


Puberty marks the change to a reproductive state, and for females, begins with breast development (thelarche) and/or the appearance of pubic hair (pubarche), then progresses to other changes including the onset of menstruation (menarche). Research has shown evidence of a trend of earlier puberty in North American and Western European girls, which may be even more pronounced for thelarche than menarche(Reference Parent, Teilmann and Juul1, Reference Cabrera, Bright and Frane2). This is important because earlier pubertal development presents clinical health risks; earlier age at thelarche(Reference Bodicoat, Schoemaker and Jones3) and menarche(Reference Titus-Ernstoff, Longnecker and Newcomb4, 5) have both been associated with increased risk of breast cancer, the most common cancer and second highest cause of cancer deaths among women in the USA(6). Specifically, every year younger at menarche has been associated with a 5 % greater risk of breast cancer(5) and thelarche at age 10 years or younger has been associated with a 23 % greater risk of breast cancer (compared with thelarche at age 11–12 years)(Reference Bodicoat, Schoemaker and Jones3).
Diet is likely to play a role in the timing of puberty and previous research has assessed the relationship of some foods and nutrients with puberty outcomes. A cross-sectional study of Spanish girls found consumption of nuts and seeds to be inversely related to menarche in teenage girls(Reference Soriguer, Gonzalez-Romero and Esteva7) and a prospective study of girls in Colombia found that a high childhood intake of red meat is significantly associated with earlier age at menarche(Reference Jansen, Marín and Mora-Plazas8). Higher intake of MUFA has been associated with a later age at menarche among peripubertal Canadian girls(Reference Moisan, Meyer and Gingras9), but a longitudinal cohort study of British girls found no evidence of an association between MUFA intake and occurrence of menarche(Reference Rogers, Northstone and Dunger10). Several studies have found menarche to be significantly delayed in girls with high childhood fibre intakes(Reference Koo, Rohan and Jain11, Reference de Ridder, Thijssen and Van’t Veer12), while other studies found no association between peripubertal fibre intakes and menarche or thelarche(Reference Moisan, Meyer and Gingras9, Reference Cheng, Remer and Prinz-Langenohl13). The inconsistent findings in the existing literature may be due to examining isolated foods or nutrients, which fails to consider potential interactions between them.
An alternative approach is to study overall food patterns, in order to capture the multiple dimensions of a diet and account for potential interactions among foods and nutrients. The aforementioned foods and nutrients are all components that define a Mediterranean-like diet: one high in plant-based foods (such as fibre-rich whole grains, vegetables, fruits, nuts and legumes), unsaturated fats and fish, but low in red and processed meats. A ‘Mediterranean diet’ generally refers to the type of diet traditionally consumed by people in Mediterranean countries such as Spain, Greece and Italy, and has been studied widely in relation to various health outcomes(Reference Dinu, Pagliai and Casini14–Reference Bloomfield, Koeller and Greer16). Research suggests a Mediterranean-like diet offers a reduction in all-cause mortality(Reference Sofi, Macchi and Abbate17) and obesity(Reference Garcia, Shook and Kerstetter18, Reference Papavagelis, Avgeraki and Augoulea19), as well as a reduction in incidence of and mortality due to cardiovascular, cerebrovascular and neoplastic diseases including cancer(Reference Schwingshackl, Schwedhelm and Galbete15, Reference Sofi, Macchi and Abbate17). However, the relationship between a Mediterranean-like diet and puberty timing and outcomes has not been evaluated to date. Thus, the present study aimed to contribute to filling a gap in the literature on this topic by evaluating the role of adherence to a Mediterranean-like diet in pubertal development in a cohort study of New Jersey girls.
Methods
Study population
The Jersey Girl Study is a longitudinal cohort study based at the Rutgers Cancer Institute of New Jersey. From 2006 to 2014, 202 eligible girls aged 9–10 years were recruited through paediatric practices, with secondary recruitment through other methods including flyers and word of mouth. Eligibility criteria included: New Jersey resident, living with biological mother, no cognitive impairments, ability to speak and read English, and no known major medical or surgical conditions affecting growth or reproductive development. At baseline, each girl participated in a study visit during which data on anthropometrics and puberty staging were collected. Annual follow-up with the cohort was done by mail through June 2018. The current study analyses cross-sectional baseline data, as well as longitudinal follow-up data on growth and puberty outcomes. Additional information on the Jersey Girl Study is available elsewhere(Reference Bandera, Chandran and Buckley20). All participating girls provided assent and their mothers signed informed consent.
