



The Emergence of a Pandemic
The outbreak of the new coronavirus infection (coronavirus disease 2019 [COVID-19]), which has become a global problem for humanity, was caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, registered in Wuhan, China, in December 2019. In Kazakhstan, the first cases of COVID-19 were detected on March 13, 2020 among people who arrived from Germany. The incidence of the disease subsequently increased exponentially throughout the world. The high migration activity of the population contributed to the spread of the viral infection around the world.
On January 30, 2020, the Director-General of the World Health Organization (WHO) declared the COVID-19 outbreak as a public health emergency of international concern (PHEIC). As of March 4, 2020, cases of COVID-19 have been reported in 77 countries. Several countries succeeded in reducing or stopping transmission of the COVID-19 virus. The Strategic Plan for Preparedness and Response to COVID-19, as recommended by WHO, was aimed at slowing and stopping transmission; preventing outbreaks and reducing the rate of spread of the disease; ensuring optimal care for all patients, especially those who are critically ill; minimizing the negative impact of the pandemic on health systems, social services, and economic activity. 1
According to WHO, countries needed to have a comprehensive preparedness package in the following situations: likelihood of further spread, potential impact on human health, effectiveness of current preparedness, and response measures. The priorities and intensity of work in each technical area depend on which scenario is currently developing in the country or part of it. 2
In Kazakhstan, the Head of State declared a state of emergency, and the Ministry of Healthcare began to develop a unique comprehensive system for assessing and forecasting the epidemiological situation with a set of restrictive measures. At the same time, the Ministry of Healthcare was faced with the task of expanding the scope of work from admitting patients and counseling to predicting the epidemiological situation throughout the country with several options to mitigate the health risks to the population. The article describes the developed comprehensive system with a set of restrictive measures for assessing and forecasting the epidemiological situation, which was approved by the WHO Country Office in the Republic of Kazakhstan. Later, it was adapted by the EU countries and applied in Kyrgyzstan.
Measures to Counter Coronavirus Disease
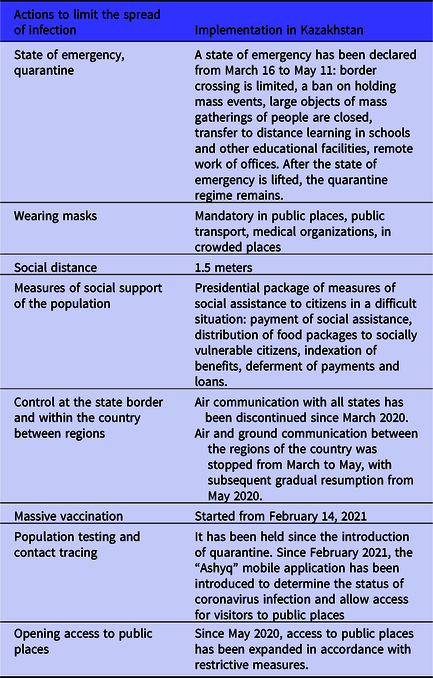
Implementing Actions to Limit the Spread of Infection in Relation to the Population of the Republic of Kazakhstan
A brief overview of the actions is presented in Table 1.
Table 1. Overview of actions taken to limit the spread of COVID-19 infection in relation to the population of the Republic of Kazakhstan
Improving the Work of the Sanitary and Epidemiological Service
To improve the work of the sanitary and epidemiological service, its status was upgraded. The Committee for Sanitary and Epidemiological Control of the Ministry of Healthcare has been established, the status and powers of the Chief State Sanitary Doctor of the Republic of Kazakhstan have been increased, and salaries for employees exercising state sanitary and epidemiological supervision have been increased. 3
Increasing the Number of Medical Organizations
In 2020, a total of 16 modular infectious diseases hospitals were built and put into operation in Kazakhstani cities, 44 outpatient care facilities were reconstructed, including 30 facilities in rural areas, 3 infectious diseases hospitals, 64 oxygen stations were put into operation, and 63 outpatient—polyclinic organizations were put into operation. Measures have been taken to provide the population with medicines, medical devices, and personal protective equipment.
Mobilization and Social Support of Medical Personnel
All medical personnel were mobilized to fight the new coronavirus infection. As the Minister of Healthcare noted, speaking at an expanded meeting of the collegium of the institution, in the context of a pandemic, it became obvious that the results of the work of medical workers have a direct social effect, on which not only the life of specific people depends, but also the stability of the economy.
