diseased action may cause an impression on the nervous system unaccompanied by pain.Footnote 137
Meanwhile, in the same month, at the same hospital, Samuel Ashwell (1798?–1852) told his students:
Pain and disease, whatever may have been said to the contrary by philosophers, are great evils, apart only from their power to discipline the mind and soften the heart: they cover with darkness the activities and enjoyments of existence. We fly from them instinctively, as we fly from death; of which we all know they are too often the servants and harbingers.Footnote 138
These quotations suggest something about shifting conceptions of pain in this period but, evidently, they do not refer explicitly to utilitarianism. Indeed, Ashwell specifically positioned himself against those ‘philosophers’ who advocated the moral virtues of pain without mentioning the very philosopher whose ideas underwrote his own argument. And yet, I would contend that such comments testify to the implicit influence of utilitarian thought within contemporary British medicine and surgery. We have already seen evidence of its role in shaping ideas about anatomical dissection, even among non-avowed Benthamites, and elsewhere I have demonstrated its influence in reconfiguring notions of medical charity in the 1830s.Footnote 139 We might also appeal to the pervasive presence of utilitarian ideas in British social thought more generally from the 1830s onwards. In 1839, for instance, one critic decried what he called ‘the vile spirit of Utilitarianism which is creeping like a plague over the land and over the age’, while more than thirty years later, another commentator claimed that ‘Utilitarianism […] may be described as practically the dominant creed of our time’.Footnote 140
Having said this, it would be misleading to suggest that the influence on surgery of the utilitarian conception of pain as ‘in itself an evil’ was sudden, complete, or unambiguous.Footnote 141 After all, even in his denunciation of pain, Ashwell held to the idea that it had some residual moral qualities, namely its ‘power to discipline the mind and soften the heart’. In the latter we detect the continued resonance of Romantic sensibility. In the former, meanwhile, we find evidence for the existence of an alternative model of pain that flourished in the decade or so immediately before the advent of anaesthesia and existed alongside utilitarian conceptions of pain as a morally vacuous evil.
In Chapter 3, we saw how the rhetoric of operative fortitude was routinely used to shape an ideal of the surgical patient as ‘bodily acquiescent and emotionally self-controlled’. This concept was of long standing, but by the 1840s it was increasingly figured as a signifier of physical hardiness and moral superiority, and those displaying such qualities were often contrasted with others who, in giving expression to their pain, fear, or suffering, failed to show the requisite degree of resolve.Footnote 142 There was, moreover, an increasingly gendered aspect to this culture of surgical self-possession. As we have seen, women had long been thought capable of equal, if not greater, displays of surgical fortitude compared to men, but by the 1840s surgical stoicism was increasingly figured as a masculine (often military) virtue, while displays of emotion were both feminised and pathologised. Of particular importance here is the spectre of hysteria; this began to re-enter medical and surgical discourse in a very pronounced way in the 1840s, spurred by works like Thomas Laycock’s Treatise on the Nervous Diseases of Women (1840), which located hysteria in women’s physiology and sexuality.Footnote 143 Such associations of femininity with pathological displays of emotion and inherent physiological weakness also found popular expression in such contemporary works as The Daughters of England (1842) by Sarah Stickney Ellis (1799–1872), which claimed that ‘woman, from her very feebleness is fearful; while from her sensitiveness she is particularly sensitive to pain’.Footnote 144
The influence of hysteria on surgical attitudes towards patients in general, and their expressions of pain in particular, is evident in the archives of Benjamin Travers junior (1808–68), who succeeded his father as surgeon to St Thomas’ Hospital in 1841. His four volumes of casebooks, which cover the period from 1843 to 1859, offer a valuable insight into the quotidian realities of surgical practice at mid-century and are remarkable for his repeated identification of moral failings in his male patients, particularly in terms of physical appearance, alcohol consumption, and propensity to masturbate.Footnote 145 As Joanne Begiato has argued, Victorian notions of manliness were rooted in forms of bodily and emotional self-mastery and a failure to conform to these ideals could, for surgeons like Travers, produce serious illness.Footnote 146 Travers made an explicit link between male expressions of emotion and the disease of hysteria, whose manifestation in women was a notable feature of his casebooks.Footnote 147 For example, in September 1843 he recorded the case of a ‘butcher’s lad’ who was ‘struck with a saw which inflicted a severe wound upon his right cheek’:
He was so restless with frequent hysteric sobbing that I bled him to a full pint from the arm although he had lost a great deal of blood from the face. Soon afterwards he became tranquil and slept for some time. He answered questions initially when he awoke, but the hysteric condition continued for some time. This is a sign of severe shock in young people and if it continues highly dangerous. It is allied to and is illustrative of the passio hysterica in Women.Footnote 148
Clearly then, from around the 1830s but especially in the 1840s, we see the articulation of two models of surgical pain that were, in essence, contradictory: one that viewed pain as a purposeless blight on human happiness, the other that considered it to be a test of character and virtue, particularly for men. The first of these regarded pain as something to be eliminated, the other as something to be endured. Neither model held complete sway and indeed, as we have seen in the case of Samuel Ashwell, it was possible for practitioners to subscribe to both simultaneously. And yet, despite their evident ambiguities, both were, in their own way, equally far removed from the Romantic conception of pain as an intersubjective social experience, productive of edifying emotions in the beholder as much as the sufferer. Moreover, in the dialectic tension between them, there emerged, if not a resolute determination that surgical pain should be eliminated, then perhaps a growing consensus that it could be.