General questionnaire
The general questionnaire from the Jersey Girl Study included items on socio-economic status, race/ethnicity, social factors and family structure, medical history, medication use, mother’s age at menarche, age of onset of the girl’s menarche and thelarche (if applicable), date of last menstrual cycle (if applicable), consumption of dietary supplements, environmental factors, prenatal and early childhood factors, and physical activity. The questionnaire was filled out at study baseline by the girls’ biological mother (or other guardian) with the assistance of the girls and study staff, if necessary.
Dietary intake assessment and adapted Mediterranean-like Diet Score
Diet history information was collected using three 24 h recalls conducted by the Dietary Data Entry Center at Cincinnati Children’s Hospital Medical Center. The data were collected by Dietary Data Entry Center staff on different days of the week, via telephone calls with the girl’s mother, over a period of approximately one week to one month around the time of the girl’s baseline study visit. The Dietary Data Entry Center uses the Nutrition Data System developed and maintained by the Nutrition Coordinating Center at the University of Minnesota(Reference Loth21). Descriptions and quantities of specific foods consumed, and the nutrient and energy intakes for each participant, were provided to the staff of the Jersey Girl Study. A systematic review of the validity of methods for dietary assessment in children suggested that 24 h dietary recalls reported by parents over at least three days, including weekdays and weekend days, provides accurate estimates of total energy intake in children of this age(Reference Burrows, Martin and Collins22).
We conducted a thorough literature search of previous studies that evaluated intake of a Mediterranean-like diet in paediatric populations. This literature was previously summarized in a systematic literature review by Idelson et al.(Reference Idelson, Scalfi and Valerio23). Most studies used the KIDMED index(Reference Serra-Majem, Ribas and Ngo24), which calculates a score based on the answers to sixteen yes/no questions about eating habits and consumption of different food groups. We reviewed twenty previous studies that used some version of a Mediterranean Diet Score, another method of assessment that has been used in adult populations(Reference Trichopoulou, Costacou and Bamia25), to assess Mediterranean diet adherence in children. Based on these indices and foods more commonly consumed in our population, we used an adapted Mediterranean-like Diet Score(Reference Idelson, Scalfi and Valerio23, Reference Trichopoulou, Costacou and Bamia25). We replaced the more traditional beneficial component of olive oil, which was marginally consumed in our study sample, with an unsaturated:saturated fat ratio in our diet score, as did several other studies of Mediterranean diet in children(Reference Tognon, Moreno and Mouratidou26–Reference Jennings, Welch and van Sluijs28). Food groups included as ‘beneficial’ components were vegetables (not potatoes), legumes, nuts, fruits, whole grains, fish, non-fat/low-fat dairy and unsaturated:saturated fat ratio (see details in Table 1). Traditionally, dairy consumed in Mediterranean countries is full-fat and considered to be detrimental, but whole-milk consumption was very low in our sample. We considered non-fat and low-fat dairy as a beneficial component, which is consistent with other studies of Mediterranean diet in children(Reference Serra-Majem, Ribas and Ngo24, Reference Jennings, Welch and van Sluijs28). Red or processed meat intake was included as a ‘detrimental’ component. The mean intake over the three 24 h dietary recalls was used. For each beneficial component, 1 point was given for an intake above the median or any intake when less than half of the sample were consumers (as with legumes, nuts and fish). For the detrimental component, 1 point was given for an intake below the median. The points were summed to give a total score which ranged from 0 to 9, with a higher score indicating higher adherence to a Mediterranean-like diet. The details of the median consumption, percentage of consumers of each food group, foods included and excluded for each category, and criteria for diet score calculation are included in Table 1. In our analysis, the Mediterranean-like Diet Score was used both as a continuous variable and a categorical variable divided into low (score 0–3), medium (score 4–5) and high (score 6–9) adherence groups, with the cut-offs based approximately on tertiles of the score in the total study sample.
Table 1 Food group categories for the Mediterranean-like Diet Score

N/A, not applicable.