Particular attention was paid to measures of social support for medical workers involved in anti-epidemic measures in the form of material assistance. All employees directly involved in the fight against COVID-19 were paid allowances for 3 risk groups. Also, as part of the implementation of the instructions of the Head of State, the Ministry of Healthcare provided a gradual increase in the salaries of doctors, bringing its increase to 2.5 times.
Meanwhile at the local level:
-
Social support for doctors is provided through the provision of hostels, compensation for utilities, communication services, social payment of rent payments, allocation of places in kindergartens, employment of spouse;
-
Within the framework of local budgets, grants are provided for training in residency for targeted training of personnel, depending on the specifics and needs of each separate region;
-
A system of distribution of young specialists was introduced, taking into account regional needs.
The above measures taken in 2020 made it possible to reduce the shortage of medical personnel in the Republic of Kazakhstan by 25%.
Vaccination
On behalf of the head of state, from February 1, 2021, vaccination against coronavirus infection has begun in the Republic of Kazakhstan. To ensure the safety and effectiveness of vaccination in 2020, more than 2000 medical workers improved their skills in vaccination tactics against COVID-19.
Currently, the following types of vaccines are used in the Republic of Kazakhstan for vaccination of the population: QazCovid-in, Sputnik V, CoronaVac (Vero Cell), Vero Cell (Sinopharm), Sputnik Light, Hayat-Vax, Comirnaty (Pfizer), Sputnik M. 4
Development of Domestic Vaccine
On March 23, 2020, the Republican State Enterprise “Research Institute of Biological Safety Problems” of the Science committee of Ministry of Education and Science of the Republic of Kazakhstan, on behalf of the President of the Republic of Kazakhstan, began to develop a vaccine against coronavirus infection COVID-19.
On May 9, 2020, scientists presented the domestic inactivated vaccine QazCovid-in, which, according to the results of preclinical tests, was included in the list of candidate vaccines for coronavirus by the WHO. According to the results of Phase I and II clinical studies of the QazCovid-in vaccine against COVID-19, good tolerance and safety were noted with single and double intramuscular administration. The high immunogenic activity of the vaccine against the SARS-CoV-2 virus was established, more pronounced after double vaccination. On December 19, 2020, phase III of clinical trials of the domestic inactivated QazCovid-in began, which will be completed in April 2021. In addition, scientists have created a subunit vaccine QazCov-P, which is currently awaiting approval for clinical trials. Also, scientists of the institute are conducting research on the development of 3 more vaccines (2 vector and 1 attenuated) on various platforms.
Along with the work of local scientists, the Russian Sputnik V vaccine is also produced at the site of the local manufacturer Karaganda Pharmaceutical Complex LLP, which is used for the mass immunization of Kazakhstanis.
Epidemiological Surveillance
In parallel with practical measures, scientific developments were unfolded. The emergence of a new coronavirus confirms that the diseases caused by this group of viruses are a threat to global health and require a detailed study of their nature and distribution. The National Center for Public Health of the Ministry of Healthcare of the Republic of Kazakhstan was among the first to study this type of virus and was the first to identify the likelihood of mutation of the British, South African, and Brazilian strains. Epidemiological monitoring systems, development of indicators for predicting biological and main social risks associated with new and anticipated respiratory infectious diseases (including COVID-19) made it possible to substantiate an integrated monitoring system, creating a scientific and practical basis for assessing the implementation of the fight against the COVID-19 pandemic in Kazakhstan.
Digital technologies are of particular importance during the COVID-19 pandemic, combining the potential to improve surveillance and combat epidemics, mainly by expanding information coverage, increasing the speed of information transfer, quickly tracking cases, and predicting the epidemiological situation. Reference Vokinger, Nittas and Witt5–Reference Sarría-Santamera, Yeskendir and Maulenkul8
In this regard, the Electronic Integrated Disease Surveillance System (EIDSS) operating based on the National Center of Public Healthcare is an information system that allows to strengthen and provide support for monitoring and prevention of diseases within the framework of the “One Healthcare” concept.
The Severe Acute Respiratory Infection (SARI) sentinel surveillance system is a prospective surveillance system introduced in 2008 by the Ministry of Healthcare of the Republic of Kazakhstan with the support of the American Centers for Disease Control and Prevention (CDC). In large cities, including Nur-Sultan and Almaty, sentinel sites are infectious diseases hospitals that conduct testing for respiratory viruses (adenovirus, parainfluenza virus I-IV, respiratory syncytial virus, human metapneumovirus, bocavirus, coronavirus, and rhinovirus) using the method of polymerase chain reaction (PCR). Since autumn 2020, samples are also being tested for the SARS-CoV-2 virus. However, the etiology of a significant proportion of SARI cases is unclear.