As many historians have recognised, despite the narrative of abortive discovery associated with anaesthesia, the period between Davy’s observations on nitrous oxide and the American dentist William T. G. Morton’s (1819–68) first public demonstration of ether in October 1846 was not entirely devoid of attempts to induce a state of insensibility in those required to submit to what The Lancet called the ‘hard doom’ of operative surgery.Footnote 149 In 1819, for example, James Wardrop bled a female patient to a state of syncope in order to remove a tumour from her head.Footnote 150 Revealingly, Wardrop’s experiment attracted relatively little interest until 1833, when he referred to it in one of his lectures, stating that it was ‘a great desideratum in surgery to discover a mode by which the pain of surgical operations could be either alleviated or diminished’.Footnote 151
However, by far the most promising, if also the most contested, form of anaesthesia that emerged in the period before ether was mesmerism. There is no space here to do full justice to the conceptual richness and cultural complexities of mesmerism. For our purposes, it is important to note that histories of mesmerism and inhalation anaesthesia have often set the two firmly in opposition. As we have already heard, Robert Liston probably did not say of ether that ‘this Yankee dodge beats mesmerism hollow’, though he did, in a letter to James Miller composed in the immediate aftermath of his famous December 1846 operation, write: ‘Hurrah! Rejoice! Mesmerism, and its professors, have met with a “heavy blow and great discouragement”’.Footnote 152 As Alison Winter has shown in her peerless history of the subject, Liston’s antipathy to mesmerism owed much to a personal dislike of John Elliotson, his rival at University College London and its most high-profile medical advocate. The same might be said of Thomas Wakley, whose friendship with Elliotson was destroyed by his radical exposure of the alleged fraudulence of Elliotson’s favourite mesmeric subjects, Elizabeth and Jane Okey.Footnote 153
Despite vociferous opposition, however, there were many practitioners who regarded mesmerism as worthy of serious study. Thus, in 1840 Thomas Laycock claimed that it had ‘engaged the attention, not merely of the unthinking multitude, but of learned professors of medicine’ and necessitated ‘a thorough revision’ in ‘the relations of mind to body’.Footnote 154 Moreover, by 1842 it was being used with increasing frequency as a means of alleviating the pain of operative surgery. In his Harveian Oration to the Royal College of Physicians, given just six months before Liston’s first operation using ether, Elliotson claimed that ‘anaesthesia, is but a form of palsy […] If this condition can be induced temporarily by art, we of necessity enable persons to undergo surgical operations without suffering’. Elliotson ‘fearlessly declare[d] that the phenomena’ of mesmerism, including ‘the prevention of pain under surgical operations [were] true’ and he ‘implore[d]’ his audience to ‘carefully investigate this important subject’.Footnote 155 In many ways, Elliotson was beseeching the wrong audience. Generally speaking, physicians were more inclined to embrace the operative use of mesmerism than were surgeons, not least because it did not have the same potential to undermine their established practice and professional authority. Commenting on the lack of surgical attendees at a demonstration of mesmeric dentistry in June 1846, for example, the Bath physician and mesmerist Henry Storer questioned whether ‘painless operations in surgery’ might ‘prove too great a shock to their nervous systems, having been so long accustomed to witnessing the contrary’.Footnote 156
Winter has documented what she calls the ‘ambivalent’ support for surgical mesmerism in the years immediately preceding the introduction of ether, suggesting that, by late 1846, it was ‘on the brink of gaining acceptance among constituencies that had long resisted’ it.Footnote 157 There were even some who thought that the ‘discovery’ of ether, far from disproving the reality of mesmerism, only confirmed its veracity. For one contributor to Blackwood’s Edinburgh Magazine, this extended to all mesmeric phenomena, including clairvoyance, while others, such as Charles Radclyffe-Hall (1820–79), were more conditional in their acceptance.Footnote 158 The ‘so-called higher phenomenon of mesmerism’, such as ‘the sublime absurdities of clairvoyance and prevision’, were ‘impossible and quite incredible’, he claimed. Nonetheless, ether confirmed the essential truth that ‘sensibility may be entirely suspended for a time by artificial means’.Footnote 159
The fundamental problem with mesmerism, as Winter has shown, was that it was beset by intractable issues of subjectivity and authority. The reality of the mesmeric trance was virtually impossible to verify, being entirely dependent on observable (but easily faked) phenomena or the testimony of experimental subjects. Even Radclyffe-Hall remained unsure as to whether the mesmeric trance was ‘feigned’, ‘real’, or ‘an hysterical vagary’. Thomas Wakley, on the other hand, was far less equivocal. For him, it was the fundamentally subjective and intersubjective qualities of mesmerism that made it at once ludicrous and dangerous. Citing the example of the Okey sisters, together with the more recent clairvoyant ‘Arsenic Prophetess’ Mrs Bird, he grounded mesmerism in a supposedly feminine capacity for deceit and a ‘morbid desire’ for attention. At the same time, he also regarded mesmerism as, in itself, a pathology of the emotions, stating that ‘The production of […] morbid conditions of the nervous system, through the influence of the emotions of the mind, is – we repeat it emphatically – one great trunk, if not the root, of the mesmeric infamy’.Footnote 160
