Letter to the editor
Sir,
Drug-induced movement disorders (DIMDs) are often considered preventable and potentially treatable neurological disorders. Despite their substantial burden, they are frequently overlooked and inadequately managed owing to poor quality of life.
We aimed to look into phenomenology, predictors of reversibility, and its impact on the quality of life of DIMD patients.
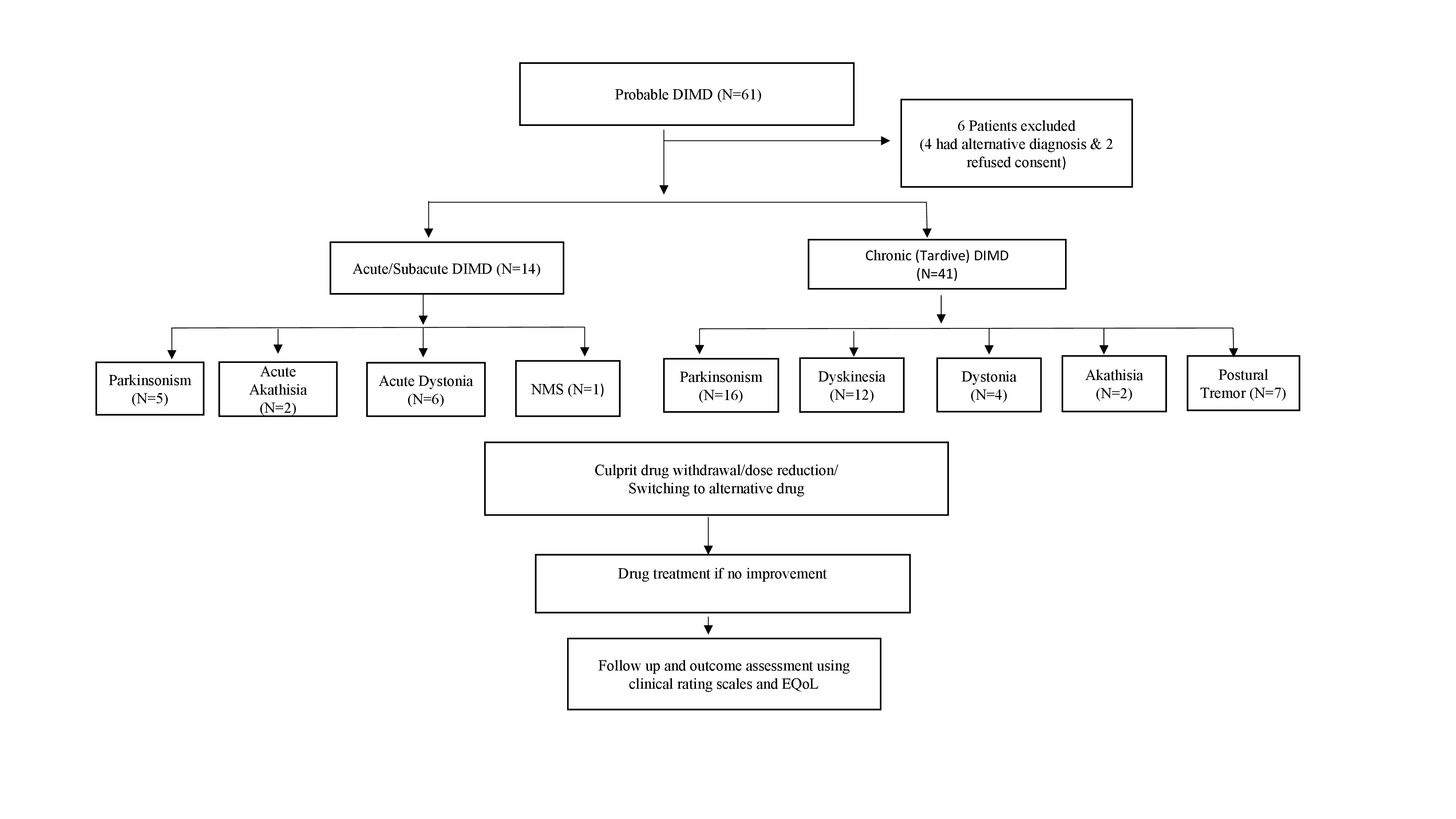
We conducted a prospective cohort study that included patients with DIMDs. The ethical committee duly approved the study (ECR/262/Inst/UP/2013/RR-16). Patients with a new-onset movement disorder secondary to exposure to a drug (probable ADR) were enrolled based on the Naranjo-Adverse Drug Reaction Probability Scale (Supplementary Figure 1). DIMD was diagnosed based on DSM-IV-TR criteria.1 We excluded patients with a pre-existing movement disorder, chronic liver disease, chronic kidney disease, and chronic alcoholism. We reviewed available medical records of drugs, their dosage, the indication for use, the latency of DIMD, total duration, co-morbidities, and positive family history. Patients were classified into different movement disorders per DSM-IV-TR criteria for medication-induced movement disorder. We used a standard videotape protocol to record abnormal movements. Clinical and video assessments of the patients were done by investigators (either HSM or SP). We used the Unified Parkinson’s Disease Rating Scale, Unified Dystonia Rating Scale, and Barnes akathisia Rating Scale for Parkinsonism, dystonia, and akathisia, respectively. The Abnormal Involuntary Movement Scale was used to assess tardive dyskinesia. The patient’s quality of life was assessed using the Hindi version of the European quality of life scale (EQ-5D-5L). It comprises five levels of difficulties, from no problem to extreme problems, in five domains scored as 0–4.
