


Use of dietary supplements is common in many Western countries including Australia, where national data indicate that almost a third of adults use these products( 1 ). However, the efficacy and safety of dietary supplements have long been debated( Reference Hathcock 2 ). Carbohydrate and/or protein drinks can offer benefits during an extended period of intensive exercise( Reference Jimenez-Flores, Heick and Davis 3 , Reference Naclerio and Larumbe-Zabala 4 ), or iron and calcium supplements can be beneficial for persons with low dietary intakes of these nutrients( Reference Craig and Mangels 5 ). Due to the high physical demands commonly experienced by military personnel, they choose to use dietary supplements to improve energy levels, performance, muscle strength and endurance, and to promote general health( Reference Lieberman, Stavinoha and McGraw 6 ). Overweight and obesity are also increasingly affecting military populations( Reference Peake, Gargett and Waller 7 , Reference Reyes-Guzman, Bray and Forman-Hoffman 8 ), which may lead to use of supplements marketed for weight loss in this population group, to help them to meet the fitness standards required for employment in military services.
However, many of the available supplements offer no health benefits( Reference Jenkinson and Harbert 9 ) and some may cause harm when multiple supplements are used, when intake exceeds the recommended dose( Reference Bishop 10 ) or when their use causes a person’s total intake to exceed recommended levels. For example, caffeine and creatine supplements can have ergogenic and performance-enhancing effects( Reference Trexler and Smith-Ryan 11 , Reference Spriet 12 ), but caffeine-containing supplements add to the caffeine intake from drinks and caffeine intake levels in US military personnel have been reported to be high( Reference Lieberman, Stavinoha and McGraw 13 ). Some studies have shown possible risks associated with high caffeine intake, including a negative effect on sleep patterns( Reference Clark and Landolt 14 ), although the effects of high caffeine intake on sleep quality in a combat environment have not been established definitively( Reference Waits, Ganz and Schillreff 15 ). Certain weight-loss related supplements have been associated with gastrointestinal distress and nervousness( Reference Burke, Seda and Allen 16 , Reference Manore 17 ).
Current evidence indicates that use of dietary supplements by military personnel is higher than that in the general population in Western countries. More than 50 % of US soldiers( Reference Lieberman, Stavinoha and McGraw 6 ) and almost 40 % of British soldiers in training( Reference Casey, Hughes and Izard 18 ) reported use of dietary supplements, with many using multiple products; and use is higher in army personnel serving in conflict zones( Reference Boos, Simms and Morris 19 , Reference Austin, McLellan and Farina 20 ). Products targeting muscle strength, muscle mass and endurance are favoured by British and US military personnel( Reference Lieberman, Stavinoha and McGraw 6 , Reference Boos, Simms and Morris 19 , Reference Boos, Wheble and Campbell 21 – Reference Austin, Price and McGraw 23 ), and weight-loss supplements are also commonly used by US military personnel( Reference Greenwood and Oria 24 ).
Most of the evidence on use of dietary supplements by military personnel comes from data collected on US and British military personnel, but evidence for Australian military personnel, who can take typical multivitamin preparations approved by the Australian Therapeutic Goods Administration at recommended doses without prior approval, is lacking. We therefore investigated levels and patterns of use of dietary supplements by Australian military personnel, particularly those who have experienced deployment to conflict zones. We studied the characteristics of dietary supplement users by assessing general demographic factors, service and lifestyle factors, and mental and physical health status.
Methods
Study design and participants
We analysed data from a large cross-sectional survey of current and ex-serving Australian Defence Force (ADF) members who deployed to the Middle East Area of Operations (MEAO) between 1 October 2001 and 31 December 2009( Reference Dobson, Treloar and Zheng 25 ). This survey included MEAO veterans deployed to Iraq or areas supporting operations in Iraq (including ships in the Persian Gulf), those deployed to Afghanistan or areas supporting operations in Afghanistan, and those attached to foreign militaries or the UN in the above areas. A small proportion (6 %) of participants had left the ADF since serving in the Middle East. These ex-serving personnel were included in the present study to capture current supplement use of all persons who had served in the Middle East previously and improve representation of all those who served.