Winter astutely observes that, compared to the intersubjectivity of mesmerism, ether and chloroform offered a more objective foundation upon which surgeons might stake their claim to professional authority. As she puts it, ‘mesmeric effects explicitly involved the relationship between two people; one might even say they consisted of that relationship. The power of ether to produce an anaesthetic state lay in a chemical, not a social relationship. Ether avoided the disturbing and sometimes subversive associations that attended the mesmeric relationship’.Footnote 161 In a profoundly important way, Winter is right. Many received the news of ether in the same way as a correspondent to The London Medical Gazette, who saw it as the death knell for mesmerism and proof that ‘their boasted power is a deception, or, at most, has no influence but over the minds of a few hysterical females’.Footnote 162 But at the same time, Winter overstates the extent to which chemical anaesthesia constituted an objective phenomenon, free from potentially ‘subversive associations’. Ether was no ‘clean break’ from the intersubjectivity of Romantic surgery, nor from the ontological ‘messiness’ and personal idiosyncrasy that characterised the pre-anaesthetic operative subject. Rather, the figure of the quiescent surgical patient, rendered emotionally absent by induced insensibility, was one that had to be forged from the chaotic and complex free-for-all of early anaesthetic practice.
In the aftermath of Liston’s first operation using ether, surgeons up and down the country sought to explore the remarkable effects of the new vapour for themselves. As a consequence, the medical and popular press published hundreds of articles, letters, and case reports on the topic in the first six months of 1847. Though this ether ‘mania’ had subsided by the summer of 1847, there was a revived interest in anaesthetic experiment, though not perhaps at quite the same level of fervid excitement, following James Young Simpson’s first use of chloroform in November of the same year. What is notable about many of these early accounts of the use of ether is not the absence of the operative subject but rather their powerful vocal, physical, and emotional presence. In some cases, of course, the patient was put into ‘a perfectly quiescent state, without motion or sound’, but in others, the uncertain effects of the vapour made for a far less placid scene.Footnote 163 At St George’s Hospital in January 1847, for example, surgeons attempted several operations under ether in front of a large audience including Liston, Benjamin Brodie, and even Jérôme Bonaparte (1784–1860). The first patient, a ‘weakly lad of 19 or 20’, could not be made to inhale an adequate quantity of the vapour due to a combination of ‘fright’ and ‘coughing’, and the procedure was terminated. The second patient, by contrast, inhaled the ether ‘con amore’ but ‘appeared to suffer a great deal from it, turning very red, or rather purple in the face and resisting at times somewhat violently’. ‘The effect on the bystanders’, The Times noted, ‘was anything but favourable, several declaring that ether was as bad as the operation, or worse’. Things did not improve for, the patient having become seemingly insensible, the surgeon proceeded to remove his diseased finger, at which point he was ‘at once restored to his senses, and shouted so loudly, and snatched his hand from the operator so vigorously as to leave no doubt that he suffered pain as acutely as if no steps had been taken to deaden it’. Unsurprisingly, the operation was declared ‘a total failure’.Footnote 164
Even in less dramatic cases, patients under ether would often flinch, lash out, or exhibit other convulsive movements. For instance, in January 1847 an ‘Irishman’ having his leg removed at the London Hospital gave ‘sly winks and facetious nods to those surrounding him […] forcing from the bystanders involuntary laughter, and converting that which was to the poor fellow a most tragic event into a scene little short of a farce’. Even so, when the effects of the ether passed off, the patient ‘could scarcely believe that his leg had been so painlessly removed’.Footnote 165 Such cases raised profound doubts, which remain to this day, as to what exactly it was that patients experienced while under the influence of anaesthetic. Though some practitioners firmly believed that ether brought about ‘a complete obliteration of existence’, others were not so sure.Footnote 166 One commentator claimed that there were numerous instances where patients could not move but ‘had been conscious all the time, and have witnessed every step of the operation performed on them’.Footnote 167 Even after the introduction of chloroform, the chemist William Thomas Brande (1788–1866) remained uncertain:
A question had been raised whether sensibility was really annihilated under the influence of these vapours, or whether the patient did not suffer at the time, but had no recollection of the pain on his recovery. This was rather a metaphysical than a physiological part of the inquiry; and there were no facts by which the question could be solved. Some patients had undoubtedly a consciousness of the operation during its performance.Footnote 168