* Wholegrain/partial wholegrain foods were included if they had a fibre:total carbohydrate ratio of 0·11 (1·1 g fibre to 10 g carbohydrates)(Reference Lloyd-Jones, Adams and Brown47).
Anthropometry and puberty assessment
Trained members of the Jersey Girl Study staff recorded the height and weight at study baseline and calculated BMI (weight in kilograms divided by the square of height in metres). BMI-for-age percentiles and Z-scores were calculated using the SAS program based on the growth charts of the Centers for Disease Control and Prevention(29).
Puberty was evaluated using the Tanner scale, which ranges from stage 1 (prepubertal) to stage 5 (post-pubertal)(Reference Marshall and Tanner30). Tanner stage was reported by the girls’ mothers using a form with pictorial representations and descriptions of each stage; a physician also examined the girls and filled out the same form at the baseline study interview. Thelarche at baseline was defined as a Tanner stage of 2 or greater, as reported by the physician (or as reported by the mother in the sixteen girls who did not have physician staging). Our previous analysis of agreement between mother and physician Tanner staging for breast development found agreement to be high (over 85 % agreement, κ = 0·7)(Reference Bandera, Williams and Marcella31).
Age at thelarche was determined using two different questions. First, at baseline and on each follow-up form, mothers were asked if girls’ breasts had started to develop, and if so, at what age. Second, mothers were asked to provide an update on Tanner staging, as discussed above, at baseline and each annual follow-up (until menarche). Age at thelarche was based purely on mothers’ report, since physician validation was available only at the time of the baseline interview. If the mother reported breast development at baseline, and reported an age of breast development, this was used as age at thelarche. When this age was missing or there were inconsistencies in the mother’s report, we determined age at thelarche as follows. If the mother reported a Tanner stage of 2 or greater before the reported age at thelarche (or age at thelarche was missing; n 36), the age at report of Tanner stage 2 (or 6 months before, in cases of girls aged 10 years or older at report) was used as an estimate of the correct age at thelarche. If a mother estimated an age in years but not months (n 16), the age in years plus 6 months was used. If the mother’s estimate at the subsequent follow-up was similar but more precise (n 2), that estimate of age was used.
Date of the first menstrual period was asked during the baseline interview and on each subsequent annual follow-up questionnaire. If only the month and year were provided, the 15th of the month was imputed as the date of first menstrual period.
Annual follow-up
Follow-up information was collected annually via mail by a form filled out by girls, their mothers, or both. The follow-up form asked if girls had reached menarche, and if so, at what date; if girls’ breasts had started to develop, and if so, at what age (years and months); and current height and weight. Tanner staging was evaluated using the same forms that had been completed at baseline. Girls were followed up for a median of 2·5 years after study baseline.
Statistical analyses
We compared participants’ characteristics between groups with high (6–9), medium (4–5) and low (0–3) Mediterranean-like Diet Score using the χ 2 test, Fisher’s exact test or ANOVA, as appropriate. Binomial regression models were fit to compute prevalence ratios and 95 % CI to examine the association between adherence to a Mediterranean-like diet and thelarche at baseline. Since the binomial regression models did not converge, we used Poisson regression models with sandwich variance estimation to approximate the model(Reference Zou32). Linear regression models were fit to compare predicted mean age at thelarche based on girls’ adherence to a Mediterranean-like diet. Cox proportional hazards models were fit to compute hazard ratios and 95 % CI to examine the association between adherence to a Mediterranean-like diet and time to menarche (using age as the time scale).
Potential confounders of interest that were considered for adjustment in the multivariable models included: age at baseline (continuous), race (White or other), annual household income (<$US 70 000, $US 70 000–84 999, $US 85 000–99 999, ≥$US 100 000), mother’s education (high school-associate degree, bachelor’s degree, master’s degree, professional/doctoral degree), total energy intake (kcal/d) at baseline, total hours of girl’s physical activity per week (at baseline) and BMI (Z-score) at baseline. Additionally, as there is a hereditary component to pubertal timing, maternal age at thelarche/menarche was considered for inclusion in the respective models. (For use in the models, the mother’s age at thelarche categories were collapsed since only two women reported thelarche before the age of 8 years.) Covariates included in the final models were selected based on a priori hypotheses as well as statistical significance level (P < 0·05) in the models.