Data collection
Data were collected in 2010 and 2011 through online surveys or hard copy questionnaires that were sent to all eligible current and former ADF members for completion. Participation was voluntary and anonymous. Full details on the participant recruitment, response rates, survey design and methodology are documented elsewhere( Reference Dobson, Treloar and Zheng 25 ). In brief, all participants completed a questionnaire that asked about demographic characteristics, their role during the most recent deployment, current health status, lifestyle behaviours and health symptoms. Participants were asked the following questions in relation to their supplement use: ‘How often do you currently take any of the following supplements? Body building supplements (such as amino acids, weight gain products, creatine etc.); Energy supplements (such as energy drinks, pills, or energy enhancing herbs); Weight loss supplements?’, with response options of ‘never’, ‘less than once a month’, ‘monthly’, ‘weekly’ and ‘daily or almost daily’. The respondent was then asked to record the name (generic or brand name) of the supplement they used, for each of the three categories.
The supplement brand name and type listed by the participant were entered into an Internet search engine to verify the product was a dietary supplement and to obtain product information. Products in each of the three supplement categories (bodybuilding, energy and weight loss) were coded into sub-categories based on the most prominent type of ingredients, including protein and amino acids, multivitamins and herbs, carbohydrates and sugars, stimulants, and creatine monohydrate. We further identified which products contained either creatine or caffeine in each sub-category, given the concern about possible side-effects associated with these ingredients. Manual coding of the data was undertaken by one author and incongruities were resolved through discussion with all authors.
Lifetime smoking history was self-reported in three categories (current smoker; ex-smoker; never smoker) and caffeine use was ascertained as the reported average daily consumption of caffeine-containing beverages (250–375 ml) grouped into four categories (none; 1–2 per day; 3–5 per day; 6 or more per day). Participants were asked to report whether they experienced selected health symptoms (e.g. sleeping difficulties, headaches, vomiting) in the past month. The Short Form-12 Survey (SF-12)( Reference Ware, Kosinski and Keller 26 ) was completed as part of the study questionnaire, and summary component scores for physical and mental health calculated using standardised methodology. Major depressive syndrome was derived using the Patient Health Questionnaire (PHQ-9) Depression module, which evaluates the frequency of nine DSM-IV (the Diagnostic and Statistical Manual of Mental Disorders, 4th edition) criteria for major depression syndrome in the last two weeks( Reference Kroenke, Spitzer and Williams 27 ). Major depression was considered present if five or more of the nine depressive symptoms were reported more than half the time in the past two weeks, and if one of the symptoms reported was depressed mood or anhedonia.
Ethical approval for the present study was obtained from the Australian Department of Defence (protocol number LREP 14-010) and The University of Queensland (protocol number 2009001441) ethics committees. Participants of the MEAO Survey provided consent in writing or electronically, and all aspects of this research complied with the Declaration of Helsinki.
Statistical analysis
We assessed the proportion of respondents who reported using supplements in each of the three supplement categories by subgroups of general demographic characteristics, service and lifestyle characteristics, and the presence or absence in the past month of a number of specified health symptoms. Differences between subgroups were ascertained by using binary logistic regression analysis to calculate OR and 95 % CI. Univariate comparisons were followed by multivariable-adjusted models with adjustment for possible confounding by all other demographic, service and lifestyle factors considered (only factors with evidence of confounding, based on evidence from the literature and changes in the risk estimate when the covariate was included, were retained in the model). Physical and mental health scores from the SF-12 instrument were continuous variables and comparisons between subgroups carried out using multivariable linear regression weighted for non-response. The total number of health symptoms was modelled as a count variable, using the negative binomial model with robust se. All data were weighted for non-response, based on the response rates in the three service groups (Navy, Army, Air Force), four service status groups (active regulars, active reserves, inactive reserve, ex-serving), three rank categories (commissioned officers, non-commissioned officers, other ranks), and among males and females. This resulted in seventy-two strata and weights calculated were the inverse of the response rate in each stratum. Count data (number of participants) in subgroups of supplement use are presented as unweighted data, but all summary statistics such as percentages, means and OR were based on weighted data. All analyses were carried out using the statistical software package SAS version 9.3.
Results
A total of 26 239 eligible ADF members were invited to participate and 14 032 (53 %) responded to the survey. Most of the respondents were male (88·9 %), mean age was 37 years (range 18–68 years), and 49·3 % were Army, 23·6 % Navy and 27·1 % Air Force personnel. Alcohol use was common (48·3 % consumed 1–2 alcoholic drinks/d, 33·9 % drank 3–5 alcoholic drinks/d and 6·1 % drank ≥6 alcoholic drinks/d), and 28·2 % were current smokers. A small proportion (6·0 %) of the participants had left the ADF since serving in the Middle East. Mean age of ex-serving participants (36·4 years) was similar to that of active regular personnel (35·8 years), while the average age of active reserve and inactive reserve personnel was slightly higher (39·7 and 37·2 years, respectively).