As with mesmerism, then, the early use of ether was marked by disruptive behaviour and uncertain facts. It was, moreover, characterised by equally unreliable testimony. According to The Lancet, ‘As a measure of insensibility to pain, we must be entirely guided by the credibility of the patient, and his own subsequent account of the matter’.Footnote 169 However, when patients were asked to give account of their experiences, which was virtually routine in the early months of 1847, they hardly offered much clarity. For one thing, the ubiquitous expressions of surprise and incredulity elicited from patients who had no recollection of having a leg amputated could easily make ether seem like a cheap parlour trick.Footnote 170 For another, what patients described was, in many cases, unnervingly reminiscent of the more extreme manifestations of mesmeric phenomena. Patients’ experiences under ether ranged from ‘optical illusions’ to full-on hallucinations.Footnote 171 One fourteen-year-old boy, upon regaining consciousness after an eye operation, ‘exclaimed, in a high tone of voice, and with great energy “I have been going to heaven; I have been seeing the angels, and I don’t know what all! I have been going to heaven, that’s all I know about it! Angels and trumpets are blowing!”’Footnote 172 Religious and spiritual visions like this were not uncommon, but neither were more prosaic hallucinations, such as a servant reliving a dispute with his master, or a woman who thought herself in a neighbour’s house surrounded by ‘several parties’ persuading her to submit to the very operation she was then undergoing.Footnote 173 These examples manifest the exact same emotional, moral, and physiological idiosyncrasy that, as we saw in Chapter 3, characterised the cultures of pre-anaesthetic surgery. Hence, what patients did or said during and immediately after operations under ether was often thought to offer an insight into their character. It is perhaps unsurprising, given prevailing social prejudices, to learn that many of the most obstreperous and disruptive patients were identified as Irish.Footnote 174 Likewise, whereas a correspondent to The Lancet thought that being ‘at the bar of judgment pleading for mercy’ from God was the kind of dream ‘which might be expected’ from ‘an interesting and delicate girl [of] good moral and religious character’, a different set of judgements presumably attached to the man who, in ‘throw[ing] his arms about’, thought himself ‘fighting and knocking somebody down in a public-house’.Footnote 175
Another aspect of ether that resembled mesmerism was its erotic connotations and potentialities. In its most extreme form, contemporaries worried that women might be rendered unconscious and sexually assaulted by ethereal assailants.Footnote 176 But even within the managed space of the operating theatre, the eroticised gaze might still manifest itself. For example, in a reference to the performance of the celebrated singer Maria Malibran (1808–36) in the aptly titled La Sonambulista, J. H. Rogers, acting house surgeon to the Middlesex Hospital, described one young woman, who was having a ‘large crop of venereal warts [removed] from the labia’ (and who may therefore have been a sex worker), thus: ‘The expression of her countenance, her action, and tone of voice, bore a striking resemblance to […] the character of Amina, in the scene where she awakes and finds herself in the bed-room of the Count’.Footnote 177
Like mesmerism, ether also, at least for a period, offered the disquieting possibility of expanding consciousness beyond conventional bounds, even to the point of madness. Thus, in February 1847, the surgeon Frederick Thomas Wintle (1803–53), medical superintendent to the Warneford Hospital insane asylum in Oxford, wrote a cautionary letter to The Lancet, citing the case of a ‘talented and intellectual individual’ who ‘had a strange delusion that he could expand the powers of his mind ad infinitum, if he could obtain a free supply of ether’. Sadly, ‘he pursued this delusion so earnestly that his mind became disordered, and, in fact, he suffered paroxysms very nearly allied to delirium tremens’.Footnote 178
As this last observation suggests, ether had potentially problematic associations with ‘altered states’ other than mesmerism. Many commentators noted the parallels between etherisation and the insensibility produced by excessive alcohol consumption as well as the delirium occasioned by opium use, associations that were only enhanced by the testimony of patients.Footnote 179 For example, the unnamed Irishman of the ‘sly winks’, mentioned above, declared ‘let’s have another go at the grog’ before inhaling ether ‘with the greatest avidity’, while a female patient at the Stockport Infirmary, when required to take the vapour for the second time, protested ‘I wish I had said nothing; you are going to give me some more of that stuff that makes folk drunk’.Footnote 180 Likewise, patients recovering from etherisation were often disinclined to be roused from a state that resembled narcotic euphoria. ‘Oh! why did you take me from that beautiful place? Let me go back. Oh! how beautiful! It is heaven!’ declared a 19-year-old girl after a tooth extraction at the Northern Dispensary, while a young man at the Westminster Hospital was recorded as exhibiting ‘a little hysterical sobbing after the operation’, The Lancet noting that, in contrast to the terrors of the past, ‘a surgical operation has now come to be a source of regret, as an enjoyment too quickly passed away’.Footnote 181
In these last two cases the patients were referred to as hysteric and, indeed, the spectre of hysteria dogged early anaesthesia as much as it did mesmerism. W. H. Hewett was not alone in his claim that ‘symptoms of hysteria’ were ‘a frequent occurrence’ of ether ‘when administered to females’.Footnote 182 In fact, not even the advent of chloroform could entirely eradicate this association and John Snow’s case books are full of references to patients exhibiting hysteric symptoms before, during, and after inhaling the vapour.Footnote 183 Having said this, whereas the early use of ether had heralded a frenzy of sensational and diverse reports, by the time Snow came to compile his casebooks in the late 1840s and 1850s, much of the plurality of anaesthetic experience had been tamed, thanks in large part to Snow himself.