This problem became most acute in the summer of 2020, when there was a significant increase in cases of pneumonia of unknown etiology, that is, with a negative PCR test for the SARS-CoV-2 virus. A significant excess in the number of these pneumonias compared with comparable periods of previous years, as well as the presence of clinical signs characteristic of COVID-19 viral pneumonias, suggested that most of them are caused by the SARS-CoV-2 virus, which was not detected by PCR testing. In this connection, at the end of July 2020, a change was made to the definition of a case of COVID-19, when a diagnosis could be made on clinical grounds without laboratory confirmation in the absence of other alternative causative agents of the disease (code U07.2). These issues require further study.
Discussion and Conclusions
The COVID-19 pandemic caused by the coronavirus (SARS-CoV-2) has wreaked havoc on public health and economies around the world. Reference Gorenkov, Khantimirova and Shevtsov9
One of the most notable features of SARS-CoV-2 infection is that most people are asymptomatic, while others have progressive, even life-threatening viral pneumonia and acute respiratory distress syndrome. Although factors influencing the severity of the disease (eg, increasing age, male gender, high body mass index, etc.) have been identified, these risk factors alone do not explain all the variability in disease severity observed among infected individuals. 10
The importance of the contribution of host genetics to the susceptibility and severity of infectious diseases is being actively studied and includes rare innate immunity errors, common genetic variations in single-nucleotide polymorphisms (SNPs), and the ability of the virus to mutate. Reference Ganna11,Reference Oude Munnink, Nieuwenhuijse and Stein12
Determining genetic factors that contribute to the susceptibility and severity of COVID-19 is of considerable research interest. It may reveal new biological insights into the pathogenesis of the disease and identify mechanistic targets for therapeutic developments or repurposing of existing drugs, since the treatment of the disease remains a very important goal despite successful development of vaccines. In particular, susceptibility to respiratory viruses such as influenza is inherited and is known to be associated with specific genetic variants in the host. In the case of COVID-19, 1 known genetic locus on chromosome 3p21.31 is associated with hospitalizations. As with other viral diseases, there are several examples of loss of function options that affect the underlying immune processes that lead to severe illness in young adults, such as the TLR711 gene and some genes involved in type 1 interferon signaling, including the receptor subunit IFNAR212. Reference Logunov, Dolzhikova and Shcheblyakov13,Reference Pairo-Castineira, Clohisey and Klalric14
Scientific work on the study of human genes associated with the incidence of coronavirus, carried out in the United Kingdom in 2000, made it possible to determine the goals for the therapy of COVID-19 with existing drugs. It was found that low expression of the IFNAR2 gene or high expression of the TYK2 gene are associated with severe forms of the disease. These studies have shown that these genetic variants, related to key mechanisms of host antiviral defense and mediators of inflammatory organ damage in COVID-19, can respond to targeted treatment with existing drugs. Reference Logunov, Dolzhikova and Shcheblyakov13
An important problem is the study of virus mutations, which seem to be a constant necessary evolutionary process, namely, linking certain genomic changes of the virus with its ability to spread, affect the severity of the disease, and also develop resistance to therapy, host immunity, or vaccines. And this issue requires careful and comprehensive research.
The issues of the spread of the virus and the clinical aspects of combating it are of considerable scientific interest. COVID-19 is a complex clinical syndrome with a wide variety of clinical manifestations. The proportion of people who are asymptomatic ranges from 20 to 75%. Most patients who do show symptoms develop only mild (40%) or moderate (40%) illness, approximately 15% develop severe illness, and <5% develop critical illness with complications such as respiratory failure, acute respiratory distress syndrome; population groups with diseases such as diabetes, hypertension, heart disease, chronic diseases are more at high risk of a serious course. Old age, smoking, and major noncommunicable lung diseases and cancer are risk factors for serious illness and death. Reference Chmielewska, Barrett and Townsend15–Reference Nagy, Pongor and Győrffy18
Current clinical treatment for COVID-19 consists of prevention and infection control measures and supportive care. The spectrum of medical treatments for COVID-19 is growing and evolving rapidly. It is believed that 2 main processes affect monitoring in health-care settings. The first phase of the development of infection is primarily due to the replication of SARS-CoV-2. Later in the course of infection, the disease is triggered by an enhanced immune/inflammatory procoagulant response that leads to tissue damage. Reference Mironov and Zabozlaev19,Reference Nikiforov, Suranova and Chernobrovkina20
Based on this understanding, antiviral therapy is expected to be most effective in the early stages, while immune/anti-inflammatory therapy may be more effective in the later stages of COVID-19.