Analysis of non-response was reported previously( Reference Dobson, Treloar and Zheng 25 ) and showed that response rates were higher among females (59 % of females responded v. 52 % of males), older persons (67 % of those aged ≥45 years responded v. 39 % of those aged 18–25 years old), personnel of the Air Force (60 % responded v. 50 % of those in the Navy and 51 % of those in the Army), those ranked as officer (63 % of officers responded v. 35 % of those in other ranks) and personnel actively serving in the military (58 % of those in active employment responded v. 32 % of ex-serving personnel).
Use of dietary supplements was common among the study participants, with 21·5 % of respondents using a dietary supplement in any of the three categories once weekly or more often. Overall, 32·3 % of participants used any of the three types of supplement investigated (at any frequency of use), with bodybuilding supplements (17·5 %) and energy supplements (24·5 %) used more often than weight-loss supplements (7·6 %); 11·6 % of participants used supplements in more than one category. A large proportion of users of bodybuilding supplements used these daily (47·9 %), while 21·7 % used these weekly and 30·4 % monthly. Energy supplements were used daily by 28·8 % of users of these supplements, weekly by 27·1 % and monthly by 44·2 %. Weight-loss supplements were used daily by 42·5 % of respondents who used such supplements, weekly by 15·5 % and monthly by 42·0 %. The number of different bodybuilding supplements used per person ranged from 1 to 5 different products (average 1·1 products per person), and this ranged from 1 to 4 different products (average 1·0 product per person) for energy supplements, and from 1 to 2 different products (average 1·0 product per person) for weight-loss products.
Types of supplements
In terms of the types of supplements used, amino acid and protein supplements were most commonly used. Overall, 51·5 % of supplement users used amino acid and protein products, followed by multivitamin or herb compounds (14·9 %) and carbohydrates and sugars (11·9 %). Overall, 40·0 % of all supplement users used a supplement containing caffeine (11·7 % of all study participants) and 12·2 % of supplement users took a product containing creatine (3·6 % of all study participants), including 4·1 % who used a pure creatine monohydrate product.
Table 1 and Fig. 1 show the distribution of supplement types reported within the three categories of supplements investigated. Users of bodybuilding supplements most commonly used amino acid and protein supplements, typically taken as bars or powder (90·1 % of all bodybuilding supplement users used these products). Multivitamin and herb compounds marketed to aid bodybuilding were also commonly used as a bodybuilding supplement (9·3 %), followed by products predominantly containing creatine monohydrate (8·5 %) and other products (2·8 %). Besides creatine, multivitamin and herb products marketed for bodybuilding also commonly contained caffeine (24·0 % of such products).
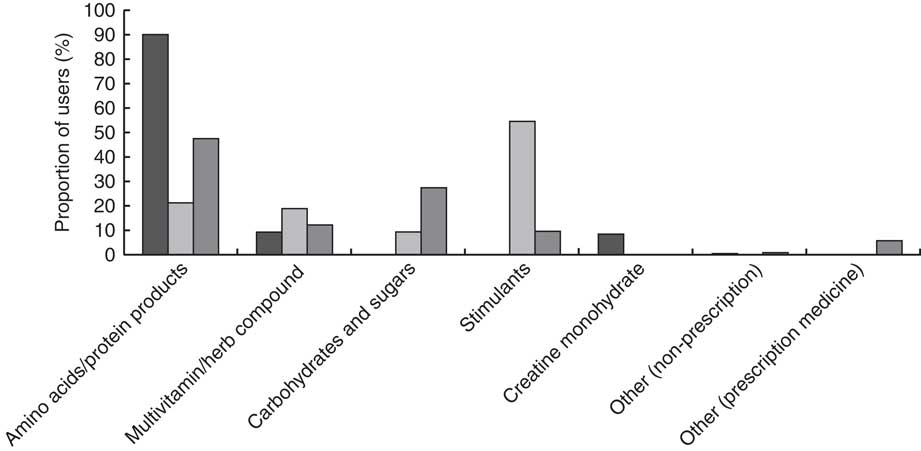
Fig. 1 Subgroups of supplements (![]() , bodybuilding supplements;
, bodybuilding supplements; ![]() , energy supplements;
, energy supplements; ![]() , weight-loss supplements) used by current and ex-serving Australian Defence Force personnel (n 14 032) who deployed to the Middle East between 2001 and 2009
, weight-loss supplements) used by current and ex-serving Australian Defence Force personnel (n 14 032) who deployed to the Middle East between 2001 and 2009
Table 1 Subgroups of supplements used by used by current and ex-serving Australian Defence Force personnel (n 14 032) who deployed to the Middle East between 2001 and 2009
* Total number of Australian Defence Force personnel in these categories do not equal to the sum of column responses because participants may have used more than one type of bodybuilding/energy/weight-loss supplement.