In addition to evaluating a Mediterranean-like dietary pattern overall, the influence of specific food groups on thelarche and menarche was explored by fitting both separate models and models which were mutually adjusted for other food groups that were part of the Mediterranean-like Diet Score. Since Mediterranean-like Diet Score of 4 comprised 23 % of the sample, sensitivity analysis was run with adherence groups recategorized as 0–3, 4 and 5–9. Another sensitivity analysis was performed by excluding those girls (n 26) whose reported Tanner staging at baseline disagreed with physician-assessed Tanner staging.
All analyses were conducted using the statistical software package SAS version 9.4.
Results
The distributions of demographic and socio-economic characteristics of the study sample are presented in Table 2. Overall, girls entered the study at a mean age of 10·02 (sd 0·58) years. They were physically active, exceeding the Centers for Disease Control and Prevention’s recommendation of 1 h physical activity/d, with a mean of 8·84 h physical activity/week. The study sample was predominantly (88 %) White and affluent, with 69 % of families having an annual income of ≥$US 100 000 per year. Mothers were highly educated, with 34 % having a bachelor’s as their highest degree, and 46 % having a master’s degree or higher level of education. These demographic and socio-economic factors did not differ by diet adherence group. Total energy intake tended to be higher with greater adherence to a Mediterranean-like diet. Dietary energy density (kcal/g food, not including water) was lower with higher adherence to a Mediterranean-like diet.
Table 2 Selected characteristics and puberty outcomes according to Mediterranean-like diet adherence in girls aged 9 or 10 years at baseline (2006–2014, n 202), Jersey Girl Study, USA

Data are presented as n and % unless indicated otherwise. Categories may not total to 100 % due to missing values.
P values for means from ANOVA; for frequencies from χ 2 test; for mother’s age at thelarche from Fisher’s exact test. Statistical significance at P < 0·05.
† 2008 was the approximate median year of recruitment for the study.
Nearly 60 % of girls (n 120) had begun breast development (Tanner stage 2 or higher) at their baseline visit, with a mean age at thelarche of 10·19 (sd 1·27) years. Girls reached menarche at a mean of 12·76 (sd 1·39) years of age. Over a median follow-up of 2·5 years (range: 0–7·5 years), 171 girls (84·65 %) reached menarche. Girls’ BMI and BMI category, and mother’s age at menarche, did not differ according to Mediterranean-like diet adherence group (Table 2). In bivariate analyses, mother’s age at thelarche differed across low, medium and high adherence groups. Although not statistically significant, girls with high adherence to a Mediterranean-like diet were less likely to have reached thelarche at baseline and tended to have later age at thelarche and menarche.
The results of the multivariable Poisson regression model for thelarche at baseline in relation to Mediterranean-like diet adherence are presented in Table 3. In the full model (adjusted for age at baseline, baseline total energy intake, BMI Z-score at baseline and mother’s age at thelarche), high adherence to a Mediterranean-like diet (score 6–9) was associated with 35 % lower prevalence of thelarche at baseline, compared with low adherence (score 0–3; prevalence ratio = 0·65, 95 % CI 0·48, 0·90). Adherence to a Mediterranean-like diet on a continuous scale also suggested a lower prevalence of thelarche at baseline per unit increase in diet adherence score, although this was not statistically significant.
Table 3 Prevalence ratio (PR) and 95 % CI for thelarche at baseline (yes v. no) according to Mediterranean-like diet adherence in girls aged 9 or 10 years at baseline (2006–2014, n 202), Jersey Girl Study, USA
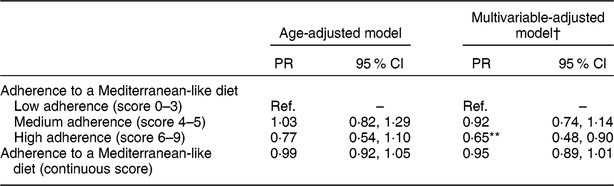
Ref., reference category.
** P < 0·01.
† The multivariable-adjusted Poisson regression model controlled for age at baseline, girl’s total energy intake, girl’s BMI Z-score at baseline and mother’s age at breast development.