It is one of the great ironies of early anaesthesia that its profound novelty made patient testimony far more clinically interesting, relevant, and audible than it had been before. As argued in Chapter 3, prior to 1846 the intraoperative experiences of patients were of comparatively little interest to surgeons. Pain was, after all, a distressing but entirely predictable consequence of cutting, slicing, and sawing the body of a sentient creature, and one of the functions of the culture of operative fortitude was to make the sufferings of the patient ‘more palatable by being refracted through the familiar cultural tropes of pathos and personal self-control’. And yet, if the screaming, writhing patient of the pre-anaesthetic era has been effectively silenced in the historical record, the unconscious patient of early anaesthesia was given remarkable licence to speak, as a returning explorer from the terra incognita of ethereal oblivion. But it was not to last. This astonishing flourishing of patient testimony was to continue for little more than a few months before the operative subject was silenced for good.Footnote 184 It is not just that, by June 1847, ‘the cases had lost all novelty’, though they had.Footnote 185 It was because, by its very diversity and subjectivity, this testimony highlighted the fundamental idiosyncrasy of anaesthetic experience and conjured uncomfortable associations with the vagaries and uncertainties of mesmerism. Indeed, in the early days of anaesthesia, idiosyncrasy was everywhere. In January 1847, for example, The Lancet observed that the ‘insensibility produced by etherization appears to be of a peculiar kind, and to vary considerably in different individuals’, while the following month, John Adams (1805–77) of the London Hospital thought the action of ether on the blood accounted for ‘its power of inducing insensibility […] according to the idiosyncrasy of the patient’.Footnote 186 This was only exacerbated by increasing reports of deaths under ether and, later, chloroform, which raised the disturbing possibility that some patients were physiologically unsuited to the new vapour.Footnote 187
If anaesthesia was going to provide the stable technological solution to the problem of pain that mesmerism had failed to do, such idiosyncrasy had to be eliminated. Chief among the practitioners who attempted to do just this was John Snow. One of Snow’s principal characteristics, as perhaps the most active promoter of anaesthesia in England, was his insatiable quest for uniformity and standardisation.Footnote 188 As historians have shown, proponents of ether and chloroform were aware that patients might respond differently to them.Footnote 189 Snow himself proposed a value-laden hierarchy of influence, suggesting that ‘Those persons whose mental faculties are most cultivated appear to retain their consciousness longest’, while ‘certain navigators and other labourers […] having the smallest possible amount of intelligence, often lose their consciousness, and get into a riotous drunken condition, almost as soon as they have begun to inhale’.Footnote 190 Nonetheless, Snow endeavoured to eliminate any doubt that ether and chloroform were universally applicable. Drawing on his unrivalled experience of its administration, he claimed: ‘From what I have seen, I feel justified in the conclusion that ether may be inhaled for nearly all surgical operations […] with safety and without ill consequences, where due care is taken’.Footnote 191 To this end, he rejected all explanations of patient death that suggested the physiological idiosyncrasies of the patient, such as a weak heart, rendered them unsuitable subjects, suggesting instead that the fault lay in poor technique, particularly in terms of the dosage administered or the method of revival employed.Footnote 192
Snow also sought to banish patient-centred subjectivity from anaesthetic practice. It is notable, for example, that he was a proponent of the use of ether to detect feigned injury among soldiers, with the idea that it might allow the surgeon to bypass subjective testimony to reveal an essential bodily truth.Footnote 193 He also had little time for metaphysical debates about the psychology of patient experience, proposing instead several clearly defined levels of anaesthetic ‘narcotism’ and suggesting that ‘Pain which is not remembered is of very little consequence, and […] should not be judged of by the expressions of the patient’.Footnote 194 Likewise, while he acknowledged that the emotions of the patient might be managed in advance of a procedure, he allowed them no role in the operation itself, claiming that ‘Fear is an affection of the mind, and can no longer exist when the patient is unconscious’.Footnote 195 Moreover, Snow sought to discipline the space of the operating theatre by quietening the post-operative patient, putting an end to those elements of etherisation that evoked the popular spectacle of mesmerism. As he wrote in 1847:
If the patient will remain silent during his recovery from the effects of ether, as he generally will, it is better not to trouble him with questions till he has perfectly regained his faculties, as conversation seems to increase the tendency to excitement of the mind that sometimes exists for a few minutes as the patient is recovering from the effects of ether. This kind of inebriation is sometimes amusing, but is not a desirable part of the effects of ether, more especially on so grave an occasion as a serious surgical operation; and therefore anything that may prevent or diminish it is worthy of attention.Footnote 196