Users of energy supplements most commonly used products that contained stimulants (54·6 % of all energy supplement users), almost always including caffeine. Users of energy supplements also often reported using amino acid and protein products (21·2 %), as well as multivitamin and herb products (18·9 %), but less often (9·3 %) products that predominantly contained carbohydrates and sugars. Users of weight-loss supplements most often used products that supplied protein and amino acids (47·5 %), carbohydrates and sugars (27·4 %), or multivitamin and herb compounds marketed to support weight loss (12·2 %). Stimulants (9·6 %), mainly containing caffeine (97·4 % of such products), were also used as weight-loss supplements, while a small proportion of weight-loss supplement users (5·8 %) reported using prescription medicines to support weight loss.
Factors associated with supplement use
Men were more likely than women to use bodybuilding and energy supplements, while women were more likely to use weight-loss supplements. There was a clear age-related pattern of use, particularly for bodybuilding and energy supplements, with around a third of the youngest participants (aged 18–29 years) using such supplements, compared with less than 15 % of the oldest (≥40 years of age) study participants (all P < 0·001; Table 2).
Table 2 Associations between general demographic, service and lifestyle factors and use of dietary supplements by current and ex-serving Australian Defence Force personnel (n 14 032) who deployed to the Middle East between 2001 and 2009
AOR, adjusted odds ratio; ref., reference category.
* Unweighted totals; totals may not add up due to missing responses.
† Percentages weighted for non-response; percentages may not sum to 100 due to rounding.
‡ Adjusted binary logistic regression models include all demographic, service and lifestyle variables listed in the table.
§ Adjusted binary logistic regression models include the variable of interest adjusted for the confounding effects of gender, age group, service, rank, smoking history at survey completion and main role on deployment.
║ Adjusted binary logistic regression models include the variable of interest adjusted for the confounding effects of gender, age group, service, rank, caffeine use at survey completion and main role on deployment.
Army personnel were more likely to use of bodybuilding and energy supplements (about 25 % for both types of supplements) compared with Navy and Air Force personnel (12·2–24·0 %), while use of weight-loss supplements was somewhat more common in Navy personnel (9·2 %) compared with Army and Air Force (8·2 and 5·0 %, respectively). Use of supplements (any type) was generally highest among personnel in lower ranks, those deployed in active regular service and in combat positions (Table 2).
There was some evidence of an association between supplement use and other lifestyle factors. Current smokers were more likely to use energy and weight-loss supplements than never smokers, although differences between these groups were small (Table 2). Participants with a high intake of caffeine-containing drinks (≥6 cups/d) were more likely to use energy and weight-loss supplements compared with persons who did not consume caffeine-containing drinks, while bodybuilding supplements were less frequently used by participants with moderate (3–5 cups/d) intake levels of caffeine-containing drinks compared with respondents who did not consume such drinks (Table 2).
Health status
In terms of recent symptoms reported by study participants, there were consistent patterns within each of the three categories of supplements (Table 3). Participants who used bodybuilding supplements reported less frequently than non-users that they suffered from a range of health problems including headaches, sleeping difficulties, flatulence, diarrhoea and indigestion, whereas such problems were more common among users of energy supplements and weight-loss supplements compared with non-users (Table 3). Multivariable modelling showed that these patterns were independent of the general demographic and job characteristics associated with supplement use, as identified in Table 2.
Table 3 Associations between physical and mental health and use of dietary supplements by current and ex-serving Australian Defence Force personnel (n 14 032) who deployed to the Middle East between 2001 and 2009
AOR, adjusted odds ratio.