Additional models were fit to further investigate the relationship of the specific dietary components of our Mediterranean-like Diet Score and thelarche (results are presented in the online supplementary material, Supplemental Table S1). Fish consumption was significantly inversely associated with thelarche (prevalence ratio = 0·77, 95 % CI 0·61, 0·97) in a fully adjusted model which was mutually adjusted for the other Mediterranean-like diet components. High v. low consumption of non-fat/low-fat dairy showed a significant inverse relationship with thelarche (prevalence ratio = 0·75, 95 % CI 0·60, 0·93) in the mutually adjusted model.
The results of a multivariable linear regression model for mean age at thelarche are presented in Table 4. In the fully adjusted model (controlling for age at baseline, baseline total energy intake, BMI Z-score at baseline and mother’s age at thelarche), our results suggested a later age at thelarche with higher Mediterranean-like diet adherence (mean age of 10·42 v. 10·05 years for high v. low adherence). Our sensitivity analysis, which excluded those girls whose maternally assessed Tanner staging at baseline disagreed with physician-assessed Tanner staging, showed similar results (data not shown). The results of a multivariable Cox proportional hazards model (using age as the time scale) for time to menarche are presented in Table 5. In the fully adjusted model (controlling for age at baseline, race, baseline total energy intake, physical activity, BMI Z-score at baseline and mother’s age at menarche), higher adherence to a Mediterranean-like diet was significantly associated with longer time to menarche for girls with high v. low adherence (hazard ratio = 0·45, 95 % CI 0·28, 0·71). Similarly, adherence to a Mediterranean-like diet on a continuous scale showed significantly longer time to menarche (hazard ratio per unit increase in diet adherence score = 0·89, 95 % CI 0·82, 0·98). Further exploring the individual diet components showed vegetable consumption and non-fat/low-fat dairy consumption to be significantly related to longer time to menarche in the mutually adjusted model (hazard ratio = 0·66, 95 % CI 0·46, 0·95 and hazard ratio = 0·63, 95 % CI 0·43, 0·91, respectively). These results are presented in the online supplementary material, Supplemental Table S2.
Table 4 Mean age at thelarche and 95 % CI according to Mediterranean-like diet adherence in girls aged 9 or 10 years at baseline (2006–2014, n 202), Jersey Girl Study, USA
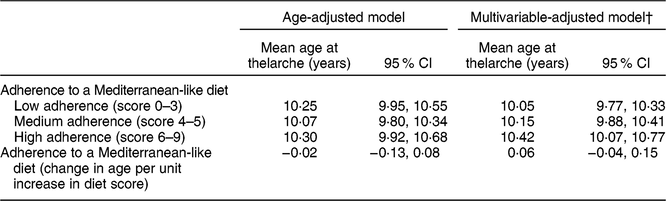
† The multivariable adjusted linear regression model controlled for age at baseline, girl’s total energy intake, girl’s BMI Z-score at baseline and mother’s age at breast development.
Table 5 Hazard ratio (HR) and 95 % CI for time to menarche according to Mediterranean-like diet adherence in girls aged 9 or 10 years at baseline (2006–2014, n 202), Jersey Girl Study, USA
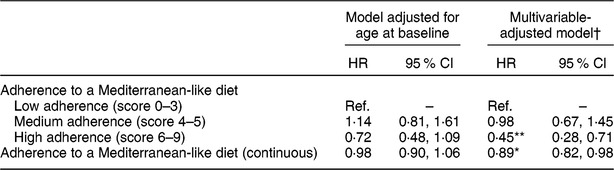
Ref., reference category.
* P < 0·05, **P < 0·01.
† The multivariable adjusted Cox model controlled for age at baseline, race, total energy intake, physical activity, girl’s BMI z-score at baseline, and maternal age at menarche.
Sensitivity analysis which recategorized Mediterranean-like Diet Score groups as 0–3, 4 and 5–9 for all of the above analyses demonstrated results that were essentially the same (data not shown).
Discussion
In the present study, higher adherence to a Mediterranean-like diet was associated with significantly lower odds of thelarche at baseline, as well as later age at thelarche. This association may be driven by higher consumption of fish and non-fat/low-fat dairy. Higher adherence to a Mediterranean-like diet was also associated with longer time to menarche in the present study. Our results suggest that this relationship may be driven by higher consumption of vegetables and non-fat/low-fat dairy.