As Stephanie Snow has demonstrated, perhaps her namesake’s most important legacy was his establishment of anaesthesia as a discrete surgical science. From the very early days of etherisation, John Snow had championed the use of specific inhalation apparatus to ensure a safe and controlled administration of vapour. By contrast, James Young Simpson, and many of this followers in Scotland, proposed the use of a simple handkerchief, or other suitable piece of cloth, to administer chloroform to their patients. John Snow opposed this Scottish mode of practice, publishing evidence that the simple infusion of a cloth was associated with a higher fatality rate than his own apparatus. Stephanie Snow locates this disagreement in two contrasting medical cosmologies, one that saw the body as an idiosyncratic entity requiring empirical knowledge, and another that viewed bodies as universal and amendable to predictable laws.Footnote 197 There is much truth in this observation, for Snow’s universalising drive was certainly calculated to minimise personal subjectivity and bodily idiosyncrasy. But as Stephanie Snow recognises, this disagreement also suggests something about divergent understandings of surgical authority and identity. The use of a simple handkerchief was minimally disruptive and allowed the surgeon to retain much of the old way of doing things, including his own untrammelled authority. By contrast, Snow’s apparatus heralded a new era of specialisation and the division of labour.Footnote 198 Moreover, whereas there was something quotidian, domestic even, about the use of a handkerchief, Snow’s inhalation apparatus, visually reproduced in countless articles and books, provided a prescient vision of surgery as a fundamentally techno-scientific practice (Figure 5.2).
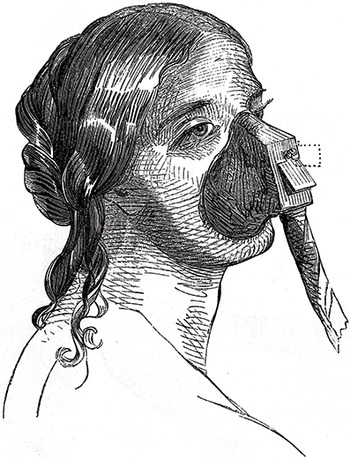
Figure 5.2 John Snow’s Apparatus for the Inhalation of Ether and Chloroform, The Lancet 51:1276 (12 February 1848), p. 179.
The advent of anaesthesia can certainly be said to have constituted a ‘revolution in practice’.Footnote 199 However, it is important to recognise that the transformation it brought about was neither immediate nor absolute and that operations without any form of pain relief would continue for many years.Footnote 200 In fact, surveying the writings of mid-nineteenth-century surgeons, one could occasionally be forgiven for thinking one had missed something. Remarkably, ether and chloroform warranted no special mention in James Syme’s 1853 account of the improvements that had taken place in surgical practice over his thirty-year career, and only a very brief reference, right at the end, in a similar lecture delivered over a decade later.Footnote 201 Meanwhile, in the published version of his introductory address to the surgical pupils of University College London in 1850, John Erichsen (1818–96) relegated chloroform to a couple of footnotes, one of which complicated, if not directly contradicted, his argument about the importance of handling surgical instruments ‘with rapidity’.Footnote 202 Similarly, if one looks at the major textbooks of the period, one often finds anaesthesia grafted somewhat awkwardly onto long-established practices. For example, Erichsen threaded chloroform through the text of his 1854 edition of The Science and Art of Surgery, but continued to recommend measures, such as covering the instruments with a towel or minimising verbal communication between the surgeon and his assistants, that were of little relevance to a world where the patient was rendered unconscious, perhaps even before they entered the operating theatre.Footnote 203 Indeed, it is notable that, by the second edition of 1857, while Erichsen had introduced a whole new section on chloroform, the paragraph on operative preparation and conduct remained unaltered.Footnote 204
Such textual practices serve as a neat exemplar of the more general ways in which anaesthesia was interpolated into established surgical cultures. They also demonstrate that the shift from the emotional regime of Romantic sensibility to one of scientific modernity was gradual and uneven. And yet, there can be little doubt that, ultimately, the introduction of anaesthesia irrevocably transformed the emotional cultures of surgery. As scholars have recognised, anaesthesia did nothing to relieve the pain associated with bodily affliction more generally. Nor did it completely eradicate anxiety and fear at the prospect of surgery.Footnote 205 Indeed, anaesthesia could produce its own anxieties. Writing in 1896, Frederick Treves claimed that ‘The majority of patients regard the anaesthetic with far greater dread than the operation’, for while ‘Of the surgeon’s work they are assured they will know nothing […] they do know that they will be horribly conscious of those palpitating moments which precede the onset of the gruesome and unholy sleep’.Footnote 206 Treves’ description of anaesthetic sleep as ‘gruesome and unholy’ attests to its continued ambiguity, but it is important to remember that these words were written half a century after the introduction of ether and that the dread of anaesthesia was significant precisely because, by rendering surgery effectively painless, it had removed much of the dread of the operation itself. In this it was truly revolutionary. But that was not all; anaesthesia also reshaped surgical experience and identity in profound and lasting ways. Indeed, it is remarkable how many surgical commentators of the period reflected on the impact that ether and chloroform had upon them as much as on their patients. The Edinburgh surgeon James Miller, who was one of the foremost early advocates of anaesthesia, dedicated a whole section of his Surgical Experience of Chloroform (1848) to the fact that ‘Anaesthesia affords great relief to the operator as well as to the patient’. Reflecting on the emotional burden it had lifted from the shoulders of surgeons, he wrote:
To no ordinarily constituted man is pain otherwise than repugnant; whether it occur in himself or in another. And, hitherto, there can be no doubt that his being compelled to inflict pain, and witness the infliction of it, has always been esteemed by the surgeon as the hardest portion of his professional lot. Now this is gone. He proceeds to operate with a mind wholly unoccupied with regard to the feelings of his patient; for he knows that all the while he will be in unconscious sleep.