* Binary logistic regression models comparing users v. non-users, adjusting for sex, age group, service, rank, service status, main role during most recent deployment, current smoking status (bodybuilding and energy supplements only) and consumption of caffeine-containing drinks (bodybuilding and weight-loss supplements only).
† Unweighted means and sd.
‡ Unweighted means and sd of Short Form-12 Health Survey Physical Component Score.
§ Unweighted means and sd of Short Form-12 Health Survey Mental Component Score.
Major depressive syndrome was more common in users v. non-users of energy supplements (4·2 v. 3·4 %) and weight-loss supplements (6·3 v. 3·4 %), but did not differ between users and non-users of bodybuilding supplements after adjustment for confounders (Table 3). Also, in terms of summary measures of physical and mental health (using the SF-12 assessment tool), physical health scores were lower on average for users of weight-loss supplements compared with non-users, but physical health was better in users compared with non-users of bodybuilding supplements (Table 3). Mental health summary scores were lower in users of energy and weight-loss supplements compared with non-users. The frequency of supplement use among users was lower for bodybuilding supplements and higher for energy supplements if the participant reported recent health symptoms; there was no such pattern for weight-loss supplements (detailed results not shown).
Discussion
Our findings show that bodybuilding, energy and weight-loss supplements are commonly used by Australian military personnel who have served in the Middle East: about one in three persons reported using at least one of these types of supplements, with one in five persons using a supplement at least once weekly. This level of supplement use appears to be higher than that in the general Australian population. National survey data showed that 19 % of Australian males aged 19–30 years, and 25 % of women in the same age group, use dietary supplements( 1 ), although specific national data on the types of supplements assessed in our study are not available for direct comparisons. We did not ask participants to report their reasons for dietary supplement use, but data from British Army soldiers suggest that general improvement of physical performance, and preparation prior to and recovery after training or physical activity may be the main motivating factors for choosing to use dietary supplements among military personnel( Reference Casey, Hughes and Izard 18 ). US data indicate that energy drinks tend to be used by Army personnel to boost energy and enhance mental alertness( Reference Stephens, Attipoe and Jones 28 ).
Compared with other military populations, supplement use was not as common in our study of Australian military personnel as in similar groups in other countries. A large survey of more than 16 000 US military personnel in 2005 indicated that 25 % used bodybuilding supplements (compared with 17 % in our study) and 21 % used weight-loss supplements (compared with only 7 % in our study), while use of energy supplements could not be compared directly between the two studies( Reference Kao, Deuster and Burnett 29 ). Very similar to our observations, use of bodybuilding supplements was more common in US Army than Navy and Air Force personnel, and more common in younger than older persons, in men, and in non-smokers compared with smokers( Reference Kao, Deuster and Burnett 29 ). Results from the US Millennium Cohort Study also indicated a higher overall use of supplements in US compared with Australian military personnel, with 47 % of US military personnel reporting use of at least one type of bodybuilding, energy or weight-loss supplement (compared with 32 % in our study). In particular, the use of energy supplements (38 %) and weight-loss supplements (19 %) was much higher in US compared with Australian military personnel( Reference Jacobson, Horton and Smith 30 ). The level of dietary supplement use in our study participants appears more similar to the level of use reported by British than US military personnel. In a survey of UK-based soldiers in training, 38 % reported current use of supplements, most commonly protein supplements and energy drinks( Reference Casey, Hughes and Izard 18 ), which is comparable to the level of use reported in our study.
Our data indicated quite clear patterns of personal characteristics that were associated with use of supplements. Bodybuilding supplements tended to be used more often by individuals in active service, with better health behaviours and of better self-reported health (with a lower level of supplement use if the person reported health symptoms). In contrast, use of energy and weight-loss supplements was not associated with service status (active or inactive), and these supplements were more commonly used by participants with poorer health behaviours and with poorer physical and mental health. However, differences in mental and physical health between groups were generally very small and the clinical significance of these differences is uncertain.
This patterning of demographic characteristics with supplement type is very similar to that observed in other studies. For example, in the US Millennium Cohort Study, users of bodybuilding supplements were generally younger, more physically active and healthier, while users of energy and weight-loss supplements tended to be less physically active and to have poorer health indicators( Reference Jacobson, Horton and Smith 30 ). Similarly in British Army soldiers in training, overall use of dietary supplements was associated with higher levels of physical activity, although supplement use was higher in smokers compared with non-smokers( Reference Casey, Hughes and Izard 18 ); we could not directly compare data for subgroups of supplements.