The present study is the first to investigate the relationship between adherence to a Mediterranean-like diet and puberty timing. Our results are consistent with previous findings suggesting that higher intakes of MUFA(Reference Moisan, Meyer and Gingras9, Reference Koo, Rohan and Jain11), fibre(Reference Koo, Rohan and Jain11, Reference de Ridder, Thijssen and Van’t Veer12), canned fish(Reference Jansen, Marín and Mora-Plazas8) and low-fat dairy(Reference Gaskins, Pereira and Quintiliano33), and lower intake of red meat(Reference Jansen, Marín and Mora-Plazas8) (all components of our Mediterranean-like Diet Score), are associated with a later age at menarche. They are also consistent with another recent study, conducted among Mexican children, which found dietary patterns characterized by vegetables and lean proteins (legumes, chicken and organ meat) to be inversely related to breast development(Reference Jansen, Zhou and Perng34). In our study, although higher adherence to a Mediterranean-like diet was associated with longer time to menarche, intakes of unsaturated fats, fibre and red meat did not show independent associations with menarche timing. Other studies have similarly observed no association between age at menarche and intake of MUFA(Reference Rogers, Northstone and Dunger10) or fibre(Reference Moisan, Meyer and Gingras9, Reference Cheng, Remer and Prinz-Langenohl13). It is plausible that relationships of MUFA and fibre intake with age at menarche observed in some previous studies actually represent the effect of an overall dietary pattern that includes high unsaturated fat and fibre intakes, such as a Mediterranean-like diet. A previous study of Spanish girls showed evidence of an inverse relationship between nut and seed consumption and menarche(Reference Soriguer, Gonzalez-Romero and Esteva7), which was not demonstrated in our sample, and may likewise have been the effect of an overall dietary pattern. Also, consumption of nuts and seeds was low in our population, which may have affected our power to detect an association.
Our analysis indicated that consumption of non-fat/low-fat dairy was independently associated with later age at both thelarche and menarche, in accordance with another recent prospective study of Chilean girls that found low-fat dairy to be associated with later age at menarche (P trend < 0·001)(Reference Gaskins, Pereira and Quintiliano33). However, several previous studies did not observe significant associations between dairy or low-fat dairy consumption in children and age at menarche(Reference Jansen, Marín and Mora-Plazas8, Reference Rogers, Northstone and Dunger10, Reference Carwile, Willett and Wang35, Reference Kwok, Leung and Lam36). A prospective study of prepubertal girls in Iran found a higher risk of earlier menarche in girls with higher milk intake, but the relationship was not significant for cheese or yoghurt consumption(Reference Tehrani, Moslehi and Asghari37). In the USA, Wiley found evidence that greater milk intake was associated with earlier age at menarche (P < 0·06)(Reference Wiley38). Thus, the association between different types of dairy intake and age at thelarche and menarche requires further study, especially since composition and hormone levels in milk and dairy products may vary across different regions and countries(Reference Schönfeldt, Hall and Smit39, Reference Kolok, Ali and Rogan40).
Consuming a Mediterranean-like diet may contribute to higher levels of sex hormone-binding globulin (SHBG)(Reference Berrino, Bellati and Secreto41) and lower levels of endogenous oestrogens(Reference Carruba, Granata and Pala42), which could result in later puberty onset. Initiation of puberty is accompanied by a release of gonadotrophins, decreased levels of SHBG and increased levels of oestrogens, and moreover, early pubertal plasma oestrogen levels predict the rate of pubertal development. Several proposed mechanisms for the influence of a Mediterranean-like diet on SHBG and hormone levels centre around the effects of fibre and phyto-oestrogens. This is consistent with our findings, since both fibre and phyto-oestrogens are found in food sources such as vegetables, fruits, seeds, nuts and beans, which are higher in a Mediterranean-like diet. For example, dietary fibre may reduce circulating bioavailable oestrogen levels(Reference de Ridder, Thijssen and Van’t Veer12, Reference Gaskins, Pereira and Quintiliano33) as well as follicle-stimulating hormone and luteinizing hormone levels(Reference de Ridder, Thijssen and Van’t Veer12). It may also inhibit the reabsorption of steroid hormones in the gut, leading to increased excretion of oestrogens from the body(Reference Goldin, Adlercreutz and Gorbach43). Phyto-oestrogens, furthermore, may stimulate liver synthesis of SHBG, which reduces biological availability of sex hormones(Reference Adlercreutz44). Thus, the observed impacts of a Mediterranean-like diet and its components on SHBG and hormone levels provide a plausible mechanism for the influence of such a diet on the timing of puberty, as we found in the present study. Further research that measures SHBG and hormone levels is needed to elucidate these mechanisms.