An extremely important problem is the impact of the epidemic on health workers and the development of measures to protect them, strengthening the prevention of infections and infection control in medical organizations. Currently, the extent of the spread of COVID-19 infection in health-care facilities in the context of Kazakhstan is unknown, and it is also unknown whether there are specific risk factors associated with the infection of health-care workers. Reference Imai, Dorigatti and Cori21,22
At the global level and in countries, there are only limited data on the problem of infection of medical workers with the SARS-CoV-2 virus. Recently, the WHO published a summary of the extent of SARS-CoV-2 infection in health-care workers. 23
Health-care workers account for approximately 14% of COVID-19 cases, according to data collected primarily from the WHO Region of the Americas and the WHO European Region as part of WHO’s global COVID-19 surveillance. However, the proportion of health-care workers infected varies widely, from 2% to 35% in countries that filled more than 75% of the health-related variables in the reported data. Infection rates of health-care workers were influenced by timing of reporting, fluctuations in transmission patterns at the population level, and adherence to prevention of infections and infectious control (PIIC) in facilities.
According to a recently published report by the International Council of Nurses, which conducted a survey in 50 countries, mainly in Europe and America, infections of medical workers account for between 1% and 32% of all confirmed cases of COVID-19. 24
In responding to the pandemic, an internationally accepted quantification of the burden of disease will be of great strategic importance, which will identify the impact of the pandemic on public health. There are several ways to determine the burden of disease. Indicators such as prevalence and incidence characterize the magnitude and severity of the health problem. Pooled health indicators such as disability-adjusted life years (DALYs) are often used to represent the burden of disease. One DALY is 1 year of “healthy” life wasted, and the burden of disease can be seen as a measurement of the difference between an effective health condition and an ideal situation free of disease and disability in old age. 25
Using the Global Burden of Disease, Injury and Risk Factors (GBD) study, data on mortality and DALYs associated with COVID-19 can be obtained, and excess population mortality can be calculated as a proportion of the impact of COVID-19 and other causes. associated with crisis conditions.
The increased rates of COVID-19 cases and deaths in high-income countries are associated with the fact that, in these countries, a significant proportion of the population consists of older people with non-communicable diseases, including cardiovascular diseases. Reference Solanki, Kelly and Cornell26–Reference Hendren, de Lemos and Ayers29
The information component in the fight against the epidemic has become an extremely important problem and very much in demand. Any preventive measures taken must be based on facts, exclude misinformation, and induce rational, adaptive, and protective behavior of the population. However, little is currently known about the interactions of changing epidemiology, pandemic management measures, media activity, population perceptions of risks, psychoemotional consequences, and public health behavior.
Coronavirus is a new infection with many more questions. Study conducted during the influenza A (H1N1) pdm09 pandemic in 2009-2010 showed that the ultimate public perception of risks and behavior is influenced by the media and is not always based on the correct interpretation of the epidemiological and scientific evidence. Reference Qiu, Shen and Zhao30
From a psychological point of view, this means high uncertainty regarding the likelihood of contagiousness, the potential severity of the disease and the ability to control the process with preventive measures. These problems require a scientific explanation. With regard to general mental health, several studies using different methods (repeated cross-sectional and longitudinal studies) have recorded an increase in stress, anxiety, and depression among all categories of the population. Reference Ushakov, Yurevich and Nestik31,32
Therefore, the analysis of the socio-psychological consequences of the COVID-19 pandemic for the adult population makes it possible to understand this process in Kazakhstan and demonstrates the role of the media and other electronic means of communication in a pandemic.
Thus, the solution to the above problems will provide an opportunity to comprehensively and scientifically strengthen the system of public health measures to allow the control of the spread of possible newly emerging respiratory infections, including COVID-19. According to the report of the Ministry of Healthcare, further improvement in health care needs to occur in the following areas: affordable medical care with priority to villages, further strengthening of primary health care, stimulating the growth of the competencies of medical workers, hiring health-care professionals, patient medicinal and biological safety. All these areas will be implemented using digital technologies. 33
Author contribution
All authors contributed equally to preparation of the manuscript.
Funding
No sources of support that require acknowledgment.
Competing interests
No conflicts of interest to disclose.


 Open access
Open access