Associations with recent health symptoms and summary measures of health status also showed fairly consistent patterning, in that users of bodybuilding supplements had better physical and mental health, in contrast to users of energy and weight-loss supplements. This pattern of associations is very similar to that reported for US Army staff( Reference Jacobson, Horton and Smith 30 ), including that of a large survey of US Armed Forces which found that multivitamin/minerals and protein/amino acid supplements were associated with better general health, eating habits and fitness levels( Reference Austin, McGraw and Lieberman 31 ). Recent US data also indicated that the use of a combination of dietary supplement products is most commonly associated with side-effects( Reference Knapik, Trone and Austin 32 , Reference Austin, Farina and Lieberman 33 ). However, because details of health symptoms in our study participants were not specifically reported in the context of dietary supplement use, we cannot draw any conclusions about side-effects from our data.
We found that the prevalence of major depressive syndrome was twice as high in users of weight-loss supplements than among non-users of weight-loss supplements. Due to the cross-sectional nature of our data collection we are unable to ascertain which factors are causes and which factors are consequences in these associations, but this observation raises the possibility that the increasing prevalence of overweight and obesity among military populations( Reference Peake, Gargett and Waller 7 , Reference Reyes-Guzman, Bray and Forman-Hoffman 8 ) may have impacts on mental as well as physical health in this group. Measures of overweight or obesity were unfortunately not available for our study participants.
We were particularly interested in the use of supplements that contain caffeine. Military personnel may have higher levels of caffeine intake than the general population because caffeine alleviates the adverse cognitive consequences of sleep deprivation (e.g. due to long work shifts) and it enhances physical performance( Reference Lieberman, Stavinoha and McGraw 13 ). However, there is also concern about possible side-effects of high caffeine intake( Reference Cohen, Attipoe and Travis 34 , Reference Wesensten 35 ), such as disturbed sleep patterns( Reference Clark and Landolt 14 ) as a result of use of caffeinated products during overnight periods of sustained wakefulness.
In our study, sleeping difficulties were higher in users of energy supplements (55 % of which contained caffeine) and weight-loss supplements (13 % of which contained caffeine) compared with non-users of such supplements. However, because of the cross-sectional nature of our data, and because we were unable to quantify caffeine intake, it is not possible to draw any firm conclusions about the role of caffeine-containing supplements in these health symptoms. Nevertheless, our data show that use of caffeine-containing supplements was common (11·7 % of all participants used these), which adds to the caffeine intake obtained from caffeine-containing drinks (40 % of respondents consumed three or more caffeine drinks daily), raising the possibility of very high caffeine intake levels in some persons. Observations from US military personnel have also indicated that use of caffeine-containing energy drinks is very common, particularly among young males, and that sleeping difficulties may be associated with this( Reference Stephens, Attipoe and Jones 28 ). Our data did not facilitate calculation of total caffeine intake for the study participants. However, it is known that the caffeine content of supplements is highly variable and poorly listed in product information( Reference Cohen, Attipoe and Travis 34 ), and thus difficult to quantify. A more detailed study on levels of caffeine intake in the Australian military, or monitoring of levels of intake at an individual level, and its impact on the health of serving personnel may therefore be warranted.
Our study is the first to report supplement use in Australian military personnel, and a major strength of the study is its large number of participants and comprehensive assessment of physical and mental health, as well as demographic and lifestyle factors. Other strengths include the fact that the response rate compared favourably with other, similar studies (as discussed in detail in the MEAO Survey report( Reference Dobson, Treloar and Zheng 25 )) and the results were weighted for non-response to control for potential response bias. Furthermore, standard, validated instruments were used, which allows comparison with other military and civilian studies.
However, the study has some limitations that need to be considered when interpreting the results. The data on dietary supplement use were self-reported by the study participants and such self-reporting may be influenced by reporting biases( Reference Sikkens, van Eijsden and Bonsel 36 ). It is a cross-sectional study and thus we were unable to ascertain whether health symptoms were a cause or a consequence of supplement use. Health status indicators were based on self-reported data, which may be affected by recall bias. However, these health data were collected as part of a larger health survey and not specifically in the context of a study of dietary supplements, thus it is very unlikely that misreporting (if any) caused a systematic bias in our present analyses. Full details on the frequency dose of supplements taken, and use of dietary supplements other than those in the categories reported here, were not ascertained in the MEAO Survey questionnaire. Thus, unfortunately, we cannot directly compare absolute amounts of supplement use (of any type) with other populations.