By silencing the patient, anaesthesia transformed the sensory landscape of the operating theatre and rendered operative surgery far more palatable. The blood and gore remained, of course, but to Miller this was not the issue. ‘Whence was it that students, dressers, and even surgeons grew pale, and sickened, and even fell, in witnessing operations?’ he asked:
Not from the mere sight of blood, or of wound; but from the manifestation of pain and agony emitted by the patient. And, now-a-days, this patient—whatever his age, or sex, or however nervous, timid, and apprehensive— gives not one sign of pain, or even discomfort, but lies in happy slumber all the while. A snort is the worst sound that he makes.Footnote 207
For surgeons such as William Fergusson (1808–77), the sensory experience of the operation might now even be actively pleasurable. ‘[I]nstead of wild outcries or stifled screams and groans coming from the patient under the surgeon’s instruments’, he suggested, the patient ‘may be made to lie as quietly as if in a calm sleep, or […] he may be mentally engaged in the most pleasing associations of thought, or singing or humming by snatches some favourite air’.Footnote 208
While the somnolence and somniloquy of the anaesthetised patient encouraged metaphors of sleeping and dreaming, the remarkable indifference of the patient to the physical trauma of surgery also invited comparison with the dissected corpse.Footnote 209 Reflecting on an early operation under ether to remove a diseased eye, for example, William Lawrence compared the previous patient he had treated for such a condition who ‘writhed in agony, not being able to control himself’ with his etherised subject who ‘lay like a body on a dissecting table, without the slightest manifestation of suffering or even consciousness, without a movement of any part’.Footnote 210 Where surgical dissection had once prepared surgeons only incompletely for their operative duties, now the two practices were virtually identical and eradicated the need for surgeons to hurry themselves. ‘[A]s there is no cause or excuse for haste in operating on a dead body stretched on a dissecting-table’, Miller wrote, ‘so there is as little cause or excuse for haste in operating on an anesthetized body of a living patient’.Footnote 211
This chapter thus comes together in the figure of the quiescent surgical body, for whether the insensible patient was dead, asleep, or somewhere in between, the emotional regime of utilitarian and techno-scientific surgery all but severed the essential intersubjectivity that had shaped the surgical cultures of the Romantic era. In both the dissecting room and the operating theatre, the surgeon might now work ‘with a mind wholly unoccupied’ by feeling. For some, this was a problem as much as a benefit. As historians have noted, there were a number of contemporaries who believed that pain was a necessary part of surgical operations.Footnote 212 Roger Sturley Nunn (1813–82), reflecting on a fatal case under ether at the Essex and Colchester Hospital in February 1847, for example, wrote that ‘Pain is doubtless our great safeguard’ and ‘should be considered as a healthy indication, and an essential concomitant with surgical operations’.Footnote 213 Meanwhile, no less an authority than Bransby Cooper stated ‘that pain was a premonitory condition’ and that ‘he should feel averse to the prevention of it’.Footnote 214 Such sentiments were given short shrift by James Miller, who, in what was surely a play on Thomas Paine’s Rights of Man (1791), decried the ‘small party’, including the notorious vivisector François Magendie (1783–1855), who, in the face of an unalloyed boon for humankind, asserted instead ‘the rights of pain’.Footnote 215 Indeed, one of the effects of anaesthesia was to divest pain of almost all of its moral value. In a remarkable address to the Hunterian Society in February 1848, for instance, Thomas Blizard Curling (1811–88) declared that the pain caused by the surgeon’s knife was unquestionably ‘an evil’ and that the ‘Fortitude displayed under suffering is […] not always so great as it appears’ because it was often a product of a physiological ‘incapacity of feeling pain’ rather than the expression of ‘moral courage’. He even went so far as to suggest that ‘monomaniacs’ who took a ‘morbid pleasure’ in pain, such as a woman whose breast was found to be ‘full of pins and needles’, fully confirmed that there was no inherent nobility in pain.Footnote 216
But pain was not the only issue. Some surgeons objected to the lack of cooperation that had once been the hallmark of the intraoperative relationship between surgeon and patient, at least in its more idealised forms. Even as late as 1855, William Coulson (1802–77) could ask John Snow whether it was ‘always desirable to suspend sensation during surgical operation’, suggesting that there were cases, such as lithotrity, ‘a delicate operation […] carried on, as it were, in the dark’, where ‘the patients’ sensations are the chief guide which direct the surgeon when he is going wrong’.Footnote 217 Moreover, there were others for whom the haptic qualities of the newly anaesthetised operative subject were deeply unnerving. According to Cooper, ‘with the exception of the flow of blood, it was like cutting through dead flesh’, and in the case of lithotomy ‘the parts fell, as it were, asunder, and the sensations were quite different on passing the finger into the bladder’.Footnote 218 Similar sentiments were also expressed by Henry Haynes Walton (1816–89) who, following up on Coulson’s questioning, claimed that in the case of cataract, ‘the lens did not start so freely after the division of the cornea as when chloroform was not used, but was more like the lens of a dead body’.Footnote 219