One strength of our study was prospective data collection on age at menarche, which avoided recall bias. Data on age at thelarche were collected within approximately 2 years of thelarche, which reduced the potential for recall bias. We collected detailed dietary data representative of the peripubertal period and the dietary recall interviews allowed for capturing intake of exact foods consumed on both weekdays and weekends. The detailed study questionnaire and anthropometric measurements, obtained during an in-person interview, also provided us with a wide range of potentially relevant confounding variables for consideration in our regression models.
Several limitations should also be acknowledged. First, the sample was predominantly White, with generally high household income and highly educated mothers, which may limit the generalizability of the findings to other populations. As with many other studies of diet and puberty, some of our analyses were cross-sectional and could have resulted in reverse causation, as over half of girls had already reached thelarche at baseline when the dietary recall was done. These analyses were based on the assumption that overall dietary patterns would tend to be stable over the time frame of only a few years(Reference Northstone, Smith and Newby45). The fact that the cross-sectional results are in the same direction as our longitudinal analysis results provides reassurance in our findings. The definition of a Mediterranean-like diet has been inconsistent in the existing literature, which impedes the ability to directly compare results across studies. While Tanner staging is a validated and widely used method of assessing thelarche, it is inherently subjective. As such, thelarche outcomes may have been potentially misclassified, although this would be expected to be non-differential with regard to diet. Differences in age at thelarche across adherence groups were relatively small and the clinical significance of this finding is unknown. However, overall findings point to later age in onset of pubertal landmarks, which warrants further study. Finally, the sample size was relatively small (n 202), which limited the statistical power of some analyses and suggests a need for larger studies to examine this important issue.
The timing of puberty is important from a public health point of view because of links between early pubertal development and subsequent clinical outcomes, including cancer risk. Therefore, identifying modifiable lifestyle factors that may prevent early onset of puberty is critical. To our knowledge, the present study is the first evaluating associations of a Mediterranean-like diet and puberty outcomes in girls in the USA. Our results suggest that higher adherence to this type of dietary pattern, high in plant-based foods (like fibre-rich whole grains, vegetables, fruits, nuts and legumes), unsaturated fats and fish, and low in red and processed meats, may decrease girls’ risk of earlier puberty. Unfortunately, in the USA, the current average daily intakes of vegetables, fruits, legumes, dairy, whole grains, seafood and nuts in this peripubertal age group are well below the recommended amounts(46). Nutrition recommendations may be easier to follow if they are operationalized as a dietary pattern or even as a healthy lifestyle rather than focused on individual foods. Our results lend support that a Mediterranean-like dietary pattern may offer some benefits to peripubertal girls. Nevertheless, further research is necessary to confirm our findings in other US paediatric populations. Future studies should also investigate the mechanism through which Mediterranean-like diet may be influencing puberty and growth by examining sex-steroid pathway hormones (including girls’ SHBG, oestrogen, androgen and gonadotrophin levels) in relation to dietary patterns.
Acknowledgements
Acknowledgements: The authors are indebted to the many organizations who helped with recruitment, but especially to Princeton Nassau Pediatrics. They are particularly grateful to all their girls and their mothers who enthusiastically agreed to contribute to the research. Financial support: This work was supported by Rutgers Cancer Institute of New Jersey and Rutgers Cancer Institute of New Jersey Foundation. The funding agencies had no role in the design, analysis or writing of this article. Conflict of interest: None disclosed. Authorship: E.A.S., E.V.B. and B.Q. designed the study; E.A.S. and E.V.B. conducted the study; E.A.S., B.Q. and Y.L. analysed the data; E.A.S. and E.V.B. wrote the first draft of the paper; B.Q., N.P., E.S.B., Y.L., Z.R.-N. and J.F. contributed to the interpretation of results; E.A.S. and E.V.B. had primary responsibility for final content. All authors read, edited and approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Rutgers University Health Sciences Institutional Review Board. All participating girls provided assent and their mothers signed informed consent.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980019002349.