There is a variety of reasons why patterns of dietary supplement use may be different among military (and general) populations of different nations, for example due to different availability of supplements, diverse product ranges, different marketing practices, different regulatory laws, differences in dietary and related health habits, etc. One of the problems with comparisons between different studies is the differences in the definition of ‘supplement user’. For example, we have chosen to focus our analyses on supplement users at any frequency of use, similar to others( Reference Casey, Hughes and Izard 18 , Reference Jacobson, Horton and Smith 30 ), while some different studies have focused on persons who use a dietary supplement at least once weekly( Reference Lieberman, Stavinoha and McGraw 6 , Reference Knapik, Trone and Austin 32 ). The questionnaire items relating to dietary supplement use in the larger health questionnaire of the MEAO Survey, from which our data were extracted, were designed to focus on the intended use of supplements (bodybuilding, energy or weight loss). However, in our analyses we have also incorporated a more ingredient-focused categorisation (amino acids, multivitamins, etc.), to the best of our ability given the available data and resources. While direct comparisons of dietary supplement use in different nations will always have limitations due to the inherent differences in dietary supplement products available around the world, it would be very useful if an agreement could be reached over a standardised method of categorising these products, as well as the frequency of use that would characterise someone as a regular supplement user.
We were able to find product information for almost all supplements reported by the study participants, but a very small number of misclassifications may have occurred. We observed that products that may be quite similar in composition are sometimes marketed for divergent purposes of use (e.g. protein supplements are marketed as bodybuilding supplements as well as weight-loss supplements), and conversely there are products that fall into the same category (e.g. weight loss) but have very little overlap in terms of ingredients( Reference Geller, Shehab and Weidle 37 ). This makes it difficult to study health effects of specific supplement ingredients in detail, but at the same time this emphasises the need to monitor for possible side-effects of dietary supplements at an individual level, including among military personnel( Reference Siano 38 ). General provision of information about dietary supplements( 39 ) would be prudent for military personnel. Military personnel are known to be healthier on average than members of the general population (the healthy soldier effect( Reference McLaughlin, Nielsen and Waller 40 )), but our findings indicate that regardless of their better health, use of dietary supplements is very common among Australian military personnel. Our data may help those in charge of reviewing the health status of ADF personnel to identify priorities for further, more detailed investigations of supplement use by military personnel, and to review the potential risks associated with use of certain dietary supplements in this large population group. The recent banning of all DMAA (dimethylamylamine) containing supplements by the Australian Therapeutic Goods Administration illustrates the need for regulation to prevent avoidable risks to the health of military personnel and the population at large.
Conclusion
In conclusion, our study shows that bodybuilding and energy supplements are commonly used by ADF personnel who have served in the Middle East. Our data indicate that patterns of use are associated with employment and lifestyle factors, as well as health symptoms. Although we were unable to ascertain absolute amounts of intake of dietary supplements and ingredients, our findings may help identify subgroups of Australian military personnel who may be at risk of possible side-effects.
Acknowledgements
Acknowledgements: The authors thank the veterans who participated in the survey. Helpful comments on this manuscript by Lieutenant Colonel Peter Nasveld are gratefully acknowledged. Financial support: The MEAO Census Study was funded by the Australian Government Department of Defence. The authors used data from the MEAO Census Study during the course of their employment with The University of Queensland, School of Public Health. The authors received no funding from the Australian Government Department of Defence for this specific work. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official, or representing the views of the Australian Defence Force or Department of Defence. The Department of Defence had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: J.C.v.d.P. oversaw data extraction and analyses, and wrote the paper; J.K. supported extraction of product data, carried out statistical analyses and helped write the paper; A.B. extracted product data and helped write the paper; C.-W.L. conceptualised the idea and helped write the paper. All authors read and approved the final manuscript. Ethics of human subject participation: Ethical approval for the present study was obtained from the Australian Department of Defence (protocol number LREP 14-010) and The University of Queensland (protocol number 2009001441) ethics committees. Participants of the MEAO Survey provided consent in writing or electronically, and all aspects of this research complied with the Declaration of Helsinki.