If such quibbling from Miller’s ‘small party’ was relatively short-lived (Miller was using the past tense, even in 1848), other concerns took somewhat longer to recede. Anaesthesia had become widespread by the 1860s, but the relative risks of ether and chloroform were still being debated in the 1870s and beyond.Footnote 220 Moreover, for some the problem with chloroform lay not in its potential toxicity or its eradication of surgical intersubjectivity, but in the fact that it had opened up a brave but uncertain new world of operative ambition. In 1851 The Lancet contemplated the moment, four years earlier, when surgeons no longer had to endure ‘the cry of agony issuing from the frail body of some poor nervous, emaciated woman, whose breast was about to be submitted to the knife; nor the scarcely less painful effect of subdued emotion, in the strong frame, while it quivered under the strokes of the scalpel’. ‘The surgeon’, it remarked, no longer had to ‘contend against these calls upon his humanity’. However, it cautioned, ‘Like all such blessings [chloroform] has its drawbacks and evils, amongst the more conspicuous of which may be mentioned the facility with which patients are now persuaded to submit to the knife, and the encouragement which it holds out to what are called “promising young men” to “carve their way into practice”’. With the patient unconscious, surgeons could now intrude deeper into those cavities of the body that had previously eluded them, continually extending their epistemological empire. Citing the highly controversial practice of ovariotomy as the most ‘frightfully illustrative’ example of this ‘operating mania’, it noted that a surgeon might now remove an ovarian tumour ‘with as much nonchalance as though it were being removed from the dead body in the dissecting-room’.Footnote 221 Looking back to the generation of surgeons immediately before anaesthesia, his generation, Wakley remarked that those modern surgeons ‘who would vainly aspire to walk in the footsteps of a COOPER or a LISTON’ would do well to remember that ‘Such men as these did not operate for the sake of cutting: they resorted to the knife only as a substitute, and that, to them, a lamentable one, for other […] resources of surgery’.Footnote 222
Conclusion
Before long Wakley would pass away, as would the very notion of the pre-anaesthetic era as a model of surgical practice. As we shall see, surgeons of the later nineteenth and early twentieth centuries would solidify the emotional regime of scientific modernity in part through their casting of what had come before as a diabolic counterpart to their own technical and technological sophistication. While surgical innovation could still provoke controversy, the expanding empire of surgery was less a cause for concern than for celebration, mirroring as it did the British state’s own increasingly acquisitive territorial ambition.Footnote 223 Moreover, where opponents both of anatomical dissection and of anaesthesia had often couched their concerns in terms of the individual patient, the harbingers of a scientific surgical modernity would, by the 1880s at least, appeal less to the individual case than to the statistically demonstrable collective good. Though this shift of emotional focus from the individual to the social would become even more pronounced as the century wore on, this chapter has located its origins in the period between 1820 and 1850 and, in particular, in the cultural and ideological influence of utilitarianism. But it has also shown that this shift was not limited to Benthamites, nor was it without ambiguity or complexity. Emotional intersubjectivity did not disappear overnight, nor, as we shall see, did the language of sentiment. The tone, however, had changed for good. Recalling the visit of the celebrated Scottish divine Thomas Chalmers (1780–1847) to witness one of his first operations under ether, James Miller claimed that it was
one of the early triumphs of Anaesthesia […] to see that man of large and tender heart witnessing a bloody and severe operation, with composure and serenity; feeling little, because the patient felt not at all; and the little that he himself did feel, far more than compensated by the thought, that a brighter day for that suffering humanity, with which he so closely and continually sympathized, had at length dawned, and that, from henceforth, throughout the domain of surgery, injury and disease were shorn of half their terrors.Footnote 224



 Open access
Open access
{kind=link}