Patients with acute/subacute DIMD were followed at one week, two weeks, and three months, whereas chronic DIMD patients were assessed at 3- and 6-month intervals using the clinical rating scales and quality of life questionnaire. Reversible DIMD was defined if the abnormal involuntary movement completely disappeared after cessation of the offending drug, whereas persistent or recurrent abnormal involuntary movement, even after discontinuation of the offending drug or if patients were taking medications to control symptoms, was defined as irreversible. Wilcoxon signed-ranked test compared the various clinical rating scales and quality of life scores at presentation and follow-up to measure the statistically significant difference. Binary logistic regression analysis detected the independent predictors of the reversibility of DIMD. SPSS software for Windows (Version 24.0) performed the statistical analysis, and P values <.05 were considered statistically significant.
We enrolled a total of 55 patients. The mean age of our study population was 46.8 ± 18.59 years (range 7–77), and almost 75% (n = 41) of patients presented with chronic DIMDs. Females (52.73%, n = 29) outnumbered males (Table 1). Drug-induced Parkinsonism (DIP) was the most common movement disorder seen in 21 (38.18%) patients. Tardive dyskinesia was noted in 12 (21.82%) patients (Table 1). Risperidone (n = 20; 36.36%) and levosulpiride (n = 16; 29.10%) were the most frequently used drugs (Table 1).
Table 1. Clinical Characteristics, Outcomes, Comparison of Clinical Rating Scales and Quality of Life at Enrolment and at Follow-Up of Patients with DIMD

* Significance (P < .05).
Abbreviations: AIMS, Abnormal Involuntary Movement Scale; BARS, Barnes Akathisia Rating Scale; EQOL-5D-5L, European Quality of Life − 5 dimensions 5 levels; UDRS, Unified Dystonia Rating Scale; UPDRS, Unified Parkinson’s Disease Rating Scale.
a Wilcoxon signed ranked tests.
b Outcome assessment for acute–subacute and chronic DIMDs were done at 3 and 6 months, respectively.
The clinical rating scale and quality of life scores (EQ-5D-5L) showed significant improvement at follow-up in both groups of DIMD patients. Among patients with acute/subacute DIMD, the disease was reversible in 10/14 (71.42%) of the patients, whereas only 10/41 (24.40%) of patients with chronic DIMD had a reversible course (P < .001).
Univariate analysis revealed that advanced age, acute–subacute DIMD, and DIP were associated with reversible outcomes. Acute–subacute DIMD (OR 2.594; 95% CI: 2.115–84.702, P = .006) and DIP (OR 1.857; 95% CI: 0.033–0.742, P = .020) were independent predictors of reversibility on binary logistic regression.
Acute dystonic reactions were common in the young, whereas chronic DIMD was observed in the elderly. Striatal degeneration and decreased metabolic inactivation of drugs likely contribute to increased sensitivity to drugs, especially dopamine blockers.
The commonest DIMD in our study was DIP. In a study of levosulpiride-induced movement disorders, Parkinsonism was the commonest, followed by tardive dyskinesia.Reference Shin, Kim, Kim, Lee and Chung2 In another study of 97 patients, tardive dystonia (n = 41; 42.2%) and postural tremor (n = 38; 39.2%) were more frequent, followed by Parkinsonism (n = 32; 33%). Different drug profiles may be a plausible explanation as most of the patients were on non-dopamine receptor blockers.Reference Chouksey and Pandey3
As the most common DIMD, DIP may be due to its relatively shorter latency (a few weeks to 3 months) after drug exposure and prominent parkinsonian features. Complete reversibility after the offending drug’s withdrawal can also be a reason; however, it may be challenging to differentiate it from the unmasking of pre-existing Parkinson’s disease. On the contrary, tardive DIMDs present with oro-facial-lingual dyskinesias, often combined with other movement disorders. Its long latency and mostly irreversible course in the elderly population with co-morbidities and multiple drug treatments seem to be the reason for the under-recognition.
In our study, antipsychotic medications were the most common drugs associated with DIMD (38.46%), of which 80% of patients took second-generation antipsychotics. Widespread usage and off-label use can be the reasons for this observation. Moreover, the study endorses that EPS remains a significant issue even with newer atypical antipsychotics deemed to have less affinity for D2 receptors.
Intriguingly, levosulpiride was associated with DIMD in many patients. Levosulpiride contributes to almost 26%–68.93% of DIMDs comprising Parkinsonism, tardive dyskinesia, akathisia, dystonia, and tremors.Reference Choudhury, Chatterjee and Singh4 The higher percentage of DIMDs attributed to levosulpiride reflects its more frequent usage in current practice, especially for gastrointestinal problems. The poor dopaminergic reserve, poor drug metabolism, and interaction with multiple drugs may be the reasons for developing DIMD in patients.Reference Miller and Jankovic5 Increased numbers may also reflect that we included patients from the gastroenterology clinic. DIP is the commonest and often reversible DIMD. Levosulpiride is notorious for causing DIMD in the elderly, requiring strict pharmacovigilance. Chronic DIMDs are frequently irreversible, necessitating more effective therapeutic options.
Author contributions
Conceptualization: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Data curation: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Funding acquisition: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Investigation: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Methodology: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Project administration: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Resources: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Software: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Supervision: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Validation: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Visualization: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Writing—original draft: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.; Writing—review and editing: R.A., S.P., R.K.G., H.S.M., S.S., S.K.K., S.R., R.V., P.K.S., N.K., R.U., I.R.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1092852922001